
The Impact of Vaccination on COVID-19 Burden of Disease in the Adult and Elderly Population: A Systematic Review of Italian Evidence
 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
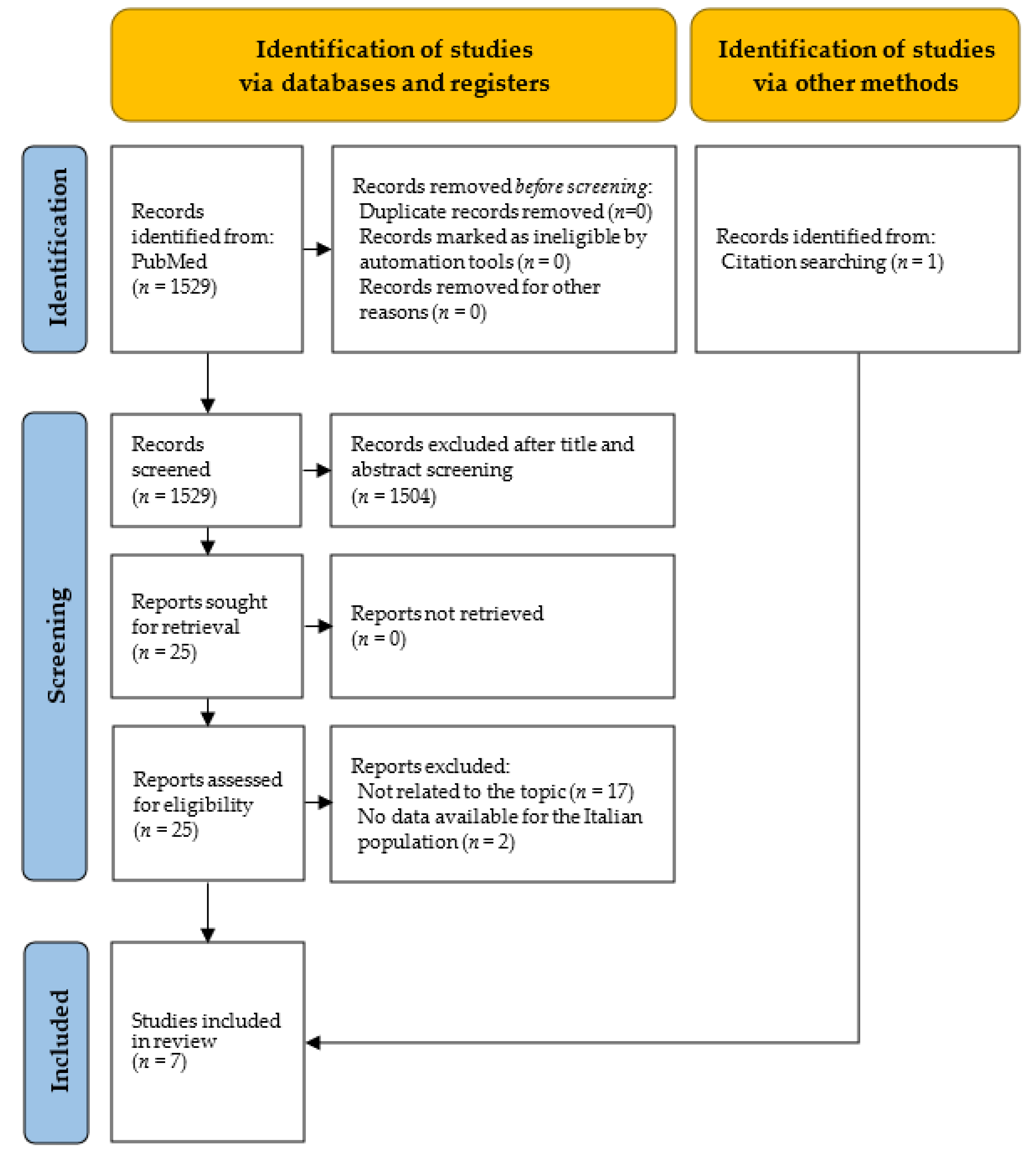
2.3. Selection Process and Data Extraction
Data Synthesis
3. Results
3.1. Effects of Vaccination on COVID-19-Related Mortality
3.1.1. Characteristics of Studies Included in the Systematic Review on COVID-19 Mortality
3.1.2. Results of Studies Included in the Systematic Review on COVID-19 Mortality
3.2. Effects of Vaccination on COVID-19-Related Complications
3.2.1. Characteristics of Studies Included in the Systematic Review on COVID-19 Complications
3.2.2. Results of Studies Included in the Systematic Review on COVID-19 Complications
3.2.3. Hospitalizations for COVID-19
3.2.4. Post-COVID-19 Syndrome
4. Discussion
- A reduction in the risk for COVID-19-related death in subjects who were fully vaccinated and/or had received a booster when compared to unvaccinated or partially vaccinated subjects;
- A reduction in hospitalizations and ICU admissions for COVID-19 in subjects who were fully vaccinated and/or had received a booster dose when compared to unvaccinated or partially vaccinated subjects;
- A reduction in the clinical severity of COVID-19 in subjects who were fully vaccinated and/or had received a booster dose when compared to unvaccinated or partially vaccinated subjects.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rovetta, A.; Bhagavathula, A.S. The Impact of COVID-19 on Mortality in Italy: Retrospective Analysis of Epidemiological Trends. JMIR Public Health Surveill. 2022, 8, e36022. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO) Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 15 December 2022).
