
Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland




Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey
- The percentage of Poles fully vaccinated at the time of the study who would be willing to receive a booster dose of the COVID-19 vaccine (third dose in the case of mRNA vaccines and AZD1222, and second dose in the case of Ad26.COV2.S);
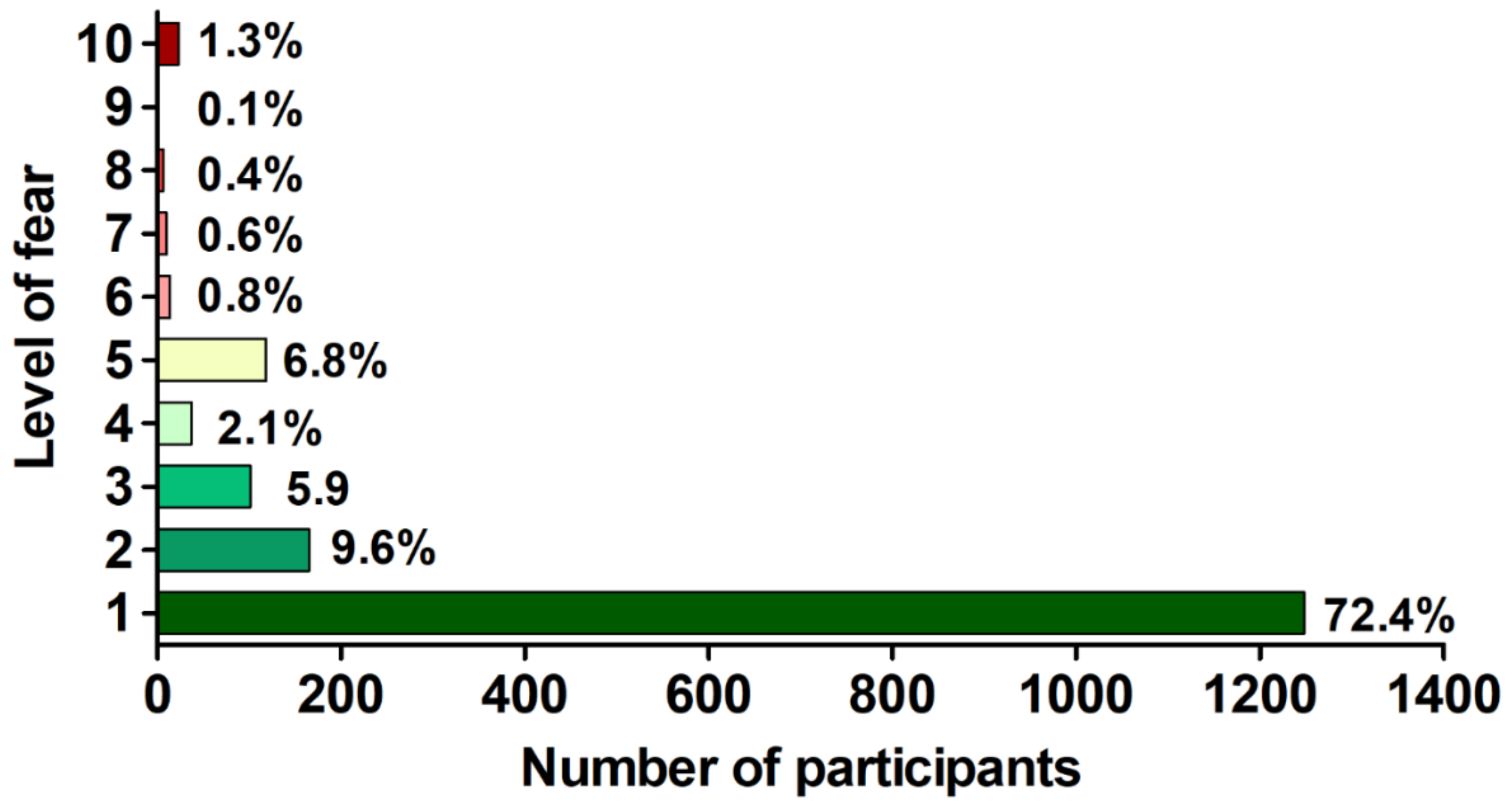
- The level of fear of booster COVID-19 vaccine dose (measured with a 10-point Likert-type scale, where 1—no fear, 10—very high level of fear) in individuals willing to receive it;
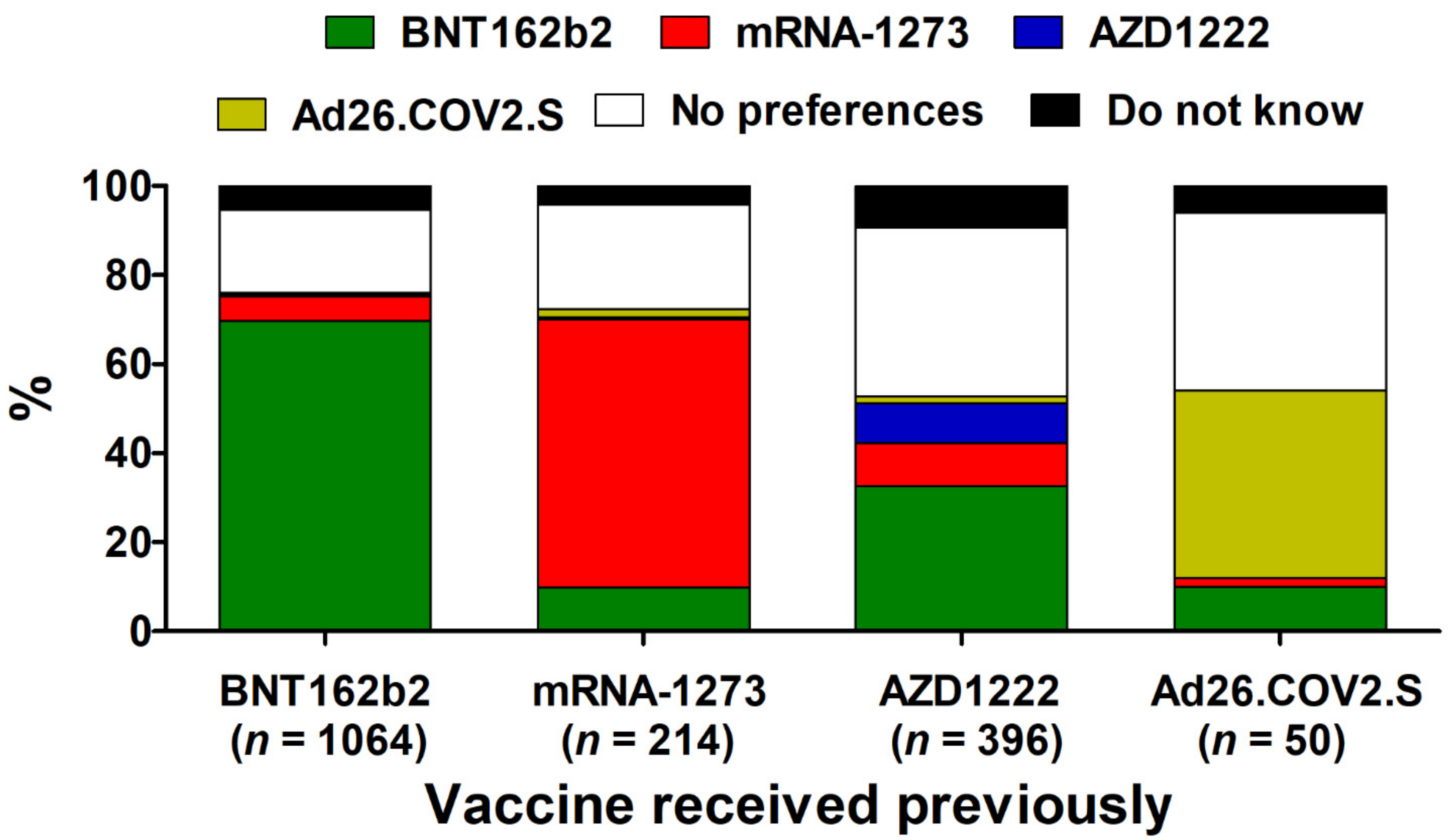
- The preferences toward specific COVID-19 vaccines (BNT162b2, mRNA-1273, AZD1222, or Ad26.COV2.S) to be administered as a booster dose and whether this corresponds to the COVID-19 vaccine given in the past;
- Primary reasons behind the unwillingness to receive a booster COVID-19 vaccine;
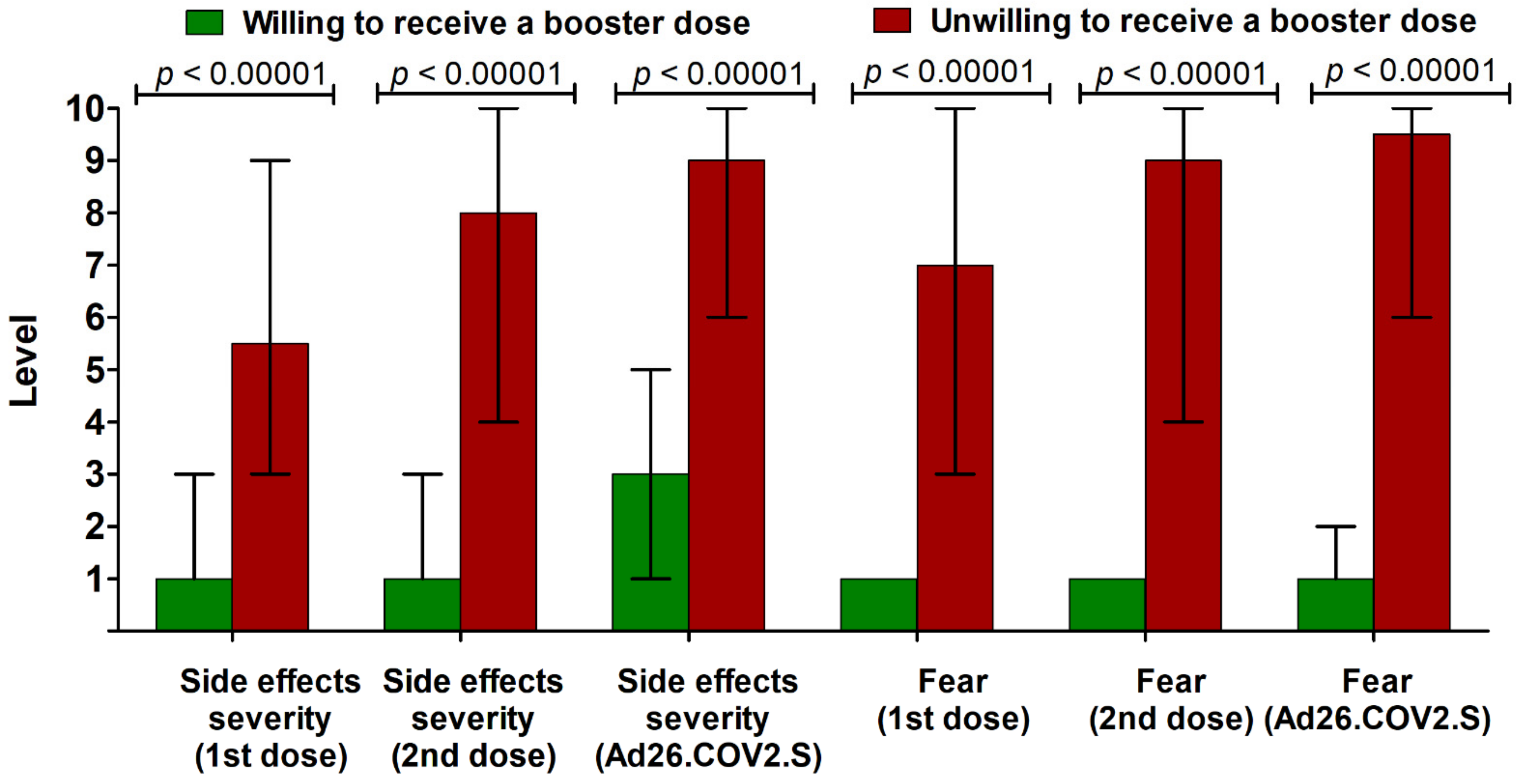
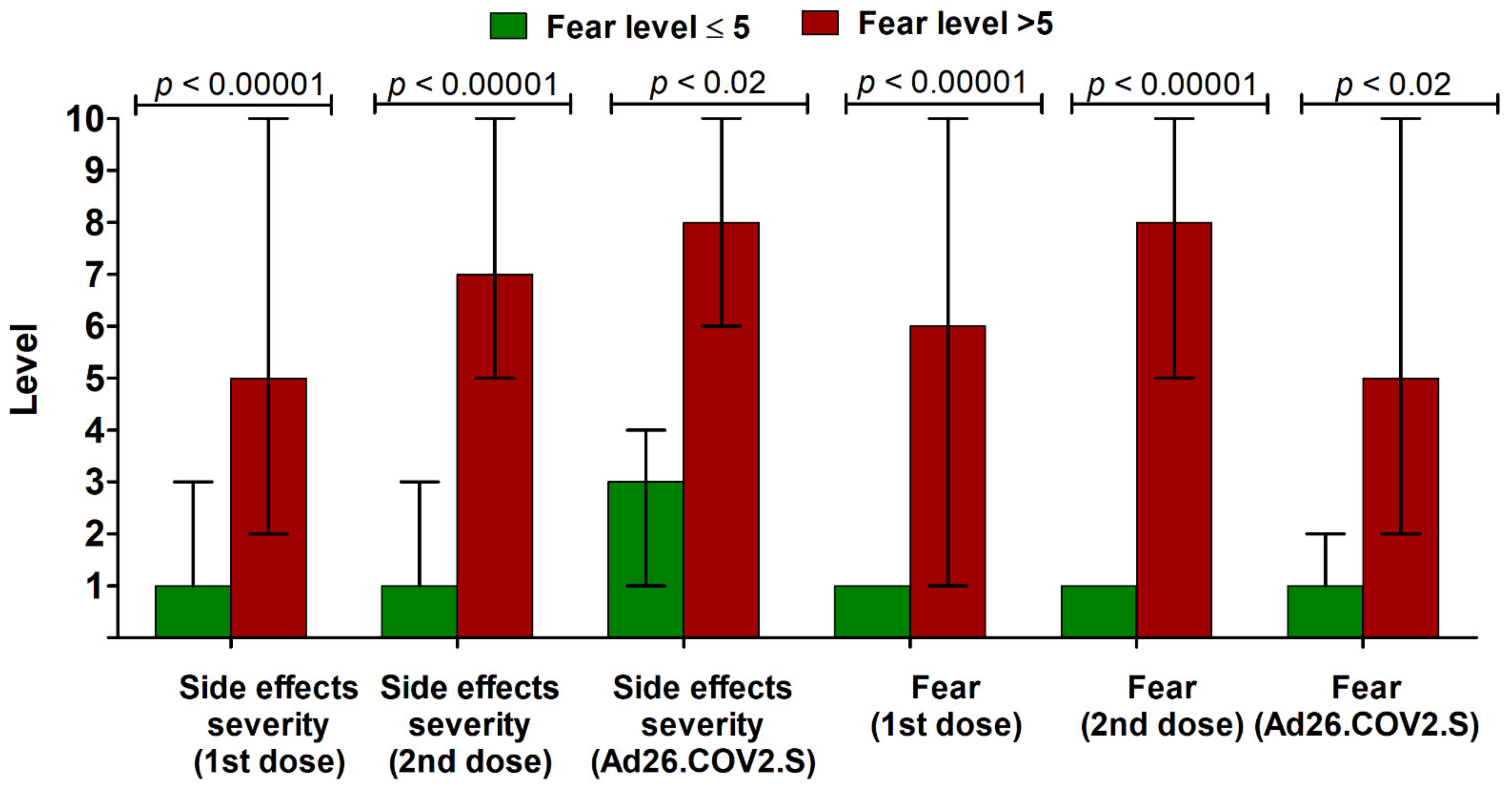
- The factors that are associated with willingness/unwillingness to receive a booster dose of the COVID-19 vaccine, including demographical characteristics (age, gender, body mass index, chronic diseases, presence of immunosuppression, SARS-CoV-2 infection status), as well as past experience with the COVID-19 vaccine evaluated as the severity level of side effects following each past dose and fear level accompanying these side effects (both measured with a 10-point Likert-type scale, where 1—no side effects or negligible side effects/no fear, 10—highly severe side effects/very high level of fear), and attitude toward influenza vaccination.
