Promoting Influenza Vaccination among Staff of Nursing Homes According to Behavioral Insights: Analyzing the Choice Architecture during a Nudge-Based Intervention

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. The Nudge Intervention
2.3. Analysis of Choice Architecture: The Qualitative Study
2.3.1. The Questionnaire
2.3.2. Qualitative Analysis on the Choice Architecture
2.4. Cross-Sectional Study
- Influenza is a serious illness (A1)
- Influenza vaccine is effective (A2)
- Healthcare workers must get vaccinated (A3)
- By getting vaccinated I protect people close to me from influenza (A4)
- It is better to get the flu than the vaccination (B1)
- Influenza vaccines have serious side effects (B2)
- Vaccine can cause influenza (B3)
- Opposed to vaccination (B4)
Statistical Analysis
3. Results
3.1. Qualitative Analysis of Choice Architecture
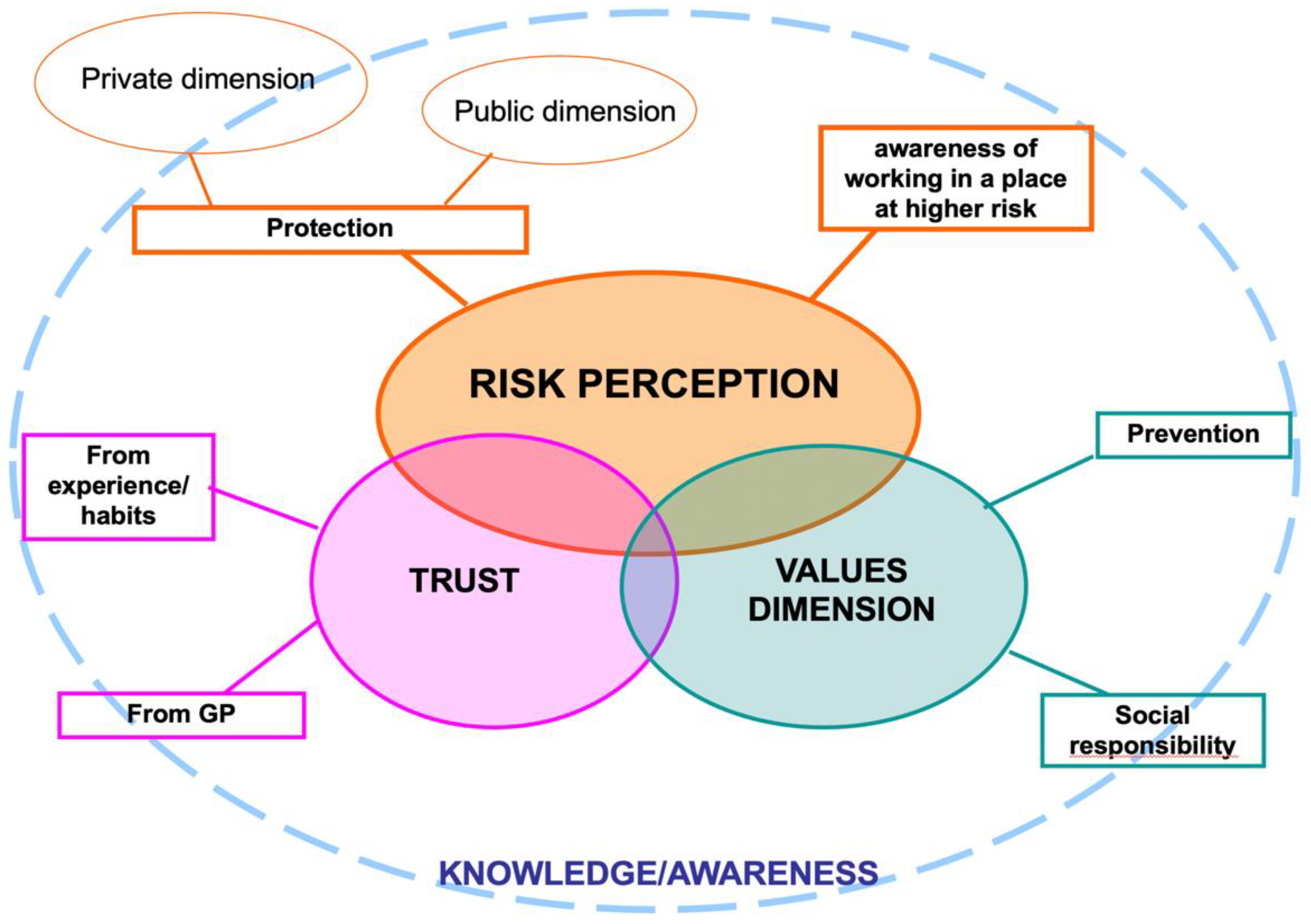
3.1.1. Reasons to Get Vaccinated
- A. Risk perception
“To avoid flu and to protect my family and NH residents, because they are fragile people” (respondent NH_5_3)
“In my opinion, vaccination is the (...) safest means of not transmitting it (influenza) to the NH residents and also to family members” (respondent NH_1-2_15)
“I have already had the vaccine to prevent getting sick” (respondent NH_1-2_11)
“Protect me and my family” (respondent NH_1-2_21)
“To avoid infecting NH residents” (respondent NH_5_6)
“I would like to get vaccinated to protect the health of fragile subjects with whom I am in daily contact” (respondent NH_8_25)
“To raise my immunity” (respondent NH_8_64)
“Too many times I find myself with low immune defenses and therefore avoid or reduce the chances of catching other viruses, also protecting my family” (respondent NH 8_42)
