
The Social Ecological Model: A Framework for Understanding COVID-19 Vaccine Uptake among Healthcare Workers—A Scoping Review

Abstract
:1. Introduction
2. Methods
2.1. Identifying the Research Questions
- What is the rate of uptake of COVID-19 vaccinations among HCWs?
- What socio-demographic factors are associated with VA or VH among HCWs?
- What factors act as barriers or facilitators for vaccine uptake among HCWs?
2.2. Searching for Relevant Studies
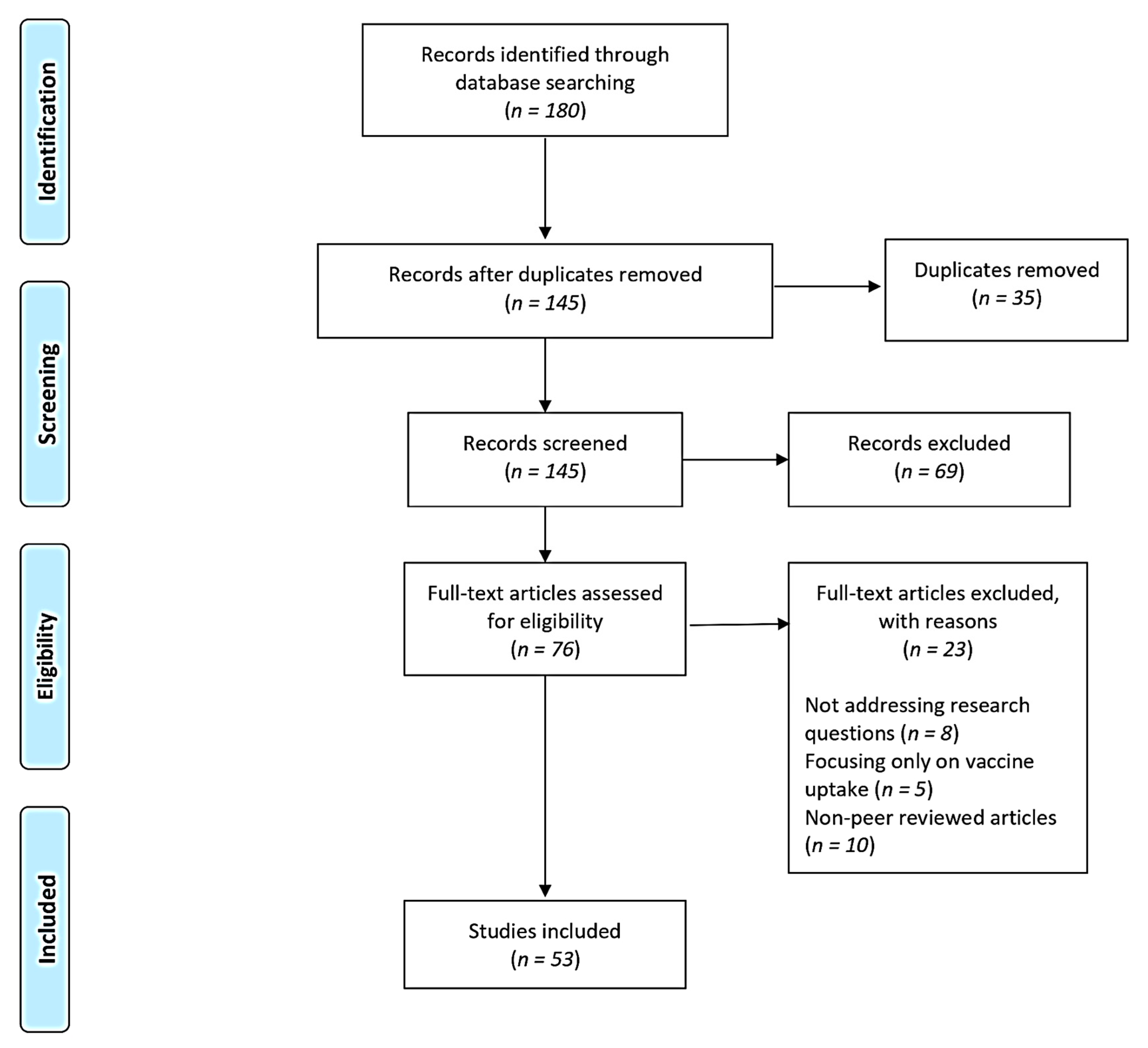
2.3. Study Selection
2.4. Charting Data
2.5. Collating, Summarising, and Reporting the Results
3. Results
3.1. Descriptive Analysis of Articles
3.2. Survey Instruments/Measurement Scales
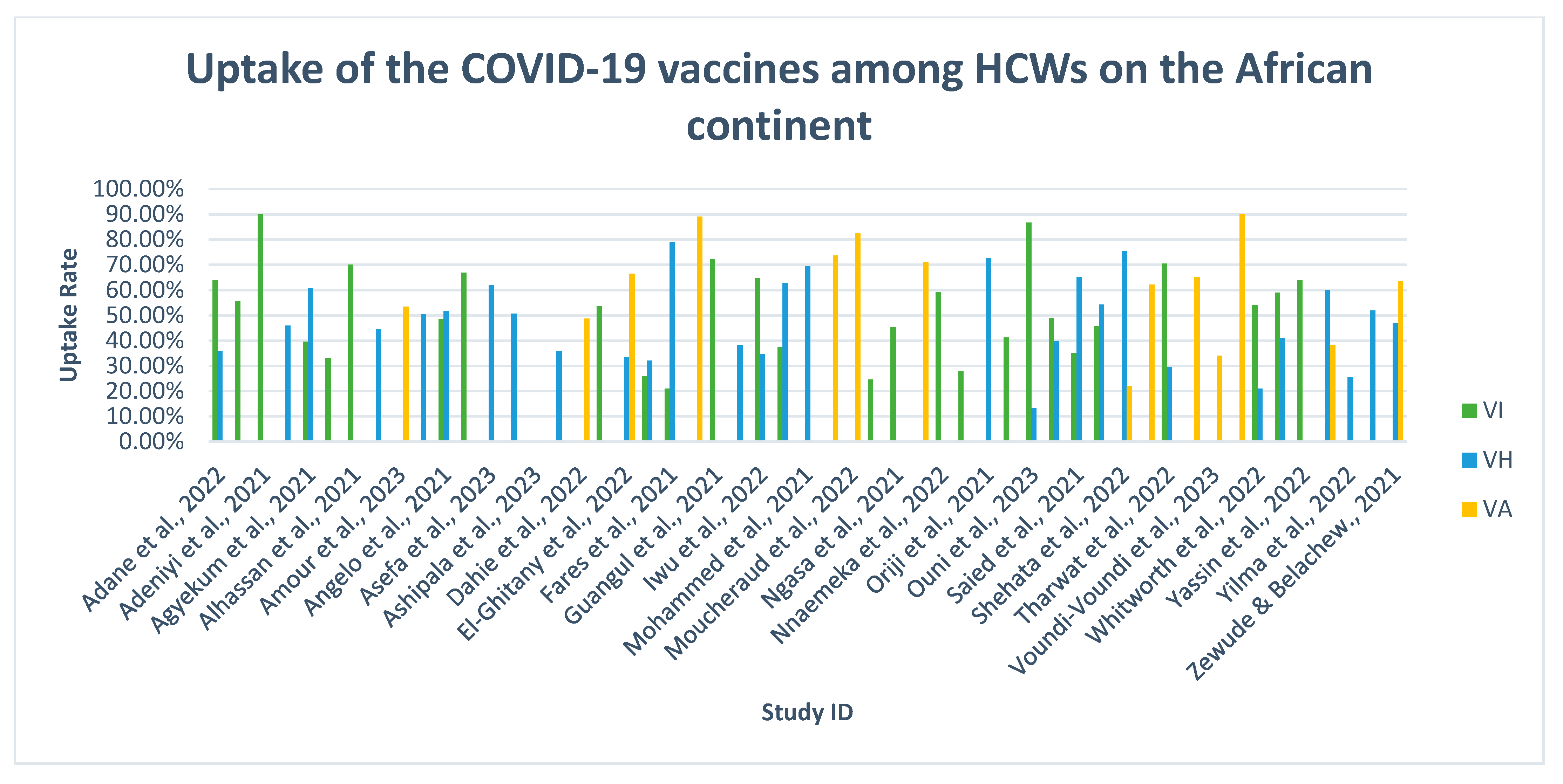
3.3. The Uptake Rate of the COVID-19 Vaccines among HCWs
3.4. Socio-Demographic Determinants Associated with VA or VH
3.5. Barriers and Facilitators Affecting Vaccine Uptake among HCWs
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy

{kind=link}
{kind=link}
| Search Terms | Filters | Results |
|---|---|---|
| kw: COVID-19 vaccine AND | Format: Article | 16 |
| kw: Vaccine Hesitancy AND | ||
| kw: Vaccine acceptance AND | Language: English | |
| kw: Africa AND | ||
| kw: Healthcare workers | Publication Year: 2020–2023 |
| Search Number | Query | Filters | Search Details | Results | Time |
|---|---|---|---|---|---|
| 10 | ((((((COVID-19 vaccines[MeSH Terms]) AND (COVID-19)) AND (vaccines)) OR (covid vaccines)) OR (intention)) OR (vaccine hesitancy)) AND (vaccine acceptance) AND (healthcare workers) AND (Africa) | Full text, Humans, English, from 2020–2023 | (((“covid 19 vaccines” [MeSH Terms] AND (“covid 19” [All Fields] OR “covid 19” [MeSH Terms] OR “covid 19 vaccines” [All Fields] OR “covid 19 vaccines” [MeSH Terms] OR “covid 19 serotherapy” [All Fields] OR “covid 19 nucleic acid testing” [All Fields] OR “covid 19 nucleic acid testing” [MeSH Terms] OR “covid 19 serological testing” [All Fields] OR “covid 19 serological testing” [MeSH Terms] OR “covid 19 testing” [All Fields] OR “covid 19 testing” [MeSH Terms] OR “sars cov 2” [All Fields] OR “sars cov 2” [MeSH Terms] OR “severe acute respiratory syndrome coronavirus 2” [All Fields] OR “ncov” [All Fields] OR “2019 ncov” [All Fields] OR ((“coronavirus” [MeSH Terms] OR “coronavirus” [All Fields] OR “cov” [All Fields]) AND 2019/11/01:3000/12/31[Date—Publication])) AND (“vaccin” [Supplementary Concept] OR “vaccin” [All Fields] OR “vaccination” [MeSH Terms] OR “vaccination” [All Fields] OR “vaccinable” [All Fields] OR “vaccinal” [All Fields] OR “vaccinate” [All Fields] OR “vaccinated” [All Fields] OR “vaccinates” [All Fields] OR “vaccinating” [All Fields] OR “vaccinations” [All Fields] OR “vaccinations” [All Fields] OR “vaccinator” [All Fields] OR “vaccinators” [All Fields] OR “vaccines” [All Fields] OR “vaccined” [All Fields] OR “vaccines” [MeSH Terms] OR “vaccines” [All Fields] OR “vaccine” [All Fields] OR “vaccins” [All Fields])) OR ((“sars cov 2” [MeSH Terms] OR “sars cov 2” [All Fields] OR “covid” [All Fields] OR “covid 19” [MeSH Terms] OR “covid 19” [All Fields]) AND (“vaccin” [Supplementary Concept] OR “vaccin” [All Fields] OR “vaccination” [MeSH Terms] OR “vaccination” [All Fields] OR “vaccinable” [All Fields] OR “vaccinal” [All Fields] OR “vaccinate” [All Fields] OR “vaccinated” [All Fields] OR “vaccinates” [All Fields] OR “vaccinating” [All Fields] OR “vaccinations” [All Fields] OR “vaccinations” [All Fields] OR “vaccinator” [All Fields] OR “vaccinators” [All Fields] OR “vaccines” [All Fields] OR “vaccined” [All Fields] OR “vaccines” [MeSH Terms] OR “vaccines” [All Fields] OR “vaccine” [All Fields] OR “vaccins” [All Fields])) OR (“intention” [MeSH Terms] OR “intention” [All Fields] OR “intent” [All Fields] OR “intentions” [All Fields] OR “intentional” [All Fields] OR “intentioned” [All Fields] OR “intents” [All Fields]) OR (“vaccination hesitancy” [MeSH Terms] OR (“vaccination” [All Fields] AND “hesitancy” [All Fields]) OR “vaccination hesitancy” [All Fields] OR (“vaccine” [All Fields] AND “hesitancy” [All Fields]) OR “vaccine hesitancy” [All Fields])) AND ((“vaccin” [Supplementary Concept] OR “vaccin” [All Fields] OR “vaccination” [MeSH Terms] OR “vaccination” [All Fields] OR “vaccinable” [All Fields] OR “vaccinal” [All Fields] OR “vaccinate” [All Fields] OR “vaccinated” [All Fields] OR “vaccinates” [All Fields] OR “vaccinating” [All Fields] OR “vaccinations” [All Fields] OR “vaccinations” [All Fields] OR “vaccinator” [All Fields] OR “vaccinators” [All Fields] OR “vaccines” [All Fields] OR “vaccined” [All Fields] OR “vaccines” [MeSH Terms] OR “vaccines” [All Fields] OR “vaccine” [All Fields] OR “vaccins” [All Fields]) AND (“accept” [All Fields] OR “acceptabilities” [All Fields] OR “acceptability” [All Fields] OR “acceptable” [All Fields] OR “acceptably” [All Fields] OR “acceptance” [All Fields] OR “acceptances” [All Fields] OR “acceptation” [All Fields] OR “accepted” [All Fields] OR “accepter” [All Fields] OR “accepters” [All Fields] OR “accepting” [All Fields] OR “accepts” [All Fields])) AND (“health personnel” [MeSH Terms] OR (“health” [All Fields] AND “personnel” [All Fields]) OR “health personnel” [All Fields] OR (“healthcare” [All Fields] AND “workers” [All Fields]) OR “healthcare workers” [All Fields]) AND (“africa” [MeSH Terms] OR “africa” [All Fields] OR “africa s” [All Fields] OR “africas” [All Fields])) AND ((fft[Filter]) AND (humans[Filter]) AND (english[Filter]) AND (2020:2023[pdat])) | 41 | 9:28:21 |
| Set No. | Searched for | Databases | Results |
|---|---|---|---|
| S9 | ((factors associated with covid- 19 vaccine hesitancy among HCWs in Africa) AND (location.exact(“Africa” OR “South Africa” OR “Nigeria” OR “Ethiopia” OR “Egypt” OR “Ghana” OR “Uganda” OR “Central Africa” OR “North Africa” OR “Sierra Leone” OR “West Africa” OR “Zambia” OR “Zimbabwe” OR “Burkina Faso” OR “Cape Town South Africa” OR “Congo-Democratic Republic of Congo” OR “East Africa” OR “Eastern Cape South Africa” OR “Kano Nigeria” OR “Kenya” OR “Malawi” OR “Mozambique”) AND at.exact(“Article”) AND la.exact(“ENG”) AND PEER(yes))) AND ((factors associated with covid-19 vaccine uptake among HCWs in Africa) AND (location.exact(“Africa” OR “South Africa” OR “Nigeria” OR “Ethiopia” OR “Egypt” OR “Ghana” OR “Uganda” OR “Central Africa” OR “North Africa” OR “Sierra Leone” OR “West Africa” OR “Zambia” OR “Zimbabwe” OR “Burkina Faso” OR “Cape Town South Africa” OR “Congo-Democratic Republic of Congo” OR “East Africa” OR “Eastern Cape South Africa” OR “Kano Nigeria” OR “Kenya” OR “Malawi” OR “Mozambique”) AND at.exact(“Article”) AND la.exact(“ENG”) AND PEER(yes))) | Coronavirus Research Database, Ebook Central, Health Research Premium Collection, Publicly Available Content Database These databases are searched for part of your query. | 48 |
Appendix B
| Author(s) & Publication Year | Country & Data Collection Period | Methodology |
