Defining Elimination of Genital Warts—A Modified Delphi Study

 , ,
, ,
Abstract
:1. Introduction
2. Method
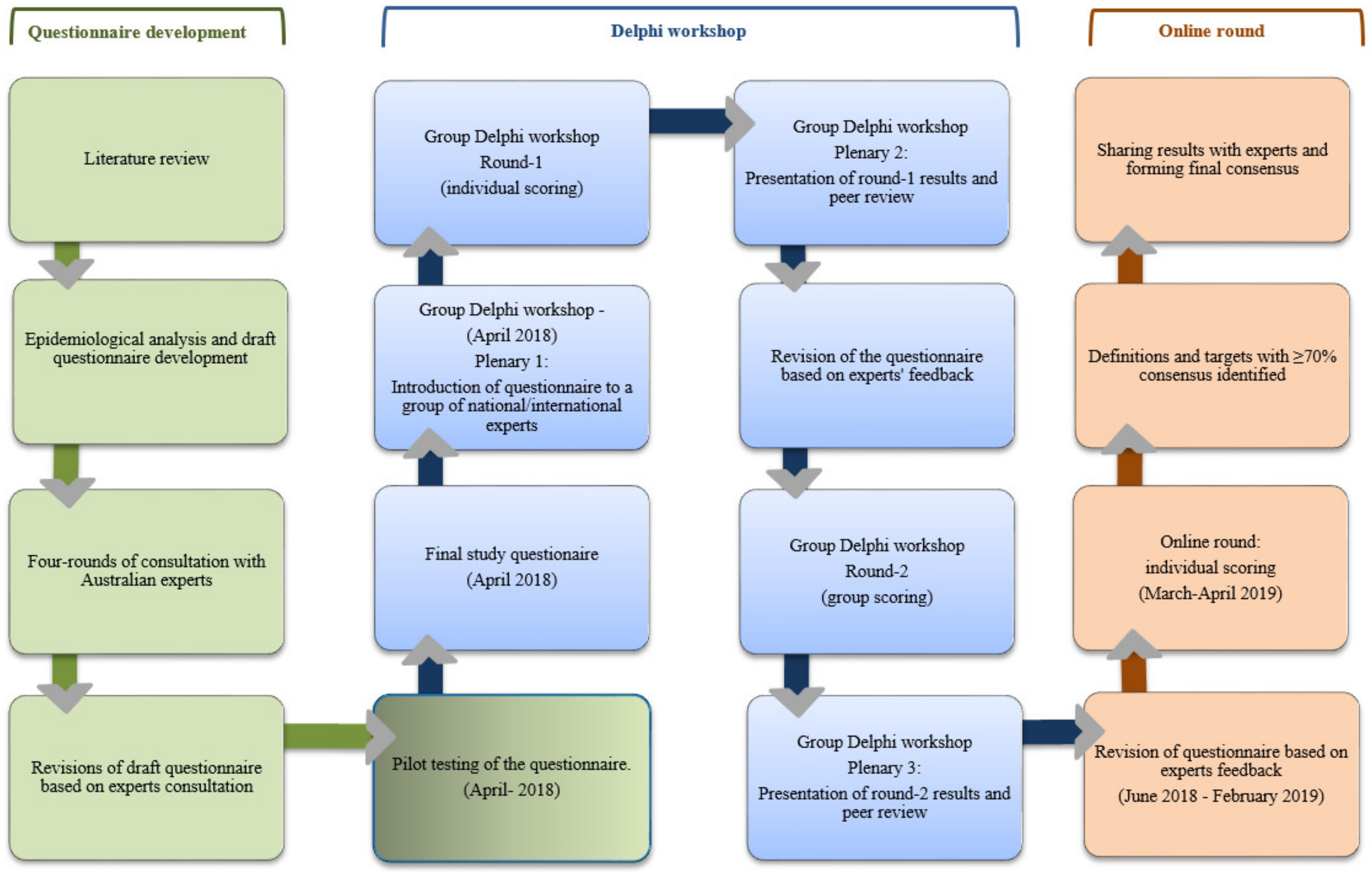
2.1. The Delphi Method
2.2. Design and Participants
2.3. Procedures
2.3.1. Epidemiological Analyses
2.3.2. Questionnaire Development
2.3.3. Delphi Workshop
2.3.4. On-Line Round
2.4. Data Analysis and Level of Consensus
2.5. Ethics Approval
2.6. Role of Funding Source
3. Results
3.1. Characteristics of the Experts
3.2. Results of Delphi Rounds 1–3
3.2.1. Conceptual Definitions (Items 1 and 2)
3.2.2. Operational Definitions/Thresholds (Items 3–6 and 10)
3.2.3. Intervention-Coverage (Item 7)
3.2.4. Elimination Measurement (Items 8 and 9)
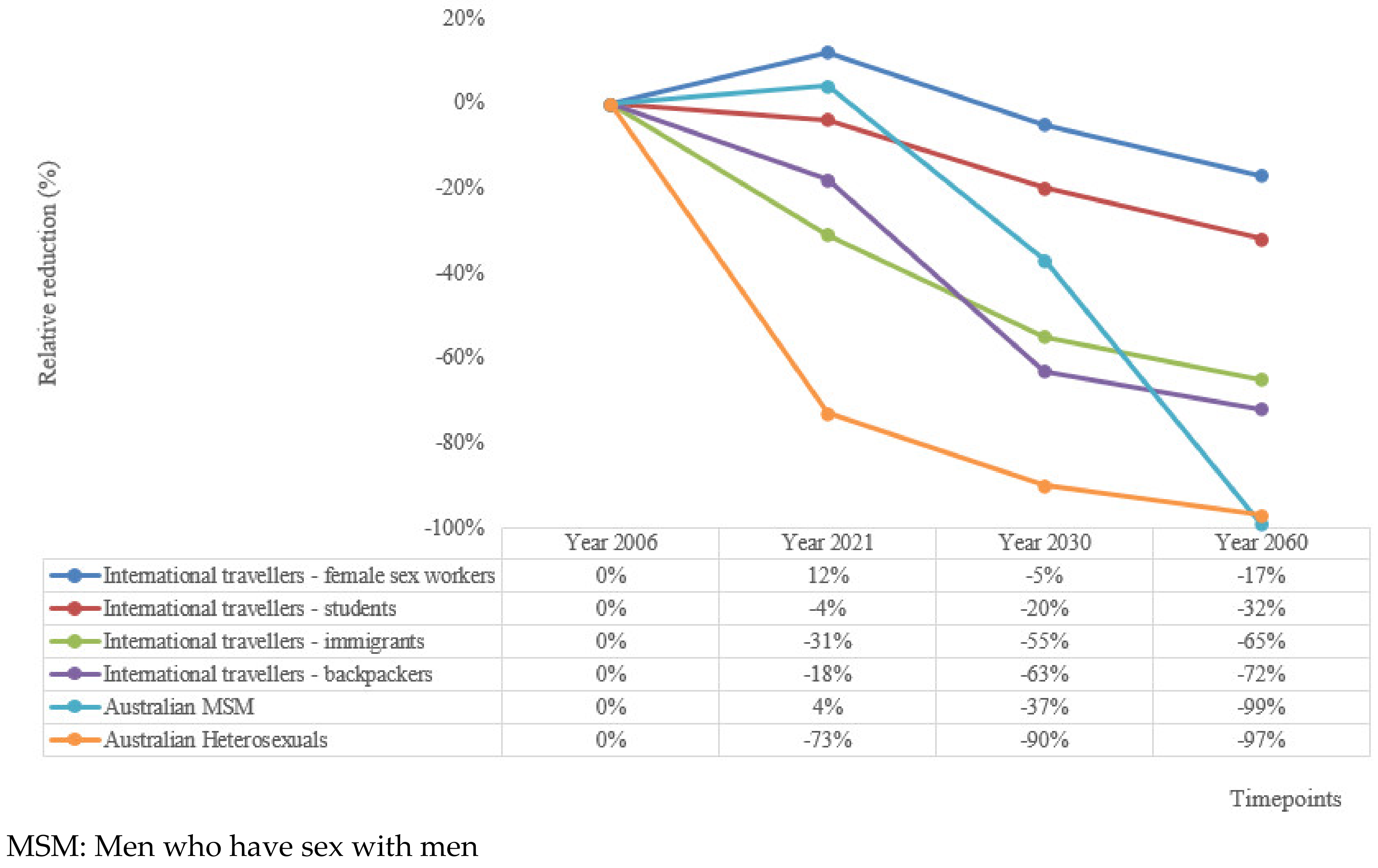
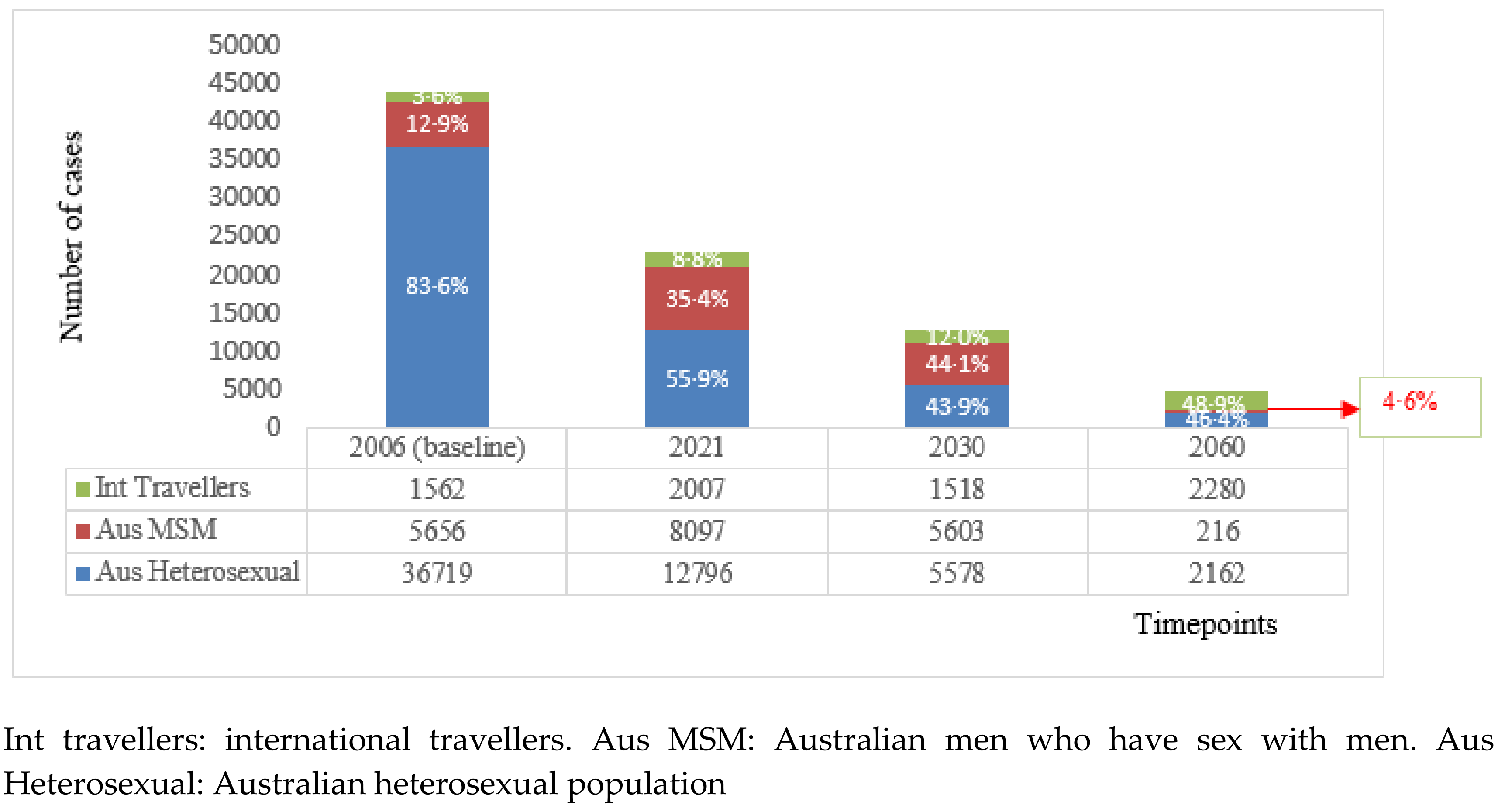
