
Humoral Response after Vaccination with Half-Dose of BNT162b2 in Subjects under 55 Years of Age

 , , , ,
, , , ,
Abstract
:1. Introduction
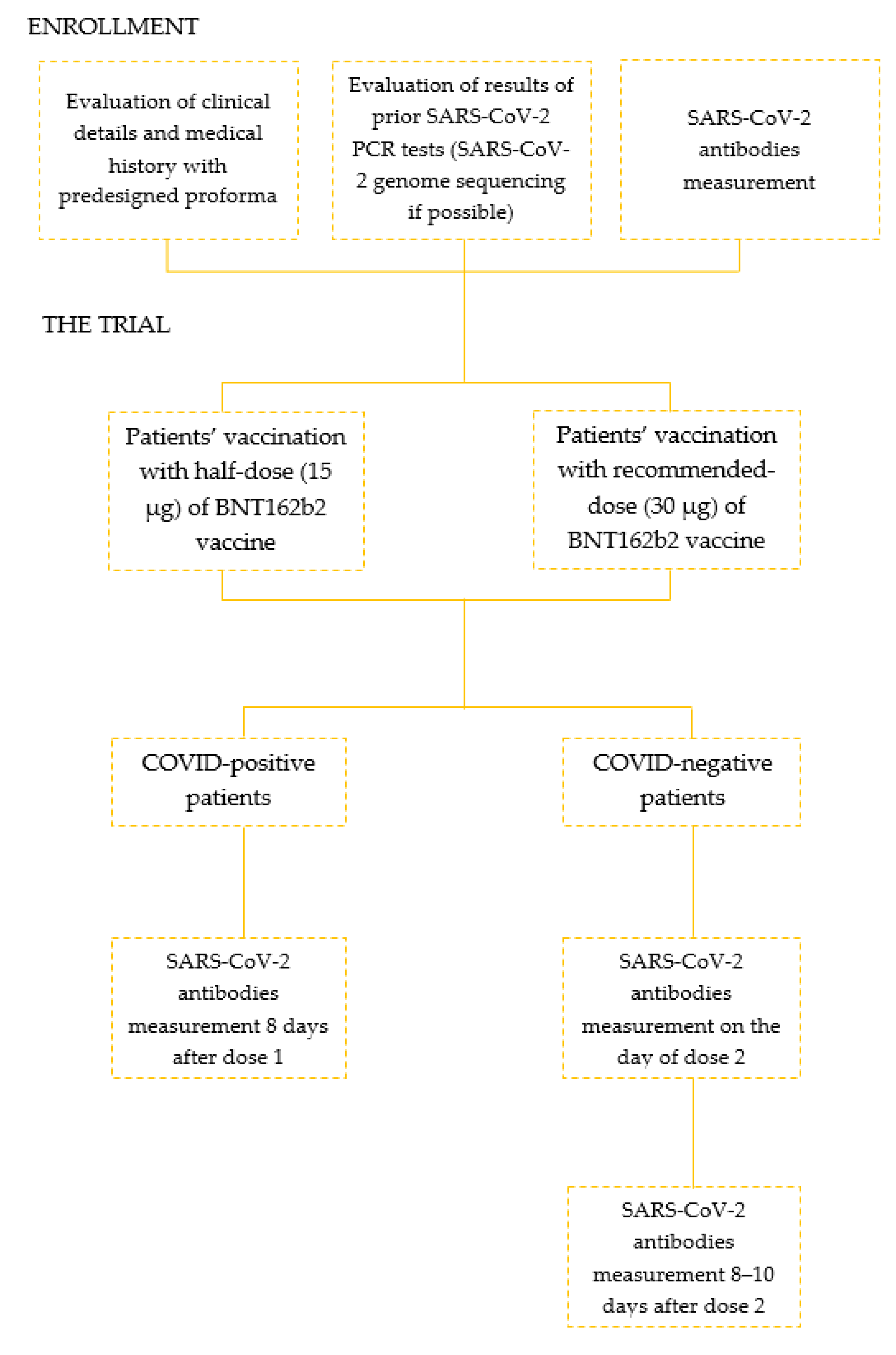
2. Materials and Methods
2.1. Ethical Policy
2.2. Vaccination
2.3. Participants
2.4. SARS-CoV-2 Antibodies Measurement
2.5. Assay Characteristics
2.6. Sequencing
2.7. Statistical Analysis
3. Results
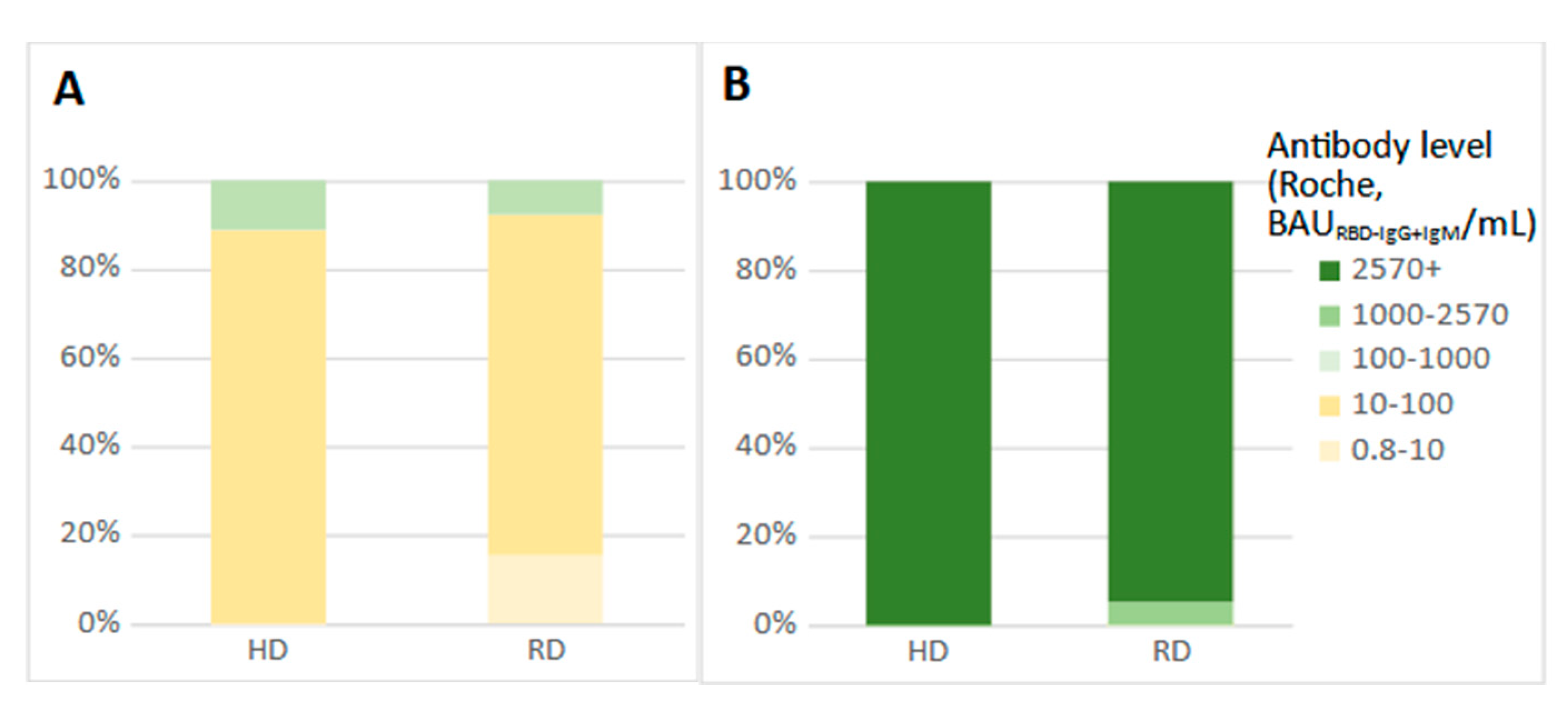