|---|---|---|
| Adane et al., 2022 [51] | Ethiopia May 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Medical Laboratory Technicians Nurses & Midwives Pharmacists Radiologists Anaesthesiologists Public Health Specialist Non-medical Auxiliary Staff Sample size: 404 Measurement scale: Likert scale |
| Adejumo et al., 2021 [49] | Nigeria October 2020 | Study design: A quantitative cross-sectional study Population target: Physicians Nurses Medical Laboratory Technicians Pharmacists Physiotherapists Other Sample size: 1470 Measurement scale: Dichotomous scale |
| Adeniyi et al., 2021 [52] | South Africa November to December 2020 | Study design: A quantitative cross-sectional study Population target: Physicians Pharmacists Nurses Allied Health Professionals Support Staff Sample size: 1380 Measurement scale: Dichotomous scale |
| Aemro et al., 2021 [53] | Ethiopia May to June 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Pharmacists Nurses Allied Health Professionals Support Staff Sample size: 418 Measurement scale: Dichotomous scale |
| Agyekum et al., 2021 [23] | Ghana January to February 2021 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Allied Health Professionals Physicians Sample size: 234 Measurement scale: Dichotomous scale |
| Ahmed et al., 2021 [54] | Ethiopia January to March 2021 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Psychiatrists Optometrists Physicians Health Officers Anaesthetics Medical Laboratory Technicians Radiologists Physiotherapists Pharmacists Other Sample size: 409 Measurement scale: Dichotomous scale |
| Alhassan et al., 2021 [55] | Ghana September to October 2020 | Study design: A quantitative cross-sectional study Population target: Pharmacists Other Sample size: 1605 Measurement scale: Dichotomous scale |
| Allagoa et al., 2021 [56] | Nigeria April 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Sample size: 182 Measurement scale: Dichotomous scale |
| Amour et al., 2023 [57] | Tanzania October to November 2021 | Study design: A mixed-method study Population target: Physicians Nurses & Midwives Pharmacists Medical Laboratory Technicians Administrative Staff Other Sample size: 1368 |
| Amuzie et al., 2021 [58] | Nigeria March 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Nurses Pharmacists Medical Laboratory Technicians Administrative Staff Allied Health Professionals Sample size: 422 Measurement scale: Dichotomous scale |
| Angelo et al., 2021 [59] | Ethiopia March 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Nurses & Midwives Medical Laboratory Technicians Pharmacist Sample size: 405 Measurement scale: Dichotomous scale |
| Annan et al., 2021 [60] | Ghana | Study design: A quantitative cross-sectional study Population target: Junior Physicians Sample size: 305 Measurement scale: Dichotomous scale |
| Asefa et al., 2023 [61] | Ethiopia July to August 2021 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Medical Laboratory Technicians Pharmacists Sample size: 421 Measurement scale: Dichotomous scale |
| Aseneh et al., 2023 [62] | Multiple countries Cameroon & Nigeria May to June 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Nurses & Midwives Administrative Staff Paramedics Pharmacists CHWs Dentists Medical Laboratory Technicians Nurse Assistants Public Health Specialist Physiotherapists Radiologists Other Sample size: 598 Measurement scale: Dichotomous scale |
| Ashipala et al., 2023 [63] | Namibia September to October 2021 | Study design: A qualitative study Population target: Nurses Sample size: 15 |
| Berhe et al., 2022 [64] | Ethiopia July 2022 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Medical Laboratory Technicians Pharmacist Psychiatrist Environmental Health Specialist Public Health Specialist Others Sample size: 403 Measurement scale: Dichotomous scale |
| Dahie et al., 2022 [65] | Somalia December 2021 to February 2022 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Medical Laboratory Technicians Public Health Specialist Dentist Pharmacist CHWs Nutritionists Other Sample size: 1281 Measurement scale: Dichotomous scale |
| Ekwebene et al., 2021 [66] | Nigeria | Study design: A quantitative cross-sectional study Population target Physicians Nurses Public Health Specialist Radiologist Dentists Optometrist Medical Laboratory Technicians Pharmacists Physiotherapist Cleaners Sample size: 445 Measurement scale: Dichotomous scale |
| El-Ghitany et al., 2022 [67] | Egypt January to June 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Nurses Pharmacist Other Sample size: 2919 Measurement scale: Dichotomous scale |
| El-Sokkary et al., 2021 [46] | Egypt January 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Dentists Pharmacists Others Sample size: 308 Measurement scale: Likert scale |
| Fares et al., 2021 [47] | Egypt December 2020 to January 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Nurses Pharmacists Dentists Physiotherapists Sample size: 385 Measurement scale: Likert scale |
| George et al., 2023 [68] | South Africa August to October 2022 | Study design: A mixed-method study Population target: Nurses Physicians Allied Health Professionals Dentists/Dental Hygienists Paramedics Pharmacists Sample size: 7763 Measurement scale: Dichotomous scale |
| Guangul et al., 2021 [69] | Ethiopia | Study design: A quantitative cross-sectional study Population target: Health Officer/Clinical officer Medical Laboratory Technicians Nurses Pharmacists Physicians Other Sample size: 668 Measurement scale: Dichotomous scale |
| Ibrahim et al., 2023 [70] | Somalia February to March 2022 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Radiologists Medical Laboratory Technicians Sample size: 1476 Measurement scale: Dichotomous scale |
| Iwu et al., 2022 [71] | Nigeria September to October 2021 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Medical Laboratory Technicians Pharmacists Sample size: 347 Measurement scale: Dichotomous scale |
| Kanyike et al., 2021 [72] | Uganda March 2021 | Study design: A quantitative cross-sectional study Population target: Medical students Sample size: 600 Measurement scale: Dichotomous scale |
| Mohammed et al., 2021 [73] | Ethiopia March to July 2021 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Medical Laboratory Technicians Anaesthetic Technicians Pharmacists Radiologists Sample size: 614 Measurement scale: Dichotomous scale |
| Mohammed et al., 2023 [74] | Ghana | Study design: A quantitative cross-sectional study Population target: Physicians Allied Health Professionals Auxiliary Employees Sample size: 424 Measurement scale: Dichotomous scale |
| Moucheraud et al., 2022 [75] | Malawi March to May 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Medical Assistants Nurses HIV Diagnostic Assistants Health Surveillance Assistants Patient Supporter Data Clerks Sample size: 400 Measurement scale: Dichotomous scale |