- Chavda, V.P.; Vuppu, S.; Mishra, T.; Kamaraj, S.; Patel, A.B.; Sharma, N.; Chen, Z.-S. Recent Review of COVID-19 Management: Diagnosis, Treatment and Vaccination. Pharmacol. Rep. 2022, 74, 1120–1148. [Google Scholar] [CrossRef] [PubMed]
- Monpara, J.D.; Sodha, S.J.; Gupta, P.K. COVID-19 Associated Complications and Potential Therapeutic Targets. Eur. J. Pharmacol. 2020, 886, 173548. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Dong, X.; Liu, G.; Gao, Y. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2022, 64, 90–107. [Google Scholar] [CrossRef] [PubMed]
- Orsi, C.; De Rocchi, D.; Cinque, S.; Crialesi, R.; Della Mea, V.; Luisa, F.; Grande, E.; Marchetti, S.; Navarra, S.; Pappagallo, M.; et al. Analysing Complications of COVID-19 from Death Certificates: Which Ones Kill Most? Riv. Stat. Uff. 2021, 1, 59–82. [Google Scholar]
- Parodi, S.M.; Liu, V.X. From Containment to Mitigation of COVID-19 in the US. JAMA 2020, 323, 1441. [Google Scholar] [CrossRef]
- Mattiuzzi, C.; Lippi, G. Primary COVID-19 Vaccine Cycle and Booster Doses Efficacy: Analysis of Italian Nationwide Vaccination Campaign. Eur. J. Public Health 2022, 32, 328–330. [Google Scholar] [CrossRef]
- Bollyky, T.J.; Gostin, L.O.; Hamburg, M.A. The Equitable Distribution of COVID-19 Therapeutics and Vaccines. JAMA 2020, 323, 2462. [Google Scholar] [CrossRef]
- Mohseni Afshar, Z.; Barary, M.; Hosseinzadeh, R.; Karim, B.; Ebrahimpour, S.; Nazary, K.; Sio, T.T.; Sullman, M.J.M.; Carson-Chahhoud, K.; Moudi, E.; et al. COVID-19 Vaccination Challenges: A Mini-Review. Hum. Vaccines Immunother. 2022, 18, 2066425. [Google Scholar] [CrossRef]
- Talic, S.; Shah, S.; Wild, H.; Gasevic, D.; Maharaj, A.; Ademi, Z.; Li, X.; Xu, W.; Mesa-Eguiagaray, I.; Rostron, J.; et al. Effectiveness of Public Health Measures in Reducing the Incidence of COVID-19, SARS-CoV-2 Transmission, and COVID-19 Mortality: Systematic Review and Meta-Analysis. BMJ 2021, 375, e068302. [Google Scholar] [CrossRef]
- Sharif, N.; Alzahrani, K.J.; Ahmed, S.N.; Dey, S.K. Efficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 714170. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Tessier, E.; Stowe, J.; Gower, C.; Kirsebom, F.; Simmons, R.; Gallagher, E.; Thelwall, S.; Groves, N.; Dabrera, G.; et al. Duration of Protection against Mild and Severe Disease by COVID-19 Vaccines. N. Engl. J. Med. 2022, 386, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, K.; Shavaleh, R.; Forouhi, M.; Disfani, H.F.; Kamandi, M.; Oskooi, R.K.; Foogerdi, M.; Soltani, M.; Rahchamani, M.; Mohaddespour, M.; et al. The Effectiveness of COVID-19 Vaccines in Reducing the Incidence, Hospitalization, and Mortality from COVID-19: A Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 873596. [Google Scholar] [CrossRef] [PubMed]
- Ssentongo, P.; Ssentongo, A.E.; Voleti, N.; Groff, D.; Sun, A.; Ba, D.M.; Nunez, J.; Parent, L.J.; Chinchilli, V.M.; Paules, C.I. SARS-CoV-2 Vaccine Effectiveness against Infection, Symptomatic and Severe COVID-19: A Systematic Review and Meta-Analysis. BMC Infect. Dis. 2022, 22, 439. [Google Scholar] [CrossRef]
- Rudan, I.; Adeloye, D.; Sheikh, A. COVID-19: Vaccines, Efficacy and Effects on Variants. Curr. Opin. Pulm. Med. 2022, 28, 180–191. [Google Scholar] [CrossRef]
- Homan, T.; Mazzilli, S.; Chieti, A.; Musa, A.; Roth, A.; Fortunato, F.; Bisceglia, L.; Prato, R.; Lopalco, P.L.; Martinelli, D. COVID-19 Vaccination Programme Effectiveness against SARS-CoV-2 Related Infections, Hospital Admissions and Deaths in the Apulia Region of Italy: A One-Year Retrospective Cohort Study. Sci. Rep. 2022, 12, 18597. [Google Scholar] [CrossRef]
- World Health Organization (WHO) COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 15 December 2022).
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.R.W.; Pollard, A.J. What Defines an Efficacious COVID-19 Vaccine? A Review of the Challenges Assessing the Clinical Efficacy of Vaccines against SARS-CoV-2. Lancet Infect. Dis. 2021, 21, e26–e35. [Google Scholar] [CrossRef]
- Maruotti, A.; Jona-Lasinio, G.; Divino, F.; Lovison, G.; Ciccozzi, M.; Farcomeni, A. Estimating COVID-19-Induced Excess Mortality in Lombardy, Italy. Aging Clin. Exp. Res. 2022, 34, 475–479. [Google Scholar] [CrossRef]
- Marcellusi, A.; Fabiano, G.; Sciattella, P.; Andreoni, M.; Mennini, F.S. The Impact of COVID-19 Vaccination on the Italian Healthcare System: A Scenario Analysis. Clin. Drug Investig. 2022, 42, 237–242. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F.; Henry, B.M. Coronavirus Disease 2019 (COVID-19): The Portrait of a Perfect Storm. Ann. Transl. Med. 2020, 8, 497. [Google Scholar] [CrossRef]
- Circolare Ministero della Salute n. 42164 del 24 December 2020. Available online: https://www.certifico.com/news/274-news/12430-circolare-ministero-della-salute-n-42164-del-24-dicembre-2020 (accessed on 15 December 2022).
