
Risk Factors for COVID-19 and Respiratory Tract Infections during the Coronavirus Pandemic

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
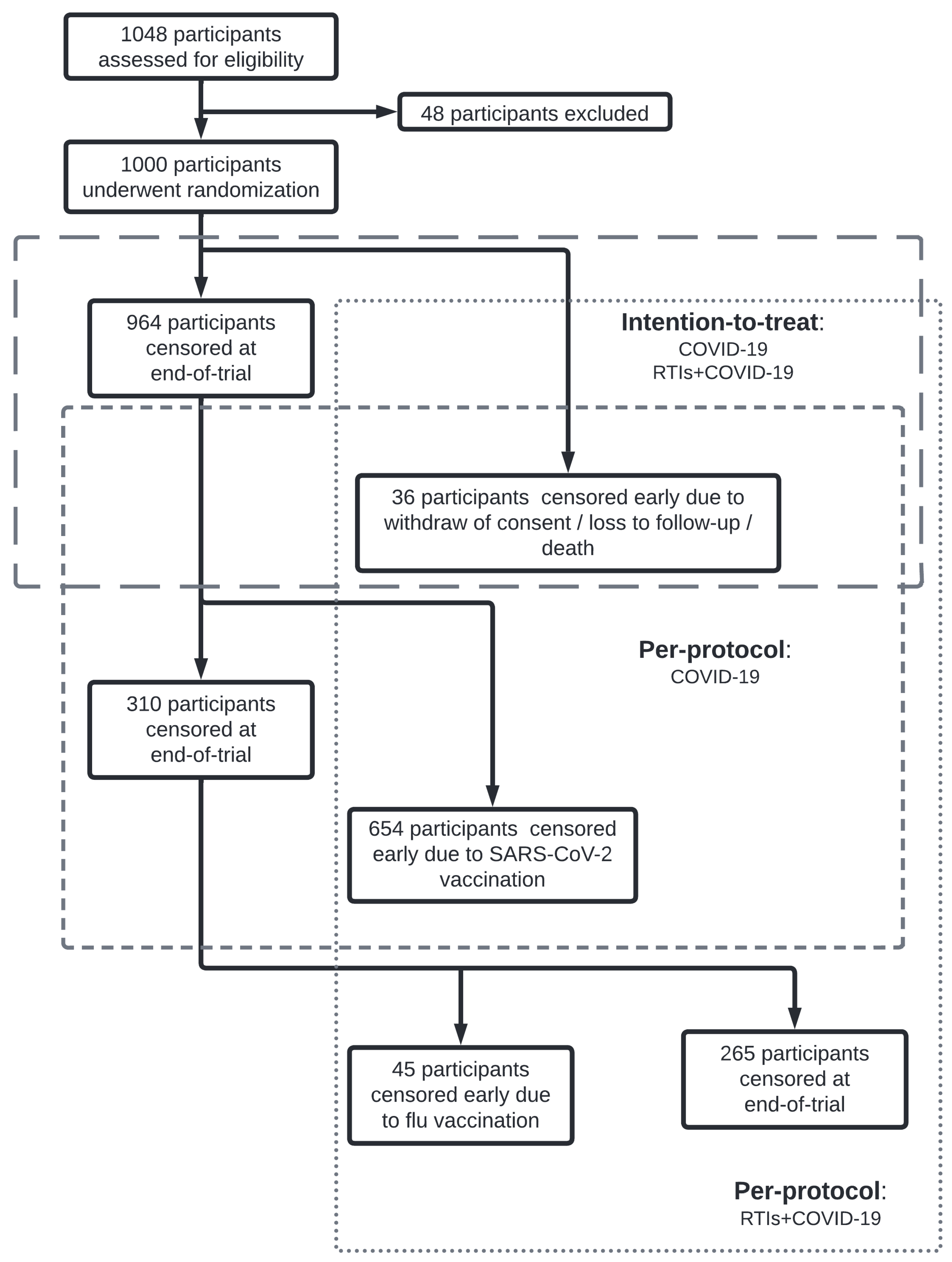
2.1. Study Design and Data Sources
2.2. Statistical Analysis
2.3. Software
3. Results
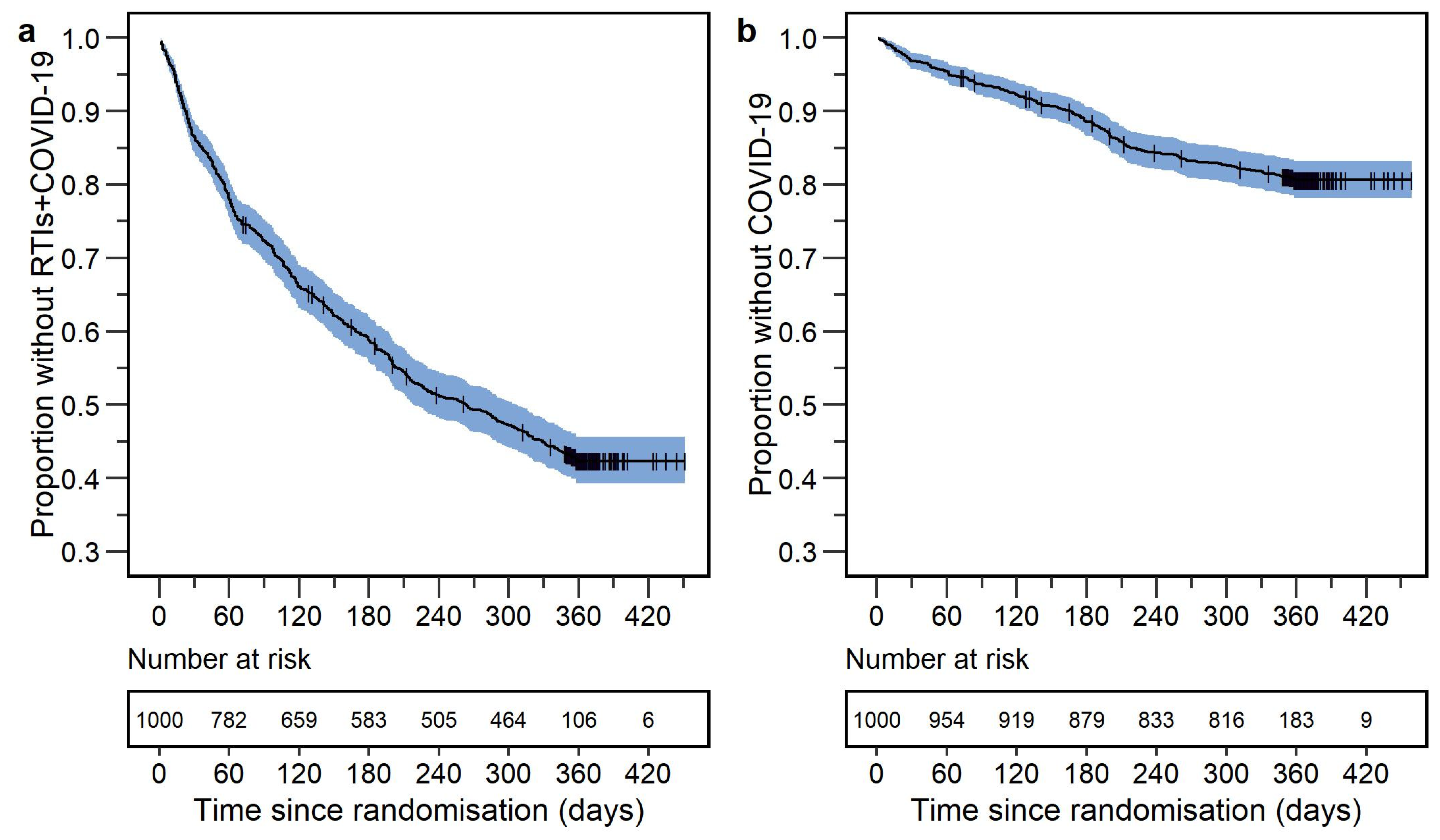
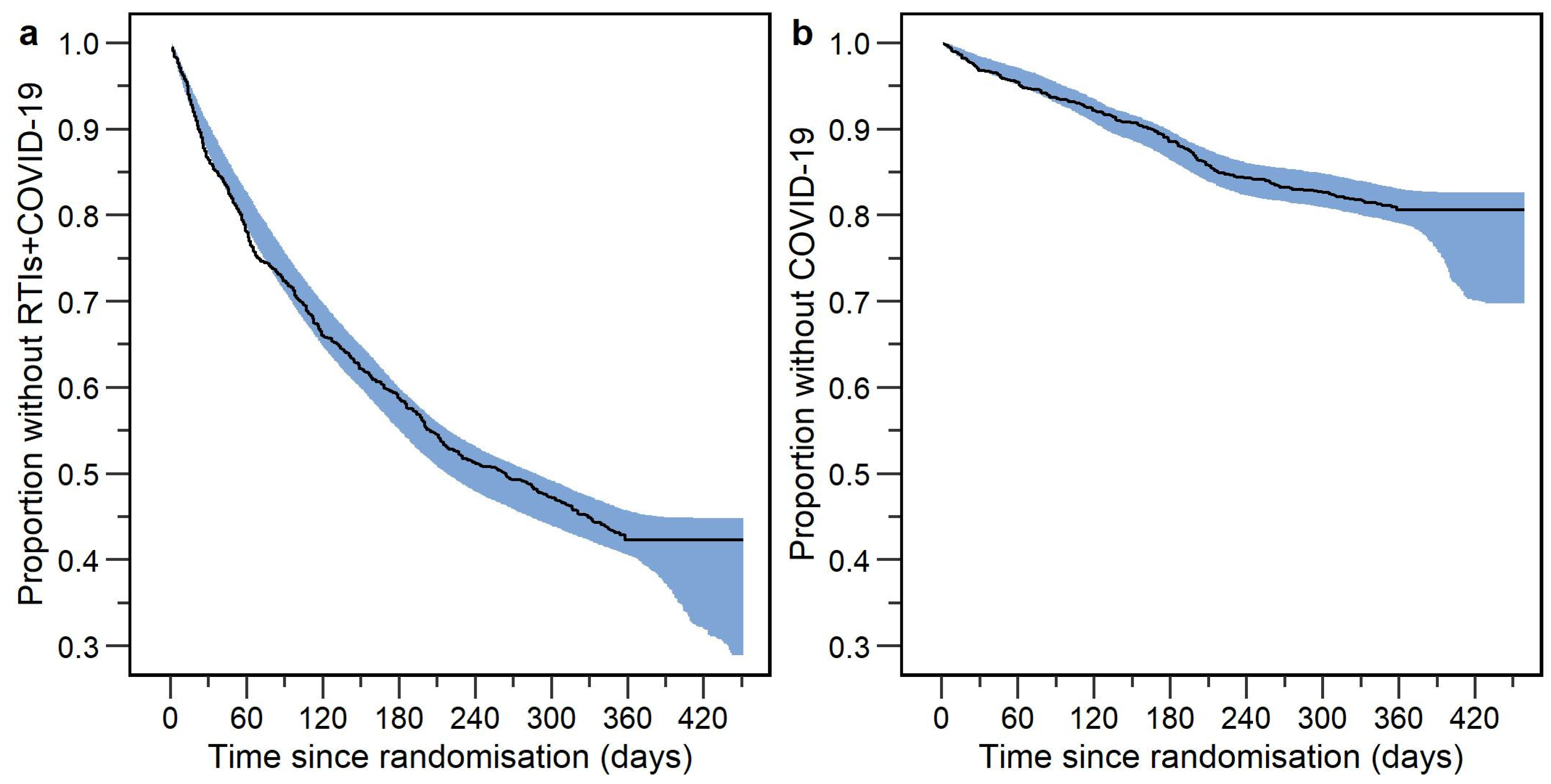
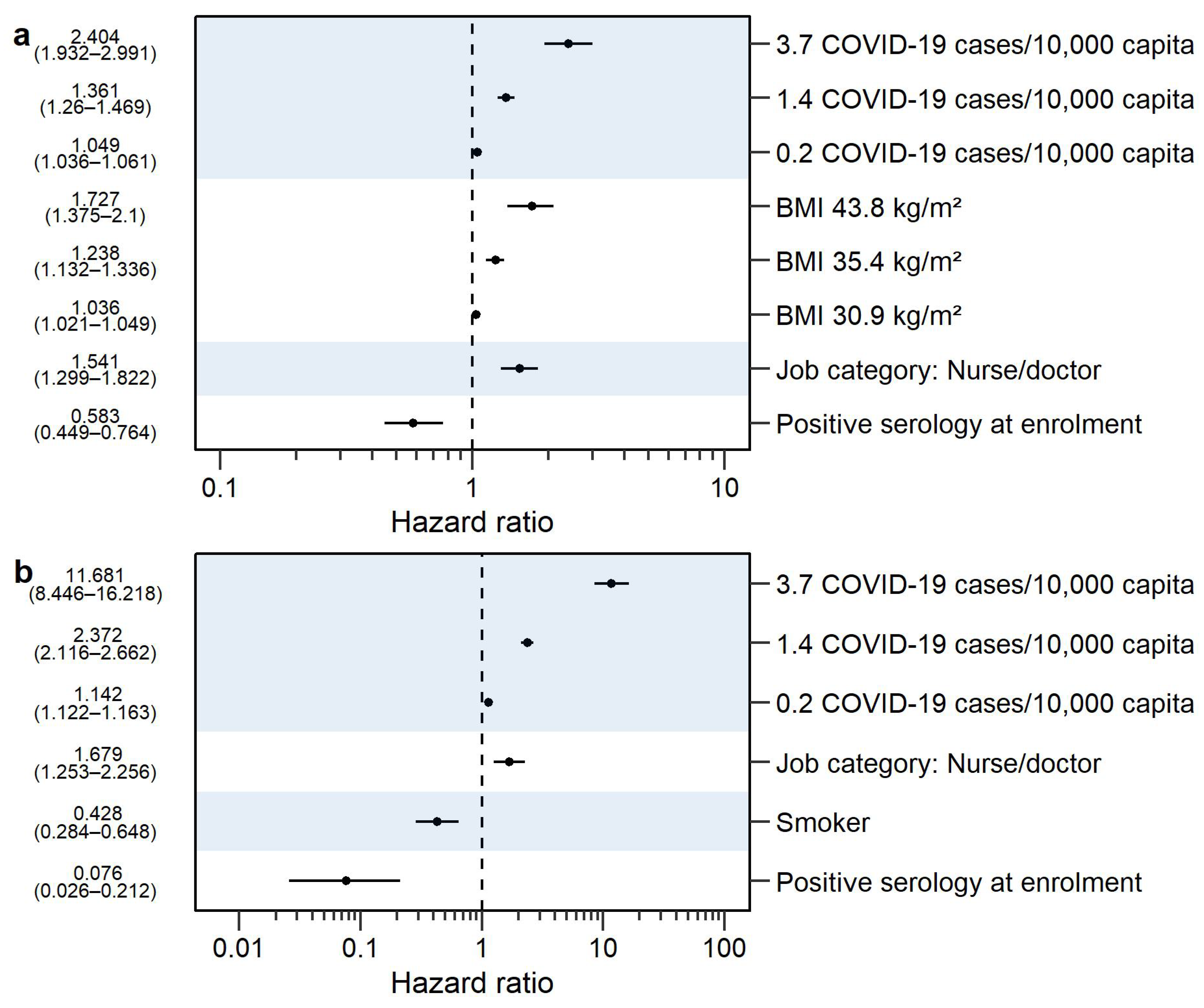
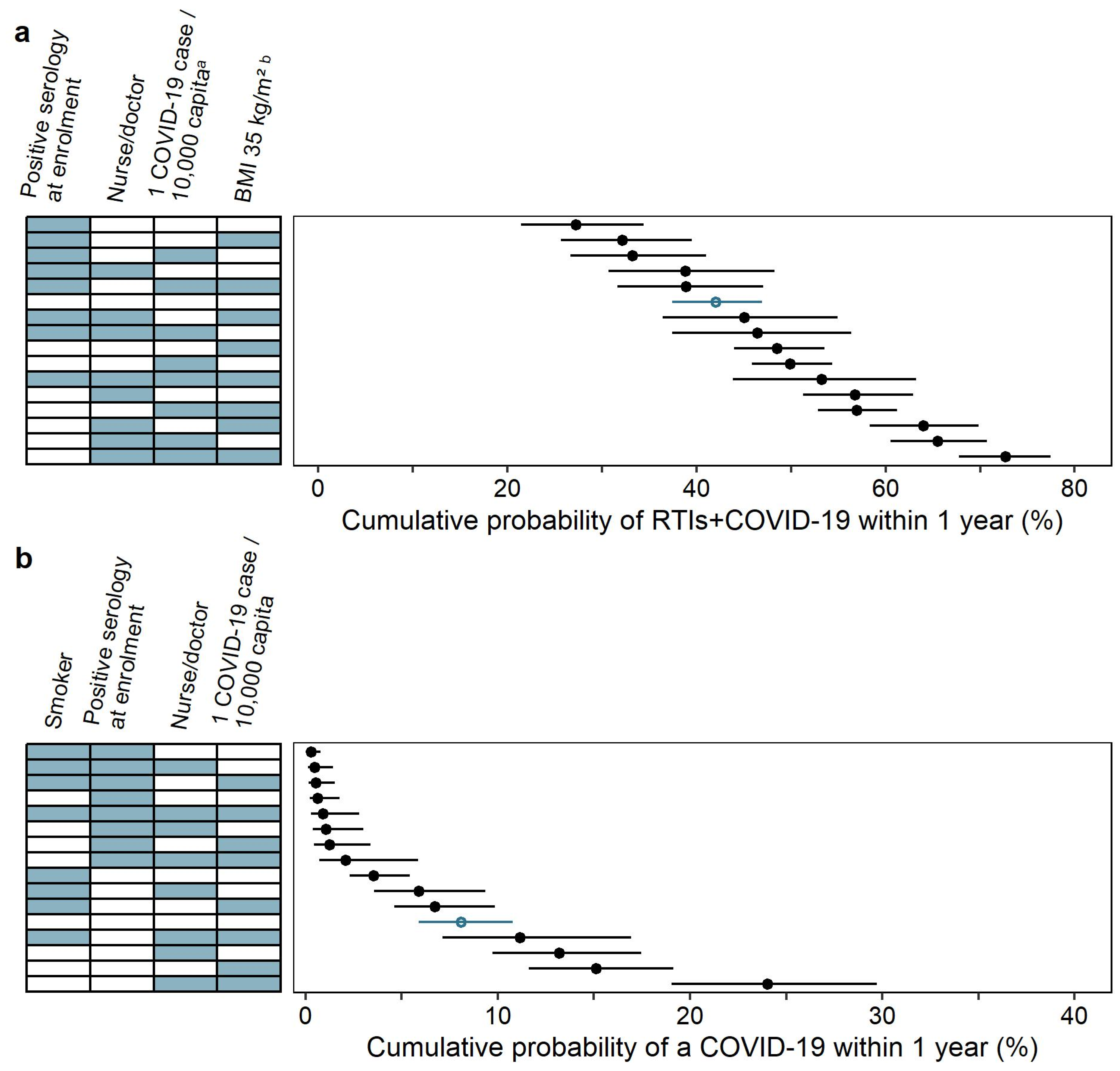
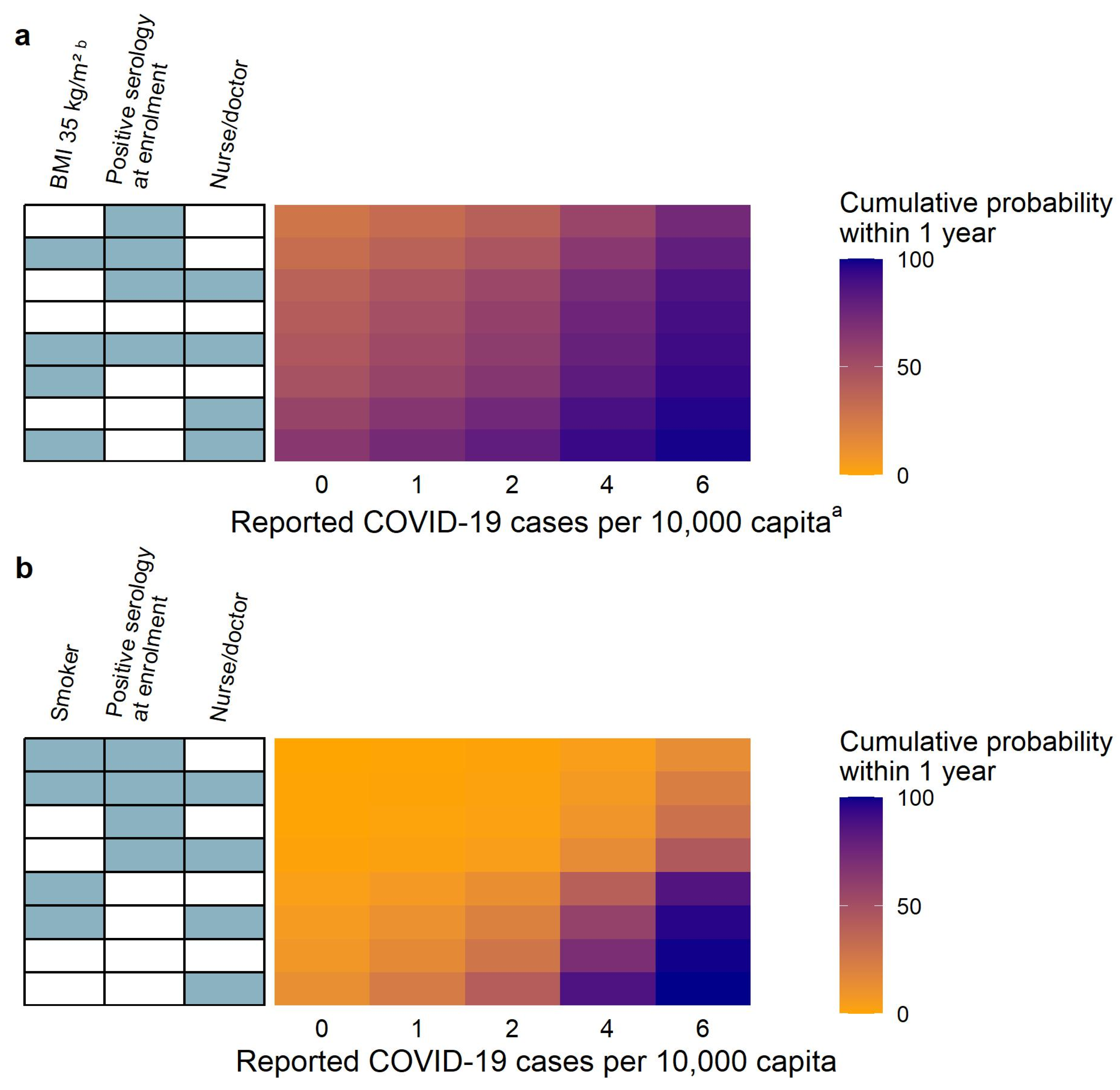
3.1. Respiratory Tract Infections including COVID-19
3.2. COVID-19
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation WHO Coronavirus (COVID-19) Dashboard. Available online: https://data.who.int/dashboards/covid19/cases?n=c (accessed on 18 January 2024).
- CDC Key Facts about Flu Season, Influenza Viruses, How Flu Spreads, and Information for Specific High Risk Groups. Available online: https://www.cdc.gov/flu/about/index.html (accessed on 18 January 2024).
- CDC Tuberculosis Risk Factors. Available online: https://www.cdc.gov/tb/topic/basics/risk.htm (accessed on 17 January 2024).
- Ho, F.K.; Celis-Morales, C.A.; Gray, S.R.; Katikireddi, S.V.; Niedzwiedz, C.L.; Hastie, C.; Ferguson, L.D.; Berry, C.; Mackay, D.F.; Gill, J.M.; et al. Modifiable and Non-Modifiable Risk Factors for COVID-19, and Comparison to Risk Factors for Influenza and Pneumonia: Results from a UK Biobank Prospective Cohort Study. BMJ Open 2020, 10, e040402. [Google Scholar] [CrossRef] [PubMed]
