
Correlates of Parental Consent to Human Papillomavirus Vaccine Uptake by Their Adolescent Daughters in ZAMBIA: Application of the Health Belief Model
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Sampling and Sample Size Considerations
2.3. Data Collection and Variables
2.4. Data Management and Analysis
3. Results
3.1. HPV and HIV-Related Characteristics
3.2. Correlates of Parental Consent to Vaccinate Daughter
3.3. Mediation Effect of Knowledge on Parental Consent for HPV Vaccination
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baisley, K.J.; Andreasen, A.; Irani, J.; Nnko, S.; Changalucha, J.; Crucitti, T.; Francis, S.; Hansen, C.H.; Hayes, R.J.; Buvé, A.; et al. HPV prevalence around the time of sexual debut in adolescent girls in Tanzania. Sex. Transm. Infect. 2020, 96, 211–219. [Google Scholar] [CrossRef]
- Bruni, L.; Diaz, M.; Castellsagué, X.; Ferrer, E.; Bosch, F.X.; de Sanjosé, S. Cervical human papillomavirus prevalence in 5 continents: Meta-analysis of 1 million women with normal cytological findings. J. Infect. Dis. 2010, 202, 1789–1799. [Google Scholar] [CrossRef]
- World Health Organization. Weekly Epidemiological Record; World Health Organization: Geneva, Switerland, 2009; Volume 84, pp. 117–132.
- UNICEF. Human Papillomavirus Vaccine: Supply and Demand Update. October 2022 [Cited 22 August 2022]. Available online: https://www.unicef.org/supply/reports/human-papillomavirus-hpv-vaccine-supply-and-demand-update2020 (accessed on 25 August 2022).
- Basu, M. All about Serum Institute’s HPV Vaccine, India’s 1st Indigenous Shot Against Cervical Cancer India. The Print. 2022. Available online: https://theprint.in/health/all-about-serum-institutes-hpv-vaccine-indias-1st-indigenous-shot-against-cervical-cancer/1037054/ (accessed on 30 July 2022).
- Drolet, M.; Bénard, É.; Pérez, N.; Brisson, M. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: Updated systematic review and meta-analysis. Lancet 2019, 394, 497–509. [Google Scholar] [CrossRef]
- Newman, P.A.; Lacombe-Duncan, A. Human papillomavirus vaccination for men: Advancing policy and practice. Future Virol. 2014, 9, 1033–1047. [Google Scholar] [CrossRef]
- Brisson, M.; Kim, J.J.; Canfell, K.; Drolet, M.; Gingras, G.; Burger, E.A.; Martin, D.; Simms, K.T.; Bénard, É.; Boily, M.-C.; et al. Impact of HPV vaccination and cervical screening on cervical cancer elimination: A comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet 2020, 395, 575–590. [Google Scholar] [CrossRef]
- Valasoulis, G.; Pouliakis, A.; Michail, G.; Kottaridi, C.; Spathis, A.; Kyrgiou, M.; Paraskevaidis, E.; Daponte, A. Alterations of HPV-Related Biomarkers after Prophylactic HPV Vaccination. A Prospective Pilot Observational Study in Greek Women. Cancers 2020, 12, 1164. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem; World Health Organisation: Geneva, Switzerland, 2020; ISBN 978-92-4-001410-7. Available online: https://www.who.int/publications/i/item/9789240014107 (accessed on 3 March 2022).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef]
- Pry, J.M.; Manasyan, A.; Kapambwe, S.; Taghavi, K.; Duran-Frigola, M.; Mwanahamuntu, M.; Sikazwe, I.; Matambo, J.; Mubita, J.; Lishimpi, K.; et al. Cervical cancer screening outcomes in Zambia, 2010–2019: A cohort study. Lancet Glob. Health 2021, 9, e832–e840. [Google Scholar] [CrossRef]