2.2. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Willingness to Receive a Booster COVID-19 Vaccine Dose
3.3. Fear of a Booster COVID-19 Vaccine Dose
3.4. Preferences of Type of Booster COVID-19 Vaccine Dose
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nowakowska, J.; Sobocińska, J.; Lewicki, M.; Lemańska, Ż.; Rzymski, P. When science goes viral: The research response during three months of the COVID-19 outbreak. Biomed. Pharmacother. 2020, 129, 110451. [Google Scholar] [CrossRef] [PubMed]
- Diéguez-Campa, C.E.; Pérez-Neri, I.; Reyes-Terán, G.; Flores-Apodaca, I.A.; Castillo-Ledón-Pretelini, J.; Mercado-Bautista, O.; Álvarez-Santana, R.; Zenteno, M.A.; Bowles, B.; Lee, Á. The 2020 research pandemic: A bibliometric analysis of publications on COVID-19 and their scientific impact during the first months. Arch. Cardiol. Mex. 2020. [Google Scholar] [CrossRef] [PubMed]
- Le, T.T.; Cramer, J.P.; Chen, R.; Mayhew, S. Evolution of the COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 667–668. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2020, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Rzymski, P.; Pazgan-Simon, M.; Simon, K.; Łapiński, T.; Zarębska-Michaluk, D.; Szczepańska, B.; Chojnicki, M.; Mozer-Lisewska, I.; Flisiak, R. Clinical Characteristics of Hospitalized COVID-19 Patients Who Received at Least One Dose of COVID-19 Vaccine. Vaccines 2021, 9, 781. [Google Scholar] [CrossRef]
