Impact of COVID-19 on Immunization Services for Maternal and Infant Vaccines: Results of a Survey Conducted by Imprint—The Immunising Pregnant Women and Infants Network


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Survey Description
2.3. Survey Validation
2.4. Ethics Approval and Data Management
2.5. Survey Analysis: Quantitative
Survey Analysis: Qualitative
3. Results
3.1. Quantitative Findings
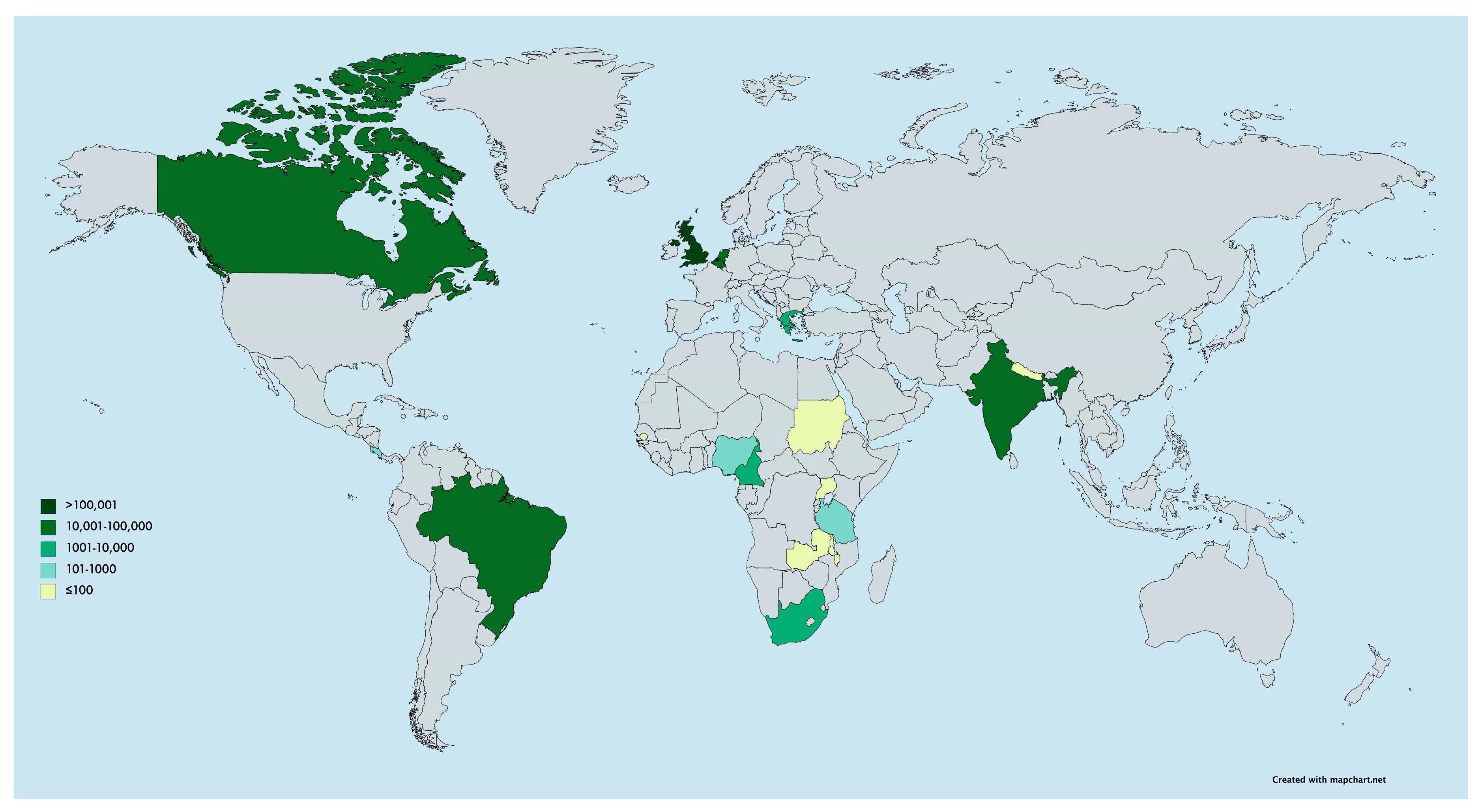
3.1.1. Participants
3.1.2. Routine Vaccine Schedules and Delivery Locations Prior to COVID-19
3.1.3. Changes to Vaccine Delivery since the COVID-19 Pandemic
3.2. Qualitative Findings
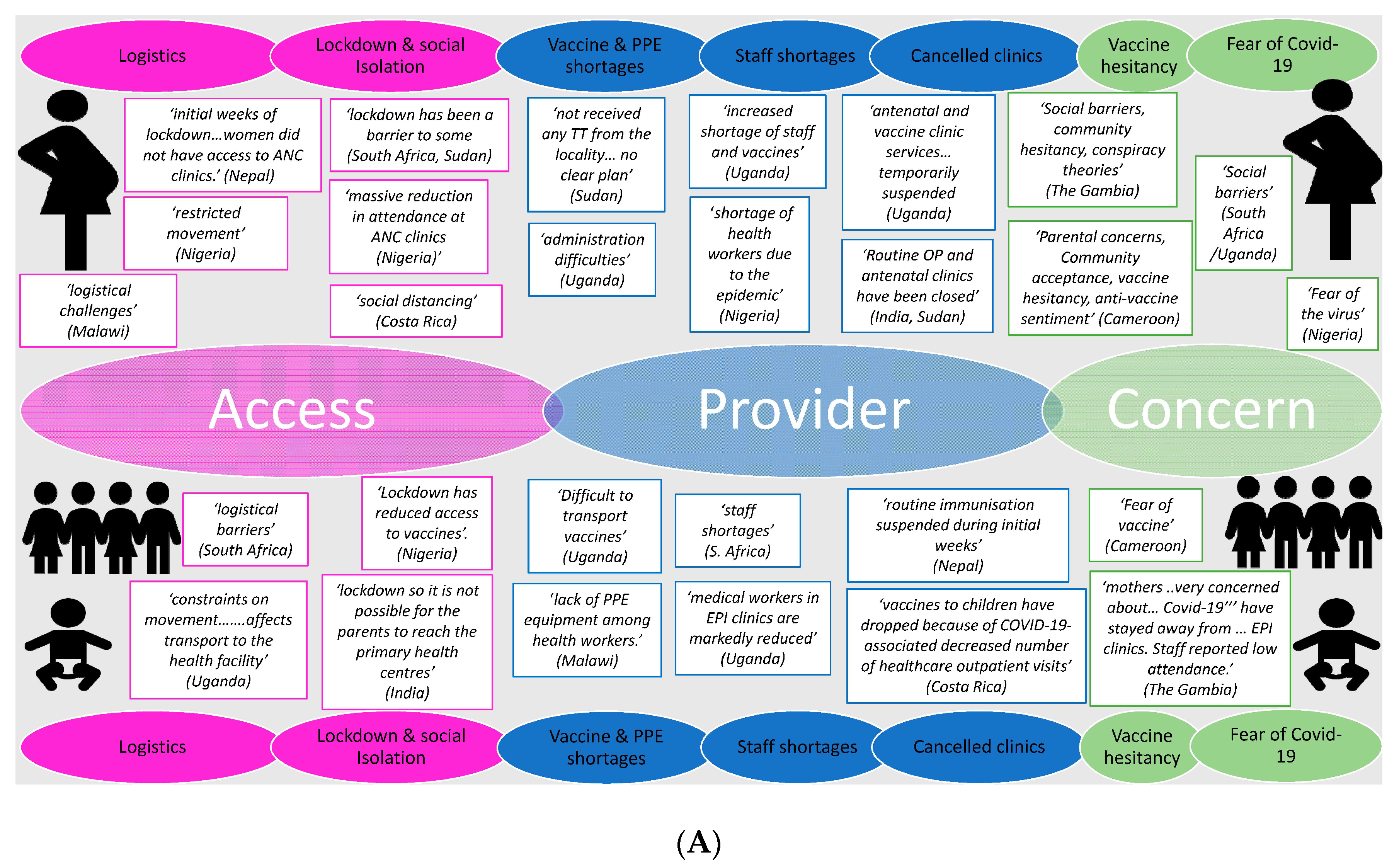
3.2.1. Issues around Vaccine Delivery and Uptake
