The Impact of Mandatory Vaccination Law in Italy on MMR Coverage Rates in Two of the Largest Italian Regions (Emilia-Romagna and Sicily): An Effective Strategy to Contrast Vaccine Hesitancy

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
- RER: 1 dose at the 13th month, and the second dose at 6 years;
- SR: 1 dose at the 13–15th month, and the second at 5–6 years.
2.1. Data Collection in Emilia-Romagna Region
- Romagna: Local Health Authorities of Forlì-Cesena, Ravenna, Rimini;
- North Emilia: Local Heath Authorities of Piacenza, Parma, Reggio Emilia, Modena;
- Central Emilia: Local Health Authorities of Bologna, Imola, Ferrara.
2.2. Data Collection in Sicily Region
- Western Sicily: Local Health Authorities of Agrigento, Caltanissetta, Palermo, Trapani;
- Eastern Sicily: Local Health Authorities of Catania, Enna, Messina, Siracusa, Ragusa.
2.3. Statistical Analysis
3. Results
3.1. Vaccine Coverage at 24 Months (First Dose)
3.2. Vaccine Coverage in Childhood (Second Dose)
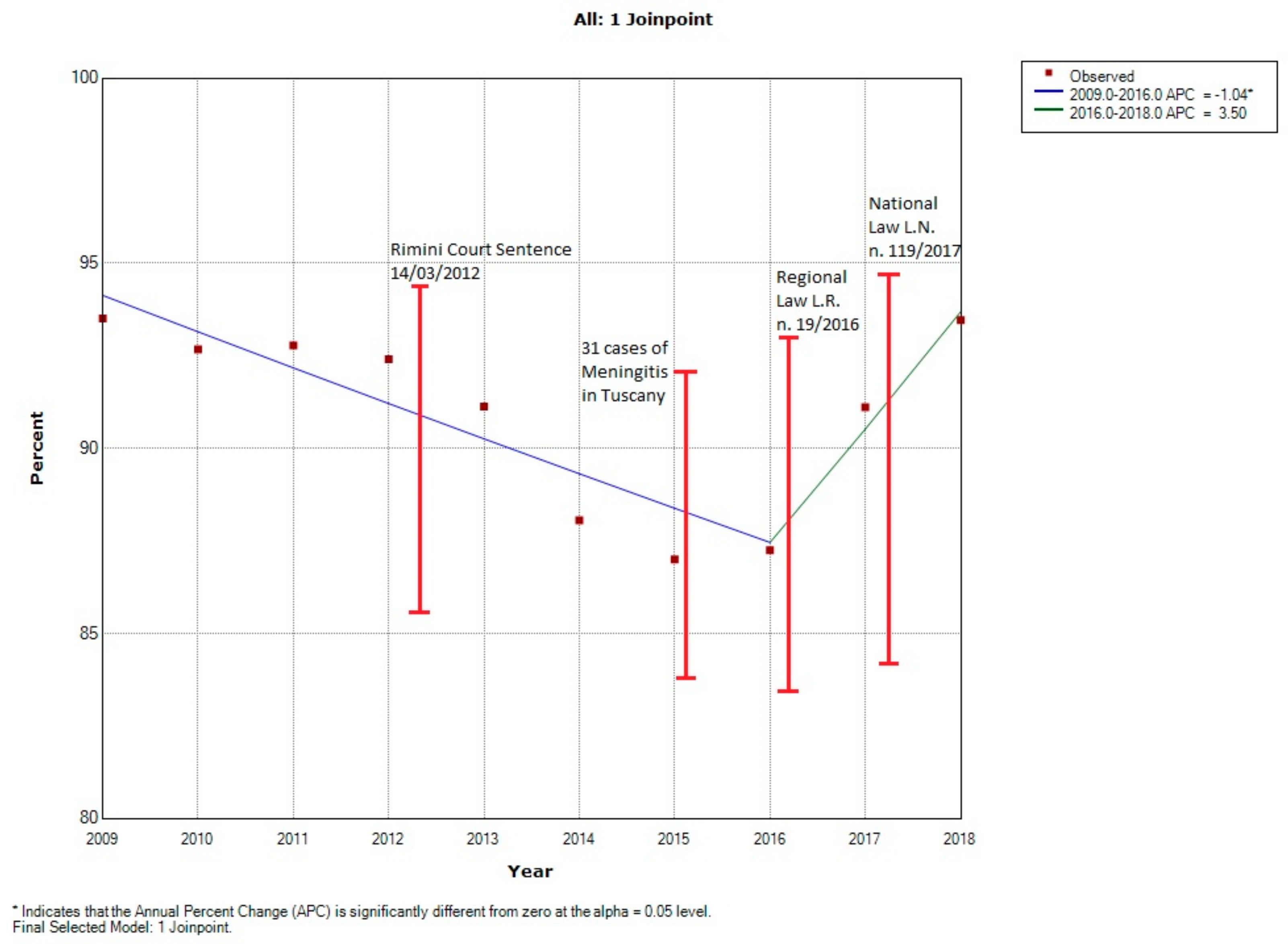
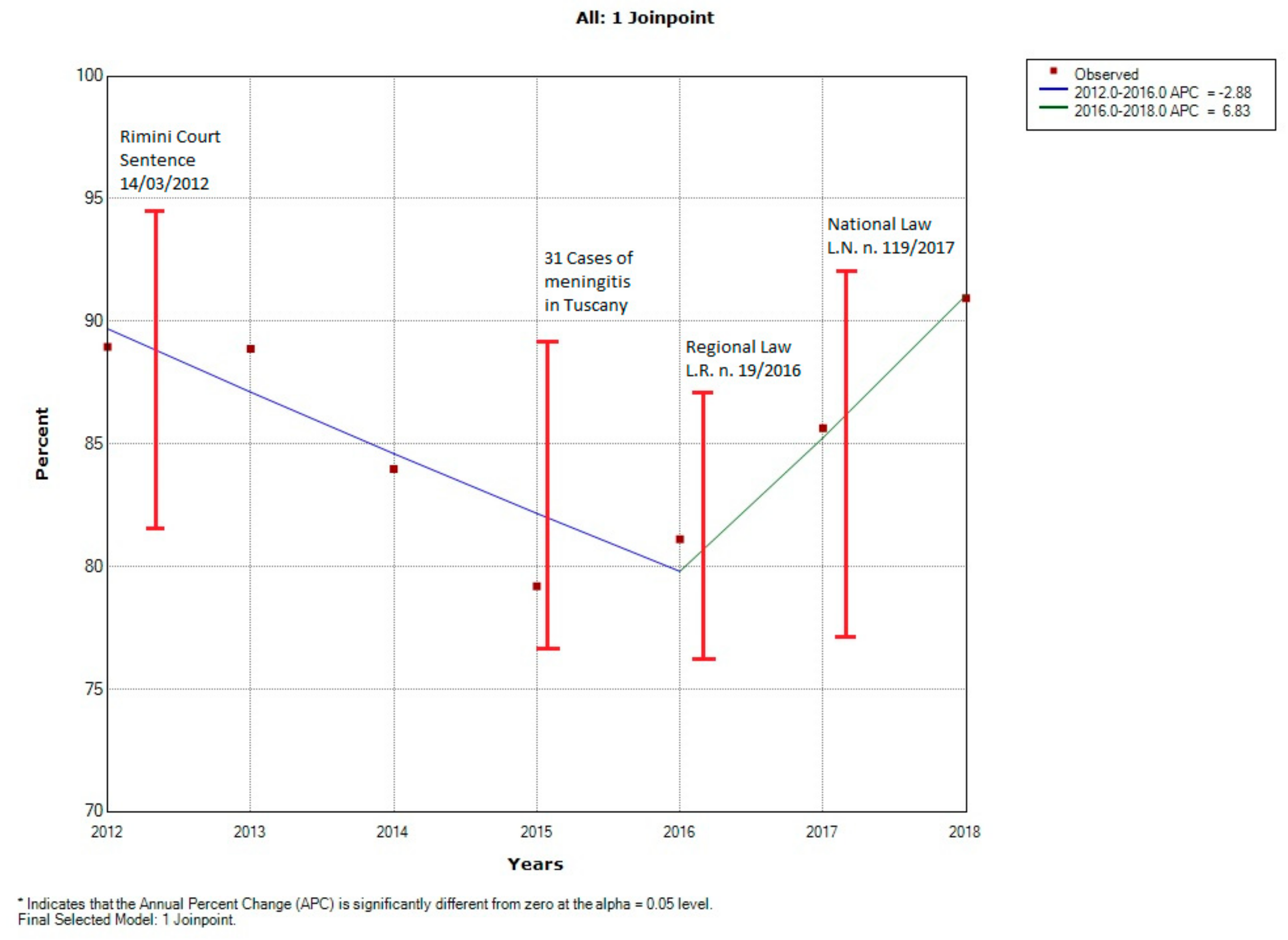
3.3. Joinpoint Analysis
3.3.1. Emilia-Romagna Region
3.3.2. Sicily Region
3.4. Index Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Strategic Advisory Group of Experts on Immunization. The Global Vaccine Action Plan 2011–2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/329097/WHO-IVB-19.07-eng.pdf?ua=1 (accessed on 15 January 2020).
