
Management of Invasive Infections due to a Rare Arthroconidial Yeast, Saprochaete capitata, in Two Patients with Acute Hematological Malignancies

 ,
, 

Abstract
:1. Introduction
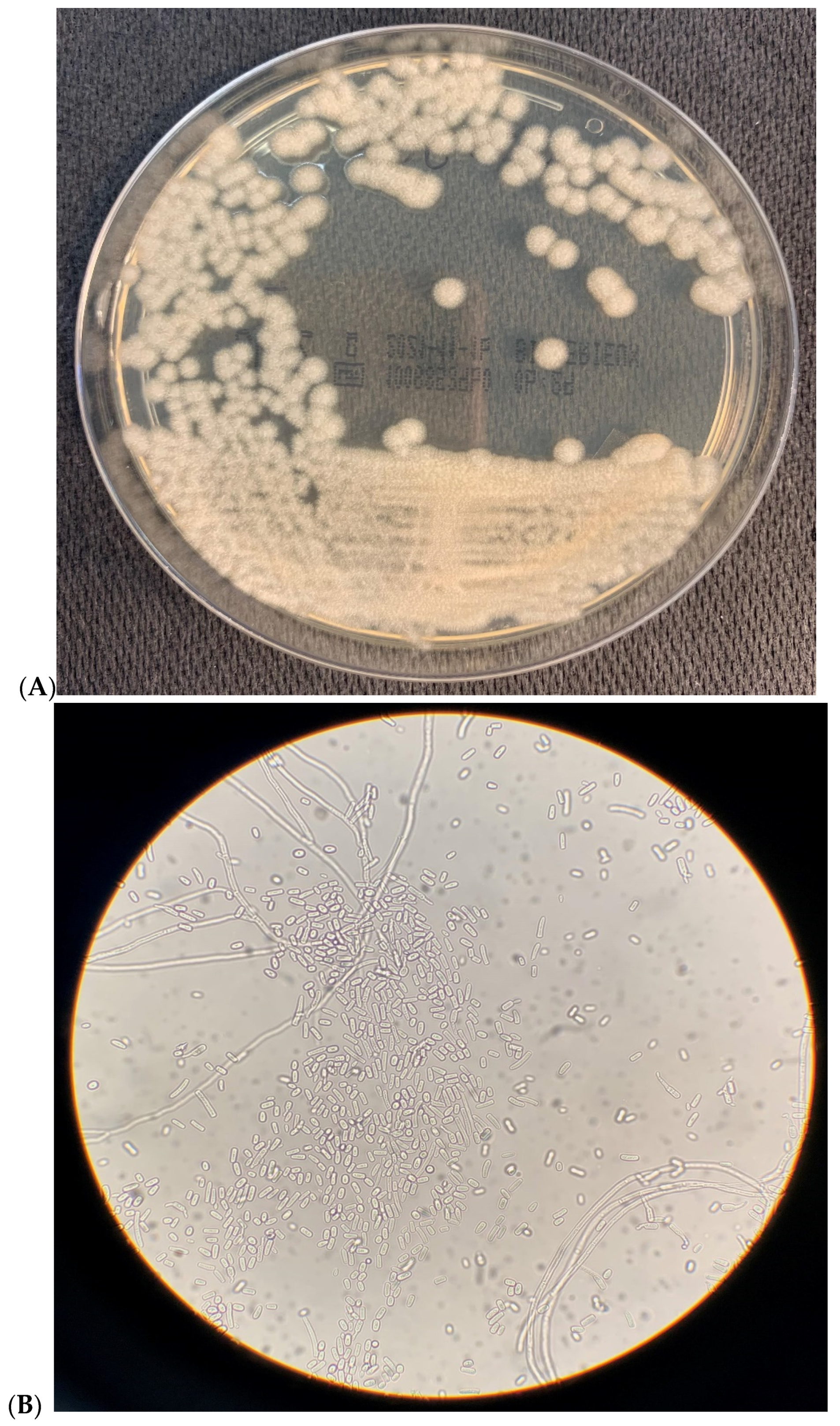
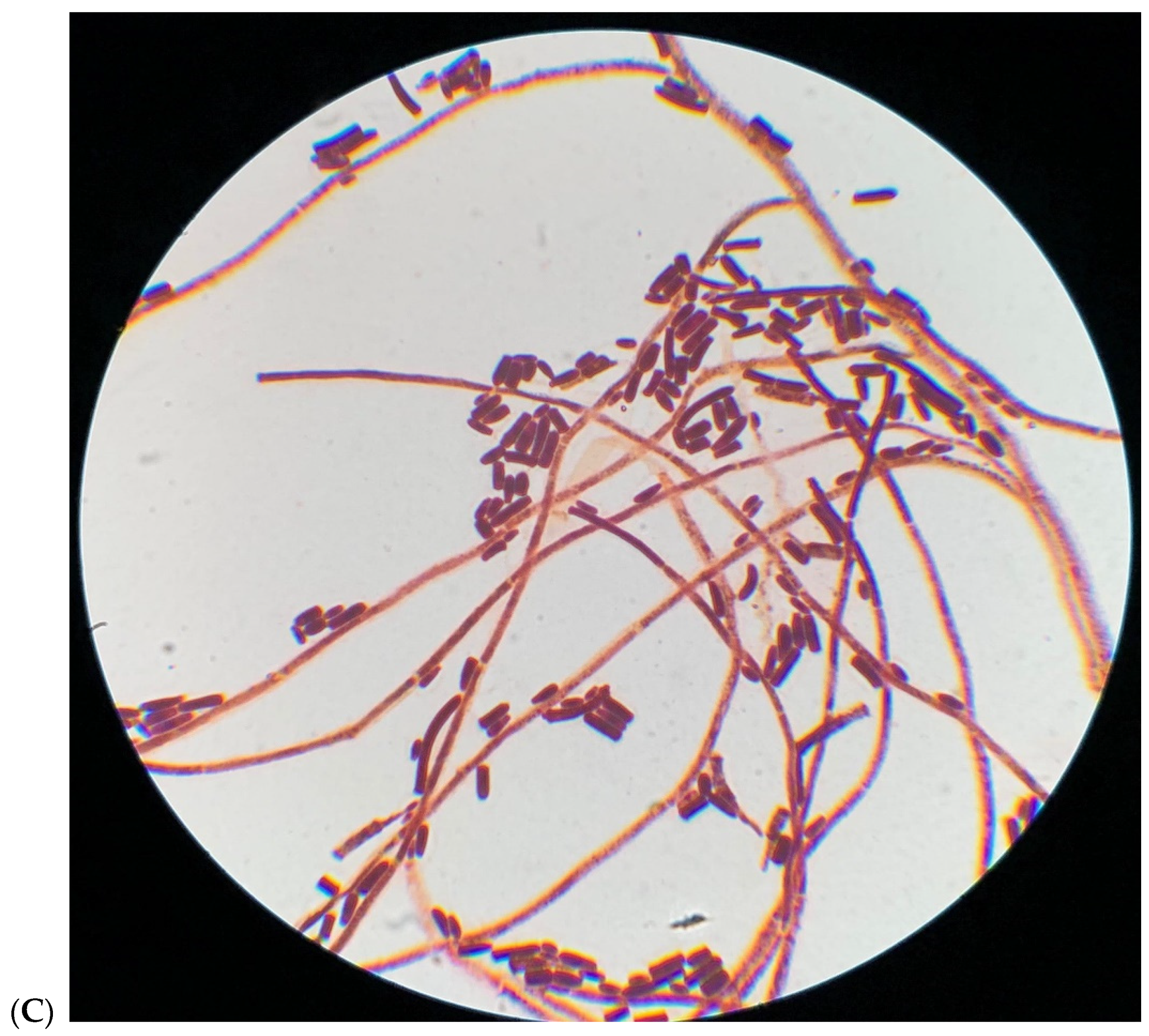
2. Microbiological Results
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Armstrong-James, D.; Bicanic, T.; Brown, G.D.; Hoving, J.C.; Meintjes, G.; Nielsen, K.; Working Group from the EMBO Workshop on AIDS-Related Mycoses. AIDS-related mycoses: Current progress in the field and future priorities. Trends Microbiol. 2017, 25, 428–430. [Google Scholar] [CrossRef] [Green Version]
- Miceli, M.H.; Diaz, J.A.; Lee, S.A. Emerging opportunistic yeast infections. Lancet Infect. Dis. 2011, 11, 142–151. [Google Scholar] [CrossRef]
- Pande, A.; Non, L.R.; Santos, C.A. Pseudozyma and other non-Candida opportunistic yeast bloodstream infections in a large stem cell transplant center. Transpl. Infect. Dis. 2017, 19, e12664. [Google Scholar] [CrossRef] [PubMed]
- De Jong, A.W.; Hagen, F. Attack, defend and persist: How the fungal pathogen Candida auris was able to emerge globally in healthcare environments. Mycopathologia 2019, 184, 353–365. [Google Scholar] [CrossRef] [Green Version]
- Potenza, L.; Chitasombat, M.N.; Klimko, N.; Bettelli, F.; Dragonetti, G.; Del Principe, M.I.; Nucci, M.; Busca, A.; Fracchiolla, N.; Sciumè, M.; et al. Rhodotorula infection in haematological patient: Risk factors and outcome. Mycoses 2018, 62, 223–229. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Rudramurthy, S.; Kale, P.; Hariprasath, P.; Dhaliwal, M.; Singhi, S.; Rao, K.L.N. Epidemiological study of a large cluster of fungaemia cases due to Kodamaea ohmeri in an Indian tertiary care centre. Clin. Microbiol. Infect. 2014, 20, O83–O89. [Google Scholar] [CrossRef] [Green Version]
- Chagas-Neto, T.C.; Chaves, G.M.; Melo, A.S.; Colombo, A.L. Bloodstream infections due to Trichosporon spp.: Species distribution, Trichosporon asahii genotypes determined on the basis of ribosomal DNA intergenic spacer 1 sequencing and antifungal susceptibility testing. J. Clin. Microbiol. 2009, 47, 1074–1081. [Google Scholar] [CrossRef] [Green Version]
