
Predictors of Acute Kidney Injury (AKI) among COVID-19 Patients at the US Department of Veterans Affairs: The Important Role of COVID-19 Vaccinations
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Population, Design, and Exclusion Criteria
2.2. Outcomes and Follow-Up
2.3. Analysis
3. Role of the Funding Source
4. Results
4.1. Patient Characteristics
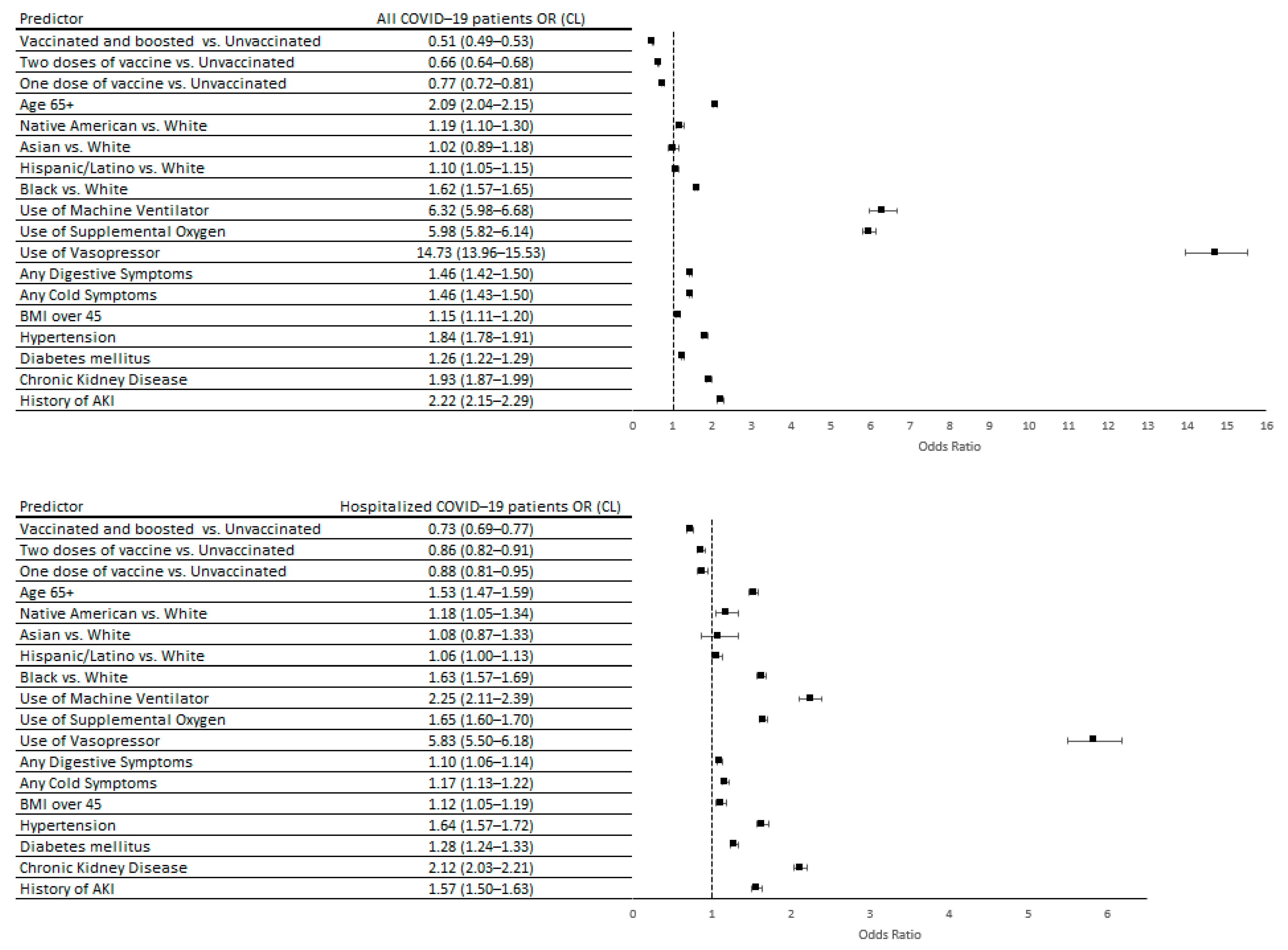
4.2. Predictors of AKI
4.3. Predictors of Mortality
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Birkelo, B.C.; Parr, S.K.; Perkins, A.M.; Greevy, R.A.; Hung, A.M.; Shah, S.C.; Arroyo, J.P.; Denton, J.; Vincz, A.J.; Matheny, M.E.; et al. Comparison of COVID-19 versus influenza on the incidence, features, and recovery from acute kidney injury in hospitalized United States Veterans. Kidney Int. 2021, 100, 894–905. [Google Scholar] [CrossRef]
- Bowe, B.; Cai, M.; Xie, Y.; Gibson, A.K.; Maddukuri, G.; Al-Aly, Z. Acute Kidney Injury in a National Cohort of Hospitalized US Veterans with COVID-19. Clin. J. Am. Soc. Nephrol. 2020, 16, 14–25. [Google Scholar] [CrossRef]
- Fisher, M.; Neugarten, J.; Bellin, E.; Yunes, M.; Stahl, L.; Johns, T.S.; Abramowitz, M.K.; Levy, R.; Kumar, N.; Mokrzycki, M.H.; et al. AKI in Hospitalized Patients with and without COVID-19: A Comparison Study. J. Am. Soc. Nephrol. 2020, 31, 2145–2157. [Google Scholar] [CrossRef]
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D.; Abate, M.; et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef]
- McAdams, M.C.; Xu, P.; Saleh, S.N.; Li, M.; Ostrosky-Frid, M.; Gregg, L.P.; Willett, D.L.; Velasco, F.; Lehmann, C.U.; Hedayati, S.S. Risk Prediction for Acute Kidney Injury in Patients Hospitalized with COVID-19. Kidney Med. 2022, 4, 100463. [Google Scholar] [CrossRef]
- Ng, J.H.; Hirsch, J.S.; Hirsch, A.; Wanchoo, R.; Shah, H.H.; Malieckal, D.A.; Ross, D.W.; Sharma, P.; Sakhiya, V.; Fishbane, S.; et al. Outcomes Among Patients Hospitalized With COVID-19 and Acute Kidney Injury. Am. J. Kidney Dis. 2021, 77, 204–215.e1. [Google Scholar] [CrossRef] [PubMed]
- Robbins-Juarez, S.Y.; Qian, L.; King, K.L.; Stevens, J.S.; Husain, S.A.; Radhakrishnan, J.; Mohan, S. Outcomes for Patients with COVID-19 and Acute Kidney Injury: A Systematic Review and Meta-Analysis. Kidney Int. Rep. 2020, 5, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Nugent, J.; Aklilu, A.; Yamamoto, Y.; Simonov, M.; Li, F.; Biswas, A.; Ghazi, L.; Greenberg, J.H.; Mansour, S.G.; Moledina, D.G.; et al. Assessment of Acute Kidney Injury and Longitudinal Kidney Function After Hospital Discharge Among Patients with and without COVID-19. JAMA Netw. Open 2021, 4, e211095. [Google Scholar] [CrossRef] [PubMed]