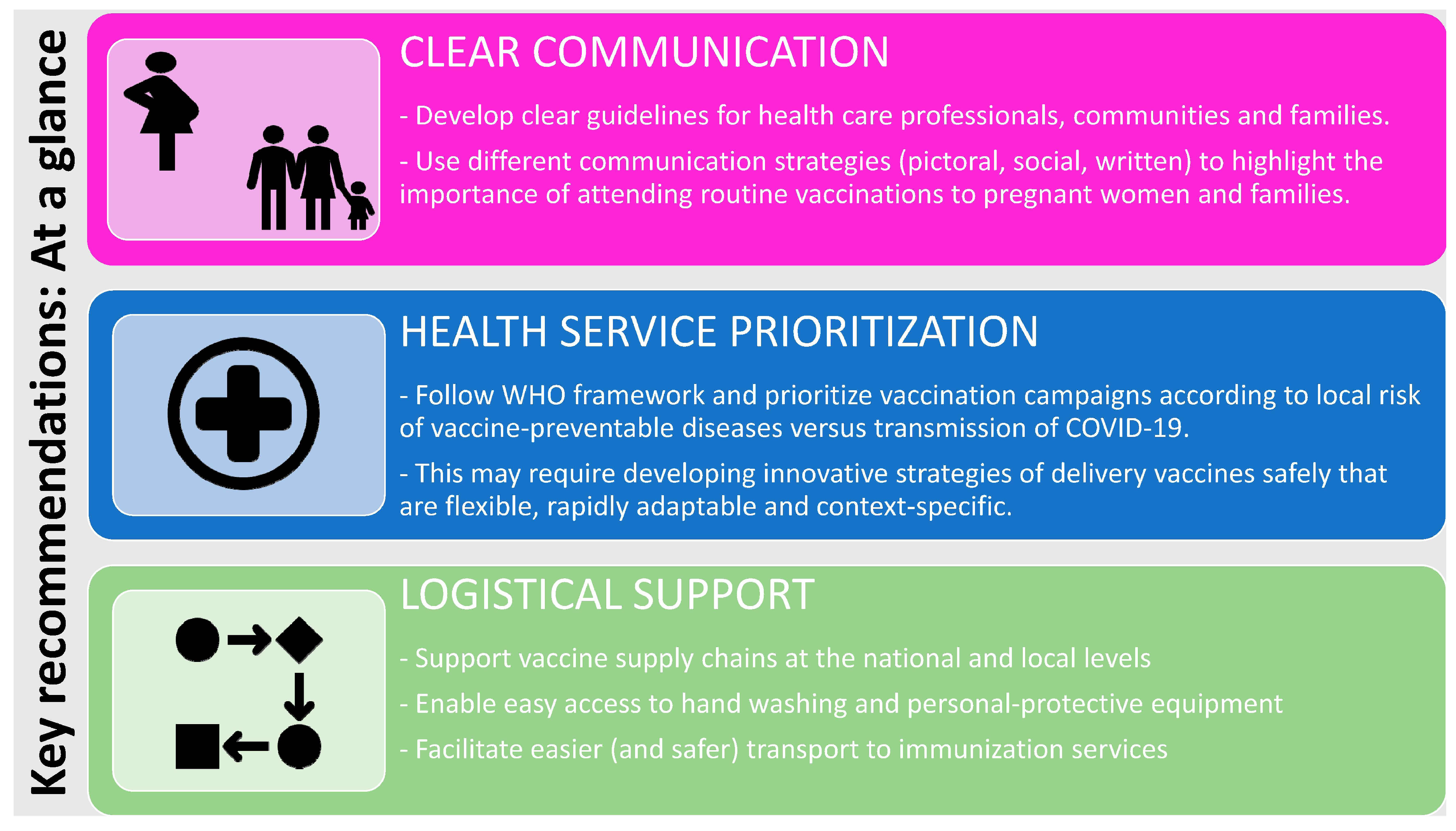
3.2.2. Regional, National and International Recommendations and Guidelines
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- LSHTM London School of Hygiene and Tropical Medicine. COVID-19 Tracker. Available online: https://vac-lshtm.shinyapps.io/ncov_tracker/ (accessed on 1 May 2020).