- Shahbazi, F.; Solgi, M.; Khazaei, S. Predisposing Risk Factors for COVID-19 Infection: A Case-Control Study. Casp. J. Intern. Med. 2020, 11, 495–500. [Google Scholar] [CrossRef]
- Beaney, T.; Neves, A.L.; Alboksmaty, A.; Ashrafian, H.; Flott, K.; Fowler, A.; Benger, J.R.; Aylin, P.; Elkin, S.; Darzi, A.; et al. Trends and Associated Factors for COVID-19 Hospitalisation and Fatality Risk in 2.3 Million Adults in England. Nat. Commun. 2022, 13, 2356. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Liang, W.; Zhong, H.; He, J.; Chen, Z.; He, G.; Song, T.; Chen, S.; Wang, P.; Li, J.; et al. Risk Factors Associated with COVID-19 Infection: A Retrospective Cohort Study Based on Contacts Tracing. Emerg. Microbes Infect. 2020, 9, 1546–1553. [Google Scholar] [CrossRef] [PubMed]
- Cordero-Franco, H.F.; De La Garza-Salinas, L.H.; Gomez-Garcia, S.; Moreno-Cuevas, J.E.; Vargas-Villarreal, J.; González-Salazar, F. Risk Factors for SARS-CoV-2 Infection, Pneumonia, Intubation, and Death in Northeast Mexico. Front. Public Health 2021, 9, 645739. [Google Scholar] [CrossRef] [PubMed]