- Kolhe, N.V.; Fluck, R.J.; Selby, N.M.; Taal, M.W. Acute kidney injury associated with COVID-19: A retrospective cohort study. PLoS Med. 2020, 17, e1003406. [Google Scholar] [CrossRef] [PubMed]
- Goldfarb, D.S.; Benstein, J.A.; Zhdanova, O.; Hammer, E.; Block, C.A.; Caplin, N.J.; Thompson, N.; Charytan, D.M. Impending Shortages of Kidney Replacement Therapy for COVID-19 Patients. Clin. J. Am. Soc. Nephrol. 2020, 15, 880–882. [Google Scholar] [CrossRef]
- Nadim, M.K.; Forni, L.G.; Mehta, R.L.; Connor, M.J., Jr.; Liu, K.D.; Ostermann, M.; Rimmelé, T.; Zarbock, A.; Bell, S.; Bihorac, A.; et al. COVID-19-associated acute kidney injury: Consensus report of the 25th Acute Disease Quality Initiative (ADQI) Workgroup. Nat. Rev. Nephrol. 2020, 16, 747–764. [Google Scholar] [CrossRef] [PubMed]
- Arentz, M.; Yim, E.; Klaff, L.; Lokhandwala, S.; Riedo, F.X.; Chong, M.; Lee, M. Characteristics and Outcomes of 21 Critically Ill Patients with COVID-19 in Washington State. JAMA 2020, 323, 1612–1614. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.T.; Shao, S.C.; Hsu, C.K.; Wu, I.W.; Hung, M.J.; Chen, Y.C. Incidence of acute kidney injury in COVID-19 infection: A systematic review and meta-analysis. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, P.; Cunha, K.; Neves, P.; Muniz, M.; Gatto, G.; Filho, N.S.; Guedes, F.; Silva, G. Renal Morphology in Coronavirus Disease: A Literature Review. Medicina 2021, 57, 258. [Google Scholar] [CrossRef] [PubMed]
- Silver, S.A.; Beaubien-Souligny, W.; Shah, P.S.; Harel, S.; Blum, D.; Kishibe, T.; Meraz-Munoz, A.; Wald, R.; Harel, Z. The Prevalence of Acute Kidney Injury in Patients Hospitalized with COVID-19 Infection: A Systematic Review and Meta-analysis. Radiology 2020, 3, 83–98.e1. [Google Scholar] [CrossRef] [PubMed]
- Long, J.D.; Strohbehn, I.; Sawtell, R.; Bhattacharyya, R.; Sise, M.E. COVID-19 Survival and its impact on chronic kidney disease. Transl. Res. 2022, 241, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; the Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Winkelmayer, W.C.; Khairallah, P.; Charytan, D.M. Nephrology and COVID-19. JAMA 2020, 324, 1137–1138. [Google Scholar] [CrossRef]