3.2.5. Revised Background Calculations
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Forman, D.; de Martel, C.; Lacey, C.J.; Soerjomataram, I.; Lortet-Tieulent, J.; Bruni, L.; Vignat, J.; Ferlay, J.; Bray, F.; Plummer, M.; et al. Global burden of human papillomavirus and related diseases. Vaccine 2012, 30, F12–F23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, L.-Y.; Garland, S.M. Human papillomavirus vaccination: The population impact. F1000Research 2017, 6, 866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Immunization, Vaccines and Biologicals-Human Papillomavirus (HPV). 2018. Available online: https://www.who.int/immunization/diseases/hpv/en/ (accessed on 26 September 2019).
- Brown, D.R.; Schroeder, J.M.; Bryan, J.T.; Stoler, M.H.; Fife, K.H. Detection of multiple human papillomavirus types in Condylomata acuminata lesions from otherwise healthy and immunosuppressed patients. J. Clin. Microbiol. 1999, 37, 3316–3322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Market Study HPV. 2018. Available online: https://www.who.int/immunization/programmes_systems/procurement/mi4a/platform/module2/WHO_HPV_market_study_public_summary.pdf (accessed on 10 November 2019).
- International Agency for Research on Cancer, World Health Organization. Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2018. Cervical Cancer Fact Sheet. 2018. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/23-Cervix-Uteri-fact-sheet.pdf (accessed on 25 November 2019).
