
Safety and Immunogenicity of Enterovirus 71 Vaccine (Vero Cell) Administered Simultaneously with Trivalent Split-Virion Influenza Vaccine in Infants Aged 6–7 Months: A Phase 4, Randomized, Controlled Trial



Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Inclusion Criteria and Exclusion Criteria
2.3. Vaccines
2.4. Randomization and Masking
2.5. Safety Assessment
2.6. Immunogenicity Assessment
2.7. Statistical Analysis
3. Results
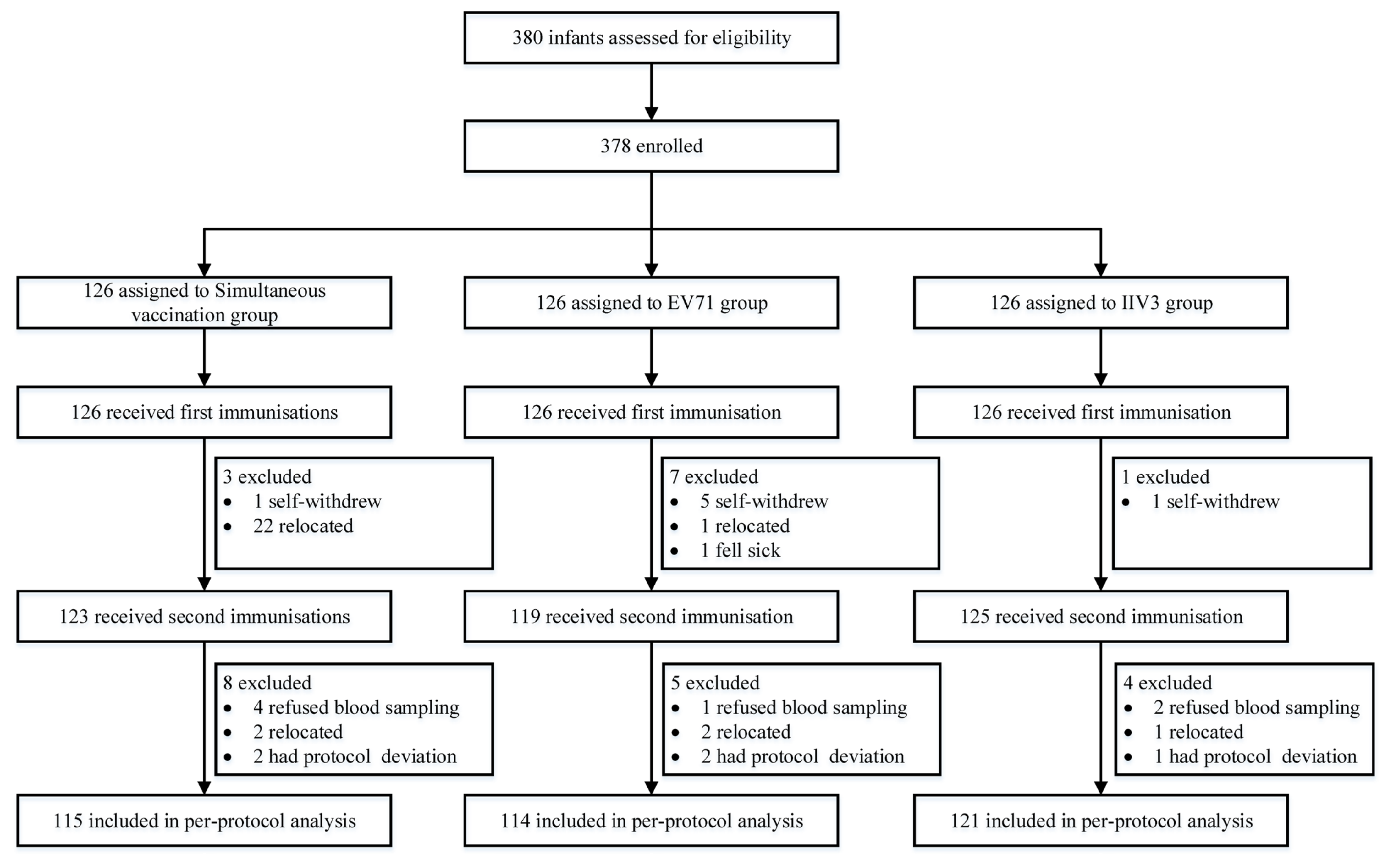
3.1. Study Participants
3.2. Safety Results
3.3. EV71 Antibody Results
3.4. Influenza Virus Antibody Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Esposito, S.; Principi, N. Hand, foot and mouth disease: Current knowledge on clinical manifestations, epidemiology, aetiology and prevention. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Xing, W.; Liao, Q.; Viboud, C.; Zhang, J.; Sun, J.; Wu, J.T.; Chang, Z.; Liu, F.; Fang, V.J.; Zheng, Y.; et al. Hand, foot, and mouth disease in China, 2008–2012: An epidemiological study. Lancet Infect. Dis. 2014, 14, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Huang, J.; Huai, Y.; Guan, X.; Klena, J.; Liu, S.; Peng, Y.; Yang, H.; Luo, J.; Zheng, J.; et al. The substantial hospitalization burden of influenza in central China: Surveillance for severe, acute respiratory infection, and influenza viruses, 2010–2012. Influenza Other Respir. Viruses 2014, 8, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Li, Y.; O’Brien, K.L.; Madhi, S.A.; Widdowson, M.A.; Byass, P.; Omer, S.B.; Abbas, Q.; Ali, A.; Amu, A.; et al. Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: A systematic review and modelling study. Lancet Glob. Health 2020, 8, e497–e510. [Google Scholar] [CrossRef] [PubMed]
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef] [PubMed]
- Kalligeros, M.; Shehadeh, F.; Mylona, E.K.; Dapaah-Afriyie, C.; van Aalst, R.; Chit, A.; Mylonakis, E. Influenza vaccine effectiveness against influenza-associated hospitalization in children: A systematic review and meta-analysis. Vaccine 2020, 38, 2893–2903. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Wang, J.; Zhang, C.; He, W.; Mo, J.; Zeng, J.; Chen, M.; Tan, Y.; Ning, C. Effectiveness of enterovirus A71 vaccine in severe hand, foot, and mouth disease cases in Guangxi, China. Vaccine 2020, 38, 1804–1809. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.P.; Liang, Z.L.; Gao, Q.; Huang, L.R.; Mao, Q.Y.; Wen, S.Q.; Liu, Y.; Yin, W.D.; Li, R.C.; Wang, J.Z. Safety and immunogenicity of a novel human Enterovirus 71 (EV71) vaccine: A randomized, placebo-controlled, double-blind, Phase I clinical trial. Vaccine 2012, 30, 3295–3303. [Google Scholar] [CrossRef] [PubMed]