“Because I want to protect (...) especially all those who cannot be vaccinated” (respondent NH_1-2_34)
“Protection towards others and helping people without immune defenses who cannot be vaccinated to feel safe in the midst of many other people who have the possibility and the luck of being able to get vaccinated” (respondent NH_8_10)
“Since we do work at risk” (respondent NH_1-2_13)
“I work in a social health facility and there is a greater risk of getting the influenza” (respondent NH_8_18)
- B. Values Dimension
“I think prevention is important” (respondent NH_8_73)
“It is a favor that should not be wasted and a social duty” (respondent NH_5_3)
“Civic sense” (respondent NH_8_31)
- C. Trust
“In my opinion, vaccination is the most effective means of preventing influenza (...)” (respondent NH_1-2_15)
“I am in favor of vaccines. I don’t want to get sick” (respondent NH_6_3)
“Already done. Always done and I’m fine” (respondent NH_3_15)
“For many years I have been vaccinated to protect the health of assisted guests and my family members because until a few years ago I had a family member at risk” (respondent NH_6_4)
“As an asthmatic, the family doctor strongly advised me to get the vaccine” (respondent NH_8_50)
“On the advice of doctors” (respondent NH_6_7)
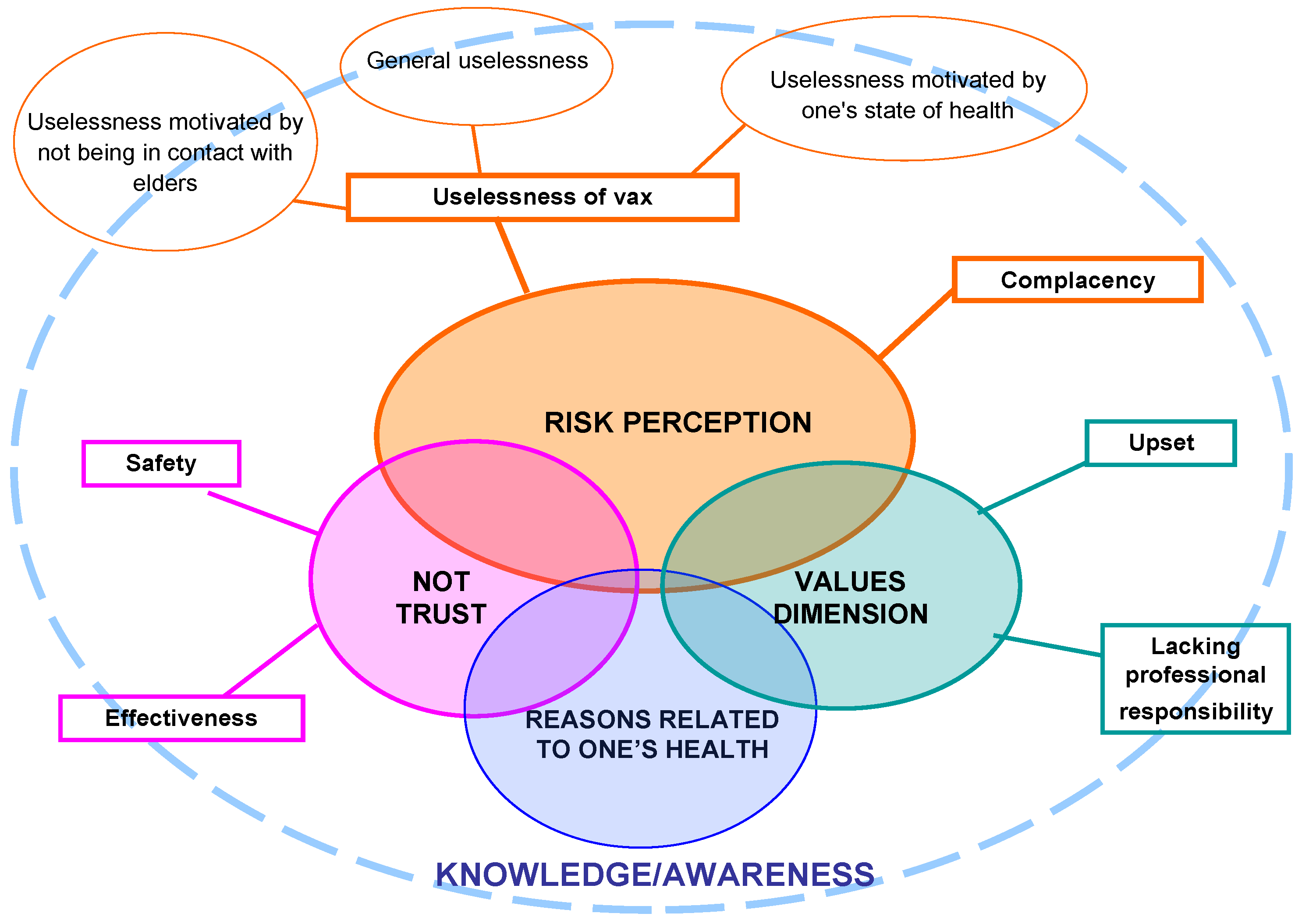
3.1.2. Reasons to Not Get Vaccinated
- A. Risk perception
“It’s hard for me to get the influenza” (respondent NH_7_5)
“I am not a person who gets sick easily, my immune defenses are very strong” (respondent NH_1-2_18)
“I believe it’s not necessary” (respondent NH_9_3)
“I think that getting vaccinated is not useful for me” (respondent NH_8_44)
“I don’t work closely with residents and I don’t get sick frequently with influenza” (respondent NH_4_8)