- Mwanahamuntu, M.H.; Sahasrabuddhe, V.V.; Kapambwe, S.; Pfaendler, K.S.; Chibwesha, C.; Mkumba, G.; Mudenda, V.; Hicks, M.L.; Vermund, S.H.; Stringer, J.S.A.; et al. Advancing cervical cancer prevention initiatives in resource-constrained settings: Insights from the Cervical Cancer Prevention Program in Zambia. PLoS Med. 2011, 8, e1001032. [Google Scholar] [CrossRef]
- Yimer, N.B.; Mohammed, M.A.; Solomon, K.; Tadese, M.; Grutzmacher, S.; Meikena, H.K.; Alemnew, B.; Sharew, N.; Habtewold, T. Cervical cancer screening uptake in Sub-Saharan Africa: A systematic review and meta-analysis. Public Health 2021, 195, 105–111. [Google Scholar] [CrossRef]
- Rohner, E.; Mulongo, M.; Pasipamire, T.; Oberlin, A.M.; Goeieman, B.; Williams, S.; Lubeya, M.K.; Rahangdale, L.; Chibwesha, C.J. Mapping the cervical cancer screening cascade among women living with HIV in Johannesburg, South Africaa. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2021, 152, 53–59. [Google Scholar] [CrossRef]
- Ministry of Health Zambia. Zambia Population-based HIV Impact Assessment (ZAMPHIA) 2016: Final Report. Lusaka 2019. Available online: https://phia.icap.columbia.edu/zambia-final-report/ (accessed on 20 September 2020).
- Stelzle, D.; Tanaka, L.F.; Lee, K.K.; Khalil, A.I.; Baussano, I.; Shah, A.S.; McAllister, D.A.; Gottlieb, S.L.; Klug, S.J.; Winkler, A.S.; et al. Estimates of the global burden of cervical cancer associated with HIV. Lancet Glob. Health 2021, 9, e161–e169. [Google Scholar] [CrossRef]
- Kayombo, M. Zambia’s Hurdles in Cervical Cancer Fight. Daily Mail. 3 March 2022. Available online: http://www.daily-mail.co.zm/zambias-hurdles-in-cervical-cancer-fight/ (accessed on 3 March 2022).
- Gavi Full Country Evaluations Team. Zambia: Finding from the 2015 GAVI Full Country Evaluation 2016 02082020; pp. 7–8. Available online: https://www.gavi.org/sites/default/files/document/2015-fce-zambia-briefpdf.pdf (accessed on 25 March 2023).
- Guide to Introducing HPV Vaccine into National Immunization Programmes 2016. Available online: https://apps.who.int/iris/handle/10665/253123 (accessed on 25 August 2022).
- Gilkey, M.B.; Calo, W.A.; Marciniak, M.W.; Brewer, N.T. Parents who refuse or delay HPV vaccine: Differences in vaccination behavior, beliefs, and clinical communication preferences. Hum. Vaccines Immunother. 2017, 13, 680–686. [Google Scholar] [CrossRef]
- Liu, F.W.; Vwalika, B.; Hacker, M.R.; Allen, S.; Awtrey, C.S. Cervical cancer and HPV vaccination: Knowledge and attitudes of adult women in Lusaka, Zambia. J. Vaccines Vaccin. 2012, 3, 6816. [Google Scholar] [CrossRef]
- Delany-Moretlwe, S.; Kelley, K.F.; James, S.; Scorgie, F.; Subedar, H.; Dlamini, N.R.; Pillay, Y.; Naidoo, N.; Chikandiwa, A.; Rees, H. Human Papillomavirus Vaccine Introduction in South Africa: Implementation Lessons from an Evaluation of the National School-Based Vaccination Campaign. Glob. Health Sci. Pr. 2018, 6, 425–438. [Google Scholar] [CrossRef]
- Ikeda, S.; Ueda, Y.; Yagi, A.; Matsuzaki, S.; Kobayashi, E.; Kimura, T.; Miyagi, E.; Sekine, M.; Enomoto, T.; Kudoh, K. HPV vaccination in Japan: What is happening in Japan? Expert Rev. Vaccines 2019, 18, 323–325. [Google Scholar] [CrossRef]