- Williamson, E.; Walker, A.J.; Bhaskaran, K.J.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. OpenSAFELY: Factors associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients. medRxiv 2020. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. SARS-CoV-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoang, A.; Chorath, K.; Moreira, A.; Evans, M.; Burmeister-Morton, F.; Burmeister, F.; Naqvi, R.; Petershack, M.; Moreira, A. COVID-19 in 7780 pediatric patients: A systematic review. EClinicalMedicine 2020, 24, 100433. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, J.; Friedland, G. Preventing COVID-19 Collateral Damage. Clin. Infect. Dis. 2020, 71, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Roberton, T.; Carter, E.D.; Chou, V.B.; Stegmuller, A.R.; Jackson, B.D.; Tam, Y.; Sawadogo-Lewis, T.; Walker, N. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e901–e908. [Google Scholar] [CrossRef]
- Saxena, S.; Skirrow, H.; Bedford, H. Routine vaccination during covid-19 pandemic response. BMJ 2020, 369, m2392. [Google Scholar] [CrossRef] [PubMed]
- WHO. Unicef Immunization Coverage: Are We Losing Ground? Available online: https://data.unicef.org/resources/immunization-coverage-are-we-losing-ground/ (accessed on 6 July 2020).
- Abbas, K.; Procter, S.R.; van Zandvoort, K.; Clark, A.; Funk, S.; Mengistu, T.; Hogan, D.; Dansereau, E.; Jit, M.; Flasche, S.; et al. Routine childhood immunisation during the COVID-19 pandemic in Africa: A benefit-risk analysis of health benefits versus excess risk of SARS-CoV-2 infection. Lancet Glob. Health 2020. [Google Scholar] [CrossRef]
- WHO. World Health Organisation: News Release. At Least 80 Million Children under One at Risk of Diseases Such as Diphtheria, Measles and Polio as COVID-19 Disrupts Routine Vaccination Efforts, Warn Gavi, WHO and UNICEF. Available online: https://www.who.int/news-room/detail/22-05-2020-at-least-80-million-children-under-one-at-risk-of-diseases-such-as-diphtheria-measles-and-polio-as-covid-19-disrupts-routine-vaccination-efforts-warn-gavi-who-and-unicef (accessed on 30 May 2020).
- WHO. Carolina Danovaro, Santosh Gurung, Lee Lee Ho, and Ann Lindstrand, Understanding the Disruption to Programmes through Rapid Polling. Available online: https://www.who.int/immunization/GIN_March-April_2020.pdf?ua=1 (accessed on 30 May 2020).
- WHO. Special Feature: Immunization and COVID-19: Second Pulse Poll. WHO, UNICEF & Gavi, in Collaboration with the Sabin Vaccine Institute’s Boost Community and the International Vaccine Access Center (IVAC) at Johns Hopkins and the Global Immunization Division/United States Centers for Disease Control and Prevention (CDC). Available online: https://www.who.int/immunization/monitoring_surveillance/immunization-and-covid-19/en/ (accessed on 6 July 2020).
- Roberts, L. Why measles deaths are surging—And coronavirus could make it worse. Nature 2020, 580, 446–447. [Google Scholar] [CrossRef]
- WHO. Statement by the Measles & Rubella Initiative: American Red Cross, U.S. CDC, UNICEF, UN Foundation and WHO. More than 117 Million Children at Risk of Missing out on Measles Vaccines, as COVID-19 Surges. Available online: https://www.who.int/immunization/diseases/measles/statement_missing_measles_vaccines_covid-19/en/ (accessed on 30 May 2020).
- IMPRINT. The Imprint Network. Available online: www.imprint-network.co.uk (accessed on 30 May 2020).