- Shrotri, M.; Navaratnam, A.M.D.; Nguyen, V.; Byrne, T.; Geismar, C.; Fragaszy, E.; Beale, S.; Fong, W.L.E.; Patel, P.; Kovar, J.; et al. Spike-antibody waning after second dose of BNT162b2 or ChAdOx1. Lancet 2021, 398, 385–387. [Google Scholar] [CrossRef]
- Yamayoshi, S.; Yasuhara, A.; Ito, M.; Akasaka, O.; Nakamura, M.; Nakachi, I.; Koga, M.; Mitamura, K.; Yagi, K.; Maeda, K.; et al. Antibody titers against SARS-CoV-2 decline, but do not disappear for several months. EClinicalMedicine 2021, 32, 100734. [Google Scholar] [CrossRef]
- Mlcochova, P.; Kemp, S.; Dhar, M.S.; Papa, G.; Meng, B.; Ferreira, I.A.T.M.; Datir, R.; Collier, D.A.; Albecka, A.; Singh, S.; et al. SARS-CoV-2 B.1.617.2 Delta variant replication and immune evasion. Nature 2021. [Google Scholar] [CrossRef] [PubMed]
- Teyssou, E.; Delagrèverie, H.; Visseaux, B.; Lambert-Niclot, S.; Brichler, S.; Ferre, V.; Marot, S.; Jary, A.; Todesco, E.; Schnuriger, A.; et al. The Delta SARS-CoV-2 variant has a higher viral load than the Beta and the historical variants in nasopharyngeal samples from newly diagnosed COVID-19 patients. J. Infect. 2021, 83, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Six Month Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. medRxiv 2021. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.; Hasan, M.R.; Chemaitelly, H.; Yassine, H.M.; Benslimane, F.M.; Khatib, H.A.A.; AlMukdad, S.; Coyle, P.; Ayoub, H.H.; Kanaani, Z.A.; et al. BNT162b2 and mRNA-1273 COVID-19 vaccine effectiveness against the Delta (B.1.617.2) variant in Qatar. medRxiv 2021. [Google Scholar] [CrossRef]