- Soi, C.; Gimbel, S.; Chilundo, B.; Muchanga, V.; Matsinhe, L.; Sherr, K. Human papillomavirus vaccine delivery in Mozambique: Identification of implementation performance drivers using the Consolidated Framework for Implementation Research (CFIR). Implement. Sci. 2018, 13, 151. [Google Scholar] [CrossRef]
- Champion, V.L.; Skinner, C.S. The Health Belief Model. In Health Behaviour and Health Education Theory, Research, and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 45–65. [Google Scholar]
- Vermandere, H.; van Stam, M.A.; Naanyu, V.; Michielsen, K.; Degomme, O.; Oort, F. Uptake of the human papillomavirus vaccine in Kenya: Testing the health belief model through pathway modelling on cohort data. Glob. Health 2016, 12, 72. [Google Scholar] [CrossRef]
- Krawczyk, A.; Knäuper, B.; Gilca, V.; Dubé, E.; Perez, S.; Joyal-Desmarais, K.; Rosberger, Z. Parents’ decision-making about the human papillomavirus vaccine for their daughters: I. Quantitative results. Hum. Vaccines Immunother. 2015, 11, 322–329. [Google Scholar] [CrossRef]
- Donadiki, E.M.; Jiménez-García, R.; Hernández-Barrera, V.; Sourtzi, P.; Carrasco-Garrido, P.; López de Andrés, A.; Jimenez-Trujillo, I.; Velonakis, E. Health Belief Model applied to non-compliance with HPV vaccine among female university students. Public Health 2014, 128, 268–273. [Google Scholar] [CrossRef]
- Firouzbakht, M.; Sharif Nia, H.; Kazeminavaei, F.; Rashidian, P. Hesitancy about COVID-19 vaccination among pregnant women: A cross-sectional study based on the health belief model. BMC Pregnancy Childbirth 2022, 22, 611. [Google Scholar] [CrossRef]
- Chisale Mabotja, M.; Levin, J.; Kawonga, M. Beliefs and perceptions regarding cervical cancer and screening associated with Pap smear uptake in Johannesburg: A cross-sectional study. PLoS ONE 2021, 16, e0246574. [Google Scholar] [CrossRef]
- Cunningham, M.S.; Davison, C.; Aronson, K.J. HPV vaccine acceptability in Africa: A systematic review. Prev. Med. 2014, 69, 274–279. [Google Scholar] [CrossRef]
- Milimo, M.; Daka, E.; Sikuyuba, L.; Nyirenda, J.; Ngoma, C. Knowledge and attitudes of parents/guardians towards uptake of human papilloma virus (HPV) vaccine in preventing cervical cancer among girls in Zambia. Afr. J. Med. Med. Sci. 2015, 3, 84–91. [Google Scholar]
- Nyambe, A.; Kampen, J.K.; Baboo, S.K.; Van Hal, G. Knowledge, attitudes and practices of cervical cancer prevention among Zambian women and men. BMC Public Health 2019, 19, 508. [Google Scholar] [CrossRef]
- Central Statistics Office. Zambia 2010 Census of Population and Housing Summary Report. 2012. Available online: https://catalog.ihsn.org/index.php/catalog/4124 (accessed on 24 August 2020).
- Kucheba, F.; Mweemba, O.; Matenga, T.F.L.; Zulu, J.M. Acceptability of the human papillomavirus vaccine in schools in Lusaka in Zambia: Role of community and formal health system factors. Glob. Public Health 2021, 16, 378–389. [Google Scholar] [CrossRef]
- Wong, L.P.; Raja Muhammad Yusoff, R.N.; Edib, Z.; Sam, I.C.; Zimet, G.D. Nationwide Survey of Knowledge and Health Beliefs regarding Human Papillomavirus among HPV-Vaccinated Female Students in Malaysia. PLoS ONE 2016, 11, e0163156. [Google Scholar] [CrossRef]
- World Health Organization. Human Papilloma Virus (HPV) Vaccine Introduced in Zambia 2013. Available online: https://www.afro.who.int/news/human-papilloma-virus-hpv-vaccine-introduced-zambia (accessed on 25 March 2023).
