Hepatitis B Seroprevalence in the Pediatric and Adolescent Population of Florence (Italy): An Update 27 Years after the Implementation of Universal Vaccination

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Confirmation of Vaccination and Anamnestic Status towards Hepatitis B
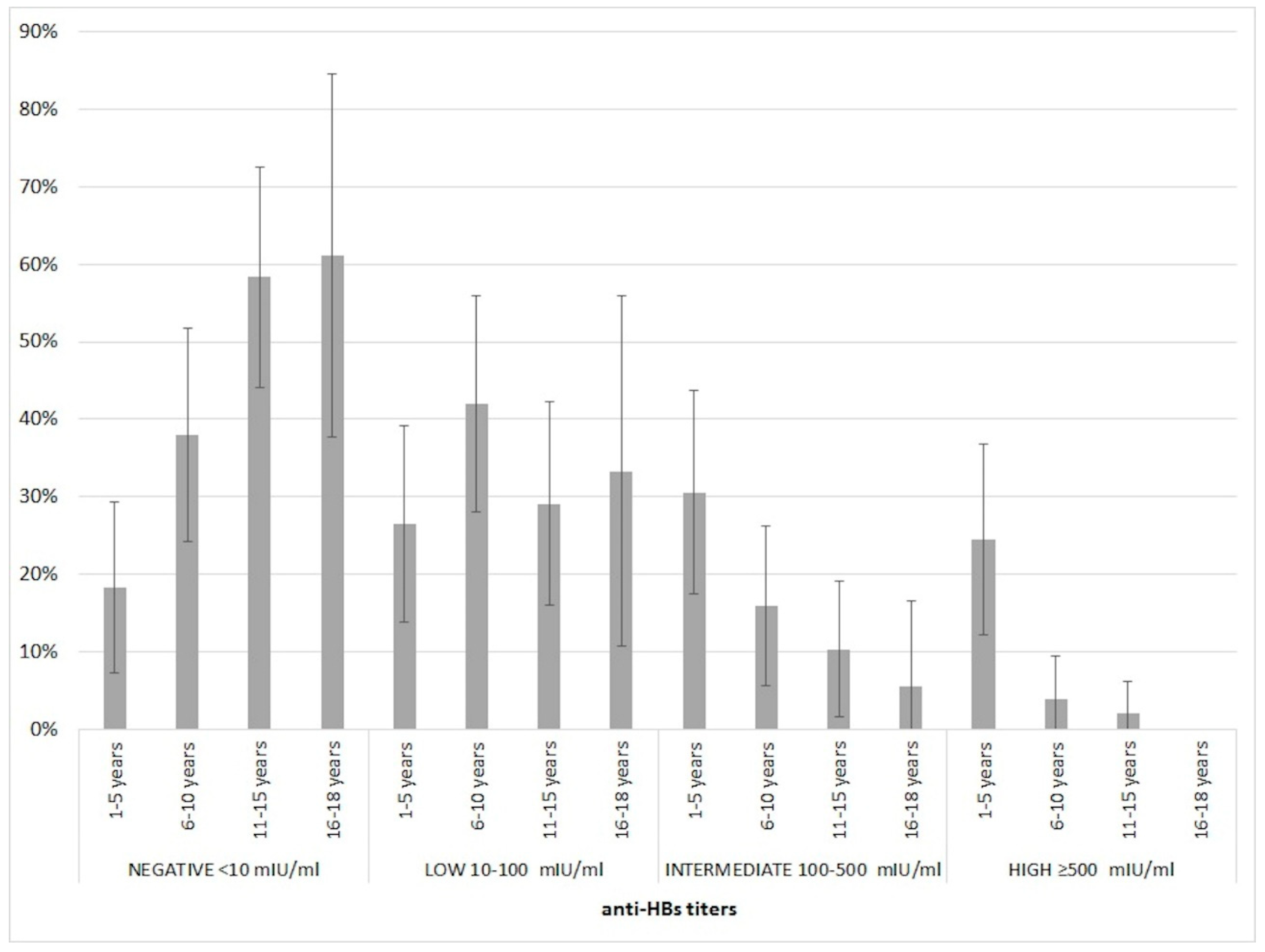
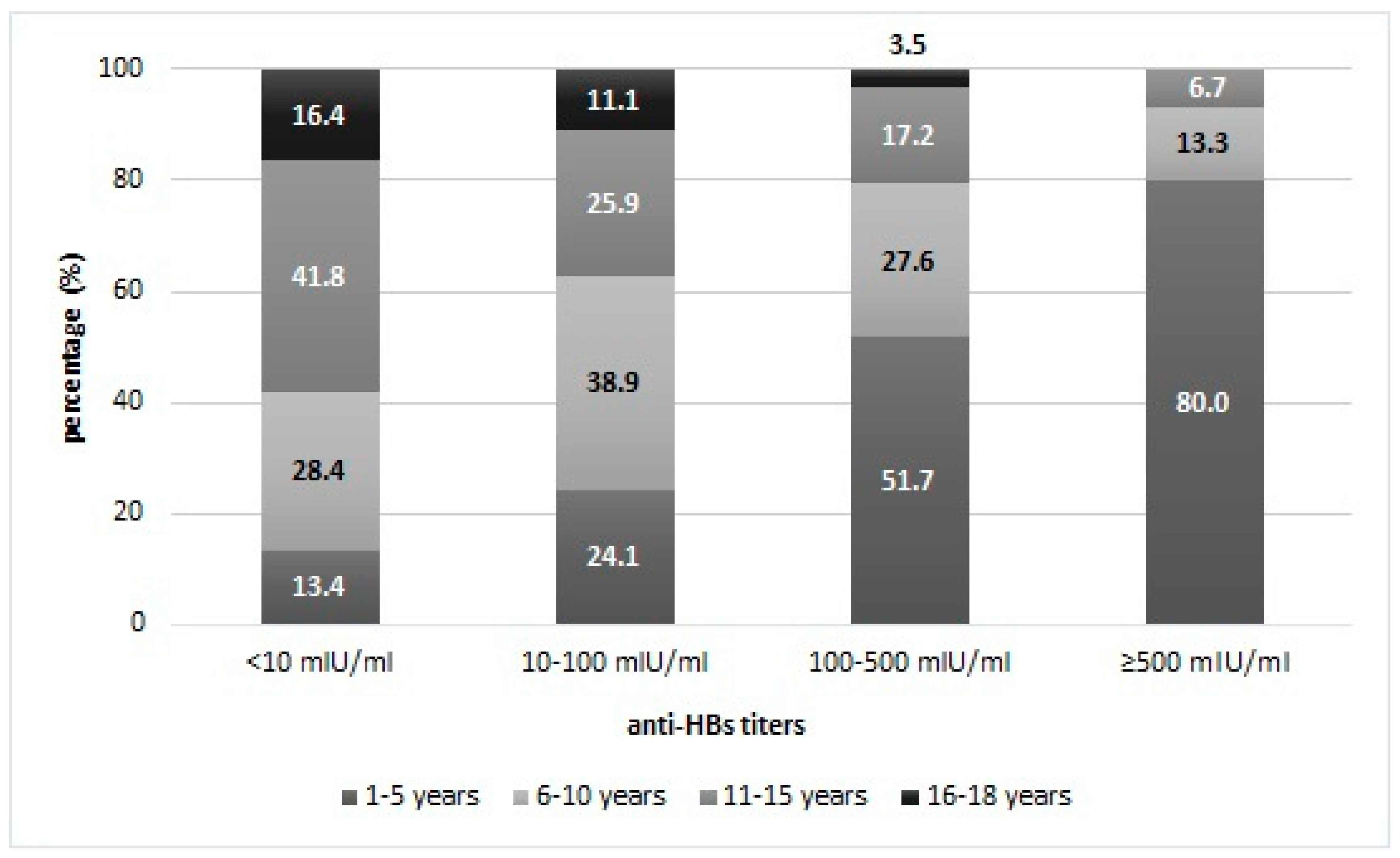
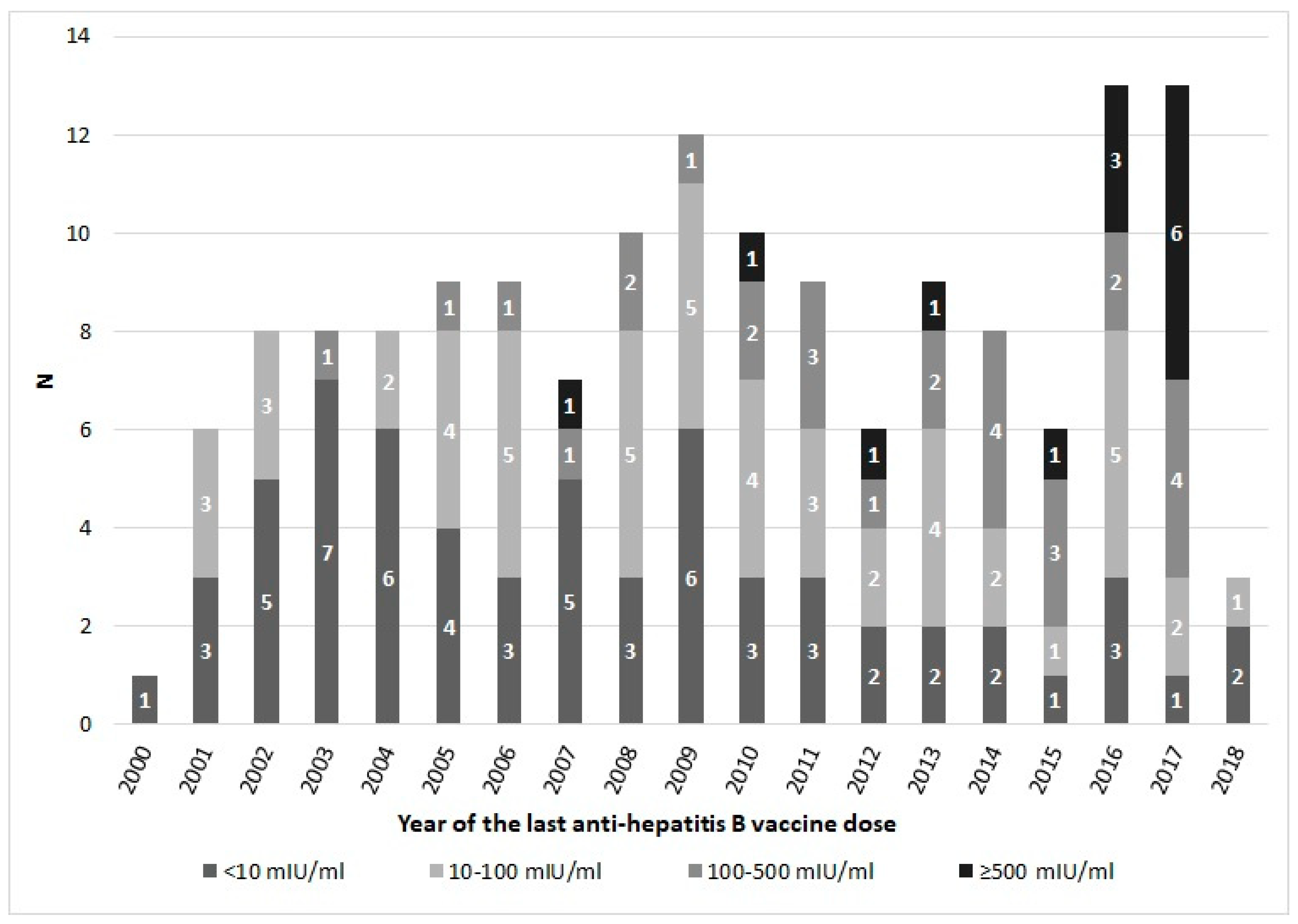
3.2. Quantitave Analysis of Anti-HBs
3.3. Multivariate Analysis
3.4. Qualitative Analysis of Anti-HBc
3.5. Trend of Serological Profile towards Hepatitis B
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Home. News. Fact Sheets. Detail. Hepatitis B. Available online: http://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 17 April 2019).
- WHO. Immunization, Vaccines and Biologicals. Vaccines and diseases. Hepatitis B. Available online: http://www.who.int/immunization/diseases/hepatitisB/en/ (accessed on 17 April 2019).
- WHO. Hepatitis B vaccines: WHO position paper—July 2017 recommendations. Vaccine 2019, 37, 223–225. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Hepatitis B in the WHO European Region. Fact Sheet—July 2018. Available online: http://www.euro.who.int/__data/assets/pdf_file/0007/377251/fact-sheet-hepatitis-b-eng.pdf?ua=1 (accessed on 17 April 2019).