- Odone, A.; Fara, G.M.; Giammaco, G.; Blangiardi, F.; Signorelli, C. The future of immunization policies in Italy and in the European Union: the declaration of Erice. Hum. Vaccin. Immunother. 2015, 11, 1268–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poland, G.A.; Jacobson, R.M. The age-old struggle against the antivaccinationists. N. Engl. J. Med. 2011, 364, 97–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odone, A.; Signorelli, C. When vaccine hesitancy makes headlines. Vaccine 2017, 35, 1209–1210. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, G.K.; Tatar, O.; Dube, E.; Amsel, R.; Knauper, B.; Naz, A.; Perez, S.; Rosberger, Z. The vaccine hesitancy scale: psychometric properties and validation. Vaccine 2018, 36, 660–667. [Google Scholar] [CrossRef]
- MacDonald, N.E.; The SAGE working group on vaccine hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Ten Threats to Global Health in 2019. Available online: https://www.who.int/emergencies/ten-threats-to-global-health-in-2019 (accessed on 2 December 2019).
- Demicheli, V.; Rivetti, A.; Debalini, M.G.; di Pietrantonj, C. Vaccines for measles, mumps and rubella in children. Cochrane Database Syst. Rev. 2012, 15. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Measles. Geneva: WHO. Available online: http://www.who.int/mediacentre/factsheets/fs286/en/ (accessed on 14 November 2019).