| Mudenda et al., 2022 [76] | Zambia February to April 2021 | Study design: A quantitative cross-sectional study Population target: Pharmacy students Sample size: 326 Measurement scale: Dichotomous scale |
| Ngasa et al., 2021 [77] | Cameroon April to June 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Medical Students Nurses Medical Laboratory Technicians Public Health Specialist Pharmacists Sample size: 371 Measurement scale: Dichotomous scale |
| Niguse et al., 2023 [78] | Ethiopia October to November 2021 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Radiologists Public Health Specialist Pharmacists Sample size: 390 Measurement scale: Dichotomous scale |
| Nnaemeka et al., 2022 [79] | Nigeria September 2021 & March 2022 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Pharmacists Medical Laboratory Technicians Radiologists Administrative Staff Physiotherapists Sample size: 1268 Measurement scale: Dichotomous scale |
| Nzaji et al., 2020 [80] | The Democratic Republic of Congo March to April 2020 | Study design: A quantitative cross-sectional study Population target: Physicians Nurses Other Sample size: 613 Measurement scale: Dichotomous scale |
| Oriji et al., 2021 [81] | Nigeria April 2021 | Study design: A quantitative cross-sectional study Population target: Nurses Pharmacists Medical Laboratory Technicians Non-clinical officers Sample size: 182 Measurement scale: Likert scale |
| Orok et al., 2022 [25] | Nigeria May to June 2021 | Study design: A quantitative cross-sectional study Population target: Medical students Sample size: 233 Measurement scale: Likert scale |
| Ouni et al., 2023 [82] | Uganda | Study design: A mixed-method study Population target: Nurses & Midwives Physicians Environmental Health Specialist Medical Laboratory Technicians Sample size: 346 |
| Robinson et al., 2021 [83] | Nigeria December 2020 to January 2021 | Study design: A quantitative cross-sectional study Population target: Ancillary Support Staff Dental Technicians Physicians Medical Laboratory Technicians Medical Consultant Nurses & Midwives Optometrists Pharmacist Physiotherapists Primary Healthcare Worker Radiologists Sample size: 1094 Measurement scale: Likert scale |
| Saied et al., 2021 [84] | Egypt January 2021 | Study design: A quantitative cross-sectional study Population target: Medical students Sample size: 2133 Measurement scale: Likert scale |
| Sharaf et al., 2022 [85] | Egypt August to October 2021 | Study design: A quantitative cross-sectional study Population target: Dental teaching staff Sample size: 171 Measurement scale: Likert scale |
| Shehata et al., 2022 [86] | Egypt March to May 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Sample size: 1268 Measurement scale: Dichotomous scale |
| Terefa et al., 2021 [87] | Ethiopia June 2021 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Medical Laboratory Technicians Pharmacists Anaesthetists Psychiatrist Dentists Public Health Specialist Other Sample size: 522 Measurement scale: Dichotomous scale |
| Tharwat et al., 2022 [88] | Egypt August to September 2021 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Administrative Staff Security Officers Radiologist Medical Laboratory Technicians Pharmacists Dentist Sample size: 455 Measurement scale: Likert scale |
| Toure et al., 2022 [43] | Guinea March to August 2021 | Study design: A mixed-method study Population target: General adult population & HCW Nurses & Midwives Medical Laboratory Technicians Physicians Sample size: 7210 (HCWs-3547) Measurement scale: Dichotomous scale |
| Voundi-Voundi et al., 2023 [89] | Cameroon January to March 2022 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Administrative Staff Sample size: 360 |
| Watermeyer et al., 2022 [90] | South Africa September to November 2021 | Study design: A qualitative study Population target: CHW Sample size: 20 |
| Whitworth et al., 2022 [91] | Multiple countries Sierra Leone DRC Uganda April to October 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Nurses & Midwives Clinical Support Staff Medical Laboratory Technicians Pharmacist Non-clinical support staff Sample size: 543 Measurement scale: Likert scale |
| Wiysonge et al., 2022 [48] | South Africa March to May 2021 | Study design: A quantitative cross-sectional study Population target: Admin Support Nurses Other HCWs Physicians Sample size: 395 Measurement scale: Likert scale |
| Yassin et al., 2022 [92] | Sudan April 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Pharmacist Nurses Medical Laboratory Technicians Administrators Others Sample size: 400 Measurement scale: Dichotomous scale |
| Yendewa et al., 2022 [93] | Sierra Leone January to March 2022 | Study design: A quantitative cross-sectional study Population target: Physicians Medical Students Pharmacists Nurses Nursing Students Sample size: 592 Measurement scale: Likert scale |
| Yilma et al., 2022 [50] | Ethiopia February to April 2021 | Study design: A quantitative cross-sectional study Population target: Nurses & Midwives Physicians Medical Laboratory Technicians Pharmacists Cleaners Others Sample size: 1314 Measurement scale: Dichotomous scale |
| Zammit et al., 2022 [94] | Tunisia January 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Dentists Pharmacists Paramedical professionals Sample size: 493 Measurement scale: Dichotomous scale |
| Zewude & Belachew, 2021 [95] | Ethiopia June 2021 | Study design: A quantitative cross-sectional study Population target: Physicians Health officer Administrative Staff Nurse Medical Laboratory Technician Pharmacist Others Sample size: 232 Measurement scale: Dichotomous scale |
References
- Islam, M.S.; Siddique, A.B.; Akter, R.; Tasnim, R.; Sujan, M.S.; Ward, P.R.; Sikder, M.T. Knowledge, Attitudes and Perceptions towards COVID-19 Vaccinations: A Cross-Sectional Community Survey in Bangladesh. BMC Public Health 2021, 21, 1851. [Google Scholar] [CrossRef]
- Ayenigbara, I.O.; Adegboro, J.S.; Ayenigbara, G.O.; Adeleke, O.R.; Olofintuyi, O.O. The challenges to a successful COVID-19 vaccination programme in Africa. Germs 2021, 11, 427–440. [Google Scholar] [CrossRef]
- Massinga Loembé, M.; Nkengasong, J.N. COVID-19 vaccine access in Africa: Global distribution, vaccine platforms, and challenges ahead. Immunity 2021, 54, 1353–1362. [Google Scholar] [CrossRef]
- Ogunleye, O.O.; Godman, B.; Fadare, J.O.; Mudenda, S.; Adeoti, A.O.; Yinka-Ogunleye, A.F.; Ogundele, S.O.; Oyawole, M.R.; Schönfeldt, M.; Rashed, W.M.; et al. Coronavirus Disease 2019 (COVID-19) Pandemic across Africa: Current Status of Vaccinations and Implications for the Future. Vaccines 2022, 10, 1553. [Google Scholar] [CrossRef]
- World Health Organization; AFRO. Africa Steps Up Targeted COVID-19 Vaccination of Most at Risk People. Available online: https://www.afro.who.int/news/africa-steps-targeted-COVID-19-vaccination-most-risk-people (accessed on 20 September 2022).