- World Health Organization. Draft: Global Strategy towards the Elimination of Cervical Cancer as a Public Health Problem; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. Global Health Sector Strategy on Sexually Transmitted Infections 2016–2021-towards Ending STIs; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Drolet, M.; Bénard, É.; Pérez, N.; Brisson, M.; HPV Vaccination Impact Study Group. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: Updated systematic review and meta-analysis. Lancet 2019, 394, 497–509. [Google Scholar] [CrossRef] [Green Version]
- Garland, S.M.; Skinner, S.R.; Brotherton, J.M. Adolescent and young adult HPV vaccination in Australia: Achievements and challenges. Prev. Med. 2011, 53, S29–S35. [Google Scholar] [CrossRef] [PubMed]
- Brill, D. Australia launches national scheme to vaccinate boys against HPV. BMJ 2013, 346, f924. [Google Scholar] [CrossRef] [PubMed]
- Kirby Institute. HIV, Viral Hepatitis and Sexually Transmissible Infections in Australia: Annual Surveillance Report 2018; Kirby Institute: UNSW Sydney, Australia, 2018. [Google Scholar]
- World Health Organization. Generic Framework for Control, Elimination and Eradication of Neglected Tropical Diseases; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Korostil, I.A.; Ali, H.; Guy, R.J.; Donovan, B.; Law, M.G.; Regan, D.G. Near elimination of genital warts in Australia predicted with extension of human papillomavirus vaccination to males. Sex. Transm. Dis. 2013, 40, 833–835. [Google Scholar] [CrossRef]
- Zhang, L.; Regan, D.G.; Ong, J.J.; Gambhir, M.; Chow, E.P.F.; Zou, H.; Law, M.; Hocking, J.; Fairley, C.K. Targeted human papillomavirus vaccination for young men who have sex with men in Australia yields significant population benefits and is cost-effective. Vaccine 2017, 35, 4923–4929. [Google Scholar] [CrossRef] [Green Version]
- Brisson, M.; Bénard, É.; Drolet, M.; Bogaards, J.A.; Baussano, I.; Vänskä, S.; Jit, M.; Boily, M.C.; Smith, M.A.; Berkhof, J.; et al. Population-level impact, herd immunity, and elimination after human papillomavirus vaccination: A systematic review and meta-analysis of predictions from transmission-dynamic models. Lancet Public Health 2016, 1, e8–e17. [Google Scholar] [CrossRef] [Green Version]
- Ball, S.L.; Winder, D.M.; Vaughan, K.; Hanna, N.; Levy, J.; Sterling, J.C.; Stanley, M.A.; Goon, P.K.C. Analyses of human papillomavirus genotypes and viral loads in anogenital warts. J. Med. Virol. 2011, 83, 1345–1350. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, M.G.; Winder, D.M.; Ball, S.L.R.; Vaughan, K.; Sonnex, C.; Stanley, M.A.; Sterling, J.C.; Goon, P.K.C. Detection of specific HPV subtypes responsible for the pathogenesis of condylomata acuminata. Virol. J. 2013, 10, 137. [Google Scholar] [CrossRef] [Green Version]
- Hasson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 2000, 32, 1008–1015. [Google Scholar] [PubMed] [Green Version]
- Van Zolingen, S.J.; Klaassen, C.A. Selection processes in a Delphi study about key qualifications in senior secondary vocational education. Technol. Forecast. Soc. Chang. 2003, 70, 317–340. [Google Scholar] [CrossRef]
- Pirotta, M.; Stein, A.N.; Conway, E.L.; Harrison, C.; Britt, H.; Garland, S.M. Genital warts incidence and healthcare resource utilisation in Australia. Sex. Transm. Infect. 2010, 86, 181–186. [Google Scholar] [CrossRef]
- Manhart, L.E.; Koutsky, L.A. Do condoms prevent genital HPV infection, external genital warts, or cervical neoplasia? A meta-analysis. Sex. Transm. Dis. 2002, 29, 725–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, F.; Prestage, G.P.; Kippax, S.C.; Pell, C.M.; Donovan, B.; Templeton, D.J.; Kaldor, J.; Grulich, A.E. Risk factors for genital and anal warts in a prospective cohort of HIV-negative homosexual men: The HIM study. Sex. Transm. Dis. 2007, 34, 488–493. [Google Scholar] [CrossRef]
- Renshaw, L.; Kim, J.; Fawkes, J.; Jeffreys, E. Migrant Sex Workers in Australia. Research and Public Policy No. 131; Australian Institute of Criminology: Canberra, Australia, 2015.