- dos Anjos, L.R.B.; da Costa, A.C.; Cardoso, A.D.R.O.; Guimarães, R.A.; Rodrigues, R.L.; Ribeiro, K.M.; Borges, K.C.M.; Carvalho, A.C.D.O.; Dias, C.I.S.; Rezende, A.D.O.; et al. Efficacy and Safety of BCG Revaccination with M. Bovis BCG Moscow to Prevent COVID-19 Infection in Health Care Workers: A Randomized Phase II Clinical Trial. Front. Immunol. 2022, 13, 841868. [Google Scholar] [CrossRef] [PubMed]
- Bergman, J.; Ballin, M.; Nordström, A.; Nordström, P. Risk Factors for COVID-19 Diagnosis, Hospitalization, and Subsequent All-Cause Mortality in Sweden: A Nationwide Study. Eur. J. Epidemiol. 2021, 36, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Guerrisi, C.; Ecollan, M.; Souty, C.; Rossignol, L.; Turbelin, C.; Debin, M.; Goronflot, T.; Boëlle, P.-Y.; Hanslik, T.; Colizza, V.; et al. Factors Associated with Influenza-like-Illness: A Crowdsourced Cohort Study from 2012/13 to 2017/18. BMC Public Health 2019, 19, 879. [Google Scholar] [CrossRef]
- Baik, I.; Curhan, G.C.; Rimm, E.B.; Bendich, A.; Willett, W.C.; Fawzi, W.W. A Prospective Study of Age and Lifestyle Factors in Relation to Community-Acquired Pneumonia in US Men and Women. Arch. Intern. Med. 2000, 160, 3082–3088. [Google Scholar] [CrossRef]
- Kolditz, M.; Tesch, F.; Mocke, L.; Höffken, G.; Ewig, S.; Schmitt, J. Burden and Risk Factors of Ambulatory or Hospitalized CAP: A Population Based Cohort Study. Respir. Med. 2016, 121, 32–38. [Google Scholar] [CrossRef]