- DAC Development Assistance Committee. List of Official Development Assistance (ODA) Recipients for Reporting on Aid in 2020. Available online: http://www.oecd.org/dac/financing-sustainable-development/development-finance-standards/daclist.htm (accessed on 20 May 2020).
- AAPOR American Association for Public Opinion Research. Best Practices for Survey Research. Available online: https://www.aapor.org/Standards-Ethics/Best-Practices.aspx (accessed on 30 May 2020).
- Kelley, K.; Clark, B.; Brown, V.; Sitzia, J. Good practice in the conduct and reporting of survey research. Int. J. Qual. Health Care 2003, 15, 262–266. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Vaccine-Preventable Diseases: Monitoring System. 2019 Global Summary. Immunization Schedule Selection Centre. Available online: https://apps.who.int/immunization_monitoring/globalsummary/schedules (accessed on 6 May 2020).
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Richards, S.H.; Campbell, J.L.; Walshaw, E.; Dickens, A.; Greco, M. A multi-method analysis of free-text comments from the UK General Medical Council Colleague Questionnaires. Med. Educ. 2009, 43, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Corner, J.; Wagland, R.; Glaser, A.; Richards, S.M. Qualitative analysis of patients’ feedback from a PROMs survey of cancer patients in England. BMJ Open 2013, 3, e002316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for Reporting Qualitative Research: A Synthesis of Recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Ministerie van Volksgezondheid, Welzijn en Sport. Dutch National Immunisation Programme. Available online: https://rijksvaccinatieprogramma.nl/english (accessed on 6 May 2020).
- WHO. Framework for Decision-Making: Implementation of Mass Vaccination Campaigns in the Context of COVID-19; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Ministry of Health and Family Welfare, Government of India. Enabling Delivery of Essential Health Services during the COVID 19 Outbreak: Guidance Note; Ministry of Health and Family Welfare: New Delhi, India, 2020. [Google Scholar]
- WHO Regional Office for Europe. Guidance on Routine Immunization Services during COVID-19 Pandemic in the WHO European Region. Available online: https://www.euro.who.int/__data/assets/pdf_file/0004/433813/Guidance-routine-immunization-services-COVID-19-pandemic.pdf?ua=1 (accessed on 30 May 2020).
- NHS. Covid-19 Prioritisation of Community Health Services. Available online: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/C0145-COVID-19-prioritisation-within-community-health-services-1-April-2020.pdf (accessed on 1 May 2020).
- PHE. Keep Calm and Carry on Vaccinating. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/873961/Vaccine_Update_306_March_2020.pdf (accessed on 22 September 2020).
- BCCDC British Columbia Centre for Disease Control. Continuity of Immunization Services during COVID-19 Pandemic. Available online: http://www.bccdc.ca/resource-gallery/Documents/Guidelines%20and%20Forms/Guidelines%20and%20Manuals/Epid/CD%20Manual/Chapter%202%20-%20Imms/Continuity_of_Immunization_Services_During_COVID-19.pdf (accessed on 30 May 2020).
- ImmunizeBC Home Page. Available online: https://immunizebc.ca/ (accessed on 30 May 2020).
- RCOG Royal College of Obstetricians and Gynaecologists. Coronavirus Infection in Pregnancy. Available online: https://www.rcog.org.uk/globalassets/documents/guidelines/2020-06-18-coronavirus-covid-19-infection-in-pregnancy.pdf (accessed on 30 May 2020).
- RCPCH, Royal College of Paediatrics and Child Health. COVID-19—Guidance for Paediatric Services; RCPCH: London, UK, 2020. [Google Scholar]
- RCN Royal College of Nursing. Overarching Principles for Maintaining the National Immunisation Programme during the COVID-19 Pandemic; Royal College of Nursing: London, UK, 2020. [Google Scholar]
- RCGP Royal College of General Practitioners. Guidance on Workload Prioritisation during COVID-19; Version 8. 2020. Available online: https://www.rcgp.org.uk/-/media/Files/Policy/A-Z-policy/2020/covid19/RCGP-guidance/202003233RCGPGuidanceprioritisationroutineworkduringCovidFINAL.ashx?la=en (accessed on 30 May 2020).