- European Centre for Disease Prevention and Control. Hepatitis B. In ECDC. Annual Epidemiological Report for 2016; ECDC: Stockholm, Sweden, 2018. [Google Scholar]
- Legge n. 165 del 27 Maggio 1991. Obbligatorietà della vaccinazione contro l’epatite virale B. in Gazzetta Ufficiale Serie Generale n. 127 del 01 June 1991. Available online: http://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=1991-06-01&atto.codiceRedazionale=091G0201&elenco30giorni=false (accessed on 18 April 2019).
- Legge n. 119 del 31 Luglio 2017. Conversione in Legge, con Modificazioni, del Decreto-Legge 7 Giugno 2017, n. 73, Recante Disposizioni Urgenti in Materia di Prevenzione Vaccinale. In Gazzetta Ufficiale Serie Generale, n. 182 del 5 August 2017. Available online: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2017-08-05&atto.codiceRedazionale=17G00132&elenco30giorni=false (accessed on 18 April 2019).
- Ministero Della Salute. Anno 2013. Coperture Vaccinali (24 mesi) (per 100 abitanti), Calcolate sui Riepiloghi Inviati Dalle Regioni e PP.AA. Dati Aggiornati al 11 August 2015. Available online: http://www.salute.gov.it/imgs/C_17_tavole_20_allegati_iitemAllegati_0_fileAllegati_itemFile_1_file.pdf (accessed on 18 April 2019).
- Ministero Della Salute. Anno 2014. Coperture Vaccinali (24 mesi) (per 100 abitanti), Calcolate sui Riepiloghi Inviati Dalle REGIONI e PP.AA. Dati Aggiornati al 20 January 2016. Available online: http://www.salute.gov.it/imgs/C_17_tavole_20_allegati_iitemAllegati_0_fileAllegati_itemFile_2_file.pdf (accessed on 18 April 2019).
- Ministero Della Salute. Anno 2015. Coperture Vaccinali (24 mesi) (per 100 abitanti), Calcolate sui Riepiloghi Inviati Dalle Regioni e PP.AA. Available online: http://www.salute.gov.it/imgs/C_17_tavole_20_allegati_iitemAllegati_0_fileAllegati_itemFile_3_file.pdf (accessed on 18 April 2019).
- Ministero Della Salute. Anno 2016. Coperture Vaccinali (24 mesi) (per 100 abitanti), Calcolate sui Riepiloghi Inviati Dalle Regioni e PP.AA. Dati Aggiornati al 05 June 2017. Available online: http://www.salute.gov.it/imgs/C_17_tavole_20_allegati_iitemAllegati_0_fileAllegati_itemFile_5_file.pdf (accessed on 18 April 2019).
- Ministero Della Salute. Anno 2017. Coperture Vaccinali (24 mesi) (per 100 abitanti), Calcolate sui Riepiloghi inviati Dalle Regioni e PP.AA. Dati Aggiornati al 28 Ferbuary 2018. Available online: http://www.salute.gov.it/imgs/C_17_tavole_20_allegati_iitemAllegati_0_fileAllegati_itemFile_6_file.pdf (accessed on 18 April 2019).
- Epicentro, Istituto Superiore di Sanità. Epatite Virale. Epidemiologia—Dati Seieva. Datiepidemiologici al 31 December 2018. Available online: https://www.epicentro.iss.it/epatite/dati-seieva#b (accessed on 18 April 2019).
- Ministero Della Salute. Piano Nazionale per la Prevenzione Delle Epatiti Virali da Virus B e C (PNEV). 2015. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2437_allegato.pdf (accessed on 2 May 2019).
- Istituto Superiore di Sanità. Bollettino Seieva. Epidemiologia delle Epatiti Virali Acute in Italia. Numero 4—Aggiornamento 2018. 2019. Available online: https://www.epicentro.iss.it/epatite/bollettino/Bollettino-4-marzo-2019.pdf (accessed on 2 May 2019).
- Regional Agency for Health. La sorveglianza epidemiologica delle malattie infettive in Toscana. Rapporto. October 2018, pp. 112–116. Available online: https://www.ars.toscana.it/images/rapporto_malattie_infettive_new.pdf (accessed on 3 June 2019).