- Durán Graeff, L.; Seidei, D.; Vehreschild, M.J.G.T.; Hamprecht, A.; Kindo, A.; Racil, Z.; Demeter, J.; De Hoog, S.; Aurbach, U.; Ziegler, M.; et al. Invasive infections due to Saprochaete and Geotrichum species report of 23 cases from the FungiScope registry. Mycoses 2017, 60, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Gulcan, A.; Gulcan, E.; Keles, M.; Aktas, E. Oral yeast colonization in peritoneal dialysis and hemodialysis patients and renal transplant recipients. Comp. Immunol. Microbiol. Infect. Dis. 2016, 46, 47–52. [Google Scholar] [CrossRef]
- Vallabhaneni, S.; Chiller, T.M. Fungal infections and new biologic therapies. Curr. Rheumatol. Rep. 2016, 18, 29. [Google Scholar] [CrossRef]
- Vallabhaneni, S.; Mody, R.K.; Walker, T.; Chiller, T. The global burden of fungal diseases. Infect. Dis. Clin. N. Am. 2016, 30, 1–11. [Google Scholar] [CrossRef]
- Colombo, A.L.; de Almeida Jùnior, J.N.; Slavin, M.A.; Chen, S.C.; Sorrell, T.C. Candida and invasive mould diseases in non-neutropenic critically ill patients and patients with haematological cancer. Lancet Infect. Dis. 2017, 17, e344–e356. [Google Scholar] [CrossRef]
- Li, H.; Guo, M.; Wang, C.; Li, Y.; Fernandez, A.M.; Ferraro, T.N.; Yang, R.; Chen, Y. Epidemiological study of Trichosporon asahii infections over the past 23 years. Epidemiol Infect. 2020, 148, e169. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Boekhoni, T.; Akova, M.; Meis, J.F.; Cornely, O.A.; Lortholary, O.; European Confederation of Medical Mycology. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of rare invasive yeast infections. Clin. Microbiol. Infect. 2014, 20, 76–98. [Google Scholar] [CrossRef] [Green Version]
- Pfaller, M.A.; Messer, S.A.; Woosley, L.N.; Jones, R.N.; Castanheira, M. Echinocandin and triazole antifungal susceptibility profiles for clinical opportunistic yeast and mold isolates collected from 2010 to 2011: Application of new CLSI clinical breakpoint and epidemiological cutoff values for characterization of geographic and temporal trends of antifungal resistance. J. Clin. Microbiol. 2013, 51, 2571–2581. [Google Scholar] [PubMed] [Green Version]