- MySurgeryWebsitemobile. NHS Immunisations FAQs (for Public). Available online: http://www.mysurgerywebsitemobile.co.uk/website/B82025/files/20200327Covid-19%20Immunisations%20FAQs.pdf (accessed on 30 May 2020).
- Chandir, S.; Siddiqi, D.; Setayesh, H.; Khan, A. Impact of COVID-19 lockdown on routine immunisation in Karachi, Pakistan. Lancet Glob. Health 2020, 8, e1118–e1120. [Google Scholar] [CrossRef]
- McDonald, H.I.; Tessier, E.; White, J.M.; Woodruff, M.; Knowles, C.; Bates, C.; Parry, J.; Walker, J.L.; Scott, J.A.; Smeeth, L.; et al. Early impact of the coronavirus disease (COVID-19) pandemic and physical distancing measures on routine childhood vaccinations in England, January to April 2020. Eurosurveillance 2020, 25, 2000848. [Google Scholar] [CrossRef]
- PHS Public Health Scotland. Uptake of First Dose of 6-in-1 Vaccine (Offered to Children at 8 Weeks of Age): Scotland. Scottish Immunisation and Recall System. Available online: https://scotland.shinyapps.io/phs-covid-wider-impact/ (accessed on 30 May 2020).
- Santoli, J.M.; Lindley, M.C.; DeSilva, M.B.; Kharbanda, E.O.; Daley, M.F.; Galloway, L.; Gee, J.; Glover, M.; Herring, B.; Kang, Y. Effects of the COVID-19 Pandemic on Routine Pediatric Vaccine Ordering and Administration—United States, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 591–593. [Google Scholar] [CrossRef]
- Martinez-Alvarez, M.; Jarde, A.; Usuf, E.; Brotherton, H.; Bittaye, M.; Samateh, A.L.; Antonio, M.; Vives-Tomas, J.; D’Alessandro, U.; Roca, A. COVID-19 pandemic in west Africa. Lancet Glob. Health 2020, 8, e631–e632. [Google Scholar] [CrossRef]
- Brolin Ribacke, K.J.; van Duinen, A.J.; Nordenstedt, H.; Höijer, J.; Molnes, R.; Froseth, T.W.; Koroma, A.P.; Darj, E.; Bolkan, H.A.; Ekström, A. The Impact of the West Africa Ebola Outbreak on Obstetric Health Care in Sierra Leone. PLoS ONE 2016, 11, e0150080. [Google Scholar] [CrossRef]
- UNICEF. Geneva Palais Briefing Note on the Impact of COVID-19 Mitigation Measures on Vaccine Supply and Logistics. Available online: https://www.unicef.org/press-releases/geneva-palais-briefing-note-impact-covid-19-mitigation-measures-vaccine-supply-and (accessed on 30 May 2020).
- Suk, J.E.; Paez Jimenez, A.; Kourouma, M.; Derrough, T.; Baldé, M.; Honomou, P.; Kolie, N.; Mamadi, O.; Tamba, K.; Lamah, K.; et al. Post-Ebola Measles Outbreak in Lola, Guinea, January–June 2015. Emerg. Infect. Dis. 2016, 22, 1106–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyer, O. DRC faces new Ebola outbreak, covid-19, and measles all at once. BMJ 2020, 369, m2219. [Google Scholar] [CrossRef] [PubMed]
- Oyo-Ita, A.; Wiysonge, C.S.; Oringanje, C.; Nwachukwu, C.E.; Oduwole, O.; Meremikwu, M.M. Interventions for improving coverage of childhood immunisation in low- and middle-income countries. Cochrane Database Syst. Rev. 2016, 7, CD008145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, H.J. A call to arms: Helping family, friends and communities navigate the COVID-19 infodemic. Nat. Rev. Immunol. 2020, 20, 449–450. [Google Scholar] [CrossRef]
- Depoux, A.; Martin, S.; Karafillakis, E.; Preet, R.; Wilder-Smith, A.; Larson, H. The pandemic of social media panic travels faster than the COVID-19 outbreak. J. Travel Med. 2020, 27, taaa031. [Google Scholar] [CrossRef] [Green Version]
- Harrison, E.A.; Wu, J.W. Vaccine confidence in the time of COVID-19. Eur. J. Epidemiol. 2020, 35, 325–330. [Google Scholar] [CrossRef] [Green Version]
- Dyer, O. Covid-19: Trump stokes protests against social distancing measures. BMJ 2020, 369, m1596. [Google Scholar] [CrossRef] [Green Version]
- JCVI. Statement from the Joint Committee on Vaccination and Immunisation (JCVI) on Immunisation Prioritisation. Available online: https://www.gov.uk/government/publications/jcvi-statement-on-immunisation-prioritisation (accessed on 30 May 2020).