- Salute, M. Della Campagna di Vaccinazione Anti COVID-19. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5452&area=nuovoCoronavirus&menu=vuoto (accessed on 12 May 2023).
- Salute, M. Della Piano e Norme Attuative—Campagna di Vaccinazione Anti COVID-19. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5452&area=nuovoCoronavirus&menu=vuoto&tab=1 (accessed on 12 May 2023).
- Gazzetta Ufficiale. Available online: https://www.gazzettaufficiale.it/eli/id/2021/06/17/21A03739/sg (accessed on 12 May 2023).
- Gazzetta Ufficiale DL 24/2022. Available online: https://www.gazzettaufficiale.it/eli/id/2022/03/24/22G00034/s (accessed on 3 May 2022).
- Salute, M. Della Vaccini COVID-19, via Libera alla Terza Dose (Booster) per Over 60 e Fragili. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioComunicatiNuovoCoronavirus.jsp?lingua=italiano&id=5835 (accessed on 12 May 2023).
- EpiCentro Piano Nazionale di Vaccinazione COVID-19. Available online: https://www.epicentro.iss.it/vaccini/covid-19-piano-vaccinazione (accessed on 10 May 2023).
- Agenzia Italiana del Farmaco Farmacovigilanza su Vaccini COVID-19. Available online: https://aifa.gov.it/farmacovigilanza-vaccini-covid-19 (accessed on 21 December 2022).
- Governo Italiano Report Vaccini Anti COVID-19. Available online: https://www.governo.it/it/cscovid19/report-vaccini/ (accessed on 21 December 2022).
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-World Effectiveness of COVID-19 Vaccines: A Literature Review and Meta-Analysis. Int. J. Infect. Dis. 2022, 114, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Monto, A.S. The Future of SARS-CoV-2 Vaccination—Lessons from Influenza. N. Engl. J. Med. 2021, 385, 1825–1827. [Google Scholar] [CrossRef] [PubMed]
- Mattiuzzi, C.; Lippi, G. Efficacy of the Second COVID-19 Vaccine Booster Dose in the Elderly. Vaccines 2023, 11, 213. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.-L.; Kuo, H.-S.; Ho, H.J.; Wu, C.-Y. COVID-19 Vaccinations Are Associated with Reduced Fatality Rates: Evidence from Cross-County Quasi-Experiments. J. Glob. Health 2021, 11, 05019. [Google Scholar] [CrossRef]
- Sacco, C.; Mateo Urdiales, A.; Rota, M.; Fabiani, M.; Petrone, D.; Boros, S.; Bressi, M.; Vescio, M.F.; Siddu, A.; Battilomo, S.; et al. Infezioni Da SARS-CoV-2, Ricoveri e Decessi Associati a COVID-19 Direttamente Evitati Dalla Vaccinazione, Italia, 27 December 2020—31 January 2022; Istituto Superiore di Sanità (ISS): Rome, Italy, 2022. [Google Scholar]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef]
- Nunes, B.; Rodrigues, A.P.; Kislaya, I.; Cruz, C.; Peralta-Santos, A.; Lima, J.; Pinto Leite, P.; Sequeira, D.; Matias Dias, C.; Machado, A. MRNA Vaccine Effectiveness against COVID-19-Related Hospitalisations and Deaths in Older Adults: A Cohort Study Based on Data Linkage of National Health Registries in Portugal, February to August 2021. Euro Surveill. Bull. Eur. Sur Mal. Transm. Eur. Commun. Dis. Bull. 2021, 26, 2100833. [Google Scholar] [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; et al. Duration of Effectiveness of Vaccines against SARS-CoV-2 Infection and COVID-19 Disease: Results of a Systematic Review and Meta-Regression. Lancet Lond. Engl. 2022, 399, 924–944. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Rivasi, G.; Bulgaresi, M.; Mossello, E.; Buscemi, P.; Lorini, C.; Balzi, D.; Barucci, R.; Del Lungo, I.; Gangemi, S.; Giardini, S.; et al. Course and Lethality of SARS-CoV-2 Epidemic in Nursing Homes after Vaccination in Florence, Italy. Vaccines 2021, 9, 1174. [Google Scholar] [CrossRef]
- Mattiuzzi, C.; Lippi, G. Efficacy of COVID-19 Vaccine Booster Doses in Older People. Eur. Geriatr. Med. 2022, 13, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Pierobon, S.; Braggion, M.; Fedeli, U.; Nordio, M.; Basso, C.; Zorzi, M. Impact of Vaccination on the Spread of SARS-CoV-2 Infection in North-East Italy Nursing Homes. A Propensity Score and Risk Analysis. Age Ageing 2022, 51, afab224. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.G.; Murtas, R.; Tunesi, S.; Decarli, A.; Bergamaschi, W. Boosters and Time from the Last Anti-COVID-19 Vaccine Dose: Lead Public Health Choices by Real-Time Epidemiological Assessment. Epidemiol. Prev. 2022, 46, 34–46. [Google Scholar] [CrossRef]
- Sacco, C.; Mateo-Urdiales, A.; Petrone, D.; Spuri, M.; Fabiani, M.; Vescio, M.F.; Bressi, M.; Riccardo, F.; Manso, M.D.; Bella, A.; et al. Estimating Averted COVID-19 Cases, Hospitalisations, Intensive Care Unit Admissions and Deaths by COVID-19 Vaccination, Italy, January−September 2021. Eurosurveillance 2021, 26, 2101001. [Google Scholar] [CrossRef] [PubMed]
- Pastorino, R.; Pezzullo, A.M.; Villani, L.; Causio, F.A.; Axfors, C.; Contopoulos-Ioannidis, D.G.; Boccia, S.; Ioannidis, J.P.A. Change in Age Distribution of COVID-19 Deaths with the Introduction of COVID-19 Vaccination. Environ. Res. 2022, 204, 112342. [Google Scholar] [CrossRef] [PubMed]