- Regional Agency for Health. Le Malattieinfettive in Toscana. Indicatori Riferiti ai casi di Malattia Negli Ultimi 10 Anni. Epatite B. 2018. Available online: https://datastudio.google.com/u/0/reporting/1CJK0ZXCjMLSMnurfUx-asrBhO2VcoyP7/page/XApi?s=jKraMR7U2uM (accessed on 15 January 2020).
- Sistema Informativo delle Malattie Infettive (SIMI)-Regione Toscana. Available online: https://datastudio.google.com/u/0/reporting/1CJK0ZXCjMLSMnurfUx-asrBhO2VcoyP7/page/XApi?s=jKraMR7U2uM (accessed on 2 March 2020).
- Bonanni, P.; Pesavento, G.; Bechini, A.; Tiscione, E.; Mannelli, F.; Benucci, C.; Nostro, A.L. Impact of universal vaccination programmes on the epidemiology of hepatitis B: 10 years of experience in Italy. Vaccine 2003, 21, 685–691. [Google Scholar] [CrossRef]
- Boccalini, S.; Pellegrino, E.; Tiscione, E.; Pesavento, G.; Bechini, A.; Levi, M.; Rapi, S.; Mercurio, S.; Mannelli, F.; Peruzzi, M.; et al. Sero-epidemiology of hepatitis B markers in the population of Tuscany, Central Italy, 20 years after the implementation of universal vaccination. Hum VaccinImmunother. 2013, 9, 636–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GeoDemo Istat. Popolazione Residente al 1° Gennaio 2017 nella Provincia di Firenze. Available online: http://demo.istat.it/pop2017/index.html (accessed on 15 January 2020).
- Amodio, E.; Tramuto, F.; Cracchiolo, M.; Sciuto, V.; De Donno, A.; Guido, M.; Rota, M.C.; Gabutti, G.; Vitale, F. The impact of ten years of infant universal Varicella vaccination in Sicily, Italy (2003–2012). Hum. Vaccin. Immunother. 2015, 11, 236–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabutti, G.; Penna, C.; Rossi, M.; Salmaso, S.; Rota, M.C.; Bella, A.; Crovari, P.; Serological Study Group. The seroepidemiology of varicella in Italy. Epidemiol. Infect. 2001, 126, 433–440. [Google Scholar] [CrossRef] [Green Version]
- Gabutti, G.; Rota, M.C.; Salmaso, S.; Bruzzone, B.M.; Bella, A.; Crovari, P.; Serological Study Group. Epidemiology of measles, mumps and Rubella in Italy. Epidemiol. Infect. 2002, 129, 543–550. [Google Scholar] [CrossRef]
- Gabutti, G.; Rota, M.C.; Guido, M.; De Donno, A.; Bella, A.; Ciofi degli Atti, M.L.; Crovari, P.; Seroepidemiology Group. The epidemiology of Varicella Zoster Virus infection in Italy. BMC Public Health 2008, 8, 372. [Google Scholar] [CrossRef] [Green Version]
- Gabutti, G.; Rota, M.C.; De Donno, A.; Guido, M.; Bella, A.; Idolo, A.; Lupi, S.; Brignole, G. e il Gruppo di studio sulla sieroepidemiologia. Sieroepidemiologia dell’infezione da VZV in Italia: Valutazione dell’impatto della vaccinazione estensiva. Sero-epidemiology of VZV infection in Italy: Impact evaluation of extensive vaccination. Epidemiol. Prev. 2014, 38 (Suppl. 2), 57–61. [Google Scholar]
- Rota, M.C.; Bella, A.; Gabutti, B.; Giambi, C.; Filia, A.; Guido, M.; De Donno, A.; Crovari, P.; Ciofi degli Atti, M.L.; Serological Study Group. Rubella seroprofile of the Italian population: An 8-year comparison. Epidemiol. Infect. 2007, 135, 555–562. [Google Scholar] [CrossRef]