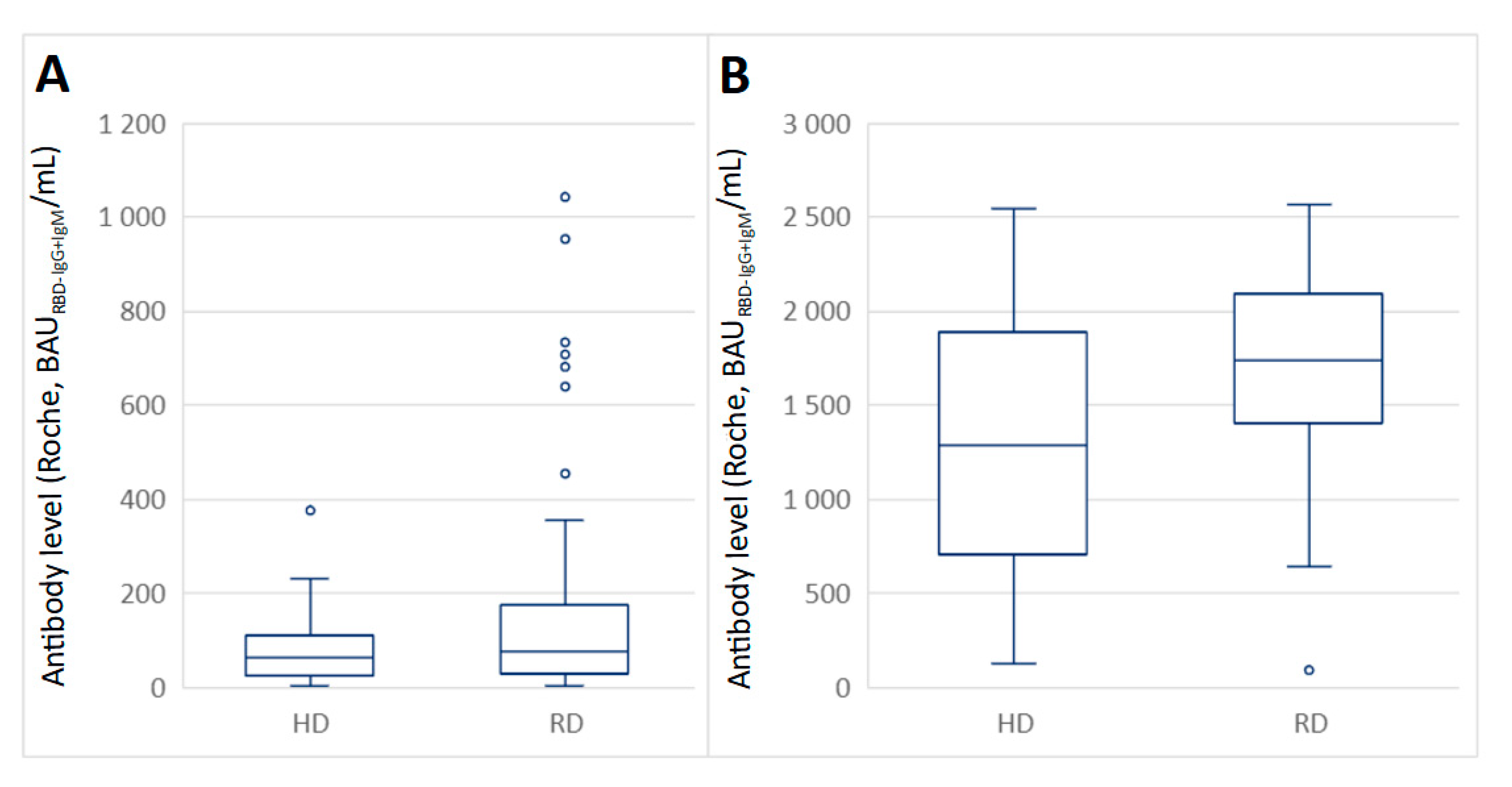
3.1. The Comparison of Mean Antibody Level in the Serum of COVID-19 Positive Subjects
3.2. The Mean Antibody Level in the Serum of COVID-19 Negative Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Safety and Immunogenicity of SARS-CoV-2 mRNA-1273 Vaccine in Older Adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Khan, S.; Imran, I.; Al Mughairbi, F.; Sheikh, F.; Hussain, J.; Khan, A.; Al-Harrasi, A. Vaccine Development against COVID-19: Study from Pre-Clinical Phases to Clinical Trials and Global Use. Vaccines 2021, 9, 836. Available online: https://www.mdpi.com/2076-393X/9/8/836 (accessed on 19 August 2021). [CrossRef]
- WHO. Vaccine Inequity Undermining Global Economic Recovery. 2021. Available online: https://www.who.int/news/item/22-07-2021-vaccine-inequity-undermining-global-economic-recovery (accessed on 19 August 2021).