- Ministerial Statement On Human Papillomavirus Vaccine By The Hon. Minister of Health, Lusaka, Zambia 2019. Available online: https://www.parliament.gov.zmpublication_docs/Ministerial%20Statement%20on%20HPV%20Vaccine.pdf (accessed on 5 September 2020).
- Kaonga, P.; Mukosha, M.; Jacobs, C.; Munakampe, M.N.; Sichone, V.; Phiri, C.C.; Makasa, M.; Vwalika, B.; Lubeya, M.K. No woman should be left behind: A decomposition analysis of socioeconomic inequalities in unsafe abortion among women presenting for abortion care services in Lusaka and Copperbelt provinces of Zambia. medRxiv 2022. [Google Scholar] [CrossRef]
- Hartung, C.; Lerer, A.; Anokwa, Y.; Tseng, C.; Brunette, W.; Borriello, G. (Eds.) Open data kit: Tools to build information services for developing regions. In Proceedings of the 4th ACM/IEEE International Conference on Information and Communication Technologies and Development, London, UK, 13–16 December 2010. [Google Scholar]
- Li, A.J.; Manzi, F.; Kyesi, F.; Makame, Y.; Mwengee, W.; Fleming, M.; Mkopi, A.; Mmbaga, S.; Lyimo, D.; Loharikar, A. Tanzania’s human papillomavirus (HPV) vaccination program: Community awareness, feasibility, and acceptability of a national HPV vaccination program, 2019. Vaccine 2022, 40 (Suppl. S1), A38–A48. [Google Scholar] [CrossRef]
- Doshi, R.H.; Casey, R.M.; Adrien, N.; Ndiaye, A.; Brennan, T.; Roka, J.L.; Bathily, A.; Ndiaye, C.; Li, A.; Garon, J.; et al. Feasibility and acceptability of nationwide HPV vaccine introduction in Senegal: Findings from community-level cross-sectional surveys, 2020. PLoS Glob. Public Health 2022, 2, e0000130. [Google Scholar] [CrossRef]
- Buis, M.L. Direct and indirect effects in a logit model. Stata J. 2010, 10, 11–29. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Strobe, I. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef]
- Fu, L.Y.; Zimet, G.D.; Latkin, C.A.; Joseph, J.G. Social Networks for Human Papillomavirus Vaccine Advice Among African American Parents. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2019, 65, 124–129. [Google Scholar] [CrossRef]
- Okunowo, A.A.; Ugwu, A.O.; Kuku, J.O.; Soibi-Harry, A.P.; Okunowo, B.O.; Ani-Ugwu, N.K.; Osunwusi, B.O.; Adenekan, M.A. Predictors, barriers and motivating factors for human papillomavirus vaccination and testing as preventive measures for cervical cancer: A study of urban women in Lagos, Nigeria. Prev. Med. Rep. 2021, 24, 101643. [Google Scholar] [CrossRef]