“I am not in direct contact with patients” (respondent NH_8_6)
“I don’t get vaccinated because I never did it” (respondent NH_6_10)
“I haven’t been vaccinated until now, so I prefer not to do it this year either” (respondent NH_6_8)
- B. Distrust
“I had physical weakness in previous times” (respondent NH_8_22)
“Because once I got vaccinated and I felt worse than when I didn’t” (respondent NH_5_19)
“Once I got vaccinated but I got the flu anyway” (respondent NH_1-2_2)
“I don’t think it’s effective” (respondent NH_1-2_3)
- C. Values Dimension
“Anti-vax” (respondent NH_9_1)
“I am against it” (respondent NH_8_60)
“I take advantage of herd immunity of nursing home’s residents” (respondent NH_1-2_39)
“I personally believe that influenza vaccine is very useful for elderly and immunocompromised but not necessary for others, even those in contact with these diseases” (respondent NH_8_55)
- D. Reasons related to one’s health
“I have an active autoimmune disease treated with immunosuppressive therapy” (respondent NH_8_1)
“Autoimmune subject. I do homeopathic vaccine” (respondent NH_7_13)
“I have only one kidney and I don’t want to overload my organism” (respondent NH_6_1)
“This year I have already got other vaccinations and I don’t feel like getting too many vaccines in the same period (I probably can’t even get them close together)” (respondent NH_8_55)
3.1.3. Interpretative Model
3.2. Data from the Cross-Sectional Study: The Nudge Group Versus the Comparison Group
4. Discussion
4.1. Choice Architecture
4.2. The Nudge Intervention in Promoting Influenza Vaccination Uptake
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Influenza (Seasonal). Available online: https://www.who.int/en/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 16 July 2020).