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; MacDonald, B.; Beltekian, D.; Dattani, S.; et al. Coronavirus Pandemic (COVID-19). Our World in Data. 2020. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 3 November 2021).
- Maxmen, A. The Fight to Manufacture COVID Vaccines in Lower-Income Countries. Nature 2021, 597, 455–457. Available online: https://www.nature.com/articles/d41586-021-02383-z (accessed on 19 August 2021). [CrossRef] [PubMed]
- Mullard, A. How COVID vaccines are being divvied up around the world. Nature 2020. [Google Scholar] [CrossRef] [PubMed]
- WHO. Interim Statement on Dose-Sparing Strategies for COVID-19 Vaccines (Fractionated Vaccine Doses). 2021. Available online: https://www.who.int/news/item/10-08-2021-interim-statement-on-dose-sparing-strategies-for-covid-19-vaccines-(fractionated-vaccine-doses) (accessed on 15 October 2021).
- Casey, R.M.; Harris, J.B.; Ahuka-Mundeke, S.; Dixon, M.G.; Kizito, G.M.; Nsele, P.M.; Umutesi, G.; Laven, J.; Kosoy, O.; Paluku, G.; et al. Immunogenicity of Fractional-Dose Vaccine during a Yellow Fever Outbreak—Final Report. N. Engl. J. Med. 2019, 381, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Ebinger, J.E.; Fert-Bober, J.; Printsev, I.; Wu, M.; Sun, N.; Prostko, J.C.; Frias, E.C.; Stewart, J.L.; Van Eyk, J.E.; Braun, J.G.; et al. Antibody responses to the BNT162b2 mRNA vaccine in individuals previously infected with SARS-CoV-2. Nat. Med. 2021, 27, 981–984. [Google Scholar] [CrossRef]
- Lukaszuk, K.; Kiewisz, J.; Rozanska, K.; Dabrowska, M.; Podolak, A.; Jakiel, G.; Woclawek-Potocka, I.; Lukaszuk, A.; Rabalski, L. Usefulness of IVD Kits for the Assessment of SARS-CoV-2 Antibodies to Evaluate the Humoral Response to Vaccination. Vaccines 2021, 9, 840. [Google Scholar] [CrossRef]
- Laboratory Testing of 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases: Interim Guidance, 17 January 2020. Available online: https://www.who.int/publications/i/item/laboratory-testing-of-2019-novel-coronavirus-(-2019-ncov)-in-suspected-human-cases-interim-guidance-17-january-2020 (accessed on 19 August 2021).
- CDC Labs. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/lab-biosafety-guidelines.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Flab-biosafety-guidelines.html (accessed on 13 July 2021).