- Rivasi, G.; Bulgaresi, M.; Bandinelli, C.; Balzi, D.; Tarantini, F.; Tognelli, S.; Lorini, C.; Buscemi, P.; Baggiani, L.; Landini, G.; et al. Long-Term Effects of SARS-CoV-2 Vaccination in the Nursing Home Setting. J. Am. Geriatr. Soc. 2022, 70, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Ripabelli, G.; Sammarco, M.L.; Rezza, G.; D’Amico, A.; De Dona, R.; Iafigliola, M.; Parente, A.; Samprati, N.; Santagata, A.; Adesso, C.; et al. A SARS-CoV-2 Outbreak Among Nursing Home Residents Vaccinated with a Booster Dose of MRNA COVID-19 Vaccine. J. Community Health 2022, 47, 598–603. [Google Scholar] [CrossRef]
- Peghin, M.; De Martino, M.; Palese, A.; Gerussi, V.; Bontempo, G.; Graziano, E.; Visintini, E.; D’Elia, D.; Dellai, F.; Marrella, F.; et al. Post–COVID-19 Syndrome and Humoral Response Association after 1 Year in Vaccinated and Unvaccinated Patients. Clin. Microbiol. Infect. 2022, 28, 1140–1148. [Google Scholar] [CrossRef]
- Lorenzoni, G.; Rosi, P.; De Rosa, S.; Ranieri, V.M.; Navalesi, P.; Gregori, D. COVID-19 VENETO ICU Network COVID-19 Vaccination Status Among Adults Admitted to Intensive Care Units in Veneto, Italy. JAMA Netw. Open 2022, 5, e2213553. [Google Scholar] [CrossRef]
- Wang, Z.; Schmidt, F.; Weisblum, Y.; Muecksch, F.; Barnes, C.O.; Finkin, S.; Schaefer-Babajew, D.; Cipolla, M.; Gaebler, C.; Lieberman, J.A.; et al. MRNA Vaccine-Elicited Antibodies to SARS-CoV-2 and Circulating Variants. Nature 2021, 592, 616–622. [Google Scholar] [CrossRef]
- Saadat, S.; Rikhtegaran Tehrani, Z.; Logue, J.; Newman, M.; Frieman, M.B.; Harris, A.D.; Sajadi, M.M. Binding and Neutralization Antibody Titers After a Single Vaccine Dose in Health Care Workers Previously Infected With SARS-CoV-2. JAMA 2021, 325, 1467–1469. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.R.; Painter, M.M.; Apostolidis, S.A.; Mathew, D.; Meng, W.; Rosenfeld, A.M.; Lundgreen, K.A.; Reynaldi, A.; Khoury, D.S.; Pattekar, A.; et al. MRNA Vaccines Induce Durable Immune Memory to SARS-CoV-2 and Variants of Concern. Science 2021, 374, abm0829. [Google Scholar] [CrossRef] [PubMed]
- Meslé, M.M.; Brown, J.; Mook, P.; Hagan, J.; Pastore, R.; Bundle, N.; Spiteri, G.; Ravasi, G.; Nicolay, N.; Andrews, N.; et al. Estimated Number of Deaths Directly Averted in People 60 Years and Older as a Result of COVID-19 Vaccination in the WHO European Region, December 2020 to November 2021. Eurosurveillance 2021, 26, 2101021. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Botero, M.L.; Fernández-Niño, J.A.; Arregocés-Castillo, L.; Ruiz-Gómez, F. Estimated Number of Deaths Directly Avoided Because of COVID-19 Vaccination among Older Adults in Colombia in 2021: An Ecological, Longitudinal Observational Study. F1000Research 2022, 11, 198. [Google Scholar] [CrossRef] [PubMed]
- Haas, E.J.; McLaughlin, J.M.; Khan, F.; Angulo, F.J.; Anis, E.; Lipsitch, M.; Singer, S.R.; Mircus, G.; Brooks, N.; Smaja, M.; et al. Infections, Hospitalisations, and Deaths Averted via a Nationwide Vaccination Campaign Using the Pfizer–BioNTech BNT162b2 MRNA COVID-19 Vaccine in Israel: A Retrospective Surveillance Study. Lancet Infect. Dis. 2022, 22, 357–366. [Google Scholar] [CrossRef]
- Goldstein, J.R.; Cassidy, T.; Wachter, K.W. Vaccinating the Oldest against COVID-19 Saves Both the Most Lives and Most Years of Life. Proc. Natl. Acad. Sci. USA 2021, 118, e2026322118. [Google Scholar] [CrossRef]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and Effectiveness of MRNA BNT162b2 Vaccine against SARS-CoV-2 Infections and COVID-19 Cases, Hospitalisations, and Deaths Following a Nationwide Vaccination Campaign in Israel: An Observational Study Using National Surveillance Data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a Third Dose of the BNT162b2 MRNA COVID-19 Vaccine for Preventing Severe Outcomes in Israel: An Observational Study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 MRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection against COVID-19 by BNT162b2 Booster across Age Groups. N. Engl. J. Med. 2021, 385, 2421–2430. [Google Scholar] [CrossRef]
- Nordström, P.; Ballin, M.; Nordström, A. Risk of Infection, Hospitalisation, and Death up to 9 Months after a Second Dose of COVID-19 Vaccine: A Retrospective, Total Population Cohort Study in Sweden. Lancet 2022, 399, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.G. Effectiveness of a Third Dose of MRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 139–145. [Google Scholar] [CrossRef]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Clinical Severity of, and Effectiveness of MRNA Vaccines against, COVID-19 from Omicron, Delta, and Alpha SARS-CoV-2 Variants in the United States: Prospective Observational Study. BMJ 2022, 376, e069761. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W. Sustained Effectiveness of Pfizer-BioNTech and Moderna Vaccines Against COVID-19 Associated Hospitalizations Among Adults—United States, March–July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1156–1162. [Google Scholar] [CrossRef]