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Paget, J.; Spreeuwenberg, P.; Charu, V.; Taylor, R.J.; Iuliano, A.D.; Bresee, J.; Simonsen, L.; Viboud, C. Global Seasonal Influenza-associated Mortality Collaborator Network and GLaMOR Collaborating Teams. Global mortality associated with seasonal influenza epidemics: New burden estimates and predictors from the GLaMOR Project. J. Global Health 2019, 9, 20421. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.E.; Brown, C.S.; Nguyen-Van-Tam, J.S. Influenza in long-term care facilities. Influenza Other Respir. Viruses 2017, 11, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Vetrano, D.L.; Collamati, A.; Magnavita, N.; Sowa, A.; Topinkova, E.; Finne-Soveri, H.; van der Roest, H.G.; Tobiasz-Adamczyk, B.; Giovannini, S.; Ricciardi, W.; et al. Health determinants and survival in nursing home residents in Europe: Results from the SHELTER study. Maturitas 2018, 107, 19–25. [Google Scholar] [CrossRef]
- Poscia, A.; Collamati, A.; Carfì, A.; Topinkova, E.; Richter, T.; Denkinger, M.; Pastorino, R.; Landi, F.; Ricciardi, W.; Bernabei, R.; et al. Influenza and pneumococcal vaccination in older adults living in nursing home: A survival analysis on the shelter study. Eur. J. Public Health 2017, 27, 1016–1020. [Google Scholar] [CrossRef]
- Pop-Vicas, A.; Rahman, M.; Gozalo, P.L.; Gravenstein, S.; Mor, V. Estimating the Effect of Influenza Vaccination on Nursing Home Residents’ Morbidity and Mortality. J. Am. Geriatr. Soc. 2015, 63, 1798–1804. [Google Scholar] [CrossRef] [Green Version]
- Frentzel, E.; Jump, R.L.P.; Archbald-Pannone, L.; Nace, D.A.; Schweon, S.J.; Gaur, S.; Naqvi, F.; Pandya, N.; Mercer, W. Infection Advisory Subcommittee of AMDA, The Society for Post-Acute and Long-Term Care Medicine. Recommendations for Mandatory Influenza Vaccinations for Health Care Personnel from AMDA’s Infection Advisory Subcommittee. J. Am. Med. Dir. Assoc. 2020, 21, 25–28.e2. [Google Scholar] [CrossRef] [Green Version]
- Daugherty, J.D.; Blake, S.C.; Grosholz, J.M.; Omer, S.B.; Polivka-West, L.; Howard, D.H. Influenza vaccination rates and beliefs about vaccination among nursing home employees. Am. J. Infect. Control 2015, 43, 100–106. [Google Scholar] [CrossRef]
- Borgey, F.; Henry, L.; Lebeltel, J.; Lescure, P.; Le Coutour, X.; Vabret, A.; Verdon, R.; Thibon, P. Effectiveness of an intervention campaign on influenza vaccination of professionals in nursing homes: A cluster-randomized controlled trial. Vaccine 2019, 37, 1260–1265. [Google Scholar] [CrossRef]
- Looijmans-van den Akker, I.; van Delden, J.J.; Verheij, T.J.; van der Sande, M.A.; van Essen, G.A.; Riphagen-Dalhuisen, J.; Hulscher, M.E.; Hak, E. Effects of a multi-faceted program to increase influenza vaccine uptake among health care workers in nursing homes: A cluster randomised controlled trial. Vaccine 2010, 28, 5086–5092. [Google Scholar] [CrossRef] [Green Version]
- Lorini, C.; Collini, F.; Gasparini, F.; Paolini, D.; Grazzini, M.; Ierardi, F.; Galletti, G.; Zanobini, P.; Gemmi, F.; Bonaccorsi, G. Health Literacy, Vaccine Confidence and Influenza Vaccination Uptake among Nursing Home Staff: A Cross-Sectional Study Conducted in Tuscany. Vaccines 2020, 30, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mc Donald, N. The SAGEWorking Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Bechini, A.; Lorini, C.; Zanobini, P.; Tacconi, F.M.; Boccalini, S.; Grazzini, M.; Bonanni, P.; Bonaccorsi, G. Utility of Healthcare System-Based Interventions in Improving the Uptake of Influenza Vaccination in Healthcare Workers at Long-Term Care Facilities: A Systematic Review. Vaccines 2020, 8, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thaler, R.; Sunstein, C. La Spinta Gentile, 7th ed.; Giangiacomo Feltrinelli Editore: Milano, Italy, 2009; pp. 10–12, 91–109. [Google Scholar]