- NHS. PHE Clinical Guidance for Healthcare Professionals on Maintaining Immunisation Programmes During COVID-19. Supported by the RCGP and RCPCH. Available online: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/06/clinical-guidance-for-hcps-on-imms-for-covid-19.pdf (accessed on 6 July 2020).
- Isenor, J.E.; Edwards, N.T.; Alia, T.A.; Slayter, K.L.; MacDougall, D.M.; McNeil, S.A.; Bowles, S.K. Impact of pharmacists as immunizers on vaccination rates: A systematic review and meta-analysis. Vaccine 2016, 34, 5708–5723. [Google Scholar] [CrossRef]
- Hussain, D. Childhood Immunisations: How a Practice Reduced Face-to-Face Time. Available online: https://www.nursinginpractice.com/covid-19/childhood-immunisations-how-practice-reduced-face-face-time (accessed on 1 May 2020).
- GAVI, The Vaccine Alliance. World Leaders Make Historic Commitments to Provide Equal Access to Vaccines for All. Available online: https://www.gavi.org/news/media-room/world-leaders-make-historic-commitments-provide-equal-access-vaccines-all (accessed on 1 July 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Occupation | N (%) |
|---|---|
| Healthcare Professional (Doctor, nurse, midwife and private healthcare provider) | 27 (56.3) |
| Laboratory based scientist | 11 (22.9) |
| Public Health Official | 4 (8.3) |
| Other * | 6 (12.5) |
| Country | Total Respondents (n) | Number of Respondents Reporting Issues Delivering Maternal Vaccines (%) | Number of Respondents Reporting Issues Delivery Newborn Vaccines (%) | Number of Respondents Reporting Issues Delivering Infant and Childhood Vaccines (%) |
|---|---|---|---|---|
| All | 48 | 24 (50) | 16 (33) | 26 (54) |
| LMIC | 36 | 19 (53) | 15 (42) | 19 (53) |
| HIC | 12 | 5 (42) | 1 (8) | 7 (58) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saso, A.; Skirrow, H.; Kampmann, B. Impact of COVID-19 on Immunization Services for Maternal and Infant Vaccines: Results of a Survey Conducted by Imprint—The Immunising Pregnant Women and Infants Network. Vaccines 2020, 8, 556. https://doi.org/10.3390/vaccines8030556
Saso A, Skirrow H, Kampmann B. Impact of COVID-19 on Immunization Services for Maternal and Infant Vaccines: Results of a Survey Conducted by Imprint—The Immunising Pregnant Women and Infants Network. Vaccines. 2020; 8(3):556. https://doi.org/10.3390/vaccines8030556
Chicago/Turabian StyleSaso, Anja, Helen Skirrow, and Beate Kampmann. 2020. "Impact of COVID-19 on Immunization Services for Maternal and Infant Vaccines: Results of a Survey Conducted by Imprint—The Immunising Pregnant Women and Infants Network" Vaccines 8, no. 3: 556. https://doi.org/10.3390/vaccines8030556
APA StyleSaso, A., Skirrow, H., & Kampmann, B. (2020). Impact of COVID-19 on Immunization Services for Maternal and Infant Vaccines: Results of a Survey Conducted by Imprint—The Immunising Pregnant Women and Infants Network. Vaccines, 8(3), 556. https://doi.org/10.3390/vaccines8030556