- Ruan, Z.; Qi, J.; Qian, Z.M.; Zhou, M.; Yang, Y.; Zhang, S.; Vaughn, M.G.; LeBaige, M.H.; Yin, P.; Lin, H. Disease Burden and Attributable Risk Factors of Respiratory Infections in China from 1990 to 2019. Lancet Reg. Health—West. Pac. 2021, 11, 100153. [Google Scholar] [CrossRef] [PubMed]
- Atsumi, E.; Yara, S.; Higa, F.; Hirata, T.; Haranaga, S.; Tateyama, M.; Fujita, J. Influence of Human T Lymphotropic Virus Type I Infection on the Etiology of Community-Acquired Pneumonia. Intern. Med. 2009, 48, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Kisiel, M.A.; Zhou, X.; Björnsson, E.; Holm, M.; Dahlman-Höglund, A.; Wang, J.; Svanes, C.; Norbäck, D.; Franklin, K.A.; Malinovschi, A.; et al. The Risk of Respiratory Tract Infections and Antibiotic Use in a General Population and among People with Asthma. ERJ Open Res. 2021, 7, 00429–2021. [Google Scholar] [CrossRef] [PubMed]
- Murphy, V.E.; Powell, H.; Wark, P.A.B.; Gibson, P.G. A Prospective Study of Respiratory Viral Infection in Pregnant Women with and without Asthma. Chest 2013, 144, 420–427. [Google Scholar] [CrossRef]