- Patel, M.S.; Volpp, K.G.; Asch, D.A. Nudge Units to Improve the Delivery of Health Care. N. Engl. J. Med. 2018, 378, 214–216. [Google Scholar] [CrossRef]
- World Health Organization. How to Implement Seasonal Influenza Vaccination of Health Workers: An Introduction Manual for National Immunization Programme Managers and Policy Makers: Pilot Version 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Patel, M.S. Nudges for influenza vaccination. Nat. Hum. Behav. 2018, 2, 720–721. [Google Scholar] [CrossRef]
- Nuffield Council on Bioethics. Public Health: Ethical Issues; Nuffield Council on Bioethics: London, UK, 2007. [Google Scholar]
- Hallsworth, M.; Chadborn, T.; Sallis, A.; Sanders, M.; Berry, D.; Greaves, F.; Clements, L.; Davies, S.C. Provision of social norm feedback to high prescribers of antibiotics in general practice: A pragmatic national randomised controlled trial. Lancet 2016, 387, 1743–1752. [Google Scholar] [CrossRef] [Green Version]
- Glaser, B.; Strauss, A. The Discovery of Grounded Theory: Strategies for Qualitative Research; Sociology Press: Mill Valley, CA, USA, 1967. [Google Scholar]
- Corbetta, P. La Ricerca Sociale: Metodologia e Tecniche—III. Le Tecniche Qualitative; Il Mulino: Bologna, Italy, 2005. [Google Scholar]
- Sala, E. L’intervista. In Il Mondo Della Ricerca Qualitativa; de Lillo, A., Ed.; UTET: Torino, Italy, 2010. [Google Scholar]
- Stein, C.H.; Mankowski, E.S. Asking, witnessing, interpreting, knowing: Conducting qualitative research in community psychology. Am. J. Commun. Psychol. 2004, 33, 21–35. [Google Scholar] [CrossRef]
- Connelly, J.; Clandinin, F.M. Narrative Inquiry. Experience and Story in Qualitative Research; Jossey Bass Publishers: San Francisco, CA, USA, 2000. [Google Scholar]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Kom, L.; Holtmann, C.; Bohm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [Green Version]
- Bonaccorsi, G.; Santomauro, F.; Porchia, B.R.; Niccolai, G.; Pellegrino, E.; Bonanni, P.; Lorini, C. Beliefs and Opinions of Health Care Workers and Students Regarding Influenza and Influenza Vaccination in Tuscany, Central Italy. Vaccines 2015, 3, 137–147. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Lorini, C.; Santomauro, F.; Guarducci, S.; Pellegrino, E.; Puggelli, F.; Balli, M.; Bonanni, P. Predictive factors associated with the acceptance of pandemic and seasonal influenza vaccination in health care workers and students in Tuscany, Central Italy. Hum. Vaccines Immunother. 2013, 9, 2603–2612. [Google Scholar] [CrossRef] [Green Version]