- Jones, C.L.; Jensen, J.D.; Scherr, C.L.; Brown, N.R.; Christy, K.; Weaver, J. The Health Belief Model as an explanatory framework in communication research: Exploring parallel, serial, and moderated mediation. Health Commun. 2015, 30, 566–576. [Google Scholar] [CrossRef]
- Clavé Llavall, A.; de Wildt, G.; Meza, G.; Tattsbridge, J.; Jones, L. Nurses’ and teachers’ perceived barriers and facilitators to the uptake of the Human Papilloma Virus (HPV) vaccination program in Iquitos, Peru: A qualitative study. PLoS ONE 2021, 16, e0255218. [Google Scholar] [CrossRef]
- Grandahl, M.; Tydén, T.; Westerling, R.; Nevéus, T.; Rosenblad, A.; Hedin, E.; Oscarsson, M. To Consent or Decline HPV Vaccination: A Pilot Study at the Start of the National School-Based Vaccination Program in Sweden. J. Sch. Health 2017, 87, 62–70. [Google Scholar] [CrossRef]
- Lubeya, M.K.; Mwanahamuntu, M.; Chibwesha, C.; Mukosha, M.; Wamunyima, M.M.; Kawonga, M. Implementation strategies to increase human papillomavirus vaccination uptake for adolescent girls in sub-Saharan Africa: A scoping review protocol. PLoS ONE 2022, 17, e0267617. [Google Scholar] [CrossRef]
- Isabirye, A.; Mbonye, M.; Asiimwe, J.B.; Kwagala, B. Factors associated with HPV vaccination uptake in Uganda: A multi-level analysis. BMC Women’s Health 2020, 20, 145. [Google Scholar] [CrossRef]
- Kurani, S.; MacLaughlin, K.L.; Jacobson, R.M.; St Sauver, J.L.; Jenkins, G.D.; Fan, C.; Jacobson, D.J.; Inselman, J.; Zhu, X.; Griffin, J.M.; et al. Socioeconomic disadvantage and human papillomavirus (HPV) vaccination uptake. Vaccine 2022, 40, 471–476. [Google Scholar] [CrossRef]
- Nyambe, A.; Lubeya, M.K. Cervical cancer and HIV in Zambian women. Lancet Glob. Health 2021, 9, e734–e735. [Google Scholar] [CrossRef]
- Mukosha, M.; Muyunda, D.; Mudenda, S.; Lubeya, M.K.; Kumwenda, A.; Mwangu, L.M.; Kaonga, P. Knowledge, attitude and practice towards cervical cancer screening among women living with human immunodeficiency virus: Implication for prevention strategy uptake. Nurs. Open 2022, 10, 2132–2141. [Google Scholar] [CrossRef]
- Wigfall, L.T.; Bynum, S.A.; Brandt, H.M.; Hébert, J.R. HPV Vaccine Awareness and Knowledge among Women Living with HIV. J. Cancer Educ. 2016, 31, 187–190. [Google Scholar] [CrossRef]