- Karki, S.; Muscatello, D.J.; Banks, E.; MacIntyre, C.R.; McIntyre, P.; Liu, B. Association between Body Mass Index and Laboratory-Confirmed Influenza in Middle Aged and Older Adults: A Prospective Cohort Study. Int. J. Obes. 2018, 42, 1480–1488. [Google Scholar] [CrossRef] [PubMed]
- Nie, W.; Zhang, Y.; Jee, S.H.; Jung, K.J.; Li, B.; Xiu, Q. Obesity Survival Paradox in Pneumonia: A Meta-Analysis. BMC Med. 2014, 12, 61. [Google Scholar] [CrossRef] [PubMed]
- Maccioni, L.; Weber, S.; Elgizouli, M.; Stoehlker, A.-S.; Geist, I.; Peter, H.-H.; Vach, W.; Nieters, A. Obesity and Risk of Respiratory Tract Infections: Results of an Infection-Diary Based Cohort Study. BMC Public Health 2018, 18, 271. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.-Y.; Forno, E.; Gogna, M.; Celedón, J.C. Obesity and Rhinitis in a Nationwide Study of Children and Adults in the United States. J. Allergy Clin. Immunol. 2016, 137, 1460–1465. [Google Scholar] [CrossRef]
- Cohen, S.; Tyrrell, D.A.; Russell, M.A.; Jarvis, M.J.; Smith, A.P. Smoking, Alcohol Consumption, and Susceptibility to the Common Cold. Am. J. Public Health 1993, 83, 1277–1283. [Google Scholar] [CrossRef]
- Aronson, M.D.; Weiss, S.T.; Ben, R.L.; Komaroff, A.L. Association between Cigarette Smoking and Acute Respiratory Tract Illness in Young Adults. JAMA 1982, 248, 181–183. [Google Scholar] [CrossRef]