- Hughes, K.; Downing, J.; Bellis, M.A.; Dillion, P.; Copeland, J. The sexual behaviour of British backpackers in Australia. Sex. Transm. Infect. 2009, 85, 477–482. [Google Scholar] [CrossRef]
- Rosenthal, D.A.; Russell, J.; Thomson, G. The health and wellbeing of international students at an Australian university. High. Educ. 2008, 55, 51–57. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 3222.0-Population Projections, Australia, 2012 (base) to 2101. 2013. Available online: http://www.abs.gov.au/ausstats/[email protected]/lookup/3222.0Media%20Release12012%20(base)%20to%202101 (accessed on 2 October 2019).
- Feiring, B.; Laake, I.; Christiansen, I.K.; Hansen, M.; Stålcrantz, J.; Ambur, O.H.; Magnus, P.; Jonassen, C.M.; Trogstad, L. Substantial decline in prevalence of vaccine-type and nonvaccine-type human papillomavirus (HPV) in vaccinated and unvaccinated girls 5 years after implementing HPV vaccine in Norway. J. Infect. Dis. 2018, 218, 1900–1910. [Google Scholar] [CrossRef]
- Donovan, B.; Franklin, N.; Guy, R.J.; Grulich, A.E.; Ali, H.; Wand, H.; Fairley, C.K. Quadrivalent human papillomavirus vaccination and trends in genital warts in Australia: Analysis of national sentinel surveillance data. Lancet Infect. Dis. 2011, 11, 39–44. [Google Scholar] [CrossRef]
- Denis Campbell. Genital Warts Vaccination to be Offered to Schoolgirls. Guardian 2011. Available online: https://www.theguardian.com/society/2011/nov/24/genital-warts-vaccination-offered-schoolgirls (accessed on 10 March 2020).
- Australian Government Department of Health. Fourth National Sexually Transmissible Infections Strategy 2018–2022. 2018. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/ohp-bbvs-1/$File/STI-Fourth-Nat-Strategy-2018-22.pdf (accessed on 26 September 2019).
- World Health Organization. A Framework for Malaria Elimination; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Framework for verifying elimination of measles and rubella. Wkly. Epidemiol. Rec. 2013, 88, 89–98. [Google Scholar]
- Danielewski, J.A.; Garland, S.M.; McCloskey, J.; Hillman, R.J.; Tabrizi, S.N. Human papillomavirus type 6 and 11 genetic variants found in 71 oral and anogenital epithelial samples from Australia. PLoS ONE 2013, 8, e63892. [Google Scholar] [CrossRef] [PubMed]
- Heinzel, P.A.; Chan, S.-Y.; Ho, L.; O’Connor, M.; Balaram, P.; Campo, M.S.; Fujinaga, K.; Kiviat, N.; Kuypers, J.; Pfister, H. Variation of human papillomavirus type 6 (HPV-6) and HPV-11 genomes sampled throughout the world. J. Clin. Microbiol. 1995, 33, 1746–1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jelen, M.M.; Chen, Z.; Kocjan, B.J.; Burt, F.J.; Chan, P.K.S.; Chouhy, D.; Combrinck, C.E.; Coutlée, F.; Estrade, C.; Ferenczy, A.; et al. Global genomic diversity of human papillomavirus 6 based on 724 isolates and 190 complete genome sequences. J. Virol. 2014, 88, 7307–7316. [Google Scholar] [CrossRef] [Green Version]
- Vinicor, F. Is diabetes a public-health disorder? Diabetes Care 1994, 17, 22–27. [Google Scholar]
- Schoolwerth, A.C.; Engelgau, M.M.; Rufo, K.H.; Vinicor, F.; Hostetter, T.H.; Chianchiano, D.; McClellan, W.M.; Warnock, D.G. Chronic Kidney Disease: A Public Health Problem That Needs a Public Health Action Plan. Prev. Chronic Dis. 2006, 3, A57. [Google Scholar]
- Pirotta, M.; Ung, L.; Stein, A.; Conway, E.L.; Mast, T.C.; Fairley, C.K.; Garland, S. The psychosocial burden of human papillomavirus related disease and screening interventions. Sex. Transm. Infect. 2009, 85, 508–513. [Google Scholar] [CrossRef]
- Conley, L.J.; Ellerbrock, T.V.; Bush, T.J.; Chiasson, M.A.; Sawo, D.; Wright, T.C. HIV-1 infection and risk of vulvovaginal and perianal condylomata acuminata and intraepithelial neoplasia: A prospective cohort study. Lancet 2002, 359, 108–113. [Google Scholar] [CrossRef]
- Hounsfield, V.L.; Freedman, E.; McNulty, A.; Bourne, C. Transgender people attending a Sydney sexual health service over a 16-year period. Sex. Health 2007, 4, 189–193. [Google Scholar] [CrossRef]
- O’Connor, C.; Berry, G.; Rohrsheim, R.; Donovan, B. Sexual health and use of condoms among local and international sex workers in Sydney. Sex. Transm. Infect. 1996, 72, 47–51. [Google Scholar] [CrossRef] [Green Version]
- Department of Education and Training Australian Government. International Student Data 2017; Basic Pivot Table 2002 Onwards. 2017. Available online: https://internationaleducation.gov.au/research/International-Student-Data/Pages/InternationalStudentData2017.aspx#Pivot_Table (accessed on 26 September 2019).