 ) affecting parental consent to vaccinate their daughter or mediated indirectly (
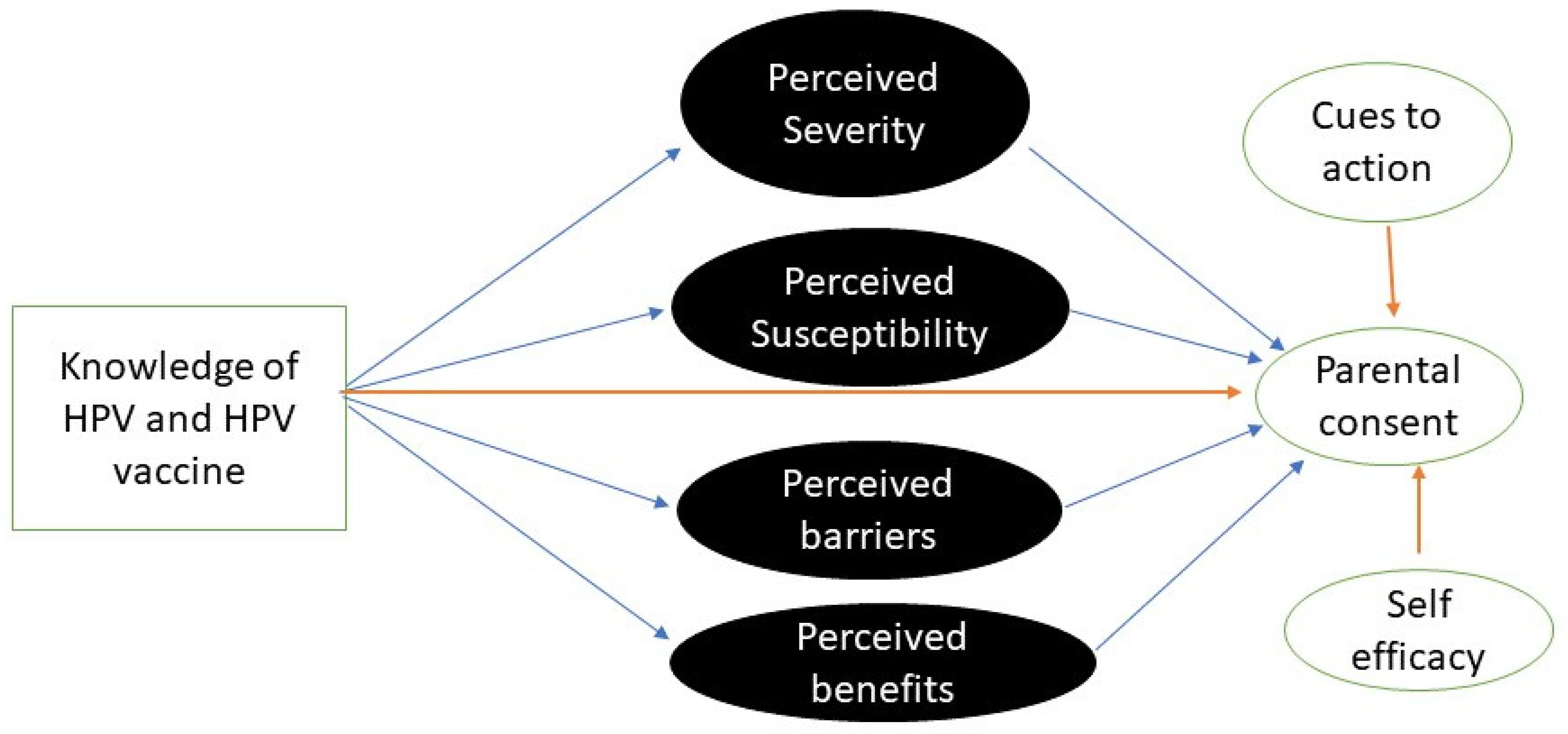
) affecting parental consent to vaccinate their daughter or mediated indirectly ( ) by 4 HBM constructs. At the same time, the other 2 HBM constructs directly affecting () the outcome.
) affecting parental consent to vaccinate their daughter or mediated indirectly () by 4 HBM constructs. At the same time, the other 2 HBM constructs directly affecting () the outcome.
) by 4 HBM constructs. At the same time, the other 2 HBM constructs directly affecting () the outcome.
) affecting parental consent to vaccinate their daughter or mediated indirectly () by 4 HBM constructs. At the same time, the other 2 HBM constructs directly affecting () the outcome.


{kind=link}
{kind=link}
| Variable | Total Sample N = 400 (%) | Parental Consent to Vaccinate a Daughter | |
|---|---|---|---|
| No, n = 185 | Yes, n = 215 | ||
| Age years mean [95% CI] | 45.7 [44.3–47.1] | 46.3 [44.1–48.6] | 45.3 [43.6–47.1] |
| Sex | |||
| Male | 50 (12.5) | 24 (13.1) | 26 (12.0) |
| Female | 350 (87.5) | 161 (87.0) | 189 (87.9) |
| Marital status | |||
| Married | 264 (66.0) | 121 (65.6) | 143 (66.5) |
| Single | 136 (34.0) | 64 (34.5) | 72 (33.5) |
| Education level | |||
| None/primary | 181 (45.3) | 89 (48.1) | 92 (42.8) |
| Secondary/Tertiary | 219 (54.8) | 96 (51.9) | 123 (57.2) |
| Employment | |||
| Unemployed | 330 (82.8) | 160 (86.5) | 170 (79.1) |
| Employed | 70 (17.3) | 25 (13.5) | 45 (20.9) |
| Daughter goes to school | |||
| Yes | 352 (88.0) | 157 (84.8) | 195 (90.7) |
| No | 48 (12.0) | 28 (15.1) | 20 (9.3) |
| Wealth index | |||
| Poorest/poorer/middle | 245 (61.3) | 124 (67.0) | 121 (56.3) |
| Richer/richest | 155 (38.8) | 61 (33.0) | 94 (43.7) |
| Total HPV/HPV vaccine knowledge mean score | 11.1 [10.0–12.2] | 9.0 [7.4–10.7] | 12.7 [11.1–14.3] |
| Characteristic | Total Population N = 400 (%) | Parental Consent to Vaccinate a Daughter | p-Value | |
|---|---|---|---|---|
| No, n = 185 (%) | Yes, n = 215 (%) | |||
| Ever been screened for cervical cancer? n = 350 | 0.001 | |||
| Yes | 247 (70.6) | 99 (61.5) | 148 (78.3) | |
| No | 103 (29.4) | 62 (38.5) | 41 (21.7) | |
| Know someone with cervical cancer? | 0.370 | |||
| Yes | 167 (41.8) | 72 (39.3) | 95 (43.8) | |