- Vasileiou, E.; Simpson, C.R.; Shi, T.; Kerr, S.; Agrawal, U.; Akbari, A.; Bedston, S.; Beggs, J.; Bradley, D.; Chuter, A.; et al. Interim Findings from First-Dose Mass COVID-19 Vaccination Roll-out and COVID-19 Hospital Admissions in Scotland: A National Prospective Cohort Study. Lancet 2021, 397, 1646–1657. [Google Scholar] [CrossRef] [PubMed]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of MRNA BNT162b2 COVID-19 Vaccine up to 6 Months in a Large Integrated Health System in the USA: A Retrospective Cohort Study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association Between MRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043–2054. [Google Scholar] [CrossRef]
- Ng, O.T.; Marimuthu, K.; Lim, N.; Lim, Z.Q.; Thevasagayam, N.M.; Koh, V.; Chiew, C.J.; Ma, S.; Koh, M.; Low, P.Y.; et al. Analysis of COVID-19 Incidence and Severity Among Adults Vaccinated With 2-Dose MRNA COVID-19 or Inactivated SARS-CoV-2 Vaccines with and Without Boosters in Singapore. JAMA Netw. Open 2022, 5, e2228900. [Google Scholar] [CrossRef]
- Chodick, G.; Tene, L.; Patalon, T.; Gazit, S.; Tov, A.B.; Cohen, D.; Muhsen, K. The Effectiveness of the First Dose of BNT162b2 Vaccine in Reducing SARS-CoV-2 Infection 13–24 Days after Immunization: Real-World Evidence. JAMA Netw. Open 2021, 4, e2115985. [Google Scholar] [CrossRef]
- Widge, A.T.; Rouphael, N.G.; Jackson, L.A.; Anderson, E.J.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Durability of Responses after SARS-CoV-2 MRNA-1273 Vaccination. N. Engl. J. Med. 2021, 384, 80–82. [Google Scholar] [CrossRef]
- Ayoubkhani, D.; Bermingham, C.; Pouwels, K.B.; Glickman, M.; Nafilyan, V.; Zaccardi, F.; Khunti, K.; Alwan, N.A.; Walker, A.S. Trajectory of Long Covid Symptoms after COVID-19 Vaccination: Community Based Cohort Study. BMJ 2022, 377, e069676. [Google Scholar] [CrossRef] [PubMed]
- Notarte, K.I.; Catahay, J.A.; Velasco, J.V.; Pastrana, A.; Ver, A.T.; Pangilinan, F.C.; Peligro, P.J.; Casimiro, M.; Guerrero, J.J.; Gellaco, M.M.L.; et al. Impact of COVID-19 Vaccination on the Risk of Developing Long-COVID and on Existing Long-COVID Symptoms: A Systematic Review. eClinicalMedicine 2022, 53, 101624. [Google Scholar] [CrossRef] [PubMed]
- de Waure, C.; Calabrò, G.E.; Ricciardi, W. Value(s) of Vaccination Project Steering Committee Recommendations to drive a value-based decision-making on vaccination. Expert Rev. Vaccines 2022, 21, 289–296. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Topic | Search String | Filters |
|---|---|---|
| Effects of vaccination on COVID-19-related mortality | (COVID-19 OR SARS-CoV-2) AND (mortality OR death OR lethal) AND Italy | English language, Adult: 19+ years |
| Effects of vaccination on COVID-19-related complications | (COVID-19 OR SARS-CoV-2) AND (complication OR sequelae OR hospitalization) AND Italy | English language, Adult: 19+ years |
| Author, Year, [Ref] | Location | Period | Study Design | Sample Characteristics | Study Aim | Vaccine Sources | Results on COVID-19-Related Mortality | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Rivasi G, 2021 [42] | Florence, Tuscany region | 1 October 2020–31 March 2021, I to III waves | Observational, retrospective | 3730 SARS-CoV-2-naïve NHs residents (mean age 84.2, 69% female) | Investigation of impact of vaccination on the course of the pandemic before and after vaccination | Comirnaty | Fully vaccinated subjects showed significantly lower mortality rates than those partially vaccinated and unvaccinated (6%, 18%, and 56%, respectively) *. The death risk was 84% and 96% lower in partially vaccinated subjects (HR 0.157, 95% CI: 0.049–0.491) and in fully vaccinated subjects (HR 0.037, 95% CI: 0.006–0.223) compared to those unvaccinated (HR 0.157, 95% CI: 0.049–0.491) * | Vaccination was followed by a marked decline in mortality among infected residents |
| Mattiuzzi C, 2022 [43] | Italy | 27 December 2020–27 November 2021, II to IV waves | Observational, retrospective | 4,487,526 Italian people ≥80 years old | Analysis of the effectiveness of booster doses in older people based on data retrieved from the ongoing nationwide Italian COVID-19 vaccination campaign | Comirnaty, Spikevax, Vaxzervria, Jcovden | An 81% and 98% lower risk ** of death in those who received booster doses compared, respectively, with those who completed the COVID-19 primary vaccination cycle or were unvaccinated | The administration of COVID-19 vaccine booster doses greatly reduced the risk of mortality |
| Pierobon S, 2022 [44] | Veneto region | I wave 21 February 2020–31 August 2020, II wave 31 August 2020–1 January 2021, III wave 1 January 2021–3 May 2021 | Observational, retrospective | 852,211 residents in the Veneto region aged between 70 and 100. 33,592 NH residents. After the 1:1 propensity score matching, the size of the two groups was equal to 31 922 cases | Analysis of the risk of hospitalization and death due to COVID-19 among NH residents in comparison with the general older population over time | N/A | During the first wave the RR in NH vs. not NH was 10.10 (95% CI: 8.17–12.47); in the second wave it was of 7.97 (95% CI: 7.17–8.87); in the third wave RR was of 0.48 (95% CI: 0.30–0.77). The overall RR was of 6.07 (95% CI: 5.58–6.61) | By the end of the COVID-19 vaccination program in NHs, the risk of death due to COVID-19 in NH residents was significantly reduced |