- Rota, M.C.; Massaria, M.; Gabutti, G.; Guido, M.; De Donno, A.; Ciofi degli Atti, M.L. Measles serological survey in the Italian population: Interpretation of results using mixture model. Vaccine 2008, 26, 4403–4409. [Google Scholar] [CrossRef]
- De Melker, H.; Pebody, R.G.; Edmunds, W.L.; Levy-Bruhl, D.; Valle, M.; Rota, M.C.; Salmaso, S.; van den Hof, S.; Berbers, G.; Salioù, P.; et al. The seroepidemiology of measles in Western Europe. Epidemiol. Infect. 2001, 126, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Pebody, R.G.; Edmunds, W.J.; Conyn-van Spaendonck, M.; Olin, P.; Berbers, G.; Rebiere, I.; Lecoeur, H.; Crovari, P.; Davidkin, I.; Gabutti, G.; et al. The seroepidemiology of rubella in western Europe. Epidemiol. Infect. 2001, 125, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A.A.; Falla, A.M.; Duffell, E.; Noori, T.; Bechini, A.; Reintjes, R.; Veldhuijzen, I.K. Estimating the scale of chronic hepatitis B virus infection among migrants in EU/EEA countries. BMC Infect. Dis. 2018, 18, 34. [Google Scholar] [CrossRef] [PubMed]
- Assad, S.; Francis, A. Over a decade of experience with a yeast recombinant hepatitis B vaccine. Vaccine 1999, 18, 57–67. [Google Scholar] [CrossRef]
- Jilg, W.; Schmidt, M.; Deinhardt, F. Decline of anti-HBs after hepatitis B vaccination and timing of revaccination. Lancet 1990, 335, 173–174. [Google Scholar] [CrossRef]
- Van Damme, P. Long-term Protection after Hepatitis B Vaccine. J. Infect. Dis. 2016, 214, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Verso, M.G.; Costantino, C.; Vitale, F.; Amodio, E. Immunization against Hepatitis B Surface Antigen (HBsAg) in a Cohort of Nursing Students Two Decades after Vaccination: Surprising Feedback. Vaccines 2019, 8, 1. [Google Scholar] [CrossRef] [Green Version]
- Hudu, S.A.; Malik, Y.A.; Niazlin, M.T.; Harmal, N.S.; Adnan, A.; Alshrari, A.S.; Sekawi, Z. Antibody and immune memory persistence post infant hepatitis B vaccination. Patient Prefer Adherence 2013, 7, 981–986. [Google Scholar] [CrossRef] [Green Version]
- Banatvala, J.E.; Van Damme, P. Hepatitis B vaccine—Do we need boosters? J. Viral Hepat. 2003, 10, 1–6. [Google Scholar] [CrossRef]
- Yuen, M.F.; Lim, W.L.; Chan, A.O.; Wong, D.K.; Sum, S.S.; Lai, C.L. 18-year follow-up study of a prospective randomized trial of hepatitis B vaccinations without booster doses in children. Clin. Gastroenterol. Hepatol. 2004, 2, 941–945. [Google Scholar] [CrossRef]
- Petersen, K.M.; Bulkow, L.R.; McMahon, B.J.; Zanis, C.; Getty, M.; Peters, H.; Parkinson, A.J. Duration of hepatitis B immunity in low risk children receiving hepatitis B vaccinations from birth. Pediatr. Infect. Dis. J. 2004, 23, 650–655. [Google Scholar] [CrossRef] [Green Version]
- Hammitt, L.L.; Hennessy, T.W.; Fiore, A.E.; Zanis, C.; Hummel, K.B.; Dunaway, E.; Bulkow, L.; McMahon, B.J. Hepatitis B immunity in children vaccinated with recombinant hepatitis B vaccine beginning at birth: A follow-up study at 15 years. Vaccine 2007, 25, 6958–6964. [Google Scholar] [CrossRef] [PubMed]
- FitzSimons, D.; Hendrickx, G.; Vorsters, A.; Van Damme, P. Hepatitis B vaccination: A completed schedule enough to control HBV lifelong? Milan, Italy, 17–18 November 2011. Vaccine 2013, 31, 584–590. [Google Scholar] [CrossRef] [PubMed]