- Bongers, A.; Riggall, G.; Kokareva, L.; Chin, B. Managing the challenges associated with decreasing demand for COVID-19 vaccination in Central and West Asia. BMJ Global Health 2022, 7, e010066. [Google Scholar] [CrossRef]
- Mutombo, P.N.; Fallah, M.P.; Munodawafa, D.; Kabel, A.; Houeto, D.; Goronga, T.; Mweemba, O.; Balance, G.; Onya, H.; Kamba, R.S.; et al. COVID-19 Vaccine Hesitancy in Africa: A Call to Action. Lancet Glob. Health 2022, 10, e320–e321. [Google Scholar] [CrossRef]
- Afolabi, A.A.; Ilesanmi, O.S. Dealing with Vaccine Hesitancy in Africa: The Prospective COVID-19 Vaccine Context. Pan Afr. Med. J. 2021, 38. [Google Scholar] [CrossRef]
- World Health Organization; AFRO. COVID-19 Vaccination in Africa Increases by Almost Three-Quarters in June 2022. Available online: https://www.afro.who.int/news/COVID-19-vaccination-africa-increases-almost-three-quarters-june-2022 (accessed on 20 September 2022).
- Privor-Dumm, L.; Excler, J.-L.; Gilbert, S.; Karim, S.S.A.; Hotez, P.J.; Thompson, D.; Kim, J.H. Vaccine access, equity and justice: COVID-19 vaccines and vaccination. BMJ Glob. Health 2023, 8, e011881. [Google Scholar] [CrossRef]
- Nchasi, G.; Okonji, O.C.; Jena, R.; Ahmad, S.; Soomro, U.; Kolawole, B.O.; Nawaz, F.A.; Essar, M.Y.; Aborode, A.T. Challenges faced by African healthcare workers during the third wave of the pandemic. Health Sci. Rep. 2022, 5, e893. [Google Scholar] [CrossRef]
- Tessema, G.A.; Kinfu, Y.; Dachew, B.A.; Tesema, A.G.; Assefa, Y.; Alene, K.A.; Aregay, A.F.; Ayalew, M.B.; Bezabhe, W.M.; Bali, A.G.; et al. The COVID-19 Pandemic and Healthcare Systems in Africa: A Scoping Review of Preparedness, Impact and Response. BMJ Glob. Health 2021, 6, e007179. [Google Scholar] [CrossRef]
- World Health Organization; AFRO. COVID-19 Vaccination Roll-Out Stagnates in Africa. Available online: https://www.afro.who.int/news/COVID-19-vaccination-roll-out-stagnates-africa (accessed on 5 November 2022).
- Galagali, P.M.; Kinikar, A.A.; Kumar, V.S. Vaccine Hesitancy: Obstacles and Challenges. Curr. Pediatr. Rep. 2022, 10, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Njoga, E.O.; Awoyomi, O.J.; Onwumere-Idolor, O.S.; Awoyomi, P.O.; Ugochukwu, I.C.I.; Ozioko, S.N. Persisting Vaccine Hesitancy in Africa: The Whys, Global Public Health Consequences and Ways-Out—COVID-19 Vaccination Acceptance Rates as Case-in-Point. Vaccines 2022, 10, 1934. [Google Scholar] [CrossRef] [PubMed]
- Baptista, S.; Naidoo, S.; Suliman, S.; Nepolo, E.; Kanoi, B.N.; Gitaka, J.; Blessing, O.M.; Enany, S. COVID-19 vaccinology landscape in Africa. Front. Immunol. 2022, 13, 95516. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; MacDonald, N.E. How Can a Global Pandemic Affect Vaccine Hesitancy? Expert Rev. Vaccines 2020, 19, 899–901. [Google Scholar] [CrossRef]
- Wang, D.; Chukwu, A.; Mwanyika-Sando, M.; Abubakari, S.W.; Assefa, N.; Madzorera, I.; Hemler, E.C.; Ismail, A.; Lankoande, B.; Mapendo, F.; et al. COVID-19 Vaccine Hesitancy and Its Determinants among Sub-Saharan African Adolescents. PLoS Glob. Public Health 2022, 2, e0000611. [Google Scholar] [CrossRef]
- Persad, G.; Peek, M.E.; Emanuel, E.J. Fairly Prioritizing Groups for Access to COVID-19 Vaccines. JAMA 2020, 324, 1601. [Google Scholar] [CrossRef]
- Pereira, B.; Fehl, A.G.; Finkelstein, S.R.; Jiga-Boy, G.M.; Caserotti, M. Scarcity in COVID-19 vaccine supplies reduces perceived vaccination priority and increases vaccine hesitancy. Psychol. Mark. 2022, 39, 921–936. [Google Scholar] [CrossRef]
- World Health Organization; AFRO. Only 1 in 4 African Health Workers Fully Vaccinated Against COVID-19. Available online: https://www.afro.who.int/news/only-1–4-african-health-workers-fully-vaccinated-against-COVID-19 (accessed on 20 September 2022).
- Agyekum, M.W.; Afrifa-Anane, G.F.; Kyei-Arthur, F.; Addo, B. Acceptability of COVID-19 Vaccination among Health Care Workers in Ghana. Adv. Public Health 2021, 2021, 9998176. [Google Scholar] [CrossRef]
- Cooper, S.; Betsch, C.; Sambala, E.Z.; Mchiza, N.; Wiysonge, C.S. Vaccine hesitancy—A potential threat to the achievements of vaccination programmes in Africa. Hum. Vaccines Immunother. 2018, 14, 2355–2357. [Google Scholar] [CrossRef]
- Orok, E.; Ndem, E.; Daniel, E. Knowledge, attitude and perception of medical students on COVID-19 vaccines: A study carried out in a Nigerian University. Front. Public Health 2022, 10, 942283. [Google Scholar] [CrossRef] [PubMed]
- Nwafor, K.A.; Samuel, N.; Basil-Eze, P.; Chika, A.M.; Irene, N.J.; Joel, A.; Oraeme, S. Evaluation of Government Communication Interventions for Public Trust and Acceptance of the COVID-19 Astrazeneca Vaccine in Ebonyi State, Nigeria. Int. J. Public Health Pharm. Pharmacol. 2020, 5, 25–37. [Google Scholar]
- Adongo, C.A.; Tuoyire, D.A.; Azuug, M.; Appiah, A.B.; Taale, F.; Amadu, I. Decolonising vaccine production: Unpacking Ghanaians’ support for made-in-Africa vaccines. Vaccine X 2023, 14, 100283. [Google Scholar] [CrossRef] [PubMed]
- Makoni, M. Tanzania refuses COVID-19 vaccines. Lancet 2021, 397, 566. [Google Scholar] [CrossRef] [PubMed]
- Yamanis, T.; Carlitz, R.; Gonyea, O.; Skaff, S.; Kisanga, N.; Mollel, H. Confronting ‘chaos’: A qualitative study assessing public health officials’ perceptions of the factors affecting Tanzania’s COVID-19 vaccine rollout. BMJ Open 2023, 13, e065081. [Google Scholar] [CrossRef]
- Al-Jayyousi, G.F.; Sherbash, M.A.M.; Ali, L.A.M.; El-Heneidy, A.; Alhussaini, N.W.Z.; Elhassan, M.E.A.; Nazzal, M.A. Factors Influencing Public Attitudes towards COVID-19 Vaccination: A Scoping Review Informed by the Socio-Ecological Model. Vaccines 2021, 9, 548. [Google Scholar] [CrossRef]
- Thomson, A.; Vallée-Tourangeau, G.; Suggs, L.S. Strategies to increase vaccine acceptance and uptake: From behavioral insights to context-specific, culturally-appropriate, evidence-based communications and interventions. Vaccine 2018, 36, 6457–6458. [Google Scholar] [CrossRef]
- MacDonald, N.E.; Comeau, J.; Dubé, È.; Graham, J.; Greenwood, M.; Harmon, S.; McElhaney, J.; McMurtry, M.C.; Middleton, A.; Steenbeek, A.; et al. Royal society of Canada COVID-19 report: Enhancing COVID-19 vaccine acceptance in Canada. Facets 2021, 6, 184–246. [Google Scholar] [CrossRef]
- Mills, M.; Rahal, C.; Brazel, D.; Yan, J.; Gieysztor, S. COVID-19 Vaccine Deployment: Behaviour, Ethics, Misinformation and Policy Strategies; The Royal Society & The British Academy: London, UK, 2020. [Google Scholar]
- Kilanowski, J.F. Breadth of the socio-ecological model. J. Agromed. 2017, 22, 295–297. [Google Scholar] [CrossRef]
- Rimer, B.K.; Glanz, K. Theory at a Glance: A Guide for Health Promotion Practice; National Cancer Institute: Bethesda, MD, USA; Department of Health and Human Services, National Institutes of Health: Bethesda, MD, USA, 2005.