| No | 233 (58.3) | 111 (60.7) | 122 (56.2) | |
| Know someone with other HPV-related cancer, e.g., vulva, penis, oral | 0.011 | |||
| Yes | 43 (10.8) | 12 (6.6) | 31 (14.3) | |
| No | 357 (89.3) | 173 (93.5) | 184 (85.6) | |
| Know someone with genital warts? | <0.001 | |||
| Yes | 85 (21.3) | 23 (12.4) | 62 (28.8) | |
| No | 315 (78.8) | 162 (87.6) | 153 (71.2) | |
| Intent to vaccinate other daughters | 0.843 | |||
| No | 31 (7.8) | 15 (8.1) | 16 (7.4) | |
| Yes | 291 (72.8) | 132 (71.4) | 159 (74.0) | |
| Not sure | 78 (19.5) | 38 (20.5) | 40 (18.6) | |
| Daughter’s HIV status? n = 319 | 0.193 | |||
| Negative | 311 (97.5) | 127 (96.2) | 184 (98.4) | |
| Positive | 8 (2.5) | 5 (3.8) | 3 (1.6) | |
| HIV status n = 320 | 0.036 | |||
| Negative | 200 (62.5) | 94 (69.1) | 106 (7.6) | |
| Positive | 120 (37.5) | 42 (30.9) | 78 (42.4) | |
| Variable | COR [95% CI] a | p-Value | AOR [95% CI] | p-Value |
|---|---|---|---|---|
| Socio-demographics | ||||
| Age (years) | 0.99 [0.97–1.01] | 0.413 | ||
| Sex | ||||
| Male | Ref | |||
| Female | 0.54 [0.28–1.03] | 0.063 | ||
| Marital status | ||||
| Married | Ref | |||
| Single | 1.04 [0.62, 1.72] | 0.890 | ||
| Education | ||||
| None/Primary | Ref | |||
| Secondary/Tertiary | 1.07 [0.64–1.73] | 0.789 | ||
| Employment | ||||
| Employed | Ref | |||
| Unemployed | 1.49 [0.76–2.91] | 0.245 | ||
| HPV/HPV vaccine knowledge mean score | 1.04 [1.01–1.06] | 0.004 | ||
| Wealth index | 0.005 | |||
| Poorest/poorer/middle | Ref | Ref | ||
| Richer/richest | 1.93 [1.16–3.21] | 0.011 | 2.32 [1.29–4.16] | |
| Health Belief Model constructs | ||||
| Perceived susceptibility score | 1.04 [0.97, 1.12] | 0.241 | 1.05 [0.96–1.14] | 0.262 |
| Perceived severity score | 0.97 [0.91, 1.04] | 0.486 | 0.98 [0.91–1.06] | 0.590 |
| Perceived benefits score | 0.99 [0.90–1.09] | 0.835 | 1.06 [0.94–1.19] | 0.321 |
| Perceived barriers score | 0.98 [0.94–1.02] | 0.313 | 0.96 [0.90–1.01] | 0.108 |
| Self-efficacy | 1.04 [0.96–1.12] | 0.356 | 0.98 [0.88–1.09] | 0.726 |
| Cues to action | 1.08 [0.98–1.20] | 0.128 | 1.05 [0.92–1.19] | 0.492 |
| HPV and HIV-related characteristics | ||||
| Ever known anyone with cervical cancer | 1.14 [0.70, 1.86] | 0.588 | ||
| Ever known anyone with HPV-related cancers | 2.60 [1.22, 5.55] | 0.013 | ||