- VINCI, V.I.a.C.I. VA COVID-19 Shared Data Resource. 2020. Available online: https://www.hsrd.research.va.gov/for_researchers/cyber_seminars/archives/3834-notes.pdf (accessed on 31 March 2023).
- Adamczak, M.; Surma, S.; Więcek, A. Acute kidney injury in patients with COVID-19: Epidemiology, pathogenesis and treatment. Adv. Clin. Exp. Med. 2022, 31, 317–326. [Google Scholar] [CrossRef]
- Legrand, M.; Bell, S.; Forni, L.; Joannidis, M.; Koyner, J.L.; Liu, K.; Cantaluppi, V. Pathophysiology of COVID-19-associated acute kidney injury. Nat. Rev. Nephrol. 2021, 17, 751–764. [Google Scholar] [CrossRef]
- Ng, J.H.; Bijol, V.; Sparks, M.A.; Sise, M.E.; Izzedine, H.; Jhaveri, K.D. Pathophysiology and Pathology of Acute Kidney Injury in Patients With COVID-19. Adv. Chronic Kidney Dis. 2020, 27, 365–376. [Google Scholar] [CrossRef]
- Teixeira, J.P.; Barone, S.; Zahedi, K.; Soleimani, M. Kidney Injury in COVID-19: Epidemiology, Molecular Mechanisms and Potential Therapeutic Targets. Int. J. Mol. Sci. 2022, 23, 2242. [Google Scholar] [CrossRef] [PubMed]
- Patil, N.; Kalgotra, P.; Sundaram, S.; Melquist, S.; Parasa, S.; Desai, M.; Sharma, P. Factors Associated with Poor Outcomes Among Patients with SARS-CoV-2 Coronavirus Infection and Gastrointestinal Symptoms. Gastro Hep Adv. 2023, 2, 37–45. [Google Scholar] [CrossRef]
- Shah, M.D.; Sumeh, A.S.; Sheraz, M.; Kavitha, M.S.; Maran, B.A.V.; Rodrigues, K.F. A mini-review on the impact of COVID 19 on vital organs. Biomed. Pharmacother. 2021, 143, 112158. [Google Scholar] [CrossRef]
- Hung, A.M.; Shah, S.C.; Bick, A.G.; Yu, Z.; Chen, H.-C.; Hunt, C.M.; Wendt, F.; Wilson, O.; Greevy, R.A.; Chung, C.P.; et al. APOL1 Risk Variants, Acute Kidney Injury, and Death in Participants with African Ancestry Hospitalized with COVID-19 From the Million Veteran Program. JAMA Intern. Med. 2022, 182, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Mermiri, M.; Mavrovounis, G.; Laou, E.; Papagiannakis, N.; Pantazopoulos, I.; Chalkias, A. Association of vasopressors with mortality in critically ill patients with COVID-19: A systematic review and meta-analysis. Anesthesiol. Perioper. Sci. 2023, 1, 10. [Google Scholar] [CrossRef]