- Ackah, M.; Ameyaw, L.; Salifu, M.G.; Asubonteng, D.P.A.; Yeboah, C.O.; Annor, E.N.; Ankapong, E.a.K.; Boakye, H. COVID-19 vaccine acceptance among health care workers in Africa: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0268711. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. Prisma Extension for Scoping Reviews (PRISMA-SCR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Classifying Health Workers. Available online: https://www.who.int/publications/m/item/classifying-health-workers (accessed on 23 August 2023).
- Lisy, K.; Porritt, K. Narrative Synthesis: Considerations and challenges. Int. J. Evid. Based Healthc. 2016, 14, 201. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Toure, A.A.; Traore, F.A.; Camara, G.; Magassouba, A.S.; Barry, I.; Kourouma, M.L.; Sylla, Y.; Conte, N.Y.; Cisse, D.; Dioubaté, N.; et al. Facilitators and Barriers to COVID-19 Vaccination among Healthcare Workers and the General Population in Guinea. BMC Infect. Dis. 2022, 22, e1000097. [Google Scholar] [CrossRef]
- Burrell, N.A.; DeAnne, P. (Eds.) The SAGE Encyclopedia of Communication Research Methods; Four Volume Set; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Bhandari, P.; Nikolopoulou, K. What Is a Likert Scale? Guide & Examples. Available online: https://www.scribbr.com/methodology/likert-scale/ (accessed on 1 April 2023).
- El-Sokkary, R.H.; El Seifi, O.S.; Hassan, H.M.; Mortada, E.M.; Hashem, M.K.; Gadelrab, M.R.; Tash, R.M. Predictors of COVID-19 Vaccine Hesitancy among Egyptian Healthcare Workers: A Cross-Sectional Study. BMC Infect. Dis. 2021, 21, 762. [Google Scholar] [CrossRef]
- Fares, S.; Elmnyer, M.M.; Mohamed, S.S.; Elsayed, R. COVID-19 Vaccination Perception and Attitude among Healthcare Workers in Egypt. J. Prim. Care Community Health 2021, 12, 215013272110133. [Google Scholar] [CrossRef]
- Wiysonge, C.S.; Alobwede, S.M.; de Marie, C.; Katoto, P.; Kidzeru, E.B.; Lumngwena, E.N.; Cooper, S.; Goliath, R.; Jackson, A.; Shey, M.S. COVID-19 Vaccine Acceptance and Hesitancy among Healthcare Workers in South Africa. Expert Rev. Vaccines 2022, 21, 549–559. [Google Scholar] [CrossRef]
- Adejumo, O.A.; Ogundele, O.A.; Madubuko, C.R.; Oluwafemi, R.O.; Okoye, O.C.; Okonkwo, K.C.; Owolade, S.S.; Junaid, O.A.; Lawal, O.M.; Enikuomehin, A.C.; et al. Perceptions of the COVID-19 Vaccine and Willingness to Receive Vaccination among Health Workers in Nigeria. Osong Public Health Res. Perspect. 2021, 12, 236. [Google Scholar] [CrossRef]
- Yilma, D.; Mohammed, R.; Abdela, S.G.; Enbiale, W.; Seifu, F.; Pareyn, M.; Liesenborghs, L.; van Griensven, J.; van Henten, S. COVID-19 Vaccine Acceptability among Healthcare Workers in Ethiopia: Do We Practice What We Preach? Trop. Med. Int. Health 2022, 27, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Adane, M.; Ademas, A.; Kloos, H. Knowledge, Attitudes, and Perceptions of COVID-19 Vaccine and Refusal to Receive COVID-19 Vaccine among Healthcare Workers in Northeastern Ethiopia. BMC Public Health 2022, 22, 128. [Google Scholar] [CrossRef] [PubMed]
- Adeniyi, O.V.; Stead, D.; Singata-Madliki, M.; Batting, J.; Wright, M.; Jelliman, E.; Abrahams, S.; Parrish, A. Acceptance of COVID-19 Vaccine among the Healthcare Workers in the Eastern Cape, South Africa: A Cross Sectional Study. Vaccines 2021, 9, 666. [Google Scholar] [CrossRef] [PubMed]
- Aemro, A.; Amare, N.S.; Shetie, B.; Demilew, B.C.; Wassie, M. Determinants of COVID-19 vaccine hesitancy among health care workers in Amhara region referral hospitals, Northwest Ethiopia: A cross-sectional study. Epidemiol. Infect. 2021, 149, e225. [Google Scholar] [CrossRef]
- Ahmed, M.H.; Kanfe, S.G.; Jarso, M. Intention to receive vaccine against COVID-19 and associated factors among health professionals working at public hospitals in resource limited settings. PLoS ONE 2021, 16, e0254391. [Google Scholar] [CrossRef]
- Alhassan, R.K.; Owusu-Agyei, S.; Ansah, E.K.; Gyapong, M. COVID-19 Vaccine Uptake among Health Care Workers in Ghana: A Case for Targeted Vaccine Deployment Campaigns in the Global South. Hum. Resour. Health 2021, 19, 136. [Google Scholar] [CrossRef]
- Allagoa, D.O.; Oriji, P.C.; Oguche, O.I.; Ozori, S.E.; Tekenah, E.S.; Obagah, L. Acceptance of COVID-19 vaccination among doctors in the Federal Medical Centre, Yenagoa, South-South, Nigeria. IOSR J. Dent. Med. Sci. 2021, 20, 60–67. [Google Scholar]
- Amour, M.A.; Mboya, I.B.; Ndumwa, H.P.; Kengia, J.T.; Metta, E.; Njiro, B.J.; Nyamuryekung’e, K.K.; Mhamilawa, L.E.; Shayo, E.H.; Ngalesoni, F.; et al. Determinants of COVID-19 Vaccine Uptake and Hesitancy among Healthcare Workers in Tanzania: A Mixed-Methods Study. COVID 2023, 3, 777–791. [Google Scholar] [CrossRef]
- Amuzie, C.I.; Odini, F.; Kalu, K.N.; Izuka, M.O.; Nwamoh, U.N.; Emma-Ukaegbu, U.; Onyike, G. COVID-19 vaccine hesitancy among healthcare workers and its socio-demographic determinants in Abia State, South-East Nigeria: A cross-sectional study. Pan Afr. Med. J. 2021, 40. [Google Scholar] [CrossRef]
- Angelo, A.T.; Alemayehu, D.S.; Dachew, A.M. Health Care Workers Intention to Accept COVID-19 Vaccine and Associated Factors in Southwestern Ethiopia, 2021. PLoS ONE 2021, 16, e0257109. [Google Scholar] [CrossRef]
- Annan, J.J.; Norman, B.R.; Mensah, B.; Enimil, A.; Kokuro, C. Willingness to Accept Vaccination against SARS-COV-2: A Survey of Junior Doctors. World J. Adv. Res. Rev. 2021, 9, 159–166. [Google Scholar] [CrossRef]
- Asefa, L.; Lemma, H.; Daba, C.; Dhengesu, D.; Ibrahim, M. COVID-19 vaccine acceptance and associated factors among health workers in West Guji zone, Southern Ethiopia: Cross-sectional study. Front. Public Health 2023, 11, 974850. [Google Scholar] [CrossRef]
- Aseneh, J.B.; Agbor, V.N.; Kadia, B.M.; Okolie, E.A.; Ofomata, C.J.; Etombi, C.L.; Ekaney, D.S.M.; Fru, Y.W.J. Factors associated with COVID-19 vaccine hesitancy among healthcare workers in Cameroon and Nigeria: A web-based cross-sectional study. Int. Health, 2023; in press. [Google Scholar] [CrossRef]
- Ashipala, D.O.; Tomas, N.; Tenete, G.C. Barriers and Facilitators Affecting the Uptake of COVID-19 Vaccines: A Qualitative Perspective of Front-line Nurses in Namibia. SAGE Open Nurs. 2023, 9, 237796082311584. [Google Scholar] [CrossRef] [PubMed]
- Berhe, E.T.; Shama, A.T.; Ahmed, M.Z.; Gesesew, H.A.; Ward, P.; Gebremeskel, T.G. Assessment of COVID-19 vaccination refusal among healthcare workers in Ethiopia. Front. Public Health 2022, 10, 929754. [Google Scholar] [CrossRef] [PubMed]
- Dahie, H.A.; Mohamoud, J.H.; Adam, M.A.; Garba, B.; Dirie, N.I.; Nur, M.A.; Mohamed, F.Y. COVID-19 Vaccine Coverage and Potential Drivers of Vaccine Uptake among Healthcare Workers in SOMALIA: A Cross-Sectional Study. Vaccines 2022, 10, 1116. [Google Scholar] [CrossRef] [PubMed]