- Peytremann, A.; Senn, N.; Mueller, Y. Are Healthcare Workers More Likely than the General Population to Consult in Primary Care for an Influenza-like Illness? Results from a Case-control Study. Influenza Other Respir. Viruses 2020, 14, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.J.; Schweiger, B.; Diner, G.; Gerlach, F.; Haaman, F.; Krause, G.; Nienhaus, A.; Buchholz, U. Seasonal Influenza Risk in Hospital Healthcare Workers Is More Strongly Associated with Household than Occupational Exposures: Results from a Prospective Cohort Study in Berlin, Germany, 2006/07. BMC Infect. Dis. 2010, 10, 8. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.-J.; Lai, C.-C.; Chao, C.-M. Changing Epidemiology of Respiratory Tract Infection during COVID-19 Pandemic. Antibiotics 2022, 11, 315. [Google Scholar] [CrossRef] [PubMed]
- Upton, C.M.; Van Wijk, R.C.; Mockeliunas, L.; Simonsson, U.S.H.; McHarry, K.; van den Hoogen, G.; Muller, C.; von Delft, A.; van der Westhuizen, H.-M.; van Crevel, R.; et al. Safety and Efficacy of BCG Re-Vaccination in Relation to COVID-19 Morbidity in Healthcare Workers: A Double-Blind, Randomised, Controlled, Phase 3 Trial. eClinicalMedicine 2022, 48, 101414. [Google Scholar] [CrossRef] [PubMed]
- CIRCULAR H 102/2020; Western Cape Government Population Data. Western Cape Government: Cape Town, South Africa, 2020.