- Bonaccorsi, G.; Lorini, C.; Porchia, B.R.; Niccolai, G.; Martino, G.; Giannarelli, L.; Santomauro, F. Influenza vaccination: Coverage and risk perception among students of the health professions at Florence University, Italy. Ann. Ig. 2013, 25, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Paoli, S.; Lorini, C.; Puggelli, F.; Sala, A.; Grazzini, M.; Paolini, D.; Bonanni, P.; Bonaccorsi, G. Assessing Vaccine Hesitancy among Healthcare Workers: A Cross-Sectional Study at an Italian Paediatric Hospital and the Development of a Healthcare Worker’s Vaccination Compliance Index. Vaccines 2019, 29, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubov, A.; Phung, C. Nudges or mandates? The ethics of mandatory flu vaccination. Vaccines 2015, 33, 2530–2535. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Gretchen, B.C. Nudge to Health: Harnessing Decision Research to Promote Health Behavior. Soc. Personal. Psychol. Compass 2013, 7, 187–198. [Google Scholar] [CrossRef]
- World Health Organization. Tailoring Immunization Programmes (TIP). Ind Introductory Overview. Available online: https://www.who.int/immunization/programmes_systems/Global_TIP_overview_July2018.pdf?ua=1 (accessed on 16 July 2020).
- Brewer, N.; Chapman, G.; Rothman, A.; Leask, J.; Kempe, A. Increasing vaccination: Putting psychological science into action. Psychol. Sci. Public Interest 2017, 18, 149–207. [Google Scholar] [CrossRef] [Green Version]
- Jonas, H. Il Principio Responsabilità. Un’etica per la Civiltà Tecnologica; Einaudi: Torino, Italy, 1990. [Google Scholar]
- Censis. La Cultura Della Vaccinazione in Italia: Un’indagine sui Genitori; Censis: Rome, Italy, 2014. [Google Scholar]
- Broers, V.J.; De Breucker, C.; Van den Broucke, S.; Luminet, O. A systematic review and meta-analysis of the effectiveness of nudging to increase fruit and vegetable choice. Eur J. Public Health 2017, 27, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Whitehead, M.; Jones, R.; Howell, R.; Lilley, R.; Pykett, J. Nudging All Over the World. Assessing the Global Impact of Behavioural Sciences on Public Policy; ESRC Report; Economic and Social Research Council: Swindon/Edinburgh, UK, 2014. [Google Scholar]
- Oliver, A. Is nudge an effective public health strategy to tackle obesity? Yes. BMJ 2011, 342. [Google Scholar] [CrossRef]
- Maltz, A.; Sarid, A. Attractive Flu Shot: A Behavioral Approach to Increasing Influenza Vaccination Uptake Rates. Med. Decis. Making 2020, 40, 774–784. [Google Scholar] [CrossRef]
- Schmidtke, K.A.; Nightingale, P.G.; Reeves, K.; Gallier, S.; Vlaev, I.; Watson, S.I.; Lilford, R.J. Randomised controlled trial of a theory-based intervention to prompt front-line staff to take up the seasonal influenza vaccine. BMJ Qual. Saf. 2020, 29, 189–197. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, B.A.; Chapman, G.B.; Franssen, F.M.; Kok, G.; Ruiter, R.A. Changing the default to promote influenza vaccination among health care workers. Vaccine 2016, 34, 1389–1392. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Macro-Category | Description | Sub-Categories |
|---|---|---|
| Risk Perception | Appropriate knowledge of the disease and its risks, awareness of working in a place at higher risk of contagion, willingness to protect oneself and others | Protection: protection for oneself and his/her net of contacts |
| Awareness of working in a place at higher risk: awareness of being in a context that exposes more to the likelihood of contracting and transmitting influenza are mainly emphasized | ||
| Values Dimension | The set of ideals or norms of the individuals of a social group, which influence their action | Prevention: the will to prevent the negative effects of the influenza for individual and social benefit |
| Social Responsibility: the collective benefit stands out as a value that guides one’s intention to get vaccinated | ||