- Ekwebene, O.C.; Obidile, V.C.; Azubuike, P.C.; Nnamani, C.P.; Dankano, N.E.; Egbuniwe, M.C. COVID-19 Vaccine Knowledge and Acceptability among Healthcare Providers in Nigeria. Int. J. Trop. Dis. Health 2021, 42, 51–60. [Google Scholar] [CrossRef]
- El-Ghitany, E.M.; Ashour, A.; Omran, E.F.; Farghaly, A.G.; Hassaan, M.A.; Azzam, N.F.A.E.-M. COVID-19 vaccine acceptance rates and predictors among the Egyptian general population and Healthcare workers, the intersectionality of age and other factors. Sci. Rep. 2022, 12, 19832. [Google Scholar] [CrossRef]
- George, G.; Nota, P.; Strauss, M.; Lansdell, E.; Peters, R.; Brysiewicz, P.; Nadesan-Reddy, N.; Wassenaar, D. Understanding COVID-19 Vaccine Hesitancy among Healthcare Workers in South Africa. Vaccines 2023, 11, 414. [Google Scholar] [CrossRef]
- Guangul, B.A.; Georgescu, G.; Osman, M.; Reece, R.; Derso, Z.; Bahiru, A.; Azeze, Z.B. Healthcare Workers Attitude towards SARS-COVID-2 Vaccine, Ethiopia. Glob. J. Infect. Dis. Clin. Res. 2021, 7, 43–48. [Google Scholar]
- Ibrahim, A.M.; Hamayoun, M.; Farid, M.; Al-Umra, U.; Shube, M.; Sumaili, K.; Shamalla, L.; Malik, S.M.M.R. COVID-19 Vaccine Acceptance and Hesitancy in Health Care Workers in Somalia: Findings from a Fragile Country with No Previous Experience of Mass Adult Immunization. Vaccines 2023, 11, 858. [Google Scholar] [CrossRef]
- Iwu, C.A.; Ositadinma, P.; Chibiko, V.; Madubueze, U.C.; Uwakwe, K.A.; Oluoha, U.R. Prevalence and Predictors of COVID-19 Vaccine Hesitancy among Health Care Workers in Tertiary Health Care Institutions in a Developing Country: A Cross-Sectional Analytical Study. Hindawi 2022, 2022, 7299092. [Google Scholar] [CrossRef]
- Kanyike, A.M.; Olum, R.; Kajjimu, J.; Ojilong, D.; Akech, G.M.; Nassozi, D.R.; Agira, D.; Wamala, N.K.; Asiimwe, A.; Matovu, D.; et al. Acceptance of the Coronavirus Disease-2019 Vaccine among Medical Students in Uganda. Trop. Med. Health 2021, 49, 37. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, R.; Nguse, T.M.; Habte, B.M.; Fentie, A.M.; Gebretekle, G.B. COVID-19 vaccine hesitancy among Ethiopian healthcare workers. PLoS ONE 2021, 16, e0261125. [Google Scholar] [CrossRef]
- Mohammed, A.; Asumah, M.N.; Padhi, B.K.; Sinha, A.; Mohammed, I.; Jamil, S.; Boasiako, O.A.; Leman, N.; Kabir, R. Predictors of SARS-CoV-2 Vaccine Uptake among Health Professionals: A Cross-Sectional Study in Ghana. Vaccines 2023, 11, 190. [Google Scholar] [CrossRef] [PubMed]
- Moucheraud, C.; Phiri, K.; Whitehead, H.S.; Songo, J.; Lungu, E.; Chikuse, E.; Phiri, S.; Van Oosterhout, J.J.; Hoffman, R.M. Uptake of the COVID-19 vaccine among healthcare workers in Malawi. Int. Health 2022, 15, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Mudenda, S.; Mukosha, M.; Hikaambo, C.N.; Meyer, J.C.; Fadare, J.; Kampamba, M.; Kalungia, A.C.; Munsaka, S.; Okoro, R.N.; Daka, V.; et al. Awareness and acceptance of COVID-19 vaccines and associated factors among pharmacy students in Zambia. Malawi Med. J. 2022, 34, 273–280. [Google Scholar] [CrossRef]
- Ngasa, N.C.; Ngasa, S.N.; Tchouda, L.A.S.; Tanisso, E.; Abanda, C.; Dingana, T.N. Spirituality and other factors associated with COVID-19 Vaccine Acceptance amongst Healthcare Workers in Cameroon. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Niguse, S.; Gebremariam, S.; Terefa, D.R.; Biset, Y.; Mekasha, E.; Meskele, K. Assessment of COVID-19 vaccine take-up and its predictors among healthcare professionals in public hospitals, Addis Ababa, Ethiopia: Facility-based cross-sectional study. Hum. Vaccines Immunother. 2023, 19, 2171181. [Google Scholar] [CrossRef]
- Nnaemeka, V.C.; Onwe, R.O.; Ekwedike, A.L.; Oyedele, O.E.; Tsiterimam, T.S.; Ochepo, O.E.; Nwokoye, N.N.; Ike, A.C. Predictors of COVID-19 Vaccine Acceptance among Healthcare Workers in Nigeria. Vaccines 2022, 10, 1645. [Google Scholar] [CrossRef]
- Nzaji, M.K.; Ngombe, L.K.; Mwamba, G.N.; Ndala, D.B.; Miema, J.M.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.; Musenga, E.M. Acceptability of Vaccination against COVID-19 among Healthcare Workers in the Democratic Republic of the Congo. Pragmatic Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Oriji, P.C.; Allagoa, D.O.; Wagio, T.J.; Obagah, L.; Tekenah, E.S.; Ozori, S.E. Hesitancy of COVID-19 Vaccination among Health Workers (Other than Doctors) in a Tertiary Hospital in South-South, Nigeria. Asian J. Res. Infect. Dis. 2021, 7, 21–31. [Google Scholar] [CrossRef]
- Ouni, P.D.; Namulondo, R.; Wanume, B.; Okia, D.; Olupot, P.O.; Nantale, R.; Matovu, J.K.; Napyo, A.; Lubaale, Y.A.M.; Nshakira, N.; et al. COVID-19 vaccine hesitancy among health workers in rural Uganda: A mixed methods study. Vaccine X 2023, 13, 100260. [Google Scholar] [CrossRef]
- Robinson, E.D.; Wilson, P.; Eleki, B.J.; Wonodi, W. Knowledge, Acceptance, and Hesitancy of COVID-19 Vaccine among Health Care Workers in Nigeria. MGM J. Med. Sci. 2021, 8, 102. [Google Scholar] [CrossRef]
- Saied, S.M.; Saied, E.M.; Kabbash, I.A.; Abdo, S.A. Vaccine Hesitancy: Beliefs and Barriers Associated with COVID-19 Vaccination among Egyptian Medical Students. J. Med. Virol. 2021, 93, 4280–4291. [Google Scholar] [CrossRef]
- Sharaf, M.; Taqa, O.; Mousa, H.; Badran, A. COVID-19 Vaccine Acceptance and Perceptions among Dental Teaching Staff of a Governmental University in Egypt. J. Egypt. Public Health Assoc. 2022, 97, 9. [Google Scholar] [CrossRef]
- Shehata, W.M.; Elshora, A.; Abu-Elenin, M.M. Physicians’ attitudes and acceptance regarding COVID-19 vaccines: A cross-sectional study in mid Delta region of Egypt. Environ. Sci. Pollut. Res. 2021, 29, 15838–15848. [Google Scholar] [CrossRef]
- Terefa, D.R.; Shama, A.T.; Feyisa, B.R.; Desisa, A.E.; Geta, E.; Chego, M.; Edosa, A.T. COVID-19 Vaccine Uptake and Associated Factors Among Health Professionals in Ethiopia. Infect. Drug Resist. 2021, 14, 5531–5541. [Google Scholar] [CrossRef]
- Tharwat, S.; Nassar, D.; Nassar, M.K.; Saad, A.; Hamdy, F. Attitude towards COVID-19 vaccination among healthcare workers: A cross sectional study from Egypt. BMC Health Serv. Res. 2022, 22, 1357. [Google Scholar] [CrossRef]
- Voundi-Voundi, E.; Songue, E.; Voundi-Voundi, J.; Nseme, E.G.; Abba-Kabir, H.; Kamgno, J. Factors associated with COVID-19 vaccine hesitancy among health personnel in Yaounde, Cameroon. Health Sci. Dis. 2023, 24, 23–27. [Google Scholar]
- Watermeyer, J.; Scott, M.; Kapueja, L.; Ware, L.J. To Trust or Not to Trust: An Exploratory Qualitative Study of Personal and Community Perceptions of Vaccines amongst a Group of Young Community Healthcare Workers in Soweto, South Africa. Health Policy Plan. 2022, 37, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Whitworth, H.S.; Kitonsa, J.; Kasonia, K.; Tindanbil, D.; Kafeero, P.; Bangura, J.; Nije, Y.; Tetsa Teta, D.; Greenwood, B.; Kavunga-Membo, H.; et al. COVID-19 Vaccine Acceptability among Healthcare Facility Workers in Sierra Leone, the Democratic Republic of Congo and Uganda: A Multi-Centre Cross-Sectional Survey. Int. J. Public Health 2022, 67, 1605113. [Google Scholar] [CrossRef] [PubMed]