- Tota, J.E.; Jiang, M.; Ramanakumar, A.V.; Walter, S.D.; Kaufman, J.S.; Coutlée, F.; Richardson, H.; Burchell, A.N.; Kouchik, A.; Maryand, M.H.; et al. Epidemiologic evaluation of human papillomavirus type competition and the potential for type replacement post-vaccination. PLoS ONE 2016, 11, e0166329. [Google Scholar] [CrossRef] [PubMed]
- Enerly, E.; Olofsson, C.; Nygård, M. Monitoring human papillomavirus prevalence in urine samples: A review. Clin. Epidemiol. 2013, 5, 67–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vorsters, A.; Micalessi, I.; Bilcke, J.; Ieven, M.; Bogers, J.; Van, D.P. Detection of human papillomavirus DNA in urine. A review of the literature. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 627–640. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, A.; Gupta, S.; Parashari, A.; Sodhani, P.; Singh, V. Urine HPV-DNA detection for cervical cancer screening: Prospects and prejudices. J. Obstet. Gynaecol. 2009, 29, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhan, S.; Amin, T.; Sampat, B.; Cook-Deegan, R.; Chandrasekharan, S. Intellectual property, technology transfer and manufacture of low-cost HPV vaccines in India. Nat. Biotechnol. 2010, 28, 671–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, M.L.; Figueroa-Downing, D.; Chiang, E.D.D.O.; Villa, L.; Baggio, M.L.; Eluf-Neto, J.; Bednarczyk, R.A.; Evans, D.P. Paving pathways: Brazil’s implementation of a national human papillomavirus immunization campaign. Rev. Panam. Salud Publica 2015, 38, 163–166. [Google Scholar]
- Brotherton, J.M.; Budd, A.; Rompotis, C.; Barlett, N.; Malloy, M.J.; Andersen, R.L.; Coulter, K.A.R.; Couvee, P.W.; Steel, N.; Ward, G.H.; et al. Is one dose of human papillomavirus vaccine as effective as three? A national cohort analysis. Papillomavirus Res. 2019, 8, 100177. [Google Scholar] [CrossRef]
- Webler, T.; Levine, D.; Rakel, H.; Renn, O. A novel approach to reducing uncertainty: The group Delphi. Technol. Forecast. Soc. Chang. 1991, 39, 253–263. [Google Scholar] [CrossRef]
- Bolger, F.; Wright, G. Improving the Delphi process: Lessons from social psychological research. Technol. Forecast. Soc. Chang. 2011, 78, 1500–1513. [Google Scholar] [CrossRef]
- Beretta, R. A critical review of the Delphi technique. Nurs. Res. 1996, 3, 79–89. [Google Scholar] [CrossRef]
- Kennedy, H.P. A model of exemplary midwifery practice: Results of a Delphi study. J. Midwifery Women Health 2000, 45, 4–19. [Google Scholar] [CrossRef]
- Hall, M.T.; Simms, K.T.; Lew, J.-B.; Smith, M.A.; Brotherton, J.M.; Saville, M.; Frazer, I.H.; Canfell, K. The projected timeframe until cervical cancer elimination in Australia: A modelling study. Lancet Public Health 2019, 4, e19–e27. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Australian | New Genital Warts Cases—n (95% CI) | Rate Per 10,000 Persons | Relative Reduction (%) | ||||
|---|---|---|---|---|---|---|---|
| Population | (95% CI) | in New Genital Warts | |||||
| International | Australian Heterosexual | Australian MSM | Consolidated Cases | from Baseline (95% CI) | |||
| Travellers | Population | Population | |||||
| Baseline (2006) | 20,091,504 | 1562 (1428–1707) | 36,719 (31,579–42,181) | 5656 (5512–5803) | 43,937 (38,519–49,691) | 21.9 (19.2–24.7) | .. |
| 2021 | 26,110,176 | 1634 (1492–1788) | 10,419 (9849–13,155) | 6593 (6437–6752) | 18,647 (17,777–21,695) | 7.1 (6.8–8.3) | 67.3 (66.8–67.9) |
| 2030 | 29,748,172 | 1364 (1232–1510) | 5012 (4350–5811) | 5034 (4897–5174) | 11,410 (10,479–12,494) | 3.8 (3.5–4.2) | 82.4 (82.1–82.8) |
| 2060 | 40,703,739 | 2280 (2110–2462) | 2162 (1876–2506) | 216 (188–247) | 4658 (4174–5215) | 1.1 (1.0–1.3) | 94.7 (94.6–94.9) |