- Chia, P.Y.; Xiang Ong, S.W.; Chiew, C.J.; Ang, L.W.; Chavatte, J.-M.; Mak, T.-M.; Cui, L.; Kalimuddin, S.; Chia, W.N.; Tan, C.W.; et al. Virological and serological kinetics of SARS-CoV-2 Delta variant vaccine-breakthrough infections: A multi-center cohort study. medRxiv 2021. [Google Scholar] [CrossRef]
- Pouwels, K.B.; Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Vihta, K.-D.; House, T.; Hay, J.; Bell, J.I.; Newton, J.N.; et al. Impact of Delta on viral burden and vaccine effectiveness against new SARS-CoV-2 infections in the UK. medRxiv 2021. [Google Scholar] [CrossRef]
- Riemersma, K.K.; Grogan, B.E.; Kita-Yarbro, A.; Halfmann, P.J.; Segaloff, H.E.; Kocharian, A.; Florek, K.R.; Westergaard, R.; Bateman, A.; Jeppson, G.E.; et al. Shedding of Infectious SARS-CoV-2 Despite Vaccination. medRxiv 2021. [Google Scholar] [CrossRef]
- Liu, Y.; Rocklöv, J. The reproductive number of the Delta variant of SARS-CoV-2 is far higher compared to the ancestral SARS-CoV-2 virus. J. Travel Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Burki, T.K. Lifting of COVID-19 restrictions in the UK and the Delta variant. Lancet Respir. Med. 2021, 9, e85. [Google Scholar] [CrossRef]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwöbel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health-Eur. 2021, 9, 100178. [Google Scholar] [CrossRef]
- Schmidt, T.; Klemis, V.; Schub, D.; Schneitler, S.; Reichert, M.C.; Wilkens, H.; Sester, U.; Sester, M.; Mihm, J. Cellular immunity predominates over humoral immunity after homologous and heterologous mRNA and vector-based COVID-19 vaccine regimens in solid organ transplant recipients. Am. J. Transplant. 2021. [Google Scholar] [CrossRef] [PubMed]