| Trust | An attitude resulting from a positive assessment of facts, circumstances, relationships, for which one trusts in the vaccine and more generally in the healthcare system and in the professionals, animated by a general feeling of safety | From experience/habits: the sense of safety and efficacy of the vaccine, mainly referred to the protection of one’s health |
| From General Practitioner (GP): safety and efficacy of the vaccine from GP or healthcare professionals |
| Macro-Category | Description | Sub-Categories |
|---|---|---|
| Risk Perception | Poor or distorted knowledge of personal or social risk related to flu assuming that there is no danger. This option is strengthened by a lack of interest in exploring the topic | Uselessness of vaccine: perception of unnecessariness about the opportunity of being vaccinated, with regard to one’s health |
| Complacency: attitude oriented towards passivity, not questioning one’s choice, lack of values towards others’ protection and social responsibility | ||
| Distrust | Attitude to negative evaluation of facts, circumstances, and relationships generating a feeling of distrust in others as well as in their own possibilities and generally producing a lack of self-confidence and peace of mind | Distrust in safety: belief that vaccines can be associated to serious diseases, collateral and unknown long-term effects, and belief that risks are greater than benefits |
| Distrust in effectiveness: belief that vaccination is an avoidable practice because it does not bring any benefits, even if it is not harmful | ||
| Values Dimension | Gaps in ideals or norms based on the awareness of the healthcare workers’ responsibilities, specifically on the norm of social protection (fragile and non-frail subjects), also achievable through personal protection. This can lead to opposition and criticism of the vaccine or partial perception of its individual and social usefulness. | Upset: very extreme position of refusal to get vaccinated |
| Lacking professional responsibility: refers to scarce or limited awareness of the responsibility of getting vaccinated due to the kind of profession | ||
| Reasons related to one’s health | Attitude towards vaccination as derived from aspects related to physical inability to be vaccinated | - |
| Categorical Variables | Whole Sample (n = 1998) | Nudge Group (n = 195) | Comparison Group (n = 1803) | p * | |
|---|---|---|---|---|---|
| % | % | % | |||
| Females | 86.9 | 87.2 | 86.9 | 0.879 | |
| Native speakers-Italian | 84.9 | 87.2 | 84.6 | 0.981 | |
| Educational level | Higher than bachelor’s degree | 2.6 | 2.6 | 2.6 | 0.088 |
| Bachelor’s degree | 18.7 | 17.4 | 18.9 | ||
| High school degree | 46.5 | 55.4 | 45.6 | ||
| Less than high school diploma | 31.2 | 23.1 | 33 | ||
| Qualification | Nurses | 12.8 | 11.8 | 12.9 | 0.251 |
| Physiotherapists | 4.3 | 4.6 | 4.2 | ||
| Health educators | 4 | 3.6 | 4 | ||
| Assistants/aides | 58.8 | 55.4 | 59.1 | ||
| Cleaning staff | 5.9 | 10.3 | 5.4 | ||
| Other nonclinical staff | 6.4 | 7.7 | 6.3 | ||
| Other clinical staff | 6.6 | 5.1 | 6.8 | ||
| Living with children of less than 9 years | 19.6 | 17.9 | 19.8 | 0.604 | |
| Living with elderly people | 20.1 | 15.4 | 20.6 | 0.22 | |
| Living with people with chronic diseases | 16.5 | 8.7 | 17.3 | 0.006 | |
| Vaccination uptake 2018–2019 | 22.3 | 23.6 | 22.1 | 0.35 | |
| Vaccination uptake 2019–2020 | 20.8 | 28 | 20 | 0.006 | |