- Vaccinations at Paediatric and Adolescent Age—Vaccination Coverage. Available online: http://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?id=20 (accessed on 13 November 2019).
- Kennedy, A.M.; Brown, C.J.; Gust, D.A. Vaccine beliefs of parents who oppose compulsory vaccination. Public Health Rep. 2005, 120, 252–258. [Google Scholar] [CrossRef]
- Vaccinazioni. Available online: http://salute.regione.emilia-romagna.it/sanita-pubblica/vaccinazioni (accessed on 2 December 2019).
- Piano Nazionale Prevenzione Vaccinale (PNPV) 2017-2019. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 20 November 2019).
- Legge 31 Luglio 2017, N. 119. Available online: http://www.gazzettaufficiale.it/eli/id/2017/08/5/17G00132/sg (accessed on 20 November 2019).
- Signorelli, C.; Guerra, R.; Siliquini, R.; Ricciardi, W. Italy’s response to vaccine hesitancy: an innovative and cost effective National Immunization Plan based on scientific evidence. Vaccine 2017, 35, 4057–4059. [Google Scholar] [CrossRef]
- ISTAT. Available online: http://dati.istat.it/Index.aspx (accessed on 15 January 2020).
- Statistica Self Service. Available online: http://statistica.regione.emilia-romagna.it/servizi-online/statistica-self-service (accessed on 15 January 2019).