| Delphi Workshop (n = 18) | Online Round (n = 16) | |
|---|---|---|
| Gender | ||
| Female | 72% | 69% |
| Male | 28% | 31% |
| Age group | ||
| ≤35 years | 11% | 13% |
| 35–44 years | 22% | 25% |
| 45–54 years | 50% | 50% |
| ≥55 years | 17% | 13% |
| Education | ||
| Masters | 6% | 6% |
| Medical degree | 11% | 6% |
| PhD | 83% | 88% |
| Professional level | ||
| Professional (non-academic) | 11% | 6% |
| Early-/mid-career academic | 22% | 25% |
| Senior academic | 67% | 69% |
| Expertise | ||
| Health policy | 6% | 6% |
| Statistics | 6% | 6% |
| Mathematical modelling | 22% | 25% |
| Vaccination/immunology | 22% | 13% |
| Epidemiology | 22% | 25% |
| Clinical and epidemiology | 17% | 19% |
| Other | 6% | 6% |
| Revised Items for Round 2 of the Delphi Workshop | Median | Mean | % Agreement | % Disagreement | Outcome |
|---|---|---|---|---|---|
| (IQR) | (COV) | (Scores 7,8 & 9) | (Scores 1,2,3 & 4) | ||
| Section-1: Conceptual definitions | |||||
| Item-1: Elimination of (endemic) transmission: Interruption of endemic genital warts transmission caused by HPV 6 and 11, and limited transmission from imported cases. | 4.5 | 4.3 | 25% | 50% | To revise item as per |
| (2.5–6.3) | (0.65) | experts’ feedback | |||
| Item-2: Elimination as a public health problem: Transmission of genital warts continues to occur (even in absence of importation) but is reduced to a level that it does not constitute a public health problem. | 6.5 | 6.7 | 50% | 25% | To revise item as per |
| (5.5–7.5) | (0.31) | experts’ feedback | |||
| Section-2: Operational thresholds | |||||
| Short-term control threshold: ≤4 cases per 10,000 population by year 2030; Equivalent to: A reduction in annual genital warts incidence by 82% by year | .. | .. | .. | .. | .. |
| 2030 | |||||
| Long-term elimination threshold: ≤1 case per 10,000 population by year 2060; Equivalent to: A reduction | .. | .. | .. | .. | .. |
| in annual genital warts incidence by 95% by year 2060 | |||||
| Item 3: The proportion of genital warts caused by non-vaccine HPV types will have an impact on the control threshold in year 2030 | 2.5 | 3.5 | 25% | 75% | To revise item as per |
| (1.7–4.2) | (0.89) | experts’ feedback | |||
| Item 4: Ongoing transmission of genital warts in Australia due to importation would have an impact on the control threshold in year 2030 | 3.5 | 3.8 | 25% | 50% | To revise item as per |
| (1.7–5.5) | (0.70) | experts’ feedback | |||
| Item 5: The proportion of genital warts caused by non-vaccine HPV types will have an impact on the elimination threshold in year 2060 | 6.0 | 5.8 | 50% | 25% | To revise item as per |
| (4.2–7.5) | (0.52) | experts’ feedback | |||
| Item 6: Ongoing transmission of genital warts in Australia due to importation would have an impact on the elimination threshold in year 2060 | 3.5 | 4.0 | 25% | 50% | To revise item as per |
| (1.7–5.7) | (0.79) | experts’ feedback | |||
| Section-3 Intervention coverage/Process threshold | |||||
| Item 7: Completion of HPV vaccination course is equal to or greater than 80% coverage in the target population | 8.0 | 7.8 | 75% | Consensus met– | |
| (7.5–8.2) | (0.16) | accept | |||
| Section-4: Measuring elimination | |||||
| Item 8: There needs to be measurement of genital warts from both general practice and sexual health clinics | 9.0 | 8.3 | 75% | .. | Consensus met– |
| (8.2–9.0) | (0.18) | accept | |||
| Item 9 (new item): Measurement should also include genotyping of genital warts | 8.0 | 8.0 | 100% | .. | Consensus met– |
| (7.0–9.0) | (0.14) | .. | accept | ||
| Revised Items for the Online Round | Median | Mean | % Agreement | % Disagreement | Outcome |