- Thuluvath, P.J.; Robarts, P.; Chauhan, M. Analysis of antibody responses after COVID-19 vaccination in liver transplant recipients and those with chronic liver diseases. J. Hepatol. 2021, in press. [Google Scholar] [CrossRef]
- Hall, V.G.; Ferreira, V.H.; Ku, T.; Ierullo, M.; Majchrzak-Kita, B.; Chaparro, C.; Selzner, N.; Schiff, J.; McDonald, M.; Tomlinson, G.; et al. Randomized Trial of a Third Dose of mRNA-1273 Vaccine in Transplant Recipients. N. Engl. J. Med. 2021, 385, 1244–1246. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA COVID-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef] [PubMed]
- Bates, T.A.; Leier, H.C.; Lyski, Z.L.; Goodman, J.R.; Curlin, M.E.; Messer, W.B.; Tafesse, F.G. Age-Dependent Neutralization of SARS-CoV-2 and P.1 Variant by Vaccine Immune Serum Samples. JAMA 2021, 326, 868–869. [Google Scholar] [CrossRef] [PubMed]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent immune response to the Biontech/Pfizer BNT162b2 COVID-19 vaccination. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Collier, D.A.; De Marco, A.; Ferreira, I.; Meng, B.; Datir, R.; Walls, A.C.; Kemp, S.S.; Bassi, J.; Pinto, D.; Fregni, C.S.; et al. Sensitivity of SARS-CoV-2 B.1.1.7 to mRNA vaccine-elicited antibodies. Nature 2021, 593, 136–141. [Google Scholar] [CrossRef]
- European Medicine Agency. ECDC and EMA Highlight Considerations for Additional and Booster Doses of COVID-19 Vaccines. Available online: https://www.ema.europa.eu/en/news/ecdc-ema-highlight-considerations-additional-booster-doses-COVID-19-vaccines (accessed on 13 September 2021).