- Oliveira, B.A.; de Oliveira, L.C.; Sabino, E.C.; Okay, T.S. SARS-CoV-2 and the COVID-19 disease: A mini review on diagnostic methods. Rev. Inst. Med. Trop. Sao Paulo. 2020, 62, 1–8. [Google Scholar] [CrossRef]
- Younes, N.; Al-Sadeq, D.W.; Al-Jighefee, H.; Younes, S.; Al-Jamal, O.; Daas, H.I.; Yassine, H.M.; Nasrallah, G.K. Challenges in Laboratory Diagnosis of the Novel Coronavirus SARS-CoV-2. Viruses 2020, 12, 582. [Google Scholar] [CrossRef]
- Chau, C.H.; Strope, J.; Figg, W.D. COVID-19 Clinical Diagnostics and Testing Technology. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 857–868. [Google Scholar] [CrossRef] [PubMed]
- Oladimeji, P.; Pickford, J. Letter of concern re: “Comparison of seven commercial RT-PCR diagnostic kits for COVID-19” van Kasteren et al., Journal of Clinical Virology. J. Clin. Virol. 2020, 130, 104536. Available online: https://europepmc.org/articles/PMC7336925 (accessed on 19 August 2021). [CrossRef] [PubMed]
- Carter, N.; Clausen, M.; Halpin, R.A.; Blackmore, C.; Cai, K.; Delpuech, O.; Kohlmann, A.; Magnusson, O.; March, R.; O’Neill, D.; et al. A novel automated SARS-CoV-2 saliva PCR test protects a global asymptomatic workforce. Sci. Rep. 2021, 11, 1–6. [Google Scholar] [CrossRef]
- van Kasteren, P.B.; van der Veer, B.; van den Brink, S.; Wijsman, L.; de Jonge, J.; van den Brandt, A. Comparison of seven commercial RT-PCR diagnostic kits for COVID-19. J. Clin. Virol. 2020, 128, 104412. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, J. Study Suggests Lasting Immunity after COVID-19, with a Big Boost from Vaccination. JAMA 2021, 326, 376–377. [Google Scholar] [CrossRef] [PubMed]
- Perkmann, T.; Perkmann-Nagele, N.; Koller, T.; Mucher, P.; Radakovics, A.; Wolzt, M.; Wagner, O.F.; Binder, C.J.; Haslacher, H. Serum antibody response to BNT162b2 after natural SARS-CoV-2 infection. Eur. J. Clin. Investig. 2021, 51, e13632. [Google Scholar] [CrossRef] [PubMed]
- Dopico, X.C.; Ols, S.; Loré, K.; Hedestam, G.B.K. Immunity to SARS-CoV-2 induced by infection or vaccination. J. Intern. Med. 2021. Available online: https://onlinelibrary.wiley.com/doi/10.1111/joim.13372 (accessed on 19 August 2021). [CrossRef]
- Study to Describe the Safety, Tolerability, Immunogenicity, and Efficacy of RNA Vaccine Candidates Against COVID-19 in Healthy Individuals. Available online: https://clinicaltrials.gov/ct2/show/NCT04368728 (accessed on 19 August 2021).
- Pfizer-BioNTech COVID-19 BNT162b2 Vaccine Effectiveness Study-Kaiser Permanente Southern California. Available online: https://clinicaltrials.gov/ct2/show/NCT04848584?term=pfizer&draw=2&rank=1 (accessed on 19 August 2021).
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA Vaccine against SARS-CoV-2—Preliminary Report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef] [PubMed]
- Mateus, J.; Dan, J.M.; Zhang, Z.; Moderbacher, C.R.; Lammers, M.; Goodwin, B.; Sette, A.; Crotty, S.; Weiskopf, D. Low dose mRNA-1273 COVID-19 vaccine generates durable T cell memory and antibodies enhanced by pre-existing crossreactive T cell memory. medRxiv 2021, preprint. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2020, 397, 99–111. [Google Scholar] [CrossRef]
- Dolgin, E. Quarter-dose of Moderna COVID vaccine still rouses a big immune response. Nat. Cell Biol. 2021. Available online: http://www.nature.com/articles/d41586-021-01893-0 (accessed on 15 October 2021). [CrossRef]
- Więcek, W.; Ahuja, A.; Kremer, M.; Gomes, A.S.; Snyder, C.; Tabarrok, A.; Tan, B.J. Could Vaccine Dose Stretching Reduce COVID-19 Deaths? 2021. Available online: https://www.ssrn.com/abstract=3864485 (accessed on 15 October 2021).