- DiazGranados, C.A.; Saway, W.; Gouaux, J.; Baron, M.; Baker, J.; Denis, M.; Jordanov, E.; Landolfi, V.; Yau, E. Safety and immunogenicity of high-dose trivalent inactivated influenza vaccine in adults 50–64 years of age. Vaccine 2015, 33, 7188–7193. [Google Scholar] [CrossRef] [PubMed]
- The European Agency for the Evaluation of Medicinal Products: Committee for proprietary medicinal products (CPMP). Note for Guidance on Harmonization of Requirements for Influenza Vaccines; CPMP/BMW/214/96; The European Agency for the Evaluation of Medicinal Products: London, UK, 1997. [Google Scholar]
- Wei, M.; Meng, F.; Wang, S.; Li, J.; Zhang, Y.; Mao, Q.; Hu, Y.; Liu, P.; Shi, N.; Tao, H.; et al. 2-Year Efficacy, Immunogenicity, and Safety of Vigoo Enterovirus 71 Vaccine in Healthy Chinese Children: A Randomized Open-Label Study. J. Infect. Dis. 2017, 215, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.W.; Meng, F.Y.; Guo, H.J.; Hao, C.S.; Mao, Q.Y.; Gao, F.; Bian, L.L.; Duan, K.; Chen, X.Q.; Li, X.G. Five-year immunity persistence following immunization with inactivated enterovirus 71 vaccine (Vero cell). Int. J. Biol. 2020, 43, 261–266. [Google Scholar] [CrossRef]
- Pan, X.J.; Fu, J.; Shen, L.Z.; Lv, H.K.; Xiao, Y.H.; Chen, H.P.; Shi, X.W. Surveillance results of adverse events following immunization of enterovirus 71 inactvated vaccine. Prev. Med. 2019, 31, 1097–1099, 1104. [Google Scholar] [CrossRef]
- Head, J.R.; Collender, P.A.; Lewnard, J.A.; Skaff, N.K.; Li, L.; Cheng, Q.; Baker, J.M.; Li, C.; Chen, D.; Ohringer, A.; et al. Early Evidence of Inactivated Enterovirus 71 Vaccine Impact Against Hand, Foot, and Mouth Disease in a Major Center of Ongoing Transmission in China, 2011-2018: A Longitudinal Surveillance Study. Clin. Infect. Dis. 2020, 71, 3088–3095. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Liang, Z.; Zeng, J.; Zhang, J.; He, P.; Su, J.; Zeng, Y.; Fan, R.; Zhao, D.; Ma, W.; et al. Immunogenicity and Safety of an Inactivated Enterovirus 71 Vaccine Administered Simultaneously With Hepatitis B Vaccine and Group A Meningococcal Polysaccharide Vaccine: A Phase 4, Open-Label, Single-Center, Randomized, Noninferiority Trial. J. Infect. Dis. 2019, 220, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yang, W.; Zhang, C.; Wu, H.; Wang, R.; Ding, Q.; Hu, Y.; Xiong, Y.; Zhang, S.; Wang, L. Immunogenicity and safety of an inactivated enterovirus 71 vaccine co-administered with measles-mumps-rubella vaccine and live-attenuated Japanese encephalitis vaccine: A phase 4, single-center, randomized controlled trial. Hum. Vaccines Immunother. 2021, 17, 5348–5354. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Chang, S.; Wang, R.; Xiao, Y.; Li, F.; Xu, Q.; Zhang, S.; Chen, X.; Zhang, S.; Zhang, M.; et al. Immunogenicity and Safety of an Inactivated Enterovirus 71 Vaccine Administered Simultaneously with Hepatitis B Virus Vaccine, Group A Meningococcal Polysaccharide Vaccine, Measles-Rubella Combined Vaccine and Japanese Encephalitis Vaccine: A Multi-Center, Randomized, Controlled Clinical Trial in China. Vaccines 2022, 10, 895. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Liao, Y.; Li, Y.; Jiang, G.; Huang, Z.; Yang, H.; Ou, Z.; Yin, Q.; Chen, J.; Deng, Y.; et al. Immunogenicity and safety of the inactivated enterovirus 71 vaccine administered concomitantly with the measles-rubella vaccine in infants aged 8 months in China: A noninferiority randomized controlled trial. Vaccine 2022, 40, 4709–4715. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.F.; Deng, P.; Guo, X.; Zheng, N.C.; Li, Q.; Qian, X.A.; Wang, Z.; Huang, J.F.; Chen, H.P.; Shi, X.W.; et al. Immunogenicity and safety of a licensed Chinese thimerosal-free trivalent split influenza virus vaccine. Chin. J. Vaccines Immun. 2019, 25, 180–183, 214. [Google Scholar]
- Wang, Z.G.; Sun, X.; Zhang, M.; Tang, F.Y.; Ma, F.B.; Xu, Y.; Hu, R.; Ma, Y.L.; Xiao, Y.L.; Chen, H.P.; et al. Immunogenicity and safety of co-immunization with 23-valent pneumococcal polysaccharide vaccine and influenza virus split vaccine for children aged 3–7 years. Chin. J. Microbiol. Immunol. 2019, 39, 758–762. [Google Scholar] [CrossRef]


{kind=link}
| Simultaneous Vaccination Group (n = 126) | EV71 Group (n = 126) | IIV3 Group (n = 126) | p | |
|---|---|---|---|---|
| Total, n (%) | 31.75 | 28.57 | 34.13 | 0.635 |
| Systemic, n (%) | 30.95 | 27.78 | 32.54 | 0.705 |
| Fever | 16.67 | 15.87 | 12.70 | 0.648 |
| Rash | 5.56 | 3.97 | 1.59 | 0.244 |
| Diarrhea | 3.17 | 1.59 | 3.97 | 0.519 |
| Vomiting | 0.79 | 0.79 | 0.79 | 1.000 |
| Unsolicited | 11.11 | 11.11 | 16.67 | 0.317 |
| Local, n (%) | 1.59 | 0.79 | 3.17 | 0.514 |
| Induration | 0.79 | 0.79 | 2.38 | 0.626 |
| Unsolicited | 0.79 | 0.00 | 0.79 | 1.000 |
| Simultaneous Vaccination Group (n = 115) | EV71 Group (n = 114) | p | |
|---|---|---|---|
| Pre-vaccination | |||
| Seropositive Rate (95% CI) | 33.04 (24.56~42.43) | 35.09 (26.38~44.59) | 0.744 |
| GMT (95% CI) | 6.04 (5.13~7.10) | 6.40 (5.25~7.79) | 0.892 |
| Post-vaccination | |||
| Seropositive Rate (95% CI) | 100.00 (96.84~100.00) | 100.00 (96.82~100.00) | 1.000 |
| Seroconversion Rate (95% CI) | 98.26 (93.86~99.79) | 97.37 (92.50~99.45) | 0.643 |
| GMT (95% CI) | 414.25 (333.72~514.23) | 514.84 (416.17~636.88) | 0.157 |
| Simultaneous Vaccination Group (n = 115) | IIV3 Group (n = 121) | p | |
|---|---|---|---|
| H1N1 | |||
| Pre-vaccination | |||
| Seropositive Rate (95% CI) | 5.22 (1.94~11.01) | 3.31 (0.91~8.25) | 0.465 |
| GMT (95% CI) | 5.31 (5.04~5.60) | 5.17 (5.00~5.36) | 0.464 |
| Post-vaccination | |||