- Krause, P.R.; Fleming, T.R.; Peto, R.; Longini, I.M.; Figueroa, J.P.; Sterne, J.A.C.; Cravioto, A.; Rees, H.; Higgins, J.P.T.; Boutron, I.; et al. Considerations in boosting COVID-19 vaccine immune responses. Lancet 2021, 398, 1377–1380. [Google Scholar] [CrossRef]
- Chagla, Z.; Pai, M. COVID-19 boosters in rich nations will delay vaccines for all. Nat. Med. 2021, 27, 1659–1660. [Google Scholar] [CrossRef]
- Geldsetzer, P. Use of Rapid Online Surveys to Assess People’s Perceptions During Infectious Disease Outbreaks: A Cross-sectional Survey on COVID-19. J. Med. Internet Res. 2020, 22, e18790. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Zeyland, J.; Poniedziałek, B.; Małecka, I.; Wysocki, J. The Perception and Attitudes toward COVID-19 Vaccines: A Cross-Sectional Study in Poland. Vaccines 2021, 9, 382. [Google Scholar] [CrossRef]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.; Failla, G.; Ricciardi, W. Attitudes, acceptance and hesitancy among the general population worldwide to receive the COVID-19 vaccines and their contributing factors: A systematic review. EClinicalMedicine 2021, 40, 101113. [Google Scholar] [CrossRef] [PubMed]
- Alqudeimat, Y.; Alenezi, D.; AlHajri, B.; Alfouzan, H.; Almokhaizeem, Z.; Altamimi, S.; Almansouri, W.; Alzalzalah, S.; Ziyab, A.H. Acceptance of a COVID-19 Vaccine and Its Related Determinants among the General Adult Population in Kuwait. Med. Princ. Pract. Int. J. Kuwait Univ. Health Sci. Cent. 2021, 30, 262–271. [Google Scholar] [CrossRef]
- Grochowska, M.; Ratajczak, A.; Zdunek, G.; Adamiec, A.; Waszkiewicz, P.; Feleszko, W. A Comparison of the Level of Acceptance and Hesitancy towards the Influenza Vaccine and the Forthcoming COVID-19 Vaccine in the Medical Community. Vaccines 2021, 9, 475. [Google Scholar] [CrossRef]
- Cochran, W.G. Sampling Techniques, 3rd ed.; Wiley: Hoboken, NJ, USA, 1977. [Google Scholar]
- Albano, L.; Matuozzo, A.; Marinelli, P.; Di Giuseppe, G. Knowledge, attitudes and behaviour of hospital health-care workers regarding influenza A/H1N1: A cross sectional survey. BMC Infect. Dis. 2014, 14, 208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantino, C.; Amodio, E.; Vitale, F.; Trucchi, C.; Maida, C.M.; Bono, S.E.; Caracci, F.; Sannasardo, C.E.; Scarpitta, F.; Vella, C.; et al. Human Papilloma Virus Infection and Vaccination: Pre-Post Intervention Analysis on Knowledge, Attitudes and Willingness to Vaccinate Among Preadolescents Attending Secondary Schools of Palermo, Sicily. Int. J. Environ. Res. Public Health 2020, 17, 5362. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, G.; Abbate, R.; Liguori, G.; Albano, L.; Angelillo, I.F. Human papillomavirus and vaccination: Knowledge, attitudes, and behavioural intention in adolescents and young women in Italy. Br. J. Cancer 2008, 99, 225–229. [Google Scholar] [CrossRef] [Green Version]
- Napolitano, F.; Napolitano, P.; Angelillo, I.F. Seasonal influenza vaccination in pregnant women: Knowledge, attitudes, and behaviors in Italy. BMC Infect. Dis. 2017, 17, 48. [Google Scholar] [CrossRef] [Green Version]
- CBOS. Research Reports. Available online: https://www.cbos.pl/EN/publications/reports.php (accessed on 13 September 2021).
- CBOS. Attitudes to Vaccination against COVID-19. Available online: https://www.cbos.pl/EN/publications/reports/2020/154_20.pdf (accessed on 13 September 2021).