- van Wijk, R.C.; Mockeliunas, L.; Upton, C.M.; Peter, J.; Diacon, A.H.; Simonsson, U.S.H. Seasonal Influence on Respiratory Tract Infection Severity Including COVID-19 Quantified through Markov Chain Modeling. CPT Pharmacomet. Syst. Pharmacol. 2023, 12, 1250–1261. [Google Scholar] [CrossRef] [PubMed]
- Van Wijk, R.C.; Simonsson, U.S.H. Finding the Right Hazard Function for Time-to-Event Modeling: A Tutorial and Shiny Application. CPT Pharmacomet. Syst. Pharmacol. 2022, 11, 991–1001. [Google Scholar] [CrossRef]
- Wählby, U.; Jonsson, E.N.; Karlsson, M.O. Comparison of Stepwise Covariate Model Building Strategies in Population Pharmacokinetic-Pharmacodynamic Analysis. AAPS PharmSci 2002, 4, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Dosne, A.-G.; Bergstrand, M.; Karlsson, M.O. An Automated Sampling Importance Resampling Procedure for Estimating Parameter Uncertainty. J. Pharmacokinet. Pharmacodyn. 2017, 44, 509–520. [Google Scholar] [CrossRef]
- Goulooze, S.C.; Välitalo, P.A.J.; Knibbe, C.A.J.; Krekels, E.H.J. Kernel-Based Visual Hazard Comparison (kbVHC): A Simulation-Free Diagnostic for Parametric Repeated Time-to-Event Models. AAPS J. 2018, 20, 5. [Google Scholar] [CrossRef]
- van Wijk, R.C.; Mockeliunas, L.; van den Hoogen, G.; Upton, C.M.; Diacon, A.H.; Simonsson, U.S.H. Reproducibility in Pharmacometrics Applied in a Phase III Trial of BCG-Vaccination for COVID-19. Sci. Rep. 2023, 13, 16292. [Google Scholar] [CrossRef]
- R Core Team R: A Language and Environment for Statistical Computing 2020; R Core Team: Vienna, Austria, 2020.
- RStudio Team RStudio: Integrated Development Environment for R 2022; RStudio Team: Boston, MA, USA, 2022.
- Beal, S.; Sheiner, L.; Boeckmann, A.; Bauer, R. NONMEM 7.4 Users Guides 1989; Icon Development Solutions: Ellicott City, MD, USA, 2014. [Google Scholar]
- Jackson, C. Flexsurv: A Platform for Parametric Survival Modeling in R. J. Stat. Softw. 2016, 70, i08. [Google Scholar] [CrossRef] [PubMed]
- Miettinen, O.S. Survival Analysis: Up from Kaplan–Meier–Greenwood. Eur. J. Epidemiol. 2008, 23, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, N.; Nyberg, J. Checklists and Best Practices to Support the Informed Use of Forest Plots to Illustrate the Impact of Covariates in Pharmacometric Models; November 2023; Vol. Poster M-122L. Available online: https://pharmetheus.com/publications/checklists-and-best-practices-to-support-the-informed-use-of-forest-plots-to-illustrate-the-impact-of-covariates-in-pharmacometric-models/ (accessed on 5 January 2024).