- West, D.J.; Calandra, G.B. Vaccine induced immunologic memory for hepatitis B surface antigen: Implications for policy on booster vaccination. Vaccine 1996, 14, 1019–1027. [Google Scholar] [CrossRef]
- Steiner, M.; Ramakrishnan, G.; Gartner, B.; Van Der Meeren, O.; Jacquet, J.M.; Schuster, V. Lasting immune memory against hepatitis B in children after primary immunization with 4 doses of DTPa-HBV-IPV/Hib in the first and 2nd year of life. BMC Infect. Dis. 2010, 10, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinke, M.; Kappes, R.; Kindler, K.; Paulus-Koschik, A.; Goering, U.; Disselhoff, J.; Soemantri, P.; Grunert, D.; Laakmann, K.H.; Gunasekaran, R.; et al. Immune memory to hepatitis B virus in 4-9-year old children vaccinated in infancy with four doses of hexavalent DTPa-HBV-IPV/Hib vaccine. Hum. Vaccin. 2009, 5, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Zanetti, A.R.; Romanò, L.; Giambi, C.; Pavan, A.; Carnelli, V.; Baitelli, G.; Malchiodi, G.; Valerio, E.; Barale, A.; Marchisio, M.A.; et al. Hepatitis B immune memory in children primed with hexavalent vaccines and given monovalent booster vaccines: An open-label, randomised, controlled, multicentre study. Lancet Infect. Dis. 2010, 10, 755–761. [Google Scholar] [CrossRef]
- Romanò, L.; Zanetti, A.R. Booster hepatitis B vaccination not necessary for long-term protection in children immunised with hexavalent vaccines. J. Prev. Med. Hyg. 2011, 52, 45–46. [Google Scholar]
- Giambi, C.; Bella, A.; Barale, A.; Montù, D.; Marchisio, M.; Oddone, M.; Zito, S.; Rapicetta, M.; Chionne, P.; Madonna, E.; et al. A cohort study to evaluate persistence of hepatitis B immunogenicity after administration of hexavalent vaccines. BMC Infect. Dis. 2008, 8, 100. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Age Groups (years) | Enrolled Subjects (N) |
|---|---|
| 1–5 | 49 |
| 6–10 | 50 |
| 11–15 | 48 |
| 16–18 | 18 |
| TOTAL | 165 |
| Age (years) | Subjects (N; %) | <10 mIU/mL | 10–100 mIU/mL | 100–500 mIU/mL | ≥500 mIU/mL | Total |
|---|---|---|---|---|---|---|
| 1–5 years | N | 9 | 13 | 15 | 12 | 49 |
| % [anti-HBs] | 18.4 | 26.5 | 30.6 | 24.5 | 100 | |
| % of the subjects | 13.4 | 24.1 | 51.7 | 80.0 | 29.7 | |
| 6–10 years | N | 19 | 21 | 8 | 2 | 50 |
| % [anti-HBs] | 38.0 | 42.00 | 16.0 | 4.0 | 100 | |
| % of the subjects | 28.4 | 38.9 | 27.6 | 13.3 | 30.3 | |
| 11–15 years | N | 28 | 14 | 5 | 1 | 48 |
| % [anti-HBs] | 58.3 | 29.2 | 10.4 | 2.1 | 100 | |
| % of the subjects | 41.8 | 25.9 | 17.2 | 6.7 | 29.1 | |
| 16–18 years | N | 11 | 6 | 1 | 0 | 18 |
| % [anti-HBs] | 61.1 | 33.3 | 5.6 | 0.0 | 100 | |
| % of the subjects | 16.4 | 11.1 | 3.5 | 0.0 | 10.9 | |
| Total | 67 | 54 | 29 | 15 | 165 | |
| 40.6 | 32.7 | 17.6 | 9.1 | 100 | ||
| Spearman’s rho = −0.4316 p < 0.0001 | ||||||
| Time Since Last | Subjects (N; %) | <10 | 10–100 | 100–500 | ≥500 | Total |
|---|---|---|---|---|---|---|
| dose (years) | mIU/mL | mIU/mL | mIU/mL | mIU/mL | ||
| 0–5 | N | 11 | 17 | 15 | 11 | 54 |
| % [anti-HBs] | 20.4 | 31.5 | 27.8 | 20.4 | 100 | |
| % of the subjects | 16.4 | 31.5 | 51.7 | 73.3 | 32.7 | |