- Zhang, J.; Pang, Q.; Zhou, T.; Meng, J.; Dong, X.; Wang, Z.; Zhang, A. Risk factors for acute kidney injury in COVID-19 patients: An updated systematic review and meta-analysis. Ren. Fail. 2023, 45, 2170809. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.K.; Bergeri, I.; Bresee, J.S.; Cowling, B.J.; Crowcroft, N.S.; Fahmy, K.; Hirve, S.; Kang, G.; Katz, M.A.; Lanata, C.F.; et al. Evaluation of post-introduction COVID-19 vaccine effectiveness: Summary of interim guidance of the World Health Organization. Vaccine 2021, 39, 4013–4024. [Google Scholar] [CrossRef]
- Falahi, S.; Kenarkoohi, A. Host factors and vaccine efficacy: Implications for COVID-19 vaccines. J. Med. Virol. 2022, 94, 1330–1335. [Google Scholar] [CrossRef]
- Chi, W.-Y.; Li, Y.-D.; Huang, H.-C.; Chan, T.E.H.; Chow, S.-Y.; Su, J.-H.; Ferrall, L.; Hung, C.-F.; Wu, T.-C. COVID-19 vaccine update: Vaccine effectiveness, SARS-CoV-2 variants, boosters, adverse effects, and immune correlates of protection. J. Biomed. Sci. 2022, 29, 1–27. [Google Scholar] [CrossRef]
- Fisk, R.J. Barriers to vaccination for coronavirus disease 2019 (COVID-19) control: Experience from the United States. Glob. Health J. 2021, 5, 51–55. [Google Scholar] [CrossRef]
- Limbu, Y.B.; Gautam, R.K.; Pham, L. The Health Belief Model Applied to COVID-19 Vaccine Hesitancy: A Systematic Review. Vaccines 2022, 10, 973. [Google Scholar] [CrossRef] [PubMed]
- Der-Martirosian, C.; Steers, W.N.; Northcraft, H.; Chu, K.; Dobalian, A. Vaccinating Veterans for COVID-19 at the U.S. Department of Veterans Affairs. Am. J. Prev. Med. 2022, 62, e317–e324. [Google Scholar] [CrossRef] [PubMed]
- Wyte-Lake, T.; Manheim, C.; Gillespie, S.M.; Dobalian, A.; Haverhals, L.M. COVID-19 Vaccination in VA Home Based Primary Care: Experience of Interdisciplinary Team Members. J. Am. Med. Dir. Assoc. 2022, 23, 917–922. [Google Scholar] [CrossRef]
- Gin, J.L.; Balut, M.D.; Dobalian, A. COVID-19 Vaccine Hesitancy among U.S. Veterans Experiencing Homelessness in Transitional Housing. Int. J. Environ. Res. Public Health 2022, 19, 15863. [Google Scholar] [CrossRef] [PubMed]
- Gin, J.L.; Kranke, D.A.; Weiss, E.L.; Dobalian, A. Military Culture and Cultural Competence in Public Health: US Veterans and SARS-CoV-2 Vaccine Uptake. J. Humanist. Psychol. 2022. [Google Scholar] [CrossRef]
- NCVAS, N.C.f.V.A.a.S. Department of Veterans Affairs Statistics at a Glance. 2022; pp. 1–6. Available online: https://www.va.gov/vetdata/docs/Quickfacts/Homepage_slideshow_3_31_22.PDF (accessed on 13 January 2023).