- Hall, V.J.; Foulkes, S.; Charlett, A.; Atti, A.; Monk, E.J.M.; Simmons, R.; Wellington, E.; Cole, M.J.; Saei, A.; Oguti, B.; et al. SARS-CoV-2 Infection Rates of Antibody-Positive Compared with Antibody-Negative Health-Care Workers in England: A Large, Multicentre, Prospective Cohort Study (SIREN). Lancet 2021, 397, 1459–1469. [Google Scholar] [CrossRef] [PubMed]
- Paleiron, N.; Mayet, A.; Marbac, V.; Perisse, A.; Barazzutti, H.; Brocq, F.-X.; Janvier, F.; Dautzenberg, B.; Bylicki, O. Impact of Tobacco Smoking on the Risk of COVID-19: A Large Scale Retrospective Cohort Study. Nicotine Tob. Res. 2021, 23, 1398–1404. [Google Scholar] [CrossRef] [PubMed]
- Tsigaris, P.; da Silva, J.A.T. Smoking Prevalence and COVID-19 in Europe. Nicotine Tob. Res. 2020, 22, 1646–1649. [Google Scholar] [CrossRef]
- Killerby, M.E.; Link-Gelles, R.; Haight, S.C.; Schrodt, C.A.; England, L.; Gomes, D.J.; Shamout, M.; Pettrone, K.; O’Laughlin, K.; Kimball, A.; et al. Characteristics Associated with Hospitalization Among Patients with COVID-19—Metropolitan Atlanta, Georgia, March–April 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 790–794. [Google Scholar] [CrossRef] [PubMed]
- Karanasos, A.; Aznaouridis, K.; Latsios, G.; Synetos, A.; Plitaria, S.; Tousoulis, D.; Toutouzas, K. Impact of Smoking Status on Disease Severity and Mortality of Hospitalized Patients with COVID-19 Infection: A Systematic Review and Meta-Analysis. Nicotine Tob. Res. 2020, 22, 1657–1659. [Google Scholar] [CrossRef]
- Chimsimbe, M.; Mucheto, P.; Gombe, N.T.; Govha, E.; Juru, T.P.; Omondi, M.; Tshimanga, M. Factors Associated with Contracting Severe Acute Respiratory Syndrome Corona Virus Type-2 in Norton Town, Zimbabwe, 2021: A Case-Control Study. J. Interv. Epidemiol. Public Health 2022, 5, 9. [Google Scholar] [CrossRef]
- Albani, V.; Loria, J.; Massad, E.; Zubelli, J. COVID-19 Underreporting and Its Impact on Vaccination Strategies. BMC Infect. Dis. 2021, 21, 1111. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | Unit | All Patients |
|---|---|---|
| Number of participants | n | 1000 |
| Gender (biological) female | n (%) | 704 (70.4%) |
| Age (median [IQR]) | years | 39 (30–49) |
| BMI (median [IQR]) | kg/m2 | 28.6 (24.1–34.6) |
| Job description | n (%) | |
| Nurse | 165 (16.5%) | |
| Doctor | 144 (14.4%) | |
| Essential worker | 691 (69.1%) | |
| Hypertension | n (%) | 174 (17.4%) |
| Asthma | n (%) | 68 (6.8%) |
| Diabetes mellitus | n (%) | 63 (6.3%) |
| Cardiovascular disease | n (%) | 24 (2.4%) |
| Self-reported smoker | n (%) | 274 (27.4%) |
| Latent tuberculosis infection | n (%) | 485 (48.5%) |
| Conversion from negative baseline to positive IGRA a | n (%) | 49 (4.9%) |
| Conversion from positive baseline to negative IGRA a | n (%) | 62 (6.2%) |
| Positive SARS-CoV-2 IgG serology at enrollment | n (%) | 153 (15.3%) |
| Self-reported expected exposure to COVID-19 patients | n (%) | 628 (62.8%) |
| South Africa District | n (%) | |
| Cape Town | 950 (95.0%) | |
| Garden Route | 50 (5.0%) |
| Parameter | Description | Estimate | RSE% | 95% CI a |
|---|---|---|---|---|
| Respiratory tract infections including COVID-19 | ||||
| λ | Scale factor in the Gompertz function | 2.679 × 10−3 | 10 | 2.282 × 10−3–3.189 × 10−3 |
| α | Shape factor in the Gompertz function | −3.609 × 10−3 | 23 | −4.467 × 10−3–−2.761 × 10−3 |
| Reported COVID-19 burden influence on the hazard | 0.237 | 13 | 0.178–0.296 | |
| Nurse/doctor job category influence on the hazard | 0.434 | 20 | 0.262–0.599 | |
| Positive SARS-CoV-2 IgG serology at enrollment influence on the hazard | −0.539 | 26 | −0.801–−0.269 | |
| BMI > 30 influence on the hazard | 3.972 × 10−2 | 20 | 2.303 × 10−2–5.366 × 10−2 | |
| COVID-19 | ||||
| λ | Scale factor in the Gompertz function | 4.231 × 10−4 | 17 | 2.854 × 10−4–4.651 × 10−4 |
| α | Shape factor in the Gompertz function | −3.666 × 10−3 | 22 | −5.186 × 10−3–2.493 × 10−3 |
| Reported COVID-19 burden influence on the hazard | 0.669 | 6 | 0.577–0.753 | |
| Nurse/doctor job category influence on the hazard | 0.515 | 29 | 0.226–0.814 | |
| Positive SARS-CoV-2 IgG serology at enrollment influence on the hazard | −2.580 | 23 | −3.657–−1.553 | |
| Smoking influence on the hazard | −0.843 | 24 | −1.257–−0.434 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mockeliunas, L.; van Wijk, R.C.; Upton, C.M.; Peter, J.; Diacon, A.H.; Simonsson, U.S.H. Risk Factors for COVID-19 and Respiratory Tract Infections during the Coronavirus Pandemic. Vaccines 2024, 12, 329. https://doi.org/10.3390/vaccines12030329
Mockeliunas L, van Wijk RC, Upton CM, Peter J, Diacon AH, Simonsson USH. Risk Factors for COVID-19 and Respiratory Tract Infections during the Coronavirus Pandemic. Vaccines. 2024; 12(3):329. https://doi.org/10.3390/vaccines12030329
Chicago/Turabian StyleMockeliunas, Laurynas, Rob C. van Wijk, Caryn M. Upton, Jonathan Peter, Andreas H. Diacon, and Ulrika S. H. Simonsson. 2024. "Risk Factors for COVID-19 and Respiratory Tract Infections during the Coronavirus Pandemic" Vaccines 12, no. 3: 329. https://doi.org/10.3390/vaccines12030329
APA StyleMockeliunas, L., van Wijk, R. C., Upton, C. M., Peter, J., Diacon, A. H., & Simonsson, U. S. H. (2024). Risk Factors for COVID-19 and Respiratory Tract Infections during the Coronavirus Pandemic. Vaccines, 12(3), 329. https://doi.org/10.3390/vaccines12030329