- Raciborski, F.; Jankowski, M.; Gujski, M.; Pinkas, J.; Samel-Kowalik, P. Changes in Attitudes towards the COVID-19 Vaccine and the Willingness to Get Vaccinated among Adults in Poland: Analysis of Serial, Cross-Sectional, Representative Surveys, January-April 2021. Vaccines 2021, 9, 832. [Google Scholar] [CrossRef]
- Kraśnicka, J.; Krajewska-Kułak, E.; Klimaszewska, K.; Cybulski, M.; Guzowski, A.; Kowalewska, B.; Jankowiak, B.; Rolka, H.; Doroszkiewicz, H.; Kułak, W. Mandatory and recommended vaccinations in Poland in the views of parents. Hum. Vaccines Immunother. 2018, 14, 2884–2893. [Google Scholar] [CrossRef] [Green Version]
- Nitsch-Osuch, A.; Gołębiak, I.; Wyszkowska, D.; Rosińska, R.; Kargul, L.; Szuba, B.; Tyszko, P.; Brydak, L.B. Influenza Vaccination Coverage Among Polish Patients with Chronic Diseases. Adv. Exp. Med. Biol. 2017, 968, 19–34. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- McLean, C.P.; Anderson, E.R. Brave men and timid women? A review of the gender differences in fear and anxiety. Clin. Psychol. Rev. 2009, 29, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, K.L.; Fink, A.L.; Plebanski, M.; Klein, S.L. Sex and Gender Differences in the Outcomes of Vaccination over the Life Course. Annu. Rev. Cell Dev. Biol. 2017, 33, 577–599. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, C.L.; Ogunseitan, O.A. Gender Differences in the Perception of Genetic Engineering Applied to Human Reproduction. Soc. Indic. Res. 1999, 46, 191–204. [Google Scholar] [CrossRef]
- Simon, R.M. Gender differences in knowledge and attitude towards biotechnology. Public Underst. Sci. 2009, 19, 642–653. [Google Scholar] [CrossRef]
- Galasso, V.; Pons, V.; Profeta, P.; Becher, M.; Brouard, S.; Foucault, M. Gender differences in COVID-19 attitudes and behavior: Panel evidence from eight countries. Proc. Natl. Acad. Sci. USA 2020, 117, 27285–27291. [Google Scholar] [CrossRef]
- Racine-Brzostek, S.E.; Yee, J.K.; Sukhu, A.; Qiu, Y.; Rand, S.; Barone, P.D.; Hao, Y.; Yang, H.S.; Meng, Q.H.; Apple, F.S.; et al. More rapid, robust and sustainable antibody responses to mRNA COVID-19 vaccine in convalescent COVID-19 individuals. JCI Insight 2021, 6, e151477. [Google Scholar] [CrossRef] [PubMed]
- Trougakos, I.P.; Terpos, E.; Zirou, C.; Sklirou, A.D.; Apostolakou, F.; Gumeni, S.; Charitaki, I.; Papanagnou, E.D.; Bagratuni, T.; Liacos, C.I.; et al. Comparative kinetics of SARS-CoV-2 anti-spike protein RBD IgGs and neutralizing antibodies in convalescent and naïve recipients of the BNT162b2 mRNA vaccine versus COVID-19 patients. BMC Med. 2021, 19, 208. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Muecksch, F.; Schaefer-Babajew, D.; Finkin, S.; Viant, C.; Gaebler, C.; Hoffmann, H.-H.; Barnes, C.O.; Cipolla, M.; Ramos, V.; et al. Naturally enhanced neutralizing breadth against SARS-CoV-2 one year after infection. Nature 2021, 595, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Perek, B.; Flisiak, R. Thrombotic Thrombocytopenia after COVID-19 Vaccination: In Search of the Underlying Mechanism. Vaccines 2021, 9, 559. [Google Scholar] [CrossRef] [PubMed]
- Jemielniak, D.; Krempovych, Y. # AstraZeneca vaccine disinformation on Twitter. medRxiv 2021. [Google Scholar] [CrossRef]
- Sadoff, J.; Le Gars, M.; Cardenas, V.; Shukarev, G.; Vaissiere, N.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Scheper, G.; Hendriks, J.; et al. Durability of antibody responses elicited by a single dose of Ad26.COV2.S and substantial increase following late boosting. medRxiv 2021. [Google Scholar] [CrossRef]
- Eshun-Wilson, I.; Mody, A.; Tram, K.H.; Bradley, C.; Sheve, A.; Fox, B.; Thompson, V.; Geng, E.H. Preferences for COVID-19 vaccine distribution strategies in the US: A discrete choice survey. PLoS ONE 2021, 16, e0256394. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Statistics |
|---|---|
| Age (years), median, interquartile Range (min–max) | 44.0, 36.0–58.0 (18–99) |
| Aged <50, % (n) | 62.3 (1513) |
| Aged ≥50, % (n) | 37.7 (914) |