- Diekema, D.J.; Petroelje, B.; Messer, S.A.; Hollis, R.J.; Pfaller, M.A. Activities of available and investigational antifungal agents against Rhodotorula species. J. Clin. Microbiol. 2005, 43, 476–478. [Google Scholar] [CrossRef] [Green Version]
- Schuermans, C.; van Bergen, M.; Coorevits, L.; Verhaegen, J.; Lagrou, K.; Surmont, I.; Jeurissen, A. Breaktrough Saprochaete capitata infections in patients receiving echinocandins: Case report and review of the literature. Med. Mycol. 2011, 49, 414–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornely, O.A.; Hoenigl, M.; Lass-Florl, C.; Chen, S.C.-A.; Kontoyiannis, D.P.; Morrissey, C.O.; Thompson, G.R.; Mycoses Study Group Education and research Consortium (MSG-ERC) and the European Confederation of Medical Mycology (ECMM). Defining breakthrough invasive fungal infection-position paper of the mycoses study group education and research consortium and the European Confederation of Medical Mycology. Mycoses 2019, 62, 716–729. [Google Scholar] [PubMed]
- Trabelsi, H.; Neji, S.; Gargouri, L.; Sellami, H.; Guidara, R.; Cheikhrouhou, F.; Bellaaj, H.; Makni, F.; Elloumi, M.; Ayadiet, A. Geotrichum capitatum septicemia: Case report and review of the literature. Mycopathologia 2015, 179, 465–469. [Google Scholar] [CrossRef]
- Ulu-Kilic, A.; Atalay, M.A.; Metan, G.; Cevahir, F.; Koc, N.; Eser, B.; Çetin, M.; Kaynar, L.; Alp, E. Saprochaetae capitata as an emerging fungus among patients with haematological malignencies. Mycoses 2015, 58, 491–497. [Google Scholar] [CrossRef]
- de Hoog, G.S.; Smith, M.T. The ribosomal gene phylogeny and species delimitation in Geotrichum and its teleomorphs. Stud. Mycol. 2004, 50, 489–515. [Google Scholar]
- Chang, W.W.; Buerger, L. Disseminated geotrichosis: Case report. Arch. Intern. Med. 1964, 113, 356–360. [Google Scholar] [CrossRef]