|---|---|---|---|---|---|
| (IQR) | (COV) | (Scores 7,8 & 9) | (Scores 1,2,3 & 4) | ||
| Conceptual definitions | |||||
| Item 1: Elimination of (endemic) transmission: Defining genital warts elimination as interruption of endemic HPV 6 & 11 transmission is not feasible due to a lack of geographic variation in HPV 6&11 subtype distribution | 7.0 | 6.9 | 81% | 6% | Consensus met– |
| (7.0–8.0) | (0.20) | agreed to reject | |||
| Item 2: Elimination as a public health problem: To reduce the burden of genital warts to a level where it no longer constitutes a public health problem | 8.0 | 7.4 | 81% | 6% | Consensus met– |
| (7.0–9.0) | (0.20) | accept | |||
| Operational thresholds^ | |||||
| Item 10 (new item): Control milestone for the year 2021—A 60% relative reduction in new genital warts diagnoses by year 2021 at a population level, as compared to the baseline of 2006; Equivalent to: Reduction of new cases of genital warts to ≤9 cases per 10,000 population by year 2021 | 7.5 | 6.8 | 75% | 13% | Consensus met– |
| (6.8–8.0) | (0.30) | accept | |||
| Item 4*: Control threshold for the year 2030—An 80% relative reduction since 2006 in new genital warts diagnoses by year 2030 at a population level, as compared to the baseline of 2006; Equivalent to: Reduction of new cases of genital warts to ≤4 cases per 10,000 population by year 2030 | 7.5 | 6.9 | 81% | 13% | Consensus met– |
| (7.0–8.0) | (0.27) | accept | |||
| Item 6*: Elimination threshold for the year 2060—A 95% relative reduction since 2006 in new genital warts diagnoses by year 2060 at a population level, as compared to the baseline of 2006 Equivalent to: Reduction of new cases of genital warts to ≤1 case per 10,000 population by year 2030 | 7.0 | 7.0 | 75% | 6% | Consensus met– |
| (6.8–8.0) | (0.24) | accept | |||
| Australian | New GW Cases—n (95% CI) | Rate Per 10,000 Persons | Relative Reduction (%) | ||||
|---|---|---|---|---|---|---|---|
| Population | (95% CI) | in New Genital Warts from | |||||
| International | Australian Heterosexual | Australian MSM | Consolidated | Baseline (95% CI) | |||
| Travellers | Population | Population | |||||
| Baseline (2006) | 20,091,504 | 1,562 (1,428–1,707) | 36,719 (31,579–42,181) | 5656 (5512–5803) | 43,937 (38,519–49,691) | 21.9 (19.2–24.7) | .. |
| 2021 | 26,110,176 | 2007 (1849–2177) | 12,796 (11,255–15,034) | 8097 (7924–8072) | 22,900 (21,029–25,483) | 8.8 (8.1–9.8) | 59.9 (59.2–60.5) |
| 2030 | 29,748,172 | 1518 (1377–1670) | 5578 (5037–6728) | 5603 (5459–5750) | 12,700 (11,873–14,149) | 4.3 (4.0–4.8) | 80.4 (80.1–80.9) |
| 2060 | 40,703,739 | 2280 (2110–2462) | 2162 (1876–2506) | 216 (188–247) | 4658 (4174–5215) | 1.1 (1.0–1.3) | 94.8 (94.6–94.9) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khawar, L.; Machalek, D.A.; Regan, D.G.; Donovan, B.; McGregor, S.; Guy, R.J. Defining Elimination of Genital Warts—A Modified Delphi Study. Vaccines 2020, 8, 316. https://doi.org/10.3390/vaccines8020316
Khawar L, Machalek DA, Regan DG, Donovan B, McGregor S, Guy RJ. Defining Elimination of Genital Warts—A Modified Delphi Study. Vaccines. 2020; 8(2):316. https://doi.org/10.3390/vaccines8020316
Chicago/Turabian StyleKhawar, Laila, Dorothy A. Machalek, David G. Regan, Basil Donovan, Skye McGregor, and Rebecca J. Guy. 2020. "Defining Elimination of Genital Warts—A Modified Delphi Study" Vaccines 8, no. 2: 316. https://doi.org/10.3390/vaccines8020316
APA StyleKhawar, L., Machalek, D. A., Regan, D. G., Donovan, B., McGregor, S., & Guy, R. J. (2020). Defining Elimination of Genital Warts—A Modified Delphi Study. Vaccines, 8(2), 316. https://doi.org/10.3390/vaccines8020316