| Gender | |
| Female, % (n) | 50.7 (1231) |
| Male, % (n) | 49.3 (1196) |
| BMI (kg/m2), median, interquartile range (min–max) | 25.5, 22.7–28.9 (14.0–56.1) |
| Underweight (<18.5), % (n) | 2.8 (69) |
| Normal weight (18.5–24.9), % (n) | 42.3 (1027) |
| Overweight (25.0–29.9), % (n) | 34.8 (844) |
| Obesity (≥30.0), % (n) | 20.1 (487) |
| Place of living | |
| Urban, % (n) | 87.0 (2112) |
| Rural, % (n) | 13.0 (315) |
| Education | |
| Primary, % (n) | 1.5 (37) |
| Secondary, % (n) | 3.5 (85) |
| Vocational, % (n) | 24.4 (591) |
| Tertiary, % (n) | 70.6 (1714) |
| Immunosuppression, % (n) | 6.2 (150) |
| Chronic disease, % (n) | 26.5 (643) |
| Diabetes, % (n) | 7.8 (190) |
| Cancer, % (n) | 2.9 (70) |
| Cardiovascular disease, % (n) | 12.2 (296) |
| Chronic kidney disease, % (n) | 2.1 (52) |
| Chronic pulmonary disease, % (n) | 3.4 (83) |
| Asthma, % (n) | 7.0 (170) |
| SARS-CoV-2 infection status | |
| Infected prior to vaccination, % (n) | 13.4 (324) |
| Infected between 1st and 2nd dose, % (n) | 1.5 (37) |
| Infected after full vaccination, % (n) | 6.1 (149) |
| No history of infection, % (n) | 79.0 (1917) |
| Influenza vaccine status | |
| Vaccinated annually, % (n) | 18.4 (447) |
| Vaccinated irregularly, % (n) | 25.2 (611) |
| Never vaccinated, % (n) | 56.4 (1369) |
| Parameter | Willing to Receive (n = 1724) | Unwilling to Receive (n = 598) | χ2 Test p-Value (with Bonferroni Correction) | |
|---|---|---|---|---|
| % | ||||
| Age | <50 | 68.1 | 31.9 | <0.00001 |
| ≥50 | 84.3 | 15.7 | ||
| Gender | Female | 80.0 | 20.0 | <0.00001 |
| Male | 68.4 | 31.6 | ||
| BMI | Underweight | 63.1 | 36.9 | <0.00001 |
| Normal BMI | 70.1 | 29.9 | ||
| Overweight | 74.0 | 26.0 | ||
| Obesity | 84.7 | 15.3 | ||
| Place of living | Urban | 74.8 | 25.2 | >0.05 |
| Rural | 70.4 | 29.6 | ||
| Education | Tertiary | 74.4 | 25.6 | >0.05 |
| Other | 73.9 | 26.1 | ||
| Immunosuppression | Yes | 88.0 | 12.0 | 0.0012 |
| No | 73.3 | 26.7 | ||
| Chronic disease | Yes | 86.5 | 13.5 | <0.00001 |
| No | 69.9 | 30.1 | ||
| SARS-CoV-2 infection status | Not infected | 80.5 | 19.5 | <0.00001 |
| Infected prior to vaccination | 66.9 | 33.1 | ||
| Infected after at least 1 dose | 21.5 | 78.5 | ||
| Influenza vaccine status | Vaccinated annually | 92.4 | 7.6 | <0.00001 |
| Vaccinated irregularly | 86.5 | 13.5 | ||
| Never vaccinated | 62.5 | 37.5 | ||
| Parameter |
Fear ≤5 (n = 1669) |
Fear >5 (n = 55) | χ2 Test
p-Value (with Bonferroni Correction) | |
|---|---|---|---|---|
| % | ||||
| Age | <50 | 95.7 | 4.3 | 0.033 |
| ≥50 | 98.3 | 1.7 | ||
| Gender | Female | 97.2 | 2.8 | >0.05 |
| Male | 96.3 | 3.7 | ||
| BMI | Underweight | 95.1 | 4.9 | >0.05 |
| Normal BMI | 97.1 | 2.9 | ||
| Overweight | 96.3 | 3.7 | ||
| Obesity | 97.2 | 2.8 | ||
| Place of living | Urban | 96.7 | 3.3 | >0.05 |
| Rural | 96.8 | 3.2 | ||
| Education | Tertiary | 97.5 | 2.5 | >0.05 |
| Other | 95.0 | 5.0 | ||
| Immunosuppression | Yes | 92.8 | 7.2 | >0.05 |
| No | 97.2 | 2.9 | ||
| Chronic disease | Yes | 97.6 | 95.1 | >0.05 |
| No | 2.4 | 4.9 | ||
| SARS-CoV-2 infection status | Not infected | 97.8 | 2.2 | <0.00001 |
| Infected prior to vaccination | 95.5 | 4.5 | ||
| Infected after at least 1 dose | 63.2 | 36.8 | ||
| Influenza vaccine status | Vaccinated annually | 96.8 | 3.2 | >0.05 |
| Vaccinated irregularly | 98.6 | 1.4 | ||
| Never vaccinated | 95.7 | 4.3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. https://doi.org/10.3390/vaccines9111286
Rzymski P, Poniedziałek B, Fal A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines. 2021; 9(11):1286. https://doi.org/10.3390/vaccines9111286
Chicago/Turabian StyleRzymski, Piotr, Barbara Poniedziałek, and Andrzej Fal. 2021. "Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland" Vaccines 9, no. 11: 1286. https://doi.org/10.3390/vaccines9111286
APA StyleRzymski, P., Poniedziałek, B., & Fal, A. (2021). Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines, 9(11), 1286. https://doi.org/10.3390/vaccines9111286