| Russo AG, 2022 [45] | Milano and Lodi, Lombardy region | 1 October 2021–31 December 2021, IV wave | Observational, retrospective | 2,936,193 ≥19-year-old residents in the provinces of Milan and Lodi | Evaluation of the efficacy of the booster dose in reducing severe SARS-CoV-2 infection in terms of hospital admissions, ICU admissions, and deaths from all causes | N/A | Boosted subjects had an HR of 0.33 (95% CI: 0.29–0.37) for death compared to unvaccinated subjects. HR values in vaccinated subjects for each vaccine dose varied as follows: 1 dose alone, HR 1.80 (95% CI: 1.56–2.09); 1 dose + COVID-19, HR 0.98 (95% CI: 0.82–1.16); 2 doses (<4 months), HR 0.31 (95% CI: 0.26–0.36); 2 doses (4–5 months), HR 0.53 (95% CI: 0.42–0.68); 2 doses (5–6 months), HR 0.57 (95% CI: 0.51–0.64); 2 doses (6–7 months), HR 1.47 (95% CI: 1.31–1.64); 2 doses (7+ months), HR 3.77 (95% CI: 3.52–4.03); 2 doses + COVID-19, HR 1.14 (95% CI: 0.96–1.36) | Two doses received in the previous 5 months and the booster dose significantly reduced the risk of death due to COVID-19 |
| Sacco C, 2021 [46] | Italy | 11 January 2021–30 September 2021, III to IV waves | Observational, retrospective | Italian people ≥12 years old | Estimation of the number of averted COVID-19 cases, hospitalizations, and deaths due to vaccination by age group, and geographical macroareas | Comirnaty, Spikevax, Vaxzervria, Jcovden | 22,067 averted deaths with vaccination (38% of expected). In particular, in the subjects ≥80 years old (71%), followed by subjects of 70–79 years old (18%), 60–69 years old (8%), and <60 years old (2%) | The largest proportion of deaths prevented by vaccination was observed in the oldest age group (≥80 years). Geographical areas that achieved high vaccination rates faster were able to prevent a larger number of deaths over the summer months. |
| Pastorino R, 2022 [47] | 40 countries | Pre vaccination 21 February 2020–27 December 2020. Vaccination 27 December 2020–30 May 2021 I to IV waves | Observational, retrospective | All countries that had a total of COVID-19 deaths >500 as of end of May 2021 | Analysis of the proportion of deaths in different age groups in vaccination versus control periods in different countries | N/A | The COVID-19 deaths in the 0–69 age group compared to the total were of 14% in entire prevaccination period, of 13% in the II wave prevaccination period, and of 16% in vaccination period, respectively | Data show that vaccination was associated with a marked change in the age distribution of COVID-19 deaths in the first 5 months of 2021 in countries that prioritized vaccination among older people, with a relative increase in the share of deaths among nonelderly people |
| Rivasi G, 2022 [48] | Florence, Tuscany region | 1 April 2021–31 October 2021, III to IV waves | Observational, perspective | 2271 NH residents (mean age 86.6, 74% female) | Investigation of the long-term impact of vaccination on lethality | Comirnaty | Lethality rate was 5% up to 6 months after the primary vaccination cycle and 8% during the following 3 months | Lethality rate was significant but lower than previously reported in unvaccinated residents of the study area |
| Author, Year, [Ref.] | Location | Period | Study Design | Sample Characteristics | Study Aim | Vaccine Sources | Results on COVID-19-Related Complications | Main Findings | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rivasi G, 2021 [42] | Florence, Tuscany region | 1 October 2020–26 December 2021 (prevaccination period), 27 December 2021–31 March 2021 (postvaccination period), I to III waves | Observational, retrospective | 3730 SARS-CoV-2-naïve NHs residents (mean age 84.2; 69% females) | Analysis of the impact of the BNT162b2 mRNA SARS-CoV-2 vaccine on the course of the epidemic in the NHs of the Florence Health District in Tuscany | Comirnaty | COVID-19 Severity * Out of a total of 100 subjects, those unvaccinated had absent or minimal symptoms, mild or severe forms, in 22%, 33% and 44% of cases respectively; the partially vaccinated subjects presented absent or minimal symptoms, mild or severe forms, in 45%, 39% and 16% of cases, respectively; fully vaccinated subjects had no or minimal symptoms, mild or severe forms, in 86%, 14% and 0% of cases, respectively. Hospitalizations ** Out of a total of 100 subjects, 33% of unvaccinated cases, 14% of partially vaccinated cases and 3% of fully vaccinated cases were hospitalized | SARS-CoV-2 vaccination was associated with lower morbidity among infected NH residents | ||||