- Yassin, E.O.; Faroug, H.A.; Ishaq, Z.B.; Mustafa, M.M.; Idris, M.M.; Widatallah, S.E.; Abd El-Raheem, G.O.; Suliman, M.Y. COVID-19 Vaccination Acceptance among Healthcare Staff in Sudan, 2021. J. Immunol. Res. 2022, 2022, 3392667. [Google Scholar] [CrossRef] [PubMed]
- Yendewa, S.A.; Ghazzawi, M.; James, P.; Smith, M.; Massaquoi, S.P.; Babawo, L.S.; Deen, G.F.; Russell, J.A.; Samai, M.; Sahr, F.; et al. COVID-19 Vaccine Hesitancy among Healthcare Workers and Trainees in Freetown, Sierra Leone: A Cross-Sectional Study. Vaccines 2022, 10, 757. [Google Scholar] [CrossRef] [PubMed]
- Zammit, N.; Gueder, A.E.; Brahem, A.; Ayouni, I.; Ghammam, R.; Fredj, S.B.; Sridi, C.; Chouchene, A.; Kalboussi, H.; Maalel, O.E.; et al. Studying SARS-CoV-2 vaccine hesitancy among health professionals in Tunisia. BMC Health Serv. Res. 2022, 22, 489. [Google Scholar] [CrossRef]
- Zewude, B.; Belachew, A. Intention to Receive the Second Round of COVID-19 Vaccine among Healthcare Workers in Eastern Ethiopia. Infect. Drug Resist. 2021, 14, 3071–3082. [Google Scholar] [CrossRef]
- Bai, L.; Zhao, Y.; Dong, J.; Liang, S.; Guo, M.; Liu, X.; Wang, X.; Huang, Z.; Sun, X.; Zhang, Z.; et al. Coinfection with Influenza A Virus Enhances SARS-COV-2 Infectivity. Cell Res. 2021, 31, 395–403. [Google Scholar] [CrossRef]
- Li, M.; Luo, Y.; Watson, R.; Zheng, Y.; Ren, J.; Tang, J.; Chen, Y. Healthcare Workers’ (hcws) attitudes and related factors towards COVID-19 vaccination: A rapid systematic review. Postgrad. Med. J. 2021, 99, 520–528. [Google Scholar] [CrossRef]
- Ghare, F.; Meckawy, R.; Moore, M.; Lomazzi, M. Determinants of Acceptance of COVID-19 Vaccination in Healthcare and Public Health Professionals: A Review. Vaccines 2023, 11, 311. [Google Scholar] [CrossRef]
- Gilmore, B.; Ndejjo, R.; Tchetchia, A.; de Claro, V.; Nyamupachitu-Mago, E.; Diallo, A.A.; Lopes, C.A.; Bhattacharyya, S. Community engagement for COVID-19 prevention and Control: A Rapid Evidence Synthesis. BMJ Glob. Health 2020, 5, e003188. [Google Scholar] [CrossRef]
- Bangalee, A.; Bangalee, V. Fake News and Fallacies: Exploring Vaccine Hesitancy in South Africa. S. Afr. Fam. Pract. 2021, 63, 3. [Google Scholar] [CrossRef] [PubMed]
- Zintel, S.; Flock, C.; Arbogast, A.L.; Forster, A.; von Wagner, C.; Sieverding, M. Gender differences in the intention to get vaccinated against COVID-19: A systematic review and meta-analysis. Public Health 2022, 31, 1303–1327. [Google Scholar]
- Naidoo, D.; Meyer-Weitz, A.; Govender, K. Factors Influencing the Intention and Uptake of COVID-19 Vaccines on the African Continent: A Scoping Review. Vaccines 2023, 11, 873. [Google Scholar] [CrossRef] [PubMed]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of Healthcare Workers towards COVID-19 Vaccination: A Survey in France and French-Speaking Parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef]
- Tabacchi, G.; Costantino, C.; Cracchiolo, M.; Ferro, A.; Marchese, V.; Napoli, G.; Palmeri, S.; Raia, D.; Restivo, V.; Siddu, A.; et al. Information Sources and Knowledge on Vaccination in a Population from Southern Italy: The ESCULAPIO Project. Hum. Vaccines Immunother. 2016, 13, 339–345. [Google Scholar] [CrossRef]
- Kestenbaum, L.A.; Feemster, K.A. Identifying and Addressing Vaccine Hesitancy. Pediatr. Ann. 2015, 44, e71–e75. [Google Scholar] [CrossRef]
- Talarek, E.; Chazan, M.; Winiarska, P.; Dembiński, Ł.; Sobierajski, T.; Banaszkiewicz, A. How Attitudes towards Vaccination Change in the Face of an Outbreak. Hum. Vaccines Immunother. 2020, 17, 805–809. [Google Scholar] [CrossRef]
- Mamani-Benito, O.; Farfán-Solís, R.; Huayta-Meza, M.; Tito-Betancur, M.; Morales-García, W.C.; Tarqui, E.E. Effect of religious fatalism and concern about new variants on the acceptance of COVID-19 vaccines. Front. Psychiatry 2023, 14, 1071543. [Google Scholar] [CrossRef]
- Peterson, C.J.; Lee, B.; Nugent, K. COVID-19 vaccination hesitancy among healthcare workers—A review. Vaccines 2022, 10, 948. [Google Scholar] [CrossRef]


| Country of Focus | Number of Studies |
|---|---|
| Ethiopia | 12 |
| Nigeria | 9 |
| South Africa (SA) | 4 |
| Ghana | 4 |
| Tanzania | 1 |
| Namibia | 1 |
| Somalia | 2 |
| Egypt | 7 |
| Uganda | 2 |
| Malawi | 1 |
| Zambia | 1 |
| Cameroon | 2 |
| The Democratic Republic of Congo (DRC) | 1 |
| Guinea | 1 |
| Sudan | 1 |
| Sierra Leone | 1 |
| Tunisia | 1 |
| Multiple African countries | 2 |
| Author(s) & Publication Year | Country | Vaccine Intention (VI) | Vaccine Hesitant (VH) | Vaccine Acceptance (VA) |
|---|---|---|---|---|
| Adane et al., 2022 [51] | Ethiopia | 64.0% | 36.0% | |
| Adejumo et al., 2021 [49] | Nigeria | 55.5% | ||
| Adeniyi et al., 2021 [52] | South Africa | 90.1% | ||
| Aemro et al., 2021 [53] | Ethiopia | 45.9% | ||
| Agyekum et al., 2021 [23] | Ghana | 39.6% | 60.7% | |
| Ahmed et al., 2021 [54] | Ethiopia | 33.2% | ||
| Alhassan et al., 2021 [55] | Ghana | 70.0% | ||
| Allagoa et al., 2021 [56] | Nigeria | 44.5% | ||
| Amour et al., 2023 [57] | Tanzania | 53.4% | ||
| Amuzie et al., 2021 [58] | Nigeria | 50.5% | ||
| Angelo et al., 2021 [59] | Ethiopia | 48.4% | 51.6% | |
| Annan et al., 2021 [60] | Ghana | 66.9% | ||
| Asefa et al., 2023 [61] | Ethiopia | 61.9% | ||
| Aseneh et al., 2023 [62] | Multiple countries Cameroon & Nigeria | 50.7% | ||
| Ashipala et al., 2023 [63] | Namibia | |||
| Berhe et al., 2022 [64] | Ethiopia | 35.8% | ||
| Dahie et al., 2022 [65] | Somalia | 48.7% | ||
| Ekwebene et al., 2021 [66] | Nigeria | 53.5% | ||
| El-Ghitany et al., 2022 [67] | Egypt | 33.5% | 66.5% | |
| El-Sokkary et al., 2021 [46] | Egypt | 26% | 32.1% | |
| Fares et al., 2021 [47] | Egypt | 21% | 79% | |
| George et al., 2023 [68] | South Africa | 89% | ||
| Guangul et al., 2021 [69] | Ethiopia | 72.2% | ||
| Ibrahim et al., 2023 [70] | Somalia | 38.2% | ||
| Iwu et al., 2022 [71] | Nigeria | 64.6% | 34.5% | |
| Kanyike et al., 2021 [72] | Uganda | 37.3% | 62.7% | |
| Mohammed et al., 2021 [73] | Ethiopia | 60.3% | ||
| Mohammed et al., 2023 [74] | Ghana | 73.6% | ||
| Moucheraud et al., 2022 [75] | Malawi | 82.5% | ||
| Mudenda et al., 2022 [76] | Zambia | 24.5% | ||
| Ngasa et al., 2021 [77] | Cameroon | 45.4% | ||
| Niguse et al., 2023 [78] | Ethiopia | 71% | ||
| Nnaemeka et al., 2022 [79] | Nigeria | 59.3% | ||
| Nzaji et al., 2020 [80] | The Democratic Republic of Congo | 27.7% | ||
| Oriji et al., 2021 [81] | Nigeria | 72.5% | ||
| Orok et al., 2022 [25] | Nigeria | 41.2% | ||