| Seroprotection Rate (95% CI) | 80.87 (72.48~87.61) | 86.78 (79.42~92.25) | 0.217 |
| Seroconversion Rate (95% CI) | 80.00 (71.52~86.88) | 86.78 (79.42~92.25) | 0.161 |
| GMT (95% CI) | 79.52 (64.88~97.46) | 88.69 (73.54~106.96) | 0.513 |
| H3N2 | |||
| Pre-vaccination | |||
| Seropositive Rate (95% CI) | 4.35 (1.43~9.85) | 9.92 (5.23~16.68) | 0.098 |
| GMT (95% CI) | 5.18 (5.02~5.36) | 5.39 (5.17~5.62) | 0.102 |
| Post-vaccination | |||
| Seroprotection Rate (95% CI) | 99.13 (95.25~99.98) | 98.35 (94.16~99.80) | 0.587 |
| Seroconversion Rate (95% CI) | 99.13 (95.25~99.98) | 98.35 (94.16~99.80) | 0.587 |
| GMT (95% CI) | 142.69 (125.92~161.69) | 125.79 (110.35~ 143.38) | 0.133 |
| B | |||
| Pre-vaccination | |||
| Seropositive Rate (95% CI) | 1.74 (0.21~6.14) | 2.48 (0.51~7.07) | 0.692 |
| GMT (95% CI) | 5.06 (4.98~5.15) | 5.09 (4.99~5.19) | 0.694 |
| Post-vaccination | |||
| Seroprotection Rate (95% CI) | 76.52 (67.71~83.92) | 80.99 (72.86~87.55) | 0.401 |
| Seroconversion Rate (95% CI) | 76.52 (67.71~83.92) | 80.99 (72.86~87.55) | 0.401 |
| GMT (95% CI) | 49.10 (42.30~56.98) | 48.88 (42.37~ 56.39) | 0.966 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, Y.; Guo, X.; Zhang, M.; Chen, Y.; Zhang, Y.; Yu, X.; Luo, L.; Chen, H.; Xu, W.; Liu, H.; et al. Safety and Immunogenicity of Enterovirus 71 Vaccine (Vero Cell) Administered Simultaneously with Trivalent Split-Virion Influenza Vaccine in Infants Aged 6–7 Months: A Phase 4, Randomized, Controlled Trial. Vaccines 2023, 11, 862. https://doi.org/10.3390/vaccines11040862
Xiao Y, Guo X, Zhang M, Chen Y, Zhang Y, Yu X, Luo L, Chen H, Xu W, Liu H, et al. Safety and Immunogenicity of Enterovirus 71 Vaccine (Vero Cell) Administered Simultaneously with Trivalent Split-Virion Influenza Vaccine in Infants Aged 6–7 Months: A Phase 4, Randomized, Controlled Trial. Vaccines. 2023; 11(4):862. https://doi.org/10.3390/vaccines11040862
Chicago/Turabian StyleXiao, Yanhui, Xue Guo, Min Zhang, Yaping Chen, Yanyang Zhang, Xiaoqing Yu, Linyun Luo, Haiping Chen, Weichai Xu, Haibo Liu, and et al. 2023. "Safety and Immunogenicity of Enterovirus 71 Vaccine (Vero Cell) Administered Simultaneously with Trivalent Split-Virion Influenza Vaccine in Infants Aged 6–7 Months: A Phase 4, Randomized, Controlled Trial" Vaccines 11, no. 4: 862. https://doi.org/10.3390/vaccines11040862
APA StyleXiao, Y., Guo, X., Zhang, M., Chen, Y., Zhang, Y., Yu, X., Luo, L., Chen, H., Xu, W., Liu, H., Wu, L., Hou, R., Ma, Y., Long, L., Ruan, J., Chen, W., & Yang, X. (2023). Safety and Immunogenicity of Enterovirus 71 Vaccine (Vero Cell) Administered Simultaneously with Trivalent Split-Virion Influenza Vaccine in Infants Aged 6–7 Months: A Phase 4, Randomized, Controlled Trial. Vaccines, 11(4), 862. https://doi.org/10.3390/vaccines11040862