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Tribunale di Rimini, sentenza n. 2010\148, Ruolo n°2010\0474; Cron. N°2012\886.
- Levi, M.; Sinisgalli, E.; Lorini, C.; Santomauro, F.; Chellini, M.; Bonanni, P. The ‘Fluad Case’ in Italy: could it have been dealt differently? Hum. Vaccin. Immunother. 2017, 13, 379–384. [Google Scholar] [CrossRef]
- Corte di appello di Bologna, sentenza n. 1767 /2014 pubblicata il 13/2/2015; Ruolo n. 803/2012. Cronologico 2014/868.
- Menichetti, F.; Fortunato, S.; Ricci, A.; Salani, F.; Ripoli, A.; Tascini, C.; Fusco, F.M.; Mencarini, J.; Bartoloni, A.; di Pietro, M. Invasive meningococcal disease due to group C N. meningitidis ST11 (cc11): the tuscany cluster 2015–2016. Vaccine 2018, 36, 5962–5966. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Restivo, V.; Ventura, G.; D’Angelo, C.; Randazzo, M.A.; Casuccio, N.; Palermo, M.; Casuccio, A.; Vitale, F. Increased vaccination coverage among adolescents and young adults in the district of Palermo as a result of a public health strategy to counteract an ‘Epidemic Panic’. Int. J. Environ. Res. Public Health 2018, 15, 1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Signorelli, C.; Odone, A.; Cella, P.; Iannazzo, S.; D’Ancona, F.; Guerra, R. Infant immunization coverage in Italy (2000–2016). Ann. Ist. Super. San. 2017, 53, 231–237. [Google Scholar]
- Tabacchi, G.; Costantino, C.; Napoli, G.; Marchese, V.; Cracchiolo, M.; Casuccio, A.; Vitale, F. Determinants of European parents’ decision on the vaccination of their children against measles, mumps and rubella: A systematic review and meta-analysis. Hum. Vaccin. Immunother. 2016, 12, 1909–1923. [Google Scholar] [CrossRef] [Green Version]
- Odone, A.; Tramutola, V.; Morgado, M.; Signorelli, C. Immunization and media coverage in Italy: An eleven-year analysis (2007–17). Hum. Vaccin. Immunother. 2018, 14, 2533–2536. [Google Scholar] [CrossRef] [Green Version]
- Bonanni, P.; Ferro, A.; Guerra, R.; Iannazzo, S.; Odone, A.; Pompa, M.G.; Rizzuto, E.; Signorelli, C. Vaccine coverage in Italy and assessment of the 2012–2014 National Immunization Prevention Plan. Epidemiol. Prev. 2015, 39, 146–158. [Google Scholar]
- Signorelli, C.; Odone, A.; Cella, P.; Iannazzo, S. Childhood vaccine coverage in Italy after the new law on mandatory immunization. Ann. Ig. 2018, 30, 1–10. [Google Scholar]
- Betsch, C.; Brewer, N.T.; Brocard, P.; Davies, P.; Gaissmaier, W.; Haase, N.; Leask, J.; Renkewitz, F.; Renner, B.; Reyna, V.F.; et al. Opportunities and challenges of Web 2. 0 for vaccination decisions. Vaccine 2012, 30, 3727–3733. [Google Scholar]
- Gori, D.; Ialonardi, M.; Odone, A.; Ricci, B.; Pascucci, M.G.; Frasca, G.; Venturi, S.; Signorelli, C.; Fantini, M.P. Vaccine hesitancy and mandatory immunizations in Emilia-Romagna Region: the case of MMR vaccine. Acta. Biomed. 2019, 90, 394–397. [Google Scholar]
- Colucci, M.E.; Veronesi, L.; Bracchi, M.T.; Zoni, R.; Caruso, L.; Capobianco, E.; Rossi, D.; Bizzarro, A.; Cantarelli, A.; Affanni, P. On field vaccine effectiveness in three periods of 2018/2019 influenza season in Emilia-Romagna Region. Acta. Biomed. 2019, 90, 21–27. [Google Scholar]
- I ‘No-Vax’ in un Partito, Movimento Punta a Regionali E-R. Available online: http://www.ansa.it/emiliaromagna/notizie/2019/03/27/regionali-in-e-r-nasce-movimento-no-vax_959b4329-46a0-42bf-aaef-1b677380dd4b.html (accessed on 22 October 2019).