- Lo Cascio, G.; Vincenzi, M.; Soldani, F.; De Carolis, E.; Maccacaro, L.; Sorrentino, A.; Nadali, G.; Cesaro, S.; Sommavilla, M.; Niero, V.; et al. Outbreak of Saprochaete clavata Sepsis in Hematology Patients: Combined Use of MALDI-TOF and Sequencing Strategy to Identify and Correlate the Episodes. Front. Microbiol. 2020, 11, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaux, S.; Criscuolo, A.; Desnos-Ollivier, M.; Diancourt, L.; Tarnaud, C.; Vandenbogaert, M.; Brisse, S.; Coignard, B.; Dromer, F. Multicenter outbreak of infections by Saprochaete clavata, an unrecognized opportunistic fungal pathogen. MBio 2014, 5, e02309-14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchta, V.; Bolehovská, R.; Hovorková, E.; Cornely, O.A.; Seidel, D.; Žák, P. Saprochaete clavata Invasive Infections—A New Threat to Hematological-Oncological Patients. Front. Microbiol. 2019, 10, 2196. [Google Scholar] [CrossRef]
- Mazzocato, S.; Marchionni, E.; Fothergill, A.W.; Sutton, D.A.; Staffolani, S.; Gesuita, R.; Skrami, E.; Fiorentini, A.; Manso, E.; Barchiesi, F. Epidemiology and outcome of systemic infections due to Saprochaete capitata: Case report and review of the literature. Infection 2015, 43, 211–215. [Google Scholar] [CrossRef]
- Erman, B.; Fırtına, S.; Aksoy, B.A.; Aydogdu, S.; Genç, G.E.; Doğan, Ö.; Bozkurt, C.; Fışgın, T.; Çipe, F.E. Invasive Saprochaete capitata Infection in a Patient with Autosomal Recessive CARD9 Deficiency and a Review of the Literature. J. Clin. Immunol. 2020, 40, 466–474. [Google Scholar] [CrossRef]
- Pamidimukkala, U.; Kancharla, A.; Sudhaharan, S.; Gundeti, S.; Mandarapu, S.; Nagalla, V.K.; Raju, S.B.; Karanam, S.D. Isolation of the Rare Opportunistic Yeast Saprochaete capitata from Clinical Samples-Experience from a Tertiary Care Hospital in Southern India and a Brief Review of the Literature. J. Clin. Diagn. Res. 2017, 11, Dc36–Dc42. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Ruiz, J.C.; Lopez-Soria, L.; Olazabal, I.; Amutio, E.; Arrieta-Aguirre, I.; Velasco-Benito, V.; Ponton, J.; Moragues, M.D. Invasive infections caused by Saprochaete capitata in patients with haematological malignancies: Report of five cases and review of the antifungal therapy. Rev. Iberoam. Micol. 