| Ouni et al., 2023 [82] | Uganda | 86.7% | 13.3% | |
| Robinson et al., 2021 [83] | Nigeria | 48.8% | 39.7% | |
| Saied et al., 2021 [84] | Egypt | 34.9% | 65.1% | |
| Sharaf et al., 2022 [85] | Egypt | 45.6% | 54.3% | |
| Shehata et al., 2022 [86] | Egypt | 75.5% | 22% | |
| Terefa et al., 2021 [87] | Ethiopia | 62.1% | ||
| Tharwat et al., 2022 [88] | Egypt | 70.5% | 29.5% | |
| Toure et al., 2022 [43] | Guinea | 65% | ||
| Voundi-Voundi et al., 2023 [89] | Cameroon | 34% | ||
| Watermeyer et al., 2022 [90] | South Africa | 90% | ||
| Whitworth et al., 2022 [91] | Multiple countries Sierra Leone DRC Uganda | 53.9% | 21% | |
| Wiysonge et al., 2022 [48] | South Africa | 59% | 41% | |
| Yassin et al., 2022 [92] | Sudan | 63.8% | ||
| Yendewa et al., 2022 [93] | Sierra Leone | 60.1% | 38.3% | |
| Yilma et al., 2022 [50] | Ethiopia | 25.5% | ||
| Zammit et al., 2022 [94] | Tunisia | 51.9% | ||
| Zewude & Belachew, 2021 [95] | Ethiopia | 46.9% | 63.4% |
| Factors | Associated with Hesitancy | Associated with Acceptance |
|---|---|---|
| Gender | Being female [50,55,85,86,89,94] | Being female [47] Being male [23,46,56,65,67,72,74,76,77,79,80,87] |
| Age | Younger [50] <30 years [53,58] <35 years [64] <40 years [73,86,94] | Age [54] >30 years [57] >40 years [65,74,87,94] Older [43,46,48,56] |
| Ethnicity | Amhara [64] | |
| Education level | Tertiary level [50,55,70,86] | Secondary level [43,67] Tertiary level [46,50,52,65,78] |
| Religion | Christian—Pentecostal denomination [71] | Not specified [48] Christian [74] |
| Marital status | Single [58] | Single [72,76] Married [43,77,78] |
| Family status | Being a parent [95] | |
| Pregnancy status | Not being pregnant [43] | |
| Medical condition | Presence of chronic illness [62] | Presence of chronic illness [43,56,59,77] |
| Residential settings | Not specified [65,79] Rural [67] Urban [77] | |
| Cadre | Nurses & midwives [50,58] Physicians [58,84] Medical laboratory technicians [50,64,71] Environmental health specialist [64] Medical students [93] | Not specified [53,73] Nurses & midwives [43,51,65] Physicians [23,48,57,59,61,65,79,80] Clinical health workers [50] Public health specialist [65] Academic staff working in hospitals [87] |
| Income level | Average [58] | Not specified [43,46] |
| Table | Factors | Barriers | Facilitators |
|---|---|---|---|
| Intrapersonal Level | |||
| Vaccine related factors | Vaccine safety | Safety concerns [23,25,33,48,50,51,55,56,57,60,61,65,66,67,68,69,70,72,74,75,76,77,78,81,82,83,84,85,86,88,91,92,95] | Confident in the COVID-19 vaccines [47,52,88] |
| Vaccine efficacy | Concerns about the effectiveness of the vaccine [23,25,65,67,69,70,76,77,78,82,84,85,86,88,92,95] | Belief that the vaccine is effective in protecting against COVID-19 [74] | |
| Vaccine knowledge | Having poor knowledge [66] | ||
| Vaccine perception | Having a negative perception [43] | ||
| Vaccine preference | Prefer to wait for another type of COVID-19 vaccine [70] | ||
| Vaccine necessity | Not a priority [70] | ||
| Vaccine experiences | Experiences of discomfort while receiving the first dose [95] | ||
| Vaccine immunity against COVID-19 | Sufficient immunity with the first dose [95] | ||
| Vaccine vs. alternative treatment | Preferred alternative treatment to the COVID-19 vaccine [61,81,95] | ||
| Vaccine development | Mistrust in science [23,47,55,56,61,66,68,69,70,74,75,77,81,82,85,90,91] | ||
| COVID-19 | Diagnosis of COVID | Prior diagnosis [23,67,91,92] | |
| Susceptibility of contracting COVID | Low perceived susceptibility [23,66,67,78,91] | High perceived susceptibility [25,47,59,63,87,92] | |
| Side-effects of COVID | Previous history of loss of smell & taste [56] | ||
| Protection against COVID | Belief in one’s immune system [65,68,76,77,95] | Requires the vaccine to protect oneself [60,72,74,78,84,88,91] | |
| Psychosocial factors | Chronic illness | Presence of chronic illness [56] | Presence of chronic illness [59] |
| Family planning | Planning pregnancy [67,70,91] | ||
| Religion | Religious beliefs [55,56,61,66,70,81,95] | ||
| Experiences with vaccines | Prior adverse reactions to vaccines [2,61] | ||
| Fear of needles & injections [70] | |||
| Against vaccinations in general [91] | |||
| Interpersonal Level | |||
| Influences | Relationship with colleagues | Being influenced by colleagues [63] | |
| Relationship with family | Requires permission from their family before taking the COVID-19 vaccine [70] | ||
| Disapproval from family [66] | |||
| Desire to protect loved ones [25,60,72,78,84,88,91,92] | |||
| Loss of someone to COVID-19 [55] | |||
| Relationship with religious leaders | Discouragement from Religious leaders [66] | ||
| Organizational Level | |||
| Institutional structures | Government & stakeholders | Lack of trust [25,43,56,57,68,81,90] | |
| Government officials not accepting vaccine uptake [66] | |||
| Vaccine accessibility | COVID-19 vaccine inaccessible [63,65,70,75] | COVID-19 vaccine accessible [63] | |
| Workplace environment | Company policy | To keep working [91] | |
| Leadership & support | Lack of support by employer [66] | ||
| Community Level | |||
| Shared norms & myths | Public health responsibility | To end the pandemic [52,78,91,92] | |
| Access to information | Lack of information [23,25,57,61,63,67,70,78] | ||
| Social media | Subscribing to misinformation or conspiracies [57,60,63,68,70,72,90] | ||
| Policy Level | |||
| Vaccination policies | Travel requirements | Requires the vaccine for future travel [47,60,63] | |
| Vaccination cost | Vaccines are provided free of charge [74,88] | ||
| Mandatory policies | Feeling coerced into accepting vaccines [82,89] | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naidoo, D.; Meyer-Weitz, A.; Govender, K. The Social Ecological Model: A Framework for Understanding COVID-19 Vaccine Uptake among Healthcare Workers—A Scoping Review. Vaccines 2023, 11, 1491. https://doi.org/10.3390/vaccines11091491
Naidoo D, Meyer-Weitz A, Govender K. The Social Ecological Model: A Framework for Understanding COVID-19 Vaccine Uptake among Healthcare Workers—A Scoping Review. Vaccines. 2023; 11(9):1491. https://doi.org/10.3390/vaccines11091491
Chicago/Turabian StyleNaidoo, Damian, Anna Meyer-Weitz, and Kaymarlin Govender. 2023. "The Social Ecological Model: A Framework for Understanding COVID-19 Vaccine Uptake among Healthcare Workers—A Scoping Review" Vaccines 11, no. 9: 1491. https://doi.org/10.3390/vaccines11091491
APA StyleNaidoo, D., Meyer-Weitz, A., & Govender, K. (2023). The Social Ecological Model: A Framework for Understanding COVID-19 Vaccine Uptake among Healthcare Workers—A Scoping Review. Vaccines, 11(9), 1491. https://doi.org/10.3390/vaccines11091491