- Italian Ministry of Health. Available online: http://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=1960 (accessed on 25 October 2019).
- La Repubblica. Muore dopo il vaccino, il figlio: "Voglio sapere cosa lo ha ucciso". Available online: https://palermo.repubblica.it/cronaca/2014/11/29/news/muore_dopo_il_vaccino_il_figlio_voglio_sapere_cosa_lo_ha_ucciso-101704244/] (accessed on 22 October 2019).
- Burioni, R.; Odone, A.; Signorelli, C. Lessons from Italy’s policy shift on immunization. Nature 2018, 555, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaccinazioni in Età Pediatrica: Impatto Dell’obbligo Sullecoperture Vaccinali in Italia. Available online: www.gimbe.org/osservatorio/Report_Osservatorio_GIMBE_2019.03_Coperture_vaccinali_2018.pdf (accessed on 15 January 2020).
- Signorelli, C.; Iannazzo, S.; Odone, A. The imperative of vaccination put into practice. Lancet Infect. Dis. 2018, 18, 26–27. [Google Scholar] [CrossRef] [Green Version]
- Il Definanziamento 2010–2019 Del Servizio Sanitario Nazionale. Available online: www.gimbe.org/osservatorio/Report_Osservatorio_GIMBE_2019.07_Definanziamento_SSN.pdf (accessed on 15 January 2020).
- Biasio, L.; Corsello, G.; Costantino, C.; Fara, G.M.; Giammanco, G.; Signorelli, C.; Vecchio, D.; Vitale, F. Communication about vaccination: a shared responsibility. Hum. Vaccin. Immunother. 2016, 12, 2984–2987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferro, A.; Odone, A.; Siddu, A.; Colucci, M.; Anello, P.; Longone, M.; Marcon, E.; Castiglia, P.; Bonanni, P.; Signorelli, C. Monitoring the web to support vaccine coverage: results of two years of the portal vaccinarSì. Epidemiol. Prev. 2015, 39, 88–93. [Google Scholar]



{kind=link}
{kind=link}
| Macro Areas | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 |
|---|---|---|---|---|---|---|---|---|---|---|
| North Emilia | 94.5 | 94.4 | 93.8 | 93.4 | 92.1 | 89.3 | 89.4 | 89.2 | 92.4 | 95.2 |
| Central Emilia | 94.0 | 93.2 | 93.5 | 92.6 | 92.6 | 89.8 | 87.4 | 87.4 | 91.3 | 96.1 |
| Romagna | 91.1 | 89.0 | 90.1 | 90.4 | 87.7 | 83.7 | 82.1 | 83.3 | 88.4 | 93.6 |
| Western Sicily | 88.7 | 89.9 | 92.3 | 91.2 | 92.2 | 87.6 | 82.6 | 85.4 | 89.1 | 92.9 |
| Eastern Sicily | 84.1 | 86.8 | 88.9 | 86.9 | 85.9 | 80.7 | 76.1 | 77.2 | 82.5 | 89.8 |
| Emilia-Romagna Region | 93.5 | 92.7 | 92.8 | 92.4 | 91.1 | 88.1 | 87.0 | 87.2 | 91.1 | 95.0 |
| Sicily Region | 86.8 | 87.8 | 91.6 | 88.9 | 88.9 | 84.0 | 79.2 | 81.1 | 85.6 | 90.9 |
| Macro Areas | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 |
|---|---|---|---|---|---|---|---|---|---|