| Mattiuzzi C, 2022 [43] | Italy | 27 December 2020–27 November 2021, II to IV waves | Observational, retrospective | 448,526 subjects ≥80-years old | Analysis of the effectiveness of COVID-19 vaccine booster doses in older people based on data retrieved from the ongoing nationwide Italian COVID-19 vaccination campaign | Comirnaty, Spikevax, Vaxzervria, Jcovden | Hospitalizations: -OR (95% CI) COVID-19-related hospitalizations of unvaccinated compared to Vaccinated (≥5 months), Vaccinated (<5 months), and Vaccinated with booster, was of 0.17 (0.16–0.19; p < 0.0019), 0.14 (0.13–0.15; p < 0.001), and 0.03 (0.02–0.04; p < 0.001), respectively. -OR (95% CI) COVID-19-related hospitalizations of Vaccinated (≥5 months) compared with Vaccinated (<5 months), and Vaccinated with booster, was of 0.80 (0.71–0.90; p < 0.001), and of 0.17 (0.14–0.21; p < 0.001), respectively. -OR (95% CI) COVID-19-related hospitalizations of Vaccinated (<5 months) compared with Vaccinated with booster, was of 0.21 (0.17–0.26; p < 0.001). ICU admissions: -OR (95% CI) COVID-19 related ICU admissions of unvaccinated compared to Vaccinated (≥5 months), Vaccinated (<5 months), and Vaccinated with booster, was of 0.10 (0.07–0.16; p < 0.001), 0.14 (0.10–0.21; p < 0.001), and 0.02 (0.01–0.04; p < 0.001) respectively. -OR (95% CI) COVID-19 related ICU admissions of Vaccinated (≥5 months) compared with Vaccinated (<5 months), and Vaccinated with booster, was of 1.41 (0.82–2.43; p = 0.210), and 0.18 (0.06–0.53; p < 0.001) respectively. -OR (95% CI) COVID-19 related ICU admissions of Vaccinated (<5 months) compared with Vaccinated with booster, was of 0.13 (0.04–0.37; p < 0.001). | The administration of COVID-19 vaccine booster doses is advisable for reducing the risk of morbidity and mortality in older people | ||||
| Pierobon S, 2022 [44] | Veneto region | I wave 21 February 2020–31 August 2020, II wave 31 August 2020–1 January 2021, III wave 1 January 2021–3 May 2021 | Observational, retrospective | 852,211 residents in the Veneto region aged between 70 and 100 years (33,592 NH residents and 818,619 non-NH residents). | Analysis of the risk of hospitalization and death due to COVID-19 among NH in comparison with the general older population over time | N/A | RRs of hospitalization for COVID-19 were the following, in I, II, and III wave: −4.89 (95% CI: 4.17–5.74), 2.50 (95% CI: 2.29–2.73) and 0.25 (95% CI: 0.16–0.38), respectively. | The probability of SARS-CoV-2 hospitalization among NH residents had dramatically decreased by the time the COVID-19 immunization campaign in NHs was complete, especially for severe forms of COVID-19 | ||||
| Russo AG, 2022 [45] | Milano and Lodi, Lombardy region | 1 October 2021–31 December 2021, IV wave | Observational, retrospective | 2,936,193 (≥19 years old) residents in the provinces of Milan and Lodi | Evaluation of the efficacy of the booster dose in reducing severe SARS-CoV-2 infection in terms of hospital admissions, ICU admissions, and deaths from all causes | N/A | HR (95% CI) (reference: unvaccinated) Hospitalizations ICU admissions | Unvaccinated subjects compared to those who received a booster have a 10-fold greater risk of being hospitalized and a 9-fold greater risk of being admitted to ICUs | ||||
| 1 dose alone | 1.34 | (1.15–1.56) | 0.28 | (0.10–0.76) | ||||||||
| 1 dose + COVID-19 | 0.07 | (0.04–0.12) | - | |||||||||
| 2 doses <4 months | 0.19 | (0.16–0.22) | 0.03 | (0.01–0.12) | ||||||||
| 2 doses (4–5 months) | 0.18 | (0.14–0.24) | 0.05 | (0.01–0.33) | ||||||||
| 2 doses (5–6 months) | 0.41 | (0.37–0.46) | 0.19 | (0.12–0.29) | ||||||||
| 2 doses (6–7 months) | 0.73 | (0.63–0.84) | 0.25 | (0.13–0.49) | ||||||||
| 2 doses 7+ months | 1.65 | (1.50–1.82) | 0.57 | (0.34–0.96) | ||||||||
| 2 doses + COVID-19 | 0.12 | (0.08–0.19) | 0.08 | (0.01–0.54) | ||||||||
| Booster dose | 0.10 | (0.08–0.12) | 0.11 | (0.03–0.35) | ||||||||
| Sacco C, 2021 [46] | Italy | 11 January 2021–30 September 2021, III to IV waves | Observational, retrospective | Italian people ≥12 years old | Estimation of the number of averted COVID-19 cases, hospitalizations, and deaths based on the effect of the vaccination campaign | Comirnaty, Spikevax, Vaxzervria, Jcovden | A total of 79,152 hospitalizations, and 9839 ICU admissions averted by the vaccination campaign. Averted events by age range and percentage (hospitalizations and ICU admissions, respectively) of the total averted events: -subjects <60 years: 23%; 18% -subjects 60–69 years: 17%; 29% -subjects 70–79 years: 19%; 30% -subjects ≥80 years: 41%, 23% | Findings show a positive impact of the COVID-19 vaccination program in Italy and suggest that the rapid vaccination of high-risk groups has prevented a considerable number of severe COVID-19 outcomes | ||||
| Rivasi G, 2022 [48] | Florence, Tuscany region | 1 April 2021–31 October 2021, III to IV waves | Observational, prospective | 2271 vaccinated (primary cycle) NH residents (mean age 86.6; 74% females) | Analysis of the long-term impact of BNT162b2 SARS-CoV-2 vaccine on breakthrough infection rates in the NHs of Florence, Italy | Comirnaty | COVID-19 severity Absent/minimal 58% Mild/moderate 25% Severe 17% 8 hospitalizations (8%) (2 on 1 April–31 July and 6 on 1 August–31 October) | Hospitalizations remained stable up to nine months following primary vaccination course | ||||