- Agha, Z.; Lofgren, R.P.; VanRuiswyk, J.V.; Layde, P.M. Are patients at Veterans Affairs medical centers sicker? A comparative analysis of health status and medical resource use. Arch. Intern. Med. 2000, 160, 3252–3257. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | AKI No. (%) | Non-AKI No. (%) | p-Value | AKI No. (%) | Non-AKI No. (%) | p-Value |
|---|---|---|---|---|---|---|
| All patients | Hospitalized patients | |||||
| Number of patients | 45,754 | 697,045 | 28,573 | 67,000 | ||
| All deaths | 15,747 (34) | 39,712 (6) | <0.0001 | 10,536 (37) | 11,188 (17) | <0.0001 |
| Comorbidities in the past 2 years prior COVID-19 diagnosis | ||||||
| History of AKI | 11,042 (24) | 33,033 (5) | <0.0001 | 7536 (26) | 9646 (14) | <0.0001 |
| History of dialysis | 466 (1) | 1769 (0.3) | <0.0001 | 325 (1) | 403 (0.6) | <0.0001 |
| Chronic kidney disease | 16,468 (36) | 62,469 (9) | <0.0001 | 10,579 (37) | 11,426 (17) | <0.0001 |
| Diabetes mellitus | 25,518 (54) | 184,021 (26) | <0.0001 | 15,399 (54) | 26,465 (40) | <0.0001 |
| Any cardiovascular disease (any CVD) | 26,124 (57) | 187,552 (27) | <0.0001 | 17,138 (60) | 32,974 (49) | <0.0001 |
| Heart failure | 11,516 (25) | 46,114 (7) | <0.0001 | 7881 (28) | 11,539 (17) | <0.0001 |
| Pulmonary heart disease | 2514 (5) | 9891 (2) | <0.0001 | 1794 (5) | 2791 (4) | <0.0001 |
| Chronic lung disease | 18,744 (41) | 174,276 (25) | <0.0001 | 12,232 (43) | 26,658 (40) | <0.0001 |
| Acute respiratory failure | 5934 (5) | 25,665 (1) | <0.0001 | 3993 (13) | 7239 (11) | <0.0001 |
| Chronic obstructive pulmonary disease (COPD) | 12,624 (28) | 86,523 (12) | <0.0001 | 8325 (29) | 17,513 (26) | <0.0001 |
| Hypertension | 38,096 (83) | 353,983 (51) | <0.0001 | 24,121 (84) | 47,534 (71) | <0.0001 |
| Never smoker | 14,782 (35) | 241,802 (42) | <0.0001 | 8973 (34) | 21,326 (35) | <0.0001 |
| Former smoker | 20,773 (49) | 240,948 (42) | <0.0001 | 12,761 (49) | 27,603 (45) | <0.0001 |
| Current smoker | 6703 (15.8) | 92,002 (16.0) | <0.0001 | 4355 (17) | 12,090 (20) | <0.0001 |
| BMI over 45 | 3693 (8) | 48,637 (7) | <0.0001 | 2094 (8) | 4502 (7) | 0.001 |
| Charlson comorbidity index (CCI) ≥ 5 | 13,385 (29) | 49,999 (7) | <0.0001 | 9411 (33) | 13,346 (20) | <0.0001 |
| Symptoms on a day or up to 30 days before COVID-19 diagnosis | ||||||
| Dyspnea | 16,861 (36) | 130,505 (18) | <0.0001 | 13,033 (46) | 26,969 (40) | <0.0001 |
| Any cold symptoms | 27,074 (59) | 291,294 (42) | <0.0001 | 19,695 (69) | 42,584 (64) | <0.0001 |
| Any digestive symptoms | 12,286 (27) | 107,423 (15) | <0.0001 | 9145 (32) | 19,097 (29) | <0.0001 |