| North Emilia | 90.1 | 90.3 | 90.4 | 89.6 | 91.2 | 91.1 | 90.2 | 88.3 | 89.6 |
| Central Emilia | 90.0 | 90.0 | 89.2 | 90.4 | 91.2 | 90.3 | 89.3 | 87.9 | 87.4 |
| Romagna | 86.4 | 87.2 | 88.4 | 88.7 | 90.0 | 88.8 | 86.3 | 86.3 | 87.5 |
| Western Sicily | N.A. | N.A. | N.A. | N.A. | 70.3 | 72.8 | 72.2 | 78.6 | 90.7 |
| Eastern Sicily | N.A. | N.A. | N.A. | N.A. | 58.7 | 58.9 | 63.6 | 69.2 | 79.2 |
| Emilia-Romagna Region | 89.1 | 89.4 | 89.6 | 89.6 | 90.9 | 90.3 | 88.9 | 87.7 | 88.5 |
| Sicily Region | N.A. | N.A. | N.A. | N.A. | 63.9 | 65.7 | 67.6 | 75.3 | 84.7 |
| N.A. = No available data | |||||||||
| Year | Unvaccinated (%) | Vaccinated (%) | Total | χ² | p-value |
|---|---|---|---|---|---|
| 2012 | 3185 (7.6) | 38,768 (92.4) | 41,953 | ||
| 2013 | 3569 (8.9) | 36,652 (91.1) | 40,221 | 44.71 | <0.001 |
| Total | 6754 | 75,420 | 82,174 | ||
| 2012 | 3185 (7.6) | 38,768 (92.4) | 41,953 | ||
| 2014 | 4700 (11.9) | 34,658 (88.1) | 39,358 | 438.77 | <0.001 |
| Total | 7885 | 73,426 | 81,311 | ||
| 2012 | 3185 (7.6) | 38,768 (92.4) | 41,953 | ||
| 2015 | 4892 (13) | 32,735 (87) | 37,627 | 636.51 | <0.001 |
| Total | 8077 | 71,503 | 79,580 | ||
| 2012 | 3185 (7.6) | 38,768 (92.4) | 41,953 | ||
| 2016 | 4716 (12.7) | 32,269 (87.3) | 36,985 | 580.88 | <0.001 |
| Total | 7,901 | 71,037 | 78,938 | ||
| 2012 | 3,185 (7.6) | 38,768 (92.4) | 41,953 | ||
| 2017 | 3,208 (8.9) | 32,874 (91.1) | 36,082 | 43.52 | <0.001 |
| Total | 6,393 | 71,642 | 78,035 | ||
| 2012 | 3,185 (7.6) | 38,768 (92.4) | 41,953 | ||
| 2018 | 2,286 (6.5) | 32,702 (93.5) | 34,988 | 32.34 | <0.001 |
| Total | 5,471 | 68,470 | 76,941 | ||
| Year | Unvaccinated (%) | Vaccinated (%) | Total | χ² | p-value |
|---|---|---|---|---|---|
| 2015 | 4892 (13) | 32,735 (87) | 37,627 | ||
| 2016 | 4716 (12.7) | 32,269 (87.3) | 36,985 | 1.04 | 0.3077 |
| Total | 9608 | 65,004 | 74,612 | ||
| 2015 | 4892 (13) | 32,735 (87) | 37,627 | ||
| 2017 | 3208 (8.9) | 32,874 (91.1) | 36,082 | 318.16 | <0.001 |
| Total | 8100 | 65,609 | 73,709 | ||
| 2015 | 4892 (13) | 32,735 (87) | 37,627 | ||
| 2018 | 2286 (6.5) | 32,702 (93.5) | 34,988 | 851.35 | <0.001 |
| Total | 7178 | 65,437 | 72,615 | ||
| Year | Unvaccinated | Vaccinated | Total | χ² | p-value |
|---|---|---|---|---|---|
| 2012 | 5304 (11) | 42,733 (89) | 48,037 | ||
| 2013 | 5201 (11.1) | 41,558 (88.9) | 46,759 | 44.71 | <0.001 |
| Total | 10,505 | 84,291 | 94,796 | ||
| 2012 | 5304 (11) | 42,733 (89) | 48,037 | ||
| 2014 | 7295 (16) | 38,220 (84) | 45,515 | 438.77 | <0.001 |
| Total | 12,599 | 80,953 | 93,552 | ||
| 2012 | 5304 (11) | 42,733 (89) | 48,037 | ||
| 2015 | 9167 (20.8) | 34,909 (79.2) | 44,076 | 636.51 | < 0.001 |