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- COVID-19: Safety and Immunogenicity of a Reduced Dose of the BioNTech/Pfizer BNT162b2 Vaccine (REDU-VAC). Available online: https://clinicaltrials.gov/ct2/show/NCT04852861 (accessed on 19 August 2021).
- Dispinseri, S.; Secchi, M.; Pirillo, M.F.; Tolazzi, M.; Borghi, M.; Brigatti, C.; De Angelis, M.L.; Baratella, M.; Bazzigaluppi, E.; Venturi, G.; et al. Neutralizing antibody responses to SARS-CoV-2 in symptomatic COVID-19 is persistent and critical for survival. Nat. Commun. 2021, 12, 2670. [Google Scholar] [CrossRef]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.; Fong, Y.; Benkeser, D.C.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune Correlates Analysis of the mRNA-1273 COVID-19 Vaccine Efficacy Trial. medRxiv 2021. Available online: https://www.medrxiv.org/content/early/2021/08/15/2021.08.09.21261290 (accessed on 19 August 2021).
- Garcia-beltran, W.F.; Lam, E.C.; Denis, K.S.; Nitido, A.D.; Zeidy, H. Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity. Cell 2021, 184, 2372–2383. [Google Scholar] [CrossRef]
- Hacisuleyman, E.; Hale, C.; Saito, Y.; Blachere, N.E.; Bergh, M.; Conlon, E.G.; Schaefer-Babajew, D.J.; DaSilva, J.; Muecksch, F.; Gaebler, C.; et al. Vaccine Breakthrough Infections with SARS-CoV-2 Variants. N. Engl. J. Med. 2021, 384, 2212–2218. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Number of Participants | Analyzed GroupMale/Female | Mean Age | Mean BMI |
|---|---|---|---|---|
| RD group (n = 188) | ||||
| Positive | 36 | 9/27 | 38.9 (10.9) | 24.8 (4.7) |
| Negative | 152 | 27/125 | 38.7 (10.5) | 24.3 (5.2) |
| HD group (n = 42) | ||||
| Positive | 9 | 3/6 | 35.1 (9.0) | 25.0 (4.8) |
| Negative | 33 | 19/14 | 39.3 (8.8) | 23.8 (4.6) |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Age between 18 and 55 years old | Diabetes |
| Willingness to participate in the study | Hypertension |
| Heart-disease | |
| Chronic pulmonary disease | |
| Severe allergies | |
| Obesity (BMI > 30) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lukaszuk, K.; Podolak, A.; Jakiel, G.; Kiewisz, J.; Woclawek-Potocka, I.; Lukaszuk, A.; Rabalski, L. Humoral Response after Vaccination with Half-Dose of BNT162b2 in Subjects under 55 Years of Age. Vaccines 2021, 9, 1277. https://doi.org/10.3390/vaccines9111277
Lukaszuk K, Podolak A, Jakiel G, Kiewisz J, Woclawek-Potocka I, Lukaszuk A, Rabalski L. Humoral Response after Vaccination with Half-Dose of BNT162b2 in Subjects under 55 Years of Age. Vaccines. 2021; 9(11):1277. https://doi.org/10.3390/vaccines9111277
Chicago/Turabian StyleLukaszuk, Krzysztof, Amira Podolak, Grzegorz Jakiel, Jolanta Kiewisz, Izabela Woclawek-Potocka, Aron Lukaszuk, and Lukasz Rabalski. 2021. "Humoral Response after Vaccination with Half-Dose of BNT162b2 in Subjects under 55 Years of Age" Vaccines 9, no. 11: 1277. https://doi.org/10.3390/vaccines9111277
APA StyleLukaszuk, K., Podolak, A., Jakiel, G., Kiewisz, J., Woclawek-Potocka, I., Lukaszuk, A., & Rabalski, L. (2021). Humoral Response after Vaccination with Half-Dose of BNT162b2 in Subjects under 55 Years of Age. Vaccines, 9(11), 1277. https://doi.org/10.3390/vaccines9111277