| Ever screened for cervical cancer | 2.32 [1.43, 3.80] | 0.001 | 1.93 [1.03–3.62] | 0.041 |
| Ever known anyone with genital warts | 2.54 [1.32–4.87] | 0.005 | 2.23 [1.04–4.76] | 0.039 |
| Daughters’ HIV status | ||||
| Negative | Ref | |||
| Positive | 0.64 [0.13, 3.01] | 0.567 | ||
| Parental HIV status | 0.078 | |||
| Negative | Ref | Ref | ||
| Positive | 1.93 [1.09, 3.42] | 0.024 | 1.07 [0.01–1.36] |
| Mediators | ||||||||
|---|---|---|---|---|---|---|---|---|
| Perceived Barriers | Perceived Susceptibility | Perceived Severity | Perceived Benefits | |||||
| Effects | OR [95% CI] | p-Value | OR [95% CI] | p-Value | OR [95% CI] | p-Value | OR [95% CI] | p-Value |
| Total | 2.37 [1.62–3.47] | <0.001 | 2.39 [1.58–3.61] | <0.001 | 2.39 [1.45–3.93] | 0.001 | 2.38 [1.53–3.71] | <0.001 |
| Indirect | 0.98 [0.95–1.01] | 0.297 | 1.01 [0.97–1.04] | 0.777 | 1.0 [0.97–1.03] | 0.901 | 1.0 [0.97–1.03] | 0.993 |
| Direct | 2.42 [1.66–3.52] | <0.001 | 2.37 [1.57–3.59] | <0.001 | 2.38 [1.45–3.90] | 0.001 | 2.39 [1.52–3.74] | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lubeya, M.K.; Chibwesha, C.J.; Mwanahamuntu, M.; Mukosha, M.; Maposa, I.; Kawonga, M. Correlates of Parental Consent to Human Papillomavirus Vaccine Uptake by Their Adolescent Daughters in ZAMBIA: Application of the Health Belief Model. Vaccines 2023, 11, 912. https://doi.org/10.3390/vaccines11050912
Lubeya MK, Chibwesha CJ, Mwanahamuntu M, Mukosha M, Maposa I, Kawonga M. Correlates of Parental Consent to Human Papillomavirus Vaccine Uptake by Their Adolescent Daughters in ZAMBIA: Application of the Health Belief Model. Vaccines. 2023; 11(5):912. https://doi.org/10.3390/vaccines11050912
Chicago/Turabian StyleLubeya, Mwansa Ketty, Carla J. Chibwesha, Mulindi Mwanahamuntu, Moses Mukosha, Innocent Maposa, and Mary Kawonga. 2023. "Correlates of Parental Consent to Human Papillomavirus Vaccine Uptake by Their Adolescent Daughters in ZAMBIA: Application of the Health Belief Model" Vaccines 11, no. 5: 912. https://doi.org/10.3390/vaccines11050912
APA StyleLubeya, M. K., Chibwesha, C. J., Mwanahamuntu, M., Mukosha, M., Maposa, I., & Kawonga, M. (2023). Correlates of Parental Consent to Human Papillomavirus Vaccine Uptake by Their Adolescent Daughters in ZAMBIA: Application of the Health Belief Model. Vaccines, 11(5), 912. https://doi.org/10.3390/vaccines11050912