| Fever | 15,081(33) | 141,499 (20) | <0.0001 | 11,289 (40) | 24,264 (36) | <0.0001 |
| Nausea | 6732 (15) | 59,327 (9) | <0.0001 | 5029 (18) | 11,007 (16) | <0.0001 |
| Diarrhea | 7601 (17) | 66,333 (10) | <0.0001 | 5632 (20) | 10,571 (17) | <0.0001 |
| COVID-19 complications within 60 days of COVID-19 diagnosis | ||||||
| Emergency department visits within 60 days of COVID-19 diagnosis | 32,896 (72) | 241,577 (35) | <0.0001 | 26,046 (91) | 57,578 (86) | <0.0001 |
| Hospital readmission within 30 days from discharge | 5076 (11) | 6401 (1) | <0.0001 | 5076 (18) | 6401 (10) | <0.0001 |
| Use of vasopressor | 5078 (11) | 3375 (0.5) | <0.0001 | 4975 (17) | 2267 (3) | <0.0001 |
| ICU admission/transfer | 12,531 (28) | 15,053 (2) | <0.0001 | 12,531 (44) | 15,053 (23) | <0.0001 |
| Use of supplemental oxygen | 20,248 (45) | 36,471 (5) | <0.0001 | 20,207 (72) | 36,087 (55) | <0.0001 |
| Use of machine ventilator | 5900 (13) | 5063 (1) | <0.0001 | 5273 (19) | 3420 (5) | <0.0001 |
| Any acute respiratory failure | 21,412 (47) | 38,682 (6) | <0.0001 | 15,258 (54) | 24,089 (36) | <0.0001 |
| Dialysis within 60 days of COVID-19 diagnosis | 1998(5) | 0 | 1669 (6) | 0 | ||
| Chronic kidney failure (CKF) 60 days | 1394 (3) | 96 (0.1) | <0.0001 | 1107 (4) | 64 (0.1) | <0.0001 |
| Demographic characteristics | ||||||
| White | 26,980 (62) | 394,455 (66) | <0.0001 | 16,253 (60) | 42,506 (67) | <0.0001 |
| Black | 12,253 (28) | 127,608 (21) | <0.0001 | 8269 (30) | 14,282 (22) | <0.0001 |
| Hispanic/Latino | 3360 (8) | 61,559 (10) | <0.0001 | 2133 (8) | 5563 (9) | <0.0001 |
| Asian | 274 (0.6) | 7997 (1) | <0.0001 | 168 (0.6) | 465 (0.7) | <0.0001 |
| Native American | 715 (1.6) | 9929 (1.5) | <0.0001 | 421 (1.5) | 958 (1.5) | <0.0001 |
| Males | 43,841 (96) | 562,173 (81) | <0.0001 | 27,458 (96) | 61,992 (93) | <0.0001 |
| Married | 22,169 (49) | 335,804 (53) | <0.0001 | 13,221 (47) | 30,227 (45) | 0.5 |
| Age 65+ | 33,392 (73) | 270,649 (39) | <0.0001 | 21,510 (75) | 41,055 (61) | <0.0001 |
| Year 2020 | 12,725 (28) | 154,376 (22) | <0.0001 | 8431 (30) | 17,204 (27) | <0.0001 |
| Year 2021 | 16,165 (35) | 233,454 (33) | <0.0001 | 9728 (34) | 22,711 (34) | <0.0001 |
| Year 2022 | 16,864 (37) | 309,215 (44) | <0.0001 | 10,414 (36) | 27,085 (40) | <0.0001 |
| Vaccination status | ||||||
| Unvaccinated before COVID-19 diagnosis | 28,130 (61) | 420,794 (60) | <0.0001 | 17,713 (62) | 39,831 (59) | <0.0001 |
| One COVID-19 vaccine before COVID-19 diagnosis | 1921 (4.2) | 30,170 (4.3) | 0.0003 | 1164 (4) | 3039 (5) | <0.0001 |