2013, 30, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Desnos-Ollivier, M.; Blanc, C.; Garcia-Hermoso, D.; Hoinard, D.; Alanio, A.; Dromer, F. Misidentification of Saprochaete clavata as Magnusiomyces capitatus in clinical isolates: Utility of internal transcribed spacer sequencing and matrix-assisted laser desorption ionization-time of flight mass spectrometry and importance of reliable databases. J. Clin. Microbiol. 2014, 52, 2196–2198. [Google Scholar]
- Kaplan, E.; Al-Hatmi, A.M.S.; Ilkit, M.; Gerrits van den Ende, A.H.G.; Hagen, F.; Meis, J.F.; de Hoog, G.S. Molecular Diagnostics of Arthroconidial Yeasts, Frequent Pulmonary Opportunists. J. Clin. Microbiol. 2018, 56, e01427-17. [Google Scholar] [CrossRef] [Green Version]
- Kolecka, A.; Khayhan, K.; Groenewald, M.; Theelen, B.; Arabatzis, M.; Velegraki, A.; Kostrzewa, M.; Mares, M.; Taj-Aldeen, S.J.; Boekhout, T. Identification of medically relevant species of arthroconidial yeasts by use of matrix-assisted laser desorption ionization-time of flight mass spectrometry. J. Clin. Microbiol. 2013, 51, 2491–2500. [Google Scholar] [CrossRef] [Green Version]
- Gadea, I.; Cuenca-Estrella, M.; Prieto, E.; Diaz-Guerra, T.M.; Garcia-Cia, J.I.; Mellado, E.; Tomas, J.F.; Rodriguez-Tuleda, J.F. Genotyping and antifungal susceptibility profile of Dipodascus capitatus isolates causing disseminated infection in seven hematological patients of a tertiary hospital. J. Clin. Microbiol. 2004, 42, 1832–1836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christakis, G.; Perlorentzou, S.; Aslanidou, M.; Megalakaki, A.; Velegraki, A. Fatal blastoschizomyces capitatus sepsis in a neutropenic patient with acute myeloid leukemia: First documented case from Greece. Mycoses 2005, 48, 216–220. [Google Scholar] [CrossRef]
- Girmenia, C.; Pagano, L.; Martino, B.; D’Antonio, D.; Fanci, R.; Specchia, G.; Melillo, L.; Buelli, M.; Pizzarelli, G.; Venditti, M.; et al. GIMEMA Infection Program. Invasive infections caused by Trichosporon species and Geotrichum capitatum in patients with hematological malignancies: A retrospective multicenter study from Italy and review of the literature. J. Clin. Microbiol. 2005, 43, 1818–1828. [Google Scholar] [CrossRef] [Green Version]