| 6–10 | N | 18 | 18 | 9 | 2 | 47 |
| % [anti-HBs] | 38.3 | 38.3 | 19.1 | 4.3 | 100 | |
| % of the subjects | 26.9 | 33.3 | 31.0 | 13.3 | 28.5 | |
| 11–15 | N | 25 | 11 | 4 | 1 | 41 |
| % [anti-HBs] | 61.0 | 26.8 | 9.8 | 2.4 | 100 | |
| % of the subjects | 37.3 | 20.4 | 13.8 | 6.7 | 24.8 | |
| 16–18 | N | 8 | 5 | 0 | 0 | 13 |
| % [anti-HBs] | 61.5 | 38.5 | 0.0 | 0.0 | 100 | |
| % of the subjects | 11.9 | 9.3 | 0.0 | 0.0 | 7.9 | |
| Unvaccinated | N | 5 | 3 | 1 | 1 | 10 |
| % [anti-HBs] | 50.0 | 30.0 | 10.0 | 10.0 | 100 | |
| % of the subjects | 7.5 | 5.6 | 3.4 | 6.7 | 6.1 | |
| Total | 67 | 54 | 29 | 15 | 165 | |
| 40.6 | 32.7 | 17.6 | 9.1 | 100 | ||
| Spearman’s rho = −0.3843 p < 0.0001 | ||||||
| Dependent Variable: Degrees of Anti-HBs Titers | |||||
|---|---|---|---|---|---|
| AOR | SE | 95% CI | p-Value | ||
| Sex | Female | - | - | - | - |
| Male | 1.10 | 0.33 | 0.61-1.98 | 0.754 | |
| Nationality | Italian | - | - | - | - |
| Foreign | 1.44 | 0.65 | 0.59-3.51 | 0.415 | |
| Time since the last dose | 0–5 years | - | - | - | - |
| 6–10 years | 0.35 | 0.13 | 0.17–0.74 | 0.006 | |
| 11–15 years | 0.15 | 0.06 | 0.06–0.35 | < 0.0001 | |
| 16–18 years | 0.13 | 0.08 | 0.04–0.43 | 0.001 | |
| Unvaccinated | 0.21 | 0.14 | 0.05–0.81 | 0.024 | |
| Studies(year) | Anti-HBs ≥ 10 mIU/mL (%) | Anti-HBc (%) | HBsAg (%) | |||
|---|---|---|---|---|---|---|
| 1–10 years | 11–20 years | 1–10 years | 11–20 years | 1–10 years | 11–20 years 1 | |
| 2000 | 78.4 | 82.4 | 0 | 0.9 | 0 | 0 |
| 2009 | 59.1 | 58.1 | 4.1 | 5.0 | 0 | 0.6 |
| 2017–2018 | 71.7 | 40.9 | 0 | 0 | 0 | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanella, B.; Bechini, A.; Boccalini, S.; Sartor, G.; Tiscione, E.; Working Group DHS; Working Group AOUMeyer; Working Group AUSLTC; Bonanni, P. Hepatitis B Seroprevalence in the Pediatric and Adolescent Population of Florence (Italy): An Update 27 Years after the Implementation of Universal Vaccination. Vaccines 2020, 8, 156. https://doi.org/10.3390/vaccines8020156
Zanella B, Bechini A, Boccalini S, Sartor G, Tiscione E, Working Group DHS, Working Group AOUMeyer, Working Group AUSLTC, Bonanni P. Hepatitis B Seroprevalence in the Pediatric and Adolescent Population of Florence (Italy): An Update 27 Years after the Implementation of Universal Vaccination. Vaccines. 2020; 8(2):156. https://doi.org/10.3390/vaccines8020156
Chicago/Turabian StyleZanella, Beatrice, Angela Bechini, Sara Boccalini, Gino Sartor, Emilia Tiscione, Working Group DHS, Working Group AOUMeyer, Working Group AUSLTC, and Paolo Bonanni. 2020. "Hepatitis B Seroprevalence in the Pediatric and Adolescent Population of Florence (Italy): An Update 27 Years after the Implementation of Universal Vaccination" Vaccines 8, no. 2: 156. https://doi.org/10.3390/vaccines8020156
APA StyleZanella, B., Bechini, A., Boccalini, S., Sartor, G., Tiscione, E., Working Group DHS, Working Group AOUMeyer, Working Group AUSLTC, & Bonanni, P. (2020). Hepatitis B Seroprevalence in the Pediatric and Adolescent Population of Florence (Italy): An Update 27 Years after the Implementation of Universal Vaccination. Vaccines, 8(2), 156. https://doi.org/10.3390/vaccines8020156