| Intention to vaccinate in 2020–2021 (very likely) | 31.5 | 37.9 | 30.8 | 0.027 | |
| Numerical Variables | Mean ± SD; Median | Mean ± SD; Median | Mean ± SD; Median | p ° | |
| Age # | 44.4 ± 11.1; 46 | 44.6 ± 10.9; 47 | 44.3 ± 11.1; 46 | 0.791 | |
| VCI # | 1.61 ± 0.83; 1.3 | 1.67 ± 0.86; 1.3 | 1.60 ± 0.83; 1.33 | 0.358 | |
| Health status # | 8.5 ± 1.3; 9.0 | 8.5 ± 1.3; 9 | 8.5 ± 1.3; 9.0 | 0.515 | |
| Motivation for Vaccination Uptake in 2019–2020 | Nudge Group (n = 55) | Comparison Group (n = 360) | p (Fisher’s Exact Test) |
|---|---|---|---|
| I do not want to get sick | 76.4 | 79.7 | 0.339 |
| Concerning my job, it is important to protect people in contact with me | 85.5 | 84.7 | 1 |
| I am vaccinated every year | 58.2 | 66.9 | 0.223 |
| I was sick with influenza in the past | 30.9 | 42.5 | 0.108 |
| The vaccine administration was convenient | 50.9 | 48.1 | 0.772 |
| I have been advised to get vaccinated | 63.6 | 54.4 | 0.224 |
| My colleagues or relatives get the vaccine | 20 | 26.1 | 0.406 |
| I felt compelled to be vaccinated | 78.2 | 71.7 | 0.337 |
| Motivation for Vaccination NON-Uptake in 2019–2020 | Nudge Group (n = 140) | Comparison Group (n = 1443) | p (Fisher’s Exact test) |
| I am not in the target group | 34.3 | 41.3 | 0.125 |
| Fear of side effects | 17.9 | 24.8 | 0.078 |
| The vaccine does not work | 9.3 | 16.2 | 0.028 |
| I am concerned about getting influenza from the vaccine | 12.1 | 15.2 | 0.385 |
| I never get sick with influenza | 47.1 | 40.3 | 0.126 |
| The vaccine administration was not convenient | 3.6 | 5.3 | 0.547 |
| I did not have time to be vaccinated | 4.3 | 8.5 | 0.103 |
| I forgot to be vaccinated | 4.3 | 6.2 | 0.458 |
| Fear of needles | 5.7 | 6.3 | 1 |
| No one informed me about the vaccination campaign | 4.3 | 6.6 | 0.366 |
| I have never been vaccinated before | 45.7 | 38.1 | 0.084 |
| I did not think about it | 19.3 | 19.3 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorini, C.; Ierardi, F.; Gatteschi, C.; Galletti, G.; Collini, F.; Peracca, L.; Zanobini, P.; Gemmi, F.; Bonaccorsi, G. Promoting Influenza Vaccination among Staff of Nursing Homes According to Behavioral Insights: Analyzing the Choice Architecture during a Nudge-Based Intervention. Vaccines 2020, 8, 600. https://doi.org/10.3390/vaccines8040600
Lorini C, Ierardi F, Gatteschi C, Galletti G, Collini F, Peracca L, Zanobini P, Gemmi F, Bonaccorsi G. Promoting Influenza Vaccination among Staff of Nursing Homes According to Behavioral Insights: Analyzing the Choice Architecture during a Nudge-Based Intervention. Vaccines. 2020; 8(4):600. https://doi.org/10.3390/vaccines8040600
Chicago/Turabian StyleLorini, Chiara, Francesca Ierardi, Claudia Gatteschi, Giacomo Galletti, Francesca Collini, Laura Peracca, Patrizio Zanobini, Fabrizio Gemmi, and Guglielmo Bonaccorsi. 2020. "Promoting Influenza Vaccination among Staff of Nursing Homes According to Behavioral Insights: Analyzing the Choice Architecture during a Nudge-Based Intervention" Vaccines 8, no. 4: 600. https://doi.org/10.3390/vaccines8040600
APA StyleLorini, C., Ierardi, F., Gatteschi, C., Galletti, G., Collini, F., Peracca, L., Zanobini, P., Gemmi, F., & Bonaccorsi, G. (2020). Promoting Influenza Vaccination among Staff of Nursing Homes According to Behavioral Insights: Analyzing the Choice Architecture during a Nudge-Based Intervention. Vaccines, 8(4), 600. https://doi.org/10.3390/vaccines8040600