- Del Principe, M.I.; Sarmati, L.; Cefalo, M.; Fontana, C.; De Santis, G.; Buccisano, F.; Maurillo, L.; De Bellis, E.; Postorino, M.; Sconocchia, G.; et al. A cluster of Geotrichum clavatum (Saprochaete clavata) infection in haematological patients: A first Italian report and review of literature. Mycoses 2016, 59, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Esposto, M.C.; Prigitano, A.; Lo Cascio, G.; Ossi, C.; Grancini, A.; Cavanna, C.; Lallitto, F.; Tejada, M.; Bandettini, R.; Mularoni, A.; et al. Yeast-like filamentous fungi: Molecular identification and in vitro susceptibility study. Med. Mycol. 2018, 57, 909–913. [Google Scholar] [CrossRef]
- Leoni, M.; Riccardi, N.; Rotulo, G.A.; Godano, E.; Faraci, M.; Bandettini, R.; Esposto, M.C.; Castagnola, E. Magnusiomyces clavatus infection in a child after allogeneic hematotopoietic stem cell transplantation: Diagnostic and therapeutic implications. Med. Mycol. Case Rep. 2018, 23, 65–67. [Google Scholar] [CrossRef]
- Salgüero Fernández, I.; Nájera Botello, L.; Orden Martinez, B.; Roustan Gullón, G. Disseminated fungemia by Saprochaete clavata. Enferm. Infecc. Microbiol. Clin. 2018, 37, 283–284. [Google Scholar] [CrossRef] [PubMed]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Bennett, J.E.; Pappas, P.G.; Maertens, J.; Lortholary, O.; et al. Revised definitions of invasive fungal disease from the European organization for research and treatment of cancer/invasive fungal infections cooperative group and the national institute of allergy and infectious diseases mycoses study group (EORTC/MSG) consensus group. Clin. Infect. Dis. 2008, 46, 1813–1821. [Google Scholar] [PubMed]
- Martino, P.; Venditti, M.; Micozzi, A.; Morace, G.; Polonelli, L.; Mantovani, M.P.; Petti, M.C.; Burgio, V.L.; Santini, C.; Serra, P.; et al. Blastoschizomyces capitatus: An emerging cause of invasive fungal disease in leukemia patients. Rev. Infect. Dis. 1990, 12, 570–582. [Google Scholar] [CrossRef]
- Martino, R.; Salavert, M.; Parody, R.; Tomas, J.F.; de la Camara, R.; Vazquez, L.; Jarque, I.; Prieto, E.; Sastre, J.L.; Gadea, I.; et al. Blastoschizomyces capitatus infection in patients with leukemia: