
Key Lessons from COVID-19: A Narrative Review Describing Qatar’s Multifactorial Approach in Executing a Vaccination Campaign

 , , and
, , and
Abstract
:1. Introduction
2. Search Strategy
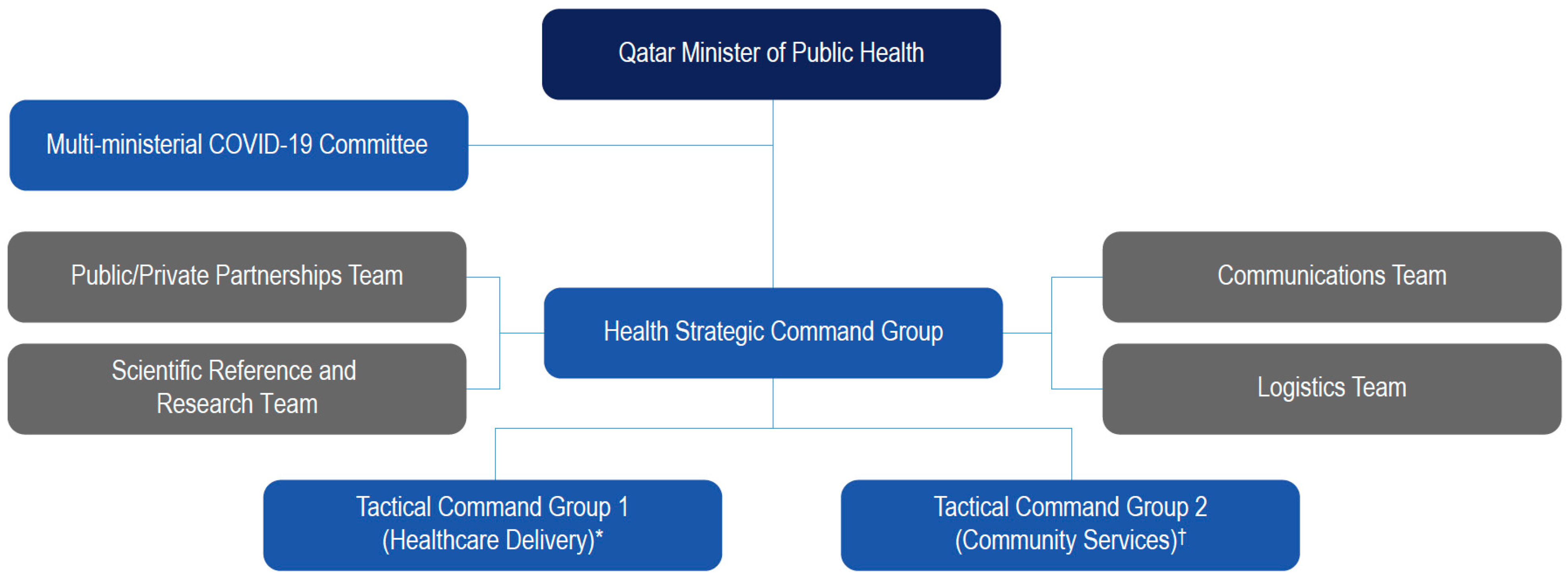
3. Response to Emergence of COVID-19 in Qatar
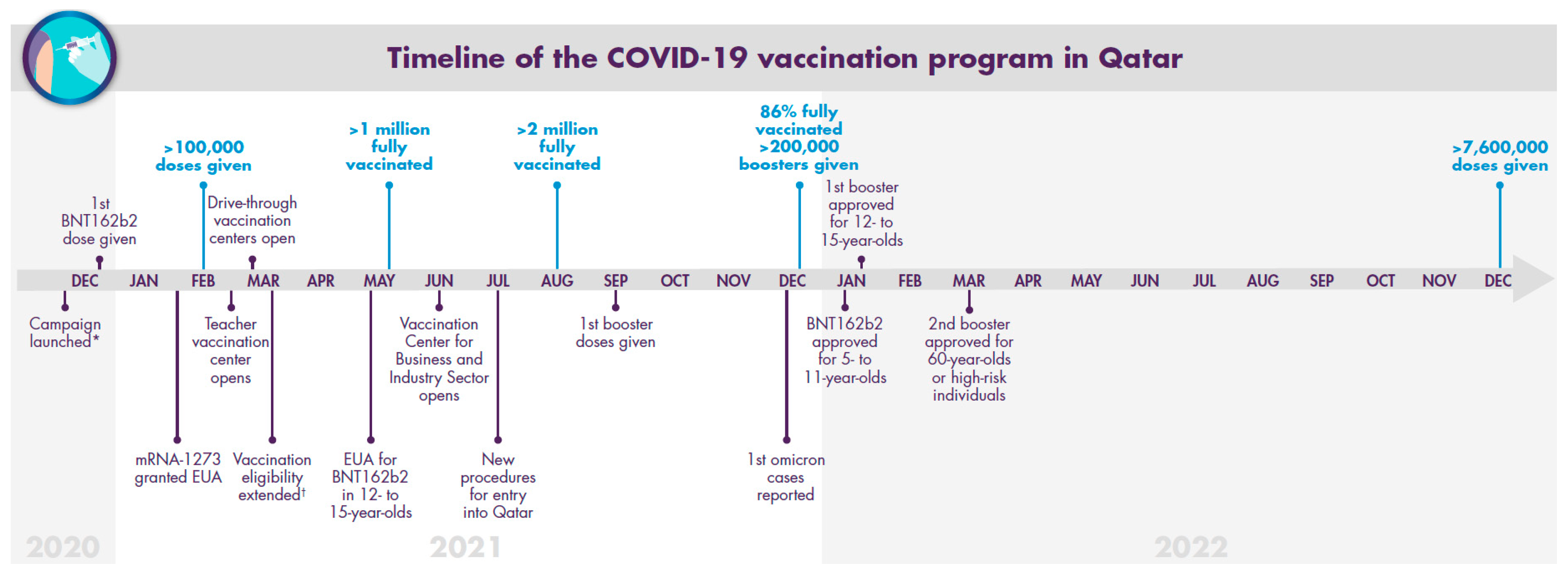
4. The Qatar COVID-19 Vaccination Campaign
4.1. December 2020
4.2. January–March 2021
4.3. April–June 2021
4.4. July–December 2021
4.5. January 2022–January 2023
5. Real-World Vaccine Effectiveness Data from Qatar
6. Previous Experience and Additional Factors Potentially Integral to the Qatar COVID-19 Vaccination Campaign
7. Vaccine Hesitancy and Mitigation of Misinformation
8. Assessing the Success of Qatar’s COVID-19 Campaign
9. Lessons Learned
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 4 January 2023).
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 4 January 2023).
- Luqmani, Y.A.; El Hashim, A. The COVID-19 pandemic: A health crisis managed, or a panic response with disastrous future consequences. Med. Princ. Pract. 2021, 21, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Douglas, M.; Katikireddi, S.V.; Taulbut, M.; McKee, M.; McCartney, G. Mitigating the wider health effects of COVID-19 pandemic response. BMJ 2020, 369, m1557. [Google Scholar] [CrossRef]
- Haldane, V.; De Foo, C.; Abdalla, S.M.; Jung, A.S.; Tan, M.; Wu, S.; Chua, A.; Verma, M.; Shrestha, P.; Singh, S.; et al. Health systems resilience in managing the COVID-19 pandemic: Lessons from 28 countries. Nat. Med. 2021, 27, 964–980. [Google Scholar] [CrossRef]
- Farrugia, G.; Plutowski, R.W. Innovation lessons from the COVID-19 pandemic. Mayo Clin. Proc. 2020, 95, 1574–1577. [Google Scholar] [CrossRef]
- Webb, E.; Hernández-Quevedo, C.; Williams, G.; Scarpetti, G.; Reed, S.; Panteli, D. Providing health services effectively during the first wave of COVID-19: A cross-country comparison on planning services, managing cases, and maintaining essential services. Health Policy 2022, 126, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Webb, E.; Winkelmann, J.; Scarpetti, G.; Behmane, D.; Habicht, T.; Kahur, K.; Kasekamp, K.; Köhler, K.; Miščikienė, L.; Misins, J.; et al. Lessons learned from the Baltic countries’ response to the first wave of COVID-19. Health Policy 2022, 126, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Waitzberg, R.; Hernández-Quevedo, C.; Bernal-Delgado, E.; Estupiñán-Romero, F.; Angulo-Pueyo, E.; Theodorou, M.; Kantaris, M.; Charalambous, C.; Gabriel, E.; Economou, C.; et al. Early health system responses to the COVID-19 pandemic in Mediterranean countries: A tale of successes and challenges. Health Policy 2022, 126, 465–475. [Google Scholar] [CrossRef]
- Saunes, I.S.; Vrangbæk, K.; Byrkjeflot, H.; Jervelund, S.S.; Birk, H.O.; Tynkkynen, L.K.; Keskimäki, I.; Sigurgeirsdóttir, S.; Janlöv, N.; Ramsberg, J.; et al. Nordic responses to Covid-19: Governance and policy measures in the early phases of the pandemic. Health Policy 2022, 126, 418–426. [Google Scholar] [CrossRef]
- Kumpunen, S.; Webb, E.; Permanand, G.; Zheleznyakov, E.; Edwards, N.; van Ginneken, E.; Jakab, M. Transformations in the landscape of primary health care during COVID-19: Themes from the European region. Health Policy 2022, 126, 391–397. [Google Scholar] [CrossRef]
- Unruh, L.; Allin, S.; Marchildon, G.; Burke, S.; Barry, S.; Siersbaek, R.; Thomas, S.; Rajan, S.; Koval, A.; Alexander, M.; et al. A comparison of 2020 health policy responses to the COVID-19 pandemic in Canada, Ireland, the United Kingdom and the United States of America. Health Policy 2022, 126, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Samadizadeh, S.; Nakstad, B.; Jamalpoor, Z.; Tahamtan, A. COVID-19 diagnosis: Lessons to learn and hints for preparedness. Expert Rev. Mol. Diagn. 2022, 22, 851–853. [Google Scholar] [CrossRef] [PubMed]
- Planning and Statistics Authority. Main Results of the General Census of Population, Housing and Establishments. Available online: https://www.psa.gov.qa/en/statistics1/StatisticsSite/Census/census2020/res/Documents/Census_2020_Res_Summary_En.pdf (accessed on 4 January 2023).
- Al-Thani, M.H.; Farag, E.; Bertollini, R.; Al Romaihi, H.E.; Abdeen, S.; Abdelkarim, A.; Daraan, F.; Elhaj Ismail, A.I.H.; Mostafa, N.; Sahl, M.; et al. SARS-CoV-2 infection is at herd immunity in the majority segment of the population of Qatar. Open Forum Infect. Dis. 2021, 8, ofab221. [Google Scholar] [CrossRef]
- The World Bank. Life Expectancy at Birth, Total (Years)—Qatar. 2020. Available online: https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=QA (accessed on 4 January 2023).
- Institute for Health Metrics and Evaluation. GBD Profile: Qatar. Available online: https://www.healthdata.org/sites/default/files/files/country_profiles/GBD/ihme_gbd_country_report_qatar.pdf (accessed on 4 January 2023).
- Al Khal, A.; Al-Kaabi, S.; Checketts, R.J. Qatar’s response to COVID-19 pandemic. Heart Views 2020, 21, 129–132. [Google Scholar] [PubMed]
- Goodman, A. The development of the Qatar Healthcare System: A review of the literature. Int. J. Clin. Med. 2015, 6, 177–185. [Google Scholar] [CrossRef]
- State of Qatar Ministry of Public Health. National Health Strategy 2018–2022. Available online: https://www.moph.gov.qa/Style%20Library/MOPH/Files/strategies/National%20Health%20Strategy%202018%20-%202022/NHS%20EN.pdf (accessed on 4 January 2023).
- Al-Dahshan, A.; Hammoud, H.; Chehab, M.; Osman, S.R.O. Vaccination coverage in Qatar: Benchmarking with global figures. Qatar Med. J. 2019, 2019, 4. [Google Scholar] [CrossRef]
- Al Kuwari, H.M.; Abdul Rahim, H.F.; Abu-Raddad, L.J.; Abou-Samra, A.B.; Al Kanaani, Z.; Al Khal, A.; Al Kuwari, E.; Al Marri, S.; Al Masalmani, M.; Al Romaihi, H.E.; et al. Epidemiological investigation of the first 5685 cases of SARS-CoV-2 infection in Qatar, 28 February–18 April 2020. BMJ Open 2020, 10, e040428. [Google Scholar] [CrossRef] [PubMed]
- Social Science Research Council. Qatar, the Coronavirus, and Cordons Sanitaires: Migrant Workers and the Use of Public Health to Define the Nation. Available online: https://items.ssrc.org/covid-19-and-the-social-sciences/qatar-the-coronavirus-and-cordons-sanitaires-migrant-workers-and-the-use-of-public-health-to-define-the-nation/ (accessed on 4 January 2023).
- Ministry of Public Health. COVID-19 Qatar National Response Action Plan March 2020. Available online: https://www.moph.gov.qa/Style%20Library/MOPH/Videos/COVID-19%20REPORT%20WEB.pdf (accessed on 4 January 2023).
- Fahey, C.; Harris, R. Qatar Says It’s Working to Protect Laborers from Coronavirus; The Associated Press: New York, NY, USA, 2020. [Google Scholar]
- Installing Ehteraz App in Mobile Phones Compulsory from Today for All; The Peninsula: Doha, Qatar, 2021; Available online: https://thepeninsulaqatar.com/article/22/05/2020/Installing-Ehteraz-app-in-mobile-phones-compulsory-from-today-for-all (accessed on 20 January 2022).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Public Health. COVID-19 Vaccination: Information for Older Persons. Available online: http://pfizer.chcshare.net/covid19vaccine/1000%20Manuscripts/COV-VAX1057%20-%20Qatar%20Regional%20MS/references/MoPH_Older%20persons.pdf (accessed on 4 January 2023).
- Qatar News Agency. Qatar confronts COVID-19 with largest vaccination campaign in its history. Qatar Tribune, 1 June 2021. [Google Scholar]
- Hasan, T.; Beardsley, J.; Marais, B.J.; Nguyen, T.A.; Fox, G.J. The implementation of mass-vaccination against SARS-CoV-2: A systematic review of existing strategies and guidelines. Vaccines 2021, 9, 326. [Google Scholar] [CrossRef]
- Primary Health Care Corporation. PHCC Administrates Over 2.2 Million COVID-19 Vaccines to Date. 28 August 2021. Available online: https://www.phcc.gov.qa/en/Media/News/PHCC-administrates-over-2-million-Covid-19-vaccines-to-date (accessed on 4 January 2023).
- CoVariants. Overview of Variants in Countries. Available online: https://covariants.org/per-country (accessed on 4 January 2023).
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. Waning of BNT162b2 vaccine protection against SARS-CoV-2 infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef]
- Our World in Data. Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations?country=~OWID_WRL (accessed on 4 January 2023).
- Qatar grants emergency use authorisation for Moderna’s COVID-19 vaccine. Pharmaceutical Technology, 12 February; 2021.
- Primary Health Care Corporation. Prime Minister Opens COVID-19 Vaccination Center at QNCC for Teachers, School Administration Staff and Other Community Members. Available online: https://www.phcc.gov.qa/en/Media/News/Prime-Minister-opens-COVID-19-vaccination-center-at-QNCC (accessed on 4 January 2023).
- Ministry of Public Health. Lowers Age Threshold for COVID-19 Vaccine; The Peninsula: Doha, Qatar, 2021; Available online: https://thepeninsulaqatar.com/article/03/03/2021/MoPh-lowers-age-threshold-for-Covid-19-vaccine-1 (accessed on 20 January 2022).
- Ministry of Public Health. COVID-19 Vaccine: Total Number of Vaccine Doses Administered. Available online: https://covid19.moph.gov.qa/EN/Pages/default.aspx (accessed on 4 January 2023).
- More than 110,000 people used drive-through centres in Lusail and Al Wakra. Qatar Tribune, 24 April; 2021.
- Hasan, M.R.; Kalikiri, M.K.R.; Mirza, F.; Sundararaju, S.; Sharma, A.; Xaba, T.; Lorenz, S.; Chemaitelly, H.; El-Kahlout, R.A.; Tsui, K.M.; et al. Real-time SARS-CoV-2 genotyping by high-throughput multiplex PCR reveals the epidemiology of the variants of concern in Qatar. Int. J. Infect. Dis. 2021, 112, 52–54. [Google Scholar] [CrossRef]
- Frenck, R.W., Jr.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, immunogenicity, and efficacy of the BNT162b2 COVID-19 vaccine in adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes Pfizer-BioNTech COVID-19 Vaccine for Emergency Use in Adolescents in Another Important Action in Fight Against Pandemic. 10 May 2021. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-pfizer-biontech-covid-19-vaccine-emergency-use (accessed on 4 January 2023).
- Parents Can Register 12-to-15-Year-Old Children for Vaccine from Tomorrow; The Peninsula: Doha, Qatar, 2021; Available online: https://thepeninsulaqatar.com/article/15/05/2021/Parents-can-register-12-to-15-year-old-children-for-vaccine-from-tomorrow (accessed on 20 January 2022).
- Qatar opens one of the largest vaccination centre in the world. Marhaba. 23 June 2021. Available online: https://marhaba.qa/qatar-opens-one-of-the-largest-vaccination-centre-in-the-world (accessed on 24 January 2022).
- Qatar Vaccination Center for Business and Industry Sector Is One of the Largest Vaccination Centers in the World; The Peninsula: Doha, Qatar, 2021; Available online: https://thepeninsulaqatar.com/article/22/06/2021/Qatar-Vaccination-Center-for-Business-and-Industry-Sector-is-one-of-the-largest-vaccination-centers-in-the-world (accessed on 24 January 2022).
- Ministry of Public Health. New Procedures on the Travel and Return Policy to the State of Qatar to Continue Facilitating Travel for Travelers as of 8 July 2021. Available online: https://www.moph.gov.qa/english/mediacenter/News/Pages/NewsDetails.aspx?ItemId=400 (accessed on 4 January 2023).
- Ministry of Public Health. Qatar Travel and Return Policy. Available online: https://covid19.moph.gov.qa/EN/travel-and-return-policy/Pages/default.aspx#:~:text=1.-,Travelers%20who%20are%20fully%20vaccinated%2C%20inside%20or%20outside%20Qatar%2C%20by,of%20a%20MOPH%20approved%20vaccine (accessed on 4 January 2023).
- Qatar Begins Administering Booster Dose of COVID-19 Vaccine; The Peninsula: Doha, Qatar, 2021; Available online: https://thepeninsulaqatar.com/article/15/09/2021/Qatar-begins-administering-booster-dose-of-Covid-19-vaccine (accessed on 21 January 2022).
- Fazeena Saleem. MoPH to Intensify Efforts in Giving Booster Dose; The Peninsula: Doha, Qatar, 2021; Available online: https://thepeninsulaqatar.com/article/24/12/2021/moph-to-intensify-efforts-in-giving-booster-dose (accessed on 21 January 2022).
- Qatar Registers Its First Four Cases of Omicron—QNA; Reuters: London, UK, 2021; Available online: https://www.reuters.com/world/middle-east/qatar-registers-its-first-four-cases-omicron-qna-2021-12-17/ (accessed on 24 January 2022).
- Mathew, S. Qatar Approves Pfizer Boosters for Children Aged 12 to 15 years; Bloomberg: New York, NY, USA, 2022; Available online: https://www.bloomberg.com/news/articles/2022-01-09/qatar-approves-pfizer-boosters-for-children-aged-12-to-15-years (accessed on 3 March 2022).
- Qatar News Agency. Qatar Starts Giving COVID-19 Vaccine to 5–11 Years Old; The Peninsula: Doha, Qatar, 2022; Available online: https://thepeninsulaqatar.com/article/30/01/2022/qatar-starts-giving-covid-19-vaccine-to-5-11-years-old (accessed on 3 January 2023).
- MOPH Approves Fourth Dose of COVID-19 Vaccine; The Peninsula: Doha, Qatar, 2022; Available online: https://thepeninsulaqatar.com/article/30/03/2022/moph-approves-fourth-dose-of-covid-19-vaccine (accessed on 3 January 2023).
- Alabdulla, M.; Reagu, S.M.; Al-Khal, A.; Elzain, M.; Jones, R.M. COVID-19 vaccine hesitancy and attitudes in Qatar: A national cross-sectional survey of a migrant-majority population. Influenza Other Respir. Viruses 2021, 15, 361–370. [Google Scholar] [CrossRef]
- Kumar, R.; Alabdulla, M.; Elhassan, N.M.; Reagu, S.M. Qatar healthcare workers’ COVID-19 vaccine hesitancy and attitudes: A national cross-sectional survey. Front. Public Health 2021, 9, 727748. [Google Scholar] [CrossRef]
- Al-Mulla, R.; Abu-Madi, M.; Talafha, Q.M.; Tayyem, R.F.; Abdallah, A.M. COVID-19 vaccine hesitancy in a representative education sector population in Qatar. Vaccines 2021, 9, 665. [Google Scholar] [CrossRef] [PubMed]
- Musa, S.; Dergaa, I.; Abdulmalik, M.A.; Ammar, A.; Chamari, K.; Saad, H.B. BNT162b2 COVID-19 vaccine hesitancy among parents of 4023 young adolescents (12–15 years) in Qatar. Vaccines 2021, 9, 981. [Google Scholar] [CrossRef] [PubMed]
- Mohan, S.; Reagu, S.; Lindow, S.; Alabdulla, M. COVID-19 vaccine hesitancy in perinatal women: A cross sectional survey. J. Perinat. Med. 2021, 49, 678–685. [Google Scholar] [CrossRef]
- Purayil, S.; Thalappil, S.; Al-Nesf, M.; Kocaturk, E. Chronic urticaria and COVID-19 vaccination: Qatar data (preliminary report of COVAC-CU-international). Qatar Med. J. 2022, 2022, 2. [Google Scholar] [CrossRef]
- Feikin, D.R.; Abu-Raddad, L.J.; Andrews, N.; Davies, M.A.; Higdon, M.M.; Orenstein, W.A.; Patel, M.K. Assessing vaccine effectiveness against severe COVID-19 disease caused by omicron variant. Report from a meeting of the World Health Organization. Vaccine 2022, 40, 3516–3527. [Google Scholar] [CrossRef]
- Chemaitelly, H.; AlMukdad, S.; Ayoub, H.H.; Altarawneh, H.N.; Coyle, P.; Tang, P.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Hasan, M.R.; et al. COVID-19 vaccine protection among children and adolescents in Qatar. N. Engl. J. Med. 2022, 387, 1865–1876. [Google Scholar] [CrossRef]
- Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Coyle, P.; Tang, P.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Hasan, M.R.; Al-Kanaani, Z.; et al. Duration of mRNA vaccine protection against SARS-CoV-2 Omicron BA.1 and BA.2 subvariants in Qatar. Nat. Commun. 2022, 13, 3082. [Google Scholar] [CrossRef] [PubMed]
- Butt, A.A.; Chemaitelly, H.; Al Khal, A.; Coyle, P.V.; Saleh, H.; Kaleeckal, A.H.; Latif, A.N.; Bertollini, R.; Abou-Samra, A.B.; Abu-Raddad, L.J. SARS-CoV-2 vaccine effectiveness in preventing confirmed infection in pregnant women. J. Clin. Investig. 2021, 131, e153662. [Google Scholar] [CrossRef]
- Altarawneh, H.N.; Chemaitelly, H.; Ayoub, H.H.; Tang, P.; Hasan, M.R.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Coyle, P.; Al-Kanaani, Z.; et al. Effects of previous infection and vaccination on symptomatic omicron infections. N. Engl. J. Med. 2022, 387, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Chemaitelly, H.; AlMukdad, S.; Joy, J.P.; Ayoub, H.H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Tang, P.; Hasan, M.R.; Coyle, P.; et al. SARS-CoV-2 vaccine effectiveness in immunosuppressed kidney transplant recipients. medRxiv. Prepr. 2021. [Google Scholar] [CrossRef]
- Butt, A.A.; Nafady-Hego, H.; Chemaitelly, H.; Abou-Samra, A.B.; Khal, A.A.; Coyle, P.V.; Kanaani, Z.A.; Kaleeckal, A.H.; Latif, A.N.; Masalmani, Y.A.; et al. Outcomes among patients with breakthrough SARS-CoV-2 infection after vaccination. Int. J. Infect. Dis. 2021, 110, 353–358. [Google Scholar] [CrossRef]