| Two doses of COVID-19 vaccine before COVID-19 diagnosis | 8388 (18) | 131,568 (19) | <0.0001 | 5136 (18) | 12,426 (19) | 0.001 |
| Vaccinated and boosted before COVID-19 diagnosis | 7315 (15.9) | 114,513 (16.5) | 0.03 | 4508 (16) | 11,704 (1) | <0.0001 |
| Hospitalized COVID-19 pt. | AKI Patients N = 28,573 | Mean/Median (SD) | Non-AKI Patients N = 67,000 | Mean/Median (SD) |
|---|---|---|---|---|
| Age at the time of COVID-19 diagnosis | 28,571 | 71/72 (12.3) | 66,967 | 66/69 (15.1) |
| CCI in the past 2 years | 28,573 | 3.6/3 (2.8) | 67,000 | 2.6/2 (2.6) |
| BMI | 28,508 | 29/28 (7.3) | 66,811 | 29/28 (7.0) |
| Hospital length of stay (LOS) in days | 26,791 | 11.9/8 (13.2) | 58,984 | 7.5/4 (11.0) |
| ICU length of stay (ICULOS) in days | 13,784 | 9.1/6 (10.3) | 19,082 | 5.6/4 (6.9) |
| Acute care length of stay (ACLOS) in days | 22,337 | 8.7/5 (11.0) | 51,451 | 6.5/4 (10.5) |
| Number of days between COVID-19 diagnosis and hospital admission | 27,561 | 3.9/0 (10.2) | 60,917 | 6/0 (12.9) |
| Number of days between COVID-19 diagnosis and ICU admission | 12,349 | 7.1/1 (11.9) | 14,644 | 7.7/1 (13.2) |
| Number of days on a ventilator | 5240 | 10.8/6 (27.6) | 3406 | 8.1/1 (33.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lukowsky, L.R.; Der-Martirosian, C.; Northcraft, H.; Kalantar-Zadeh, K.; Goldfarb, D.S.; Dobalian, A. Predictors of Acute Kidney Injury (AKI) among COVID-19 Patients at the US Department of Veterans Affairs: The Important Role of COVID-19 Vaccinations. Vaccines 2024, 12, 146. https://doi.org/10.3390/vaccines12020146
Lukowsky LR, Der-Martirosian C, Northcraft H, Kalantar-Zadeh K, Goldfarb DS, Dobalian A. Predictors of Acute Kidney Injury (AKI) among COVID-19 Patients at the US Department of Veterans Affairs: The Important Role of COVID-19 Vaccinations. Vaccines. 2024; 12(2):146. https://doi.org/10.3390/vaccines12020146
Chicago/Turabian StyleLukowsky, Lilia R., Claudia Der-Martirosian, Heather Northcraft, Kamyar Kalantar-Zadeh, David S. Goldfarb, and Aram Dobalian. 2024. "Predictors of Acute Kidney Injury (AKI) among COVID-19 Patients at the US Department of Veterans Affairs: The Important Role of COVID-19 Vaccinations" Vaccines 12, no. 2: 146. https://doi.org/10.3390/vaccines12020146
APA StyleLukowsky, L. R., Der-Martirosian, C., Northcraft, H., Kalantar-Zadeh, K., Goldfarb, D. S., & Dobalian, A. (2024). Predictors of Acute Kidney Injury (AKI) among COVID-19 Patients at the US Department of Veterans Affairs: The Important Role of COVID-19 Vaccinations. Vaccines, 12(2), 146. https://doi.org/10.3390/vaccines12020146