| Ripabelli G, 2022 [49] | Molise region | 18 October 2021–2 November 2021, IV wave | Observational, prospective | 87 subjects (71 NH residents (median age 89; 73% females) and 16 HCWs (median age 52.5; 93.75% females)) | Description of the impact of vaccination in terms of hospitalizations during the SARS-CoV-2 outbreak caused by the Delta (B.1.617.2) variant | Comirnaty, Spikevax | 38 infected (44%), 3 hospitalizations (3% of the subjects, 8% of the infected, 4% of the residents, 0% of the HCWs), 0 ICU admissions (0%) | A booster dose of mRNA vaccine resulted in high protection against severe disease and hospitalization | ||||
| Peghin M, 2022 [50] | Udine, Friuli Venezia Giulia region | COVID-19 diagnosis 1 March 2020–31 May 2020 Follow-up at 12 months 1 March 2021–31 May 2021 I wave and III wave | Observational, prospective | At 12 months, 479 patients (53% females), 132 vaccinated with primary cycle (71% females) and 347 unvaccinated (46% females) | Description of the impact of vaccination and the role of humoral responses on post-COVID-19 syndrome 1 year after the onset of SARS-CoV-2 | Comirnaty, Spikevax, Vaxzervria, Jcovden | Acute COVID-19 severity * in overall, vaccinated, and unvaccinated subjects, respectively: -Asymptomatic: 8.0%, 14.4%, 5.5%; -Mild: 67.7%, 65.1%, 68.7%; -Severe/critical: 24.3%, 20.5%, 25.8% COVID-19 management in overall, vaccinated, and unvaccinated subjects, respectively: -Outpatient: 71.0%, 75.0%, 69.4%; -Inpatient ward: 24.6%, 22.7%, 25.4%; -Inpatient ICU: 4.4%, 2.3%, 5.2%. Post-COVID-19 syndrome at 6 months in overall, vaccinated, and unvaccinated subjects, respectively: -42.0%, 33.3%, 45.2% Post-COVID-19 symptoms at 12 months compared with post-COVID-19 symptoms at 6 months in Vaccinated and Unvaccinated subjects, respectively: -Unaffected + unchanged: 65.9%, 71.2%; -Worsened: 22.7%, 15.8%; -Improved: 11.4%, 13.0% | Post-COVID-19 syndrome rates are high up to 1 year after acute infection, and receiving the SARS-CoV-2 vaccine is not associated with worsening post-COVID-19 symptoms | ||||
| Lorenzoni G, 2022 [51] | Veneto region (San Donà di Piave e Jesolo, Ca’ Foncello, Belluno, Dell’Angelo hospital, ULSS 6 Euganea) | May 2021–December 2021, III to IV waves | Observational, retrospective | 748 patients (mean age 62 years, 138 (18%) vaccinated (≥2 doses), 58 (8%) partially vaccinated (1 dose), 552 (74%) not vaccinated) | Analysis and comparison of ICU admissions for COVID-19-associated acute respiratory distress syndrome in vaccinated and unvaccinated subjects | N/A | The median time from vaccine administration to ICU admission was **: 22.5 days (IQR, 16.0–49.8 days) for partially vaccinated; 159.0 days (IQR, 112.0–192.0 days) for fully vaccinated. The median time from vaccine administration to hospital admission was **: 16.0 days (IQR, 11.0–32.5 days) for partially vaccinated; 154.0 days (IQR, 110.0–190.0 days) for fully vaccinated. | Vaccinated patients received the second dose of vaccine a median of 5 months before admission to the ICU, whereas for partially vaccinated patients, the median ICU admission time occurred while they awaited the second dose | ||||
| Article and Study Period | Administered Vaccines | Vaccination Status | Absent/Minimal | Mild | Severe/Critical |
|---|---|---|---|---|---|
| Rivasi G, 2022 [48] 1 April 2021–31 October 2021 | Comirnaty | FV | 58% | 25% | 17% |
| Rivasi G, 2021 [42] 1 October 2020–31 March 2021 | FV | 86% | 14% | 0% | |
| Comirnaty | PV | 45% | 39% | 16% | |
| UV | 22% | 33% | 44% | ||
| Peghin M, 2022 [50] 1 March 2020–31 May 2020 | Comirnaty, Spikevax, Vaxzervria, Jcovden | FV | 14% | 65% | 21% |
| UV | 6% | 69% | 26% |
| Age | COVID-19 Cases | Hospitalizations | ICU Admissions |
|---|---|---|---|
| <60 1 | 62.7% | 23.3% | 18.1% |
| 60–69 | 12.0% | 16.6% | 28.6% |
| 70–79 | 9.2% | 19.2% | 30.2% |
| ≥80 | 15.9% | 40.7% | 22.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calabrò, G.E.; Pappalardo, C.; D’Ambrosio, F.; Vece, M.; Lupi, C.; Lontano, A.; Di Russo, M.; Ricciardi, R.; de Waure, C. The Impact of Vaccination on COVID-19 Burden of Disease in the Adult and Elderly Population: A Systematic Review of Italian Evidence. Vaccines 2023, 11, 1011. https://doi.org/10.3390/vaccines11051011
Calabrò GE, Pappalardo C, D’Ambrosio F, Vece M, Lupi C, Lontano A, Di Russo M, Ricciardi R, de Waure C. The Impact of Vaccination on COVID-19 Burden of Disease in the Adult and Elderly Population: A Systematic Review of Italian Evidence. Vaccines. 2023; 11(5):1011. https://doi.org/10.3390/vaccines11051011
Chicago/Turabian StyleCalabrò, Giovanna Elisa, Ciro Pappalardo, Floriana D’Ambrosio, Michele Vece, Chiara Lupi, Alberto Lontano, Mattia Di Russo, Roberto Ricciardi, and Chiara de Waure. 2023. "The Impact of Vaccination on COVID-19 Burden of Disease in the Adult and Elderly Population: A Systematic Review of Italian Evidence" Vaccines 11, no. 5: 1011. https://doi.org/10.3390/vaccines11051011
APA StyleCalabrò, G. E., Pappalardo, C., D’Ambrosio, F., Vece, M., Lupi, C., Lontano, A., Di Russo, M., Ricciardi, R., & de Waure, C. (2023). The Impact of Vaccination on COVID-19 Burden of Disease in the Adult and Elderly Population: A Systematic Review of Italian Evidence. Vaccines, 11(5), 1011. https://doi.org/10.3390/vaccines11051011