- Chemaitelly, H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Tang, P.; Hasan, M.R.; Malek, J.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. mRNA-1273 COVID-19 vaccine effectiveness against the B.1.1.7 and B.1.351 variants and severe COVID-19 disease in Qatar. Nat. Med. 2021, 27, 1614–1621. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Butt, A.A.; National Study Group for, C.-V. Effectiveness of the BNT162b2 COVID-19 Vaccine against the B.1.1.7 and B.1.351 Variants. N. Engl. J. Med. 2021, 385, 187–189. [Google Scholar] [CrossRef]
- Tang, P.; Hasan, M.R.; Chemaitelly, H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; AlMukdad, S.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. BNT162b2 and mRNA-1273 COVID-19 vaccine effectiveness against the SARS-CoV-2 Delta variant in Qatar. Nat. Med. 2021, 27, 2136–2143. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Tang, P.; Hasan, M.R.; Coyle, P.; et al. Effect of mRNA vaccine boosters against SARS-CoV-2 Omicron infection in Qatar. N. Engl. J. Med. 2022, 386, 1804–1816. [Google Scholar] [CrossRef]
- Hamad Medical Corporation. MOPH, PHCC and HMC Launch Public Influenza Vaccination Campaign. Available online: https://www.hamad.qa/EN/news/2018/October/Pages/MOPH-PHCC-and-HMC-launch-Public-Influenza-Vaccination-Campaign.aspx (accessed on 4 January 2023).
- State of Qatar Ministry of Public Health. A Report on Qatar’s National Response to COVID-19. Available online: https://apps.who.int/gb/statements/WHA73_RESUMED/PDF/Qatar-13.2-14.pdf (accessed on 4 January 2023).
- Mundodan, J.H.; Hasnain, S.; Al Jubni, H.; Khogali, H.; Al Bayat, S.; Al-Romaihi, H. Adverse Events Following Immunization (AEFI) surveillance in Qatar: 2014–2018. J. Pharmacovigil. 2020, 8, 287. [Google Scholar]
- World Health Organization. Strategy to Achieve Global COVID-19 Vaccination by Mid-2022. Available online: https://cdn.who.int/media/docs/default-source/immunization/covid-19/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022.pdf (accessed on 4 January 2023).
- MacDonald, N.E.; Hesitancy, S.W.G.o.V. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Abdul Karim, M.; Reagu, S.M.; Ouanes, S.; Waheed Khan, A.; Smidi, W.S.; Al-Baz, N.; Alabdulla, M. Prevalence and correlates of COVID-19 vaccine hesitancy among the elderly in Qatar: A cross-sectional study. Medicine 2022, 101, e29741. [Google Scholar] [CrossRef] [PubMed]
- Johns Hopkins Center for Communication Programs. COVID Behaviors Dashboard. Available online: https://covidbehaviors.org/ (accessed on 4 January 2023).
- Reagu, S.; Mohan, S.; Awwad, J.; Alabdulla, M. Maternal vaccine hesitancy towards COVID-19 immunisation of children in Qatar: A population-based cross-sectional study. Epidemiol. Health 2022, 44, e2022056. [Google Scholar] [CrossRef]
- Khatatbeh, M.; Albalas, S.; Khatatbeh, H.; Momani, W.; Melhem, O.; Al Omari, O.; Tarhini, Z.; A’Aqoulah, A.; Al-Jubouri, M.; Nashwan, A.J.; et al. Children’s rates of COVID-19 vaccination as reported by parents, vaccine hesitancy, and determinants of COVID-19 vaccine uptake among children: A multi-country study from the Eastern Mediterranean Region. BMC Public Health 2022, 22, 1375. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Public Health. Coronavirus Disease 2019 (COVID-19): Trusted Information Source. Available online: https://covid19.moph.gov.qa/EN/Covid19-Vaccine/Pages/Trusted-Information-Source.aspx (accessed on 4 January 2023).
- Ahmad, R.; Hillman, S. Laboring to communicate: Use of migrant languages in COVID-19 awareness campaign in Qatar. Multilingua 2021, 40, 303–337. [Google Scholar] [CrossRef]
- State of Qatar Government Communications Office. In Focus Coronavirus (COVID-19). Available online: https://www.gco.gov.qa/en/focus/covid-19/ (accessed on 4 January 2023).
- Qatar Computing Research Institute. Social Media, Technology and COVID-19: The View from QCRI Scientists. Available online: https://www.hbku.edu.qa/en/news/social-media-technology (accessed on 4 January 2023).
- Alkaabi, I.; Abita, M.; Mahdi, Y.; Ouda, A.; Malki, M.I. Knowledge, Attitude, Practices, and Sources of Information (KAPS) toward COVID-19 during the second wave pandemic among university population in Qatar: A cross-sectional study. Front. Public Health 2022, 10, 906159. [Google Scholar] [CrossRef]
- Kumar, D.; Chandra, R.; Mathur, M.; Samdariya, S.; Kapoor, N. Vaccine hesitancy: Understanding better to address better. Isr. J. Health Policy Res. 2016, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; Al Kanaani, Z.; Al Khal, A.; Al Kuwari, E.; Butt, A.A.; Coyle, P.; Jeremijenko, A.; Kaleeckal, A.H.; et al. Characterizing the Qatar advanced-phase SARS-CoV-2 epidemic. Sci. Rep. 2021, 11, 6233. [Google Scholar] [CrossRef]
- US Centers for Disease Control and Prevention. Variants of the Virus: What You Need to Know. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/omicron-variant.html (accessed on 4 January 2023).
- Qatar Sees Spike in COVID Cases As It Enters ‘Third Wave’. Aljazeera. Available online: https://www.aljazeera.com/news/2022/1/3/qatar-sees-spike-in-covid-cases-as-it-enters-third-wave (accessed on 4 January 2023).
- Qatar Reimposes COVID-19 Curbs on Rising Cases. Argus. Available online: https://www.argusmedia.com/en/news/2290021-qatar-reimposes-covid19-curbs-on-rising-cases (accessed on 4 January 2023).
- Al-Jayyousi, G.F.; Nour, M.; Suliman, J.; Abed Alah, M.; Ali, K.; Abdeen, S.; Al-Thani, M.; Jaffrey, S.; Al-Romaihi, H.E.; Farag, E. Barriers to practicing COVID-19 preventive behaviors among migrant workers in Qatar: A qualitative study during the first wave of the pandemic. Int. J. Public Health 2022, 67, 1604881. [Google Scholar] [CrossRef]
- Alinier, G.; Al Badawi, A.K.A.; Gharib, R.; Ramsumar, S.; Morris, B.D. Setting up a temporary isolation tent site for asymptomatic COVID-19 positive male migrant workers in Qatar. Qatar Med. J. 2022, 2022, 55. [Google Scholar] [CrossRef]
- Tawe Ngi, A.M.; Johnston, S.; Albayat, S.S.; Bansal, D.; Ahmed, S.; Sallam, M.A.; Al-Romaihi, H.E.; Al-Thani, M.; Farag, E.; Emara, M.M. Pre-symptomatic and asymptomatic transmission of COVID-19: Implications for control measures in Qatar. Qatar Med. J. 2021, 2021, 59. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Dose 1 | Dose 2 | Dose 3 | Dose 4 | Total | |
|---|---|---|---|---|---|
| Pfizer | 1,521,352 | 1,514,436 | 1,259,362 | 83,642 | 4,378,792 |
| Moderna | 1,132,198 | 1,083,948 | 624,023 | 211,391 | 3,051,560 |
| AstraZeneca | 94,597 | 41,359 | 17,399 | 17,115 | 170,470 |
| Total | 2,748,147 | 2,639,743 | 1,900,784 | 312,148 | 7,600,822 |
| Migrant Majority [55] | Healthcare Workers [56] | Education Sector [57] | Parents of Young Adolescents [58] | Perinatal Women [59] | |
|---|---|---|---|---|---|
| Study dates | 15 October 2020–15 November 2020 | 15 October 2020–15 November 2020 | February 2021 | 17 May 2021–3 June 2021 | 15 October 2020–15 November 2020 |
| Population | Total population surveyed, 7821 Non-national participants, 6907 | Healthcare workers, 1546 | Qatar University employees and students, 462 | Parents of 12-to-15-year-old adolescents, 4023 | Pregnant or lactating women, 341 |
| Study design | Cross-sectional survey | Cross-sectional survey | Cross-sectional survey | Cross-sectional study | Cross-sectional survey |
| Vaccine hesitancy rate |
|
|
|
|
|
| Concerns |
|
|
|
|
|
| Proposed measures to address vaccine hesitancy |
|
|
|
|
|
| Cases, n | Deaths, n (%) | Fully Vaccinated, % | |
|---|---|---|---|
| Global | 655,689,115 | 6,671,624 (1.02) | 64.5 |
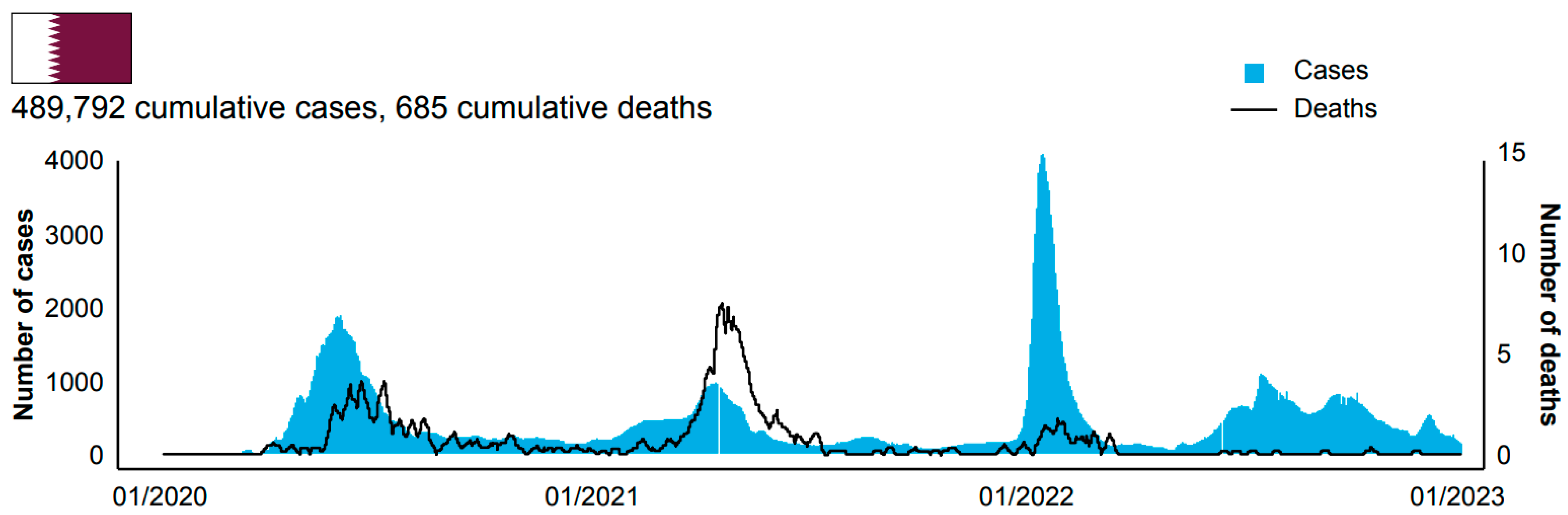
| Qatar | 489,792 | 685 (0.14) | 98.9 |
| Bahrain | 696,614 | 1536 (0.22) | 72.1 |
| Kuwait | 662,747 | 2570 (0.39) | 78.3 |
| Oman | 399,154 | 4628 (1.16) | 59.7 |
| Saudi Arabia | 827,071 | 9521 (1.15) | 72.8 |
| United Arab Emirates | 1,047,109 | 2348 (0.22) | 99.0 |
| United Kingdom | 24,135,084 | 198,937 (0.82) | 74.6 |
| United States | 99,423,758 | 1,082,265 (1.09) | 68.3 |
| South Africa | 4,048,580 | 102,568 (2.53) | 35.5 |
| China | 10,322,499 | 31,914 (0.31) | 86.8 |
| Challenges | Successes |
|---|---|
| Protecting the health, well-being, and prosperity of Qatar’s citizens and residents by preparing for, monitoring, responding to, and recovering from COVID-19 outbreaks [24] |
|
| Access to healthcare due to rapid spread of COVID-19 among migrant workers [18,25] |
|
| Limiting viral transmission [22,26,47,91] |
|
| Vaccine availability [29,30,31,36,45,46,49,50,72,73] |
|
| Protection of at-risk populations [34,56,57,58,59,67,74] |
|
| Emerging variants [41,49,50,90] |
|
| Timely public health responses |
|
| Vaccine hesitancy and misinformation [18,26,74,81,82,83,84] |
|
| Measuring success of the vaccination program (see Table 3) |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albayat, S.; Almaslamani, M.; Alromaihi, H.; Khogali, H.; Mundodan, J.; Joury, J.; Haridy, H. Key Lessons from COVID-19: A Narrative Review Describing Qatar’s Multifactorial Approach in Executing a Vaccination Campaign. Vaccines 2023, 11, 953. https://doi.org/10.3390/vaccines11050953
Albayat S, Almaslamani M, Alromaihi H, Khogali H, Mundodan J, Joury J, Haridy H. Key Lessons from COVID-19: A Narrative Review Describing Qatar’s Multifactorial Approach in Executing a Vaccination Campaign. Vaccines. 2023; 11(5):953. https://doi.org/10.3390/vaccines11050953
Chicago/Turabian StyleAlbayat, Soha, Muna Almaslamani, Hamad Alromaihi, Hayat Khogali, Jesha Mundodan, Jean Joury, and Hammam Haridy. 2023. "Key Lessons from COVID-19: A Narrative Review Describing Qatar’s Multifactorial Approach in Executing a Vaccination Campaign" Vaccines 11, no. 5: 953. https://doi.org/10.3390/vaccines11050953
APA StyleAlbayat, S., Almaslamani, M., Alromaihi, H., Khogali, H., Mundodan, J., Joury, J., & Haridy, H. (2023). Key Lessons from COVID-19: A Narrative Review Describing Qatar’s Multifactorial Approach in Executing a Vaccination Campaign. Vaccines, 11(5), 953. https://doi.org/10.3390/vaccines11050953