| Total | 14,201 | 77,642 | 92,113 | ||
| 2012 | 5304 (11) | 42,733 (89) | 48,037 | ||
| 2016 | 8296 (18.9) | 35,621 (81.1) | 43,917 | 580.88 | < 0.001 |
| Total | 13,600 | 78,354 | 91,954 | ||
| 2012 | 5304 (11) | 42,733 (89) | 48,037 | ||
| 2017 | 6204 (14.4) | 36,983 (85.6) | 43,187 | 43.52 | < 0.001 |
| Total | 11,508 | 79,716 | 91,224 | ||
| 2012 | 5304 (11) | 42,733 (89) | 48,037 | ||
| 2018 | 3752 (9.1) | 37,659 (90.9) | 41,411 | 95.92 | <0.001 |
| Total | 9056 | 80,392 | 89,448 | ||
| Year | Unvaccinated | Vaccinated | Total | χ² | p-value |
|---|---|---|---|---|---|
| 2015 | 9167 (20.8) | 34,909 (79.2) | 44,076 | ||
| 2016 | 8296 (18.9) | 35,621 (81.1) | 43,917 | 50.34 | 0.01 |
| Total | 17,463 | 70,530 | 87,993 | ||
| 2015 | 9167 (20.8) | 34,909 (79.2) | 44,076 | ||
| 2017 | 6204 (14.4) | 36,983 (85.6) | 43,187 | 318.16 | < 0.001 |
| Total | 15,371 | 71,892 | 87,263 | ||
| 2015 | 9167 (20.8) | 34,909 (79.2) | 44,076 | ||
| 2018 | 3752 (9.1) | 37,659 (90.9) | 41,411 | 2,293.1 | <0.001 |
| Total | 12,919 | 72,568 | 85,487 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gori, D.; Costantino, C.; Odone, A.; Ricci, B.; Ialonardi, M.; Signorelli, C.; Vitale, F.; Fantini, M.P. The Impact of Mandatory Vaccination Law in Italy on MMR Coverage Rates in Two of the Largest Italian Regions (Emilia-Romagna and Sicily): An Effective Strategy to Contrast Vaccine Hesitancy. Vaccines 2020, 8, 57. https://doi.org/10.3390/vaccines8010057
Gori D, Costantino C, Odone A, Ricci B, Ialonardi M, Signorelli C, Vitale F, Fantini MP. The Impact of Mandatory Vaccination Law in Italy on MMR Coverage Rates in Two of the Largest Italian Regions (Emilia-Romagna and Sicily): An Effective Strategy to Contrast Vaccine Hesitancy. Vaccines. 2020; 8(1):57. https://doi.org/10.3390/vaccines8010057
Chicago/Turabian StyleGori, Davide, Claudio Costantino, Anna Odone, Beatrice Ricci, Magda Ialonardi, Carlo Signorelli, Francesco Vitale, and Maria Pia Fantini. 2020. "The Impact of Mandatory Vaccination Law in Italy on MMR Coverage Rates in Two of the Largest Italian Regions (Emilia-Romagna and Sicily): An Effective Strategy to Contrast Vaccine Hesitancy" Vaccines 8, no. 1: 57. https://doi.org/10.3390/vaccines8010057
APA StyleGori, D., Costantino, C., Odone, A., Ricci, B., Ialonardi, M., Signorelli, C., Vitale, F., & Fantini, M. P. (2020). The Impact of Mandatory Vaccination Law in Italy on MMR Coverage Rates in Two of the Largest Italian Regions (Emilia-Romagna and Sicily): An Effective Strategy to Contrast Vaccine Hesitancy. Vaccines, 8(1), 57. https://doi.org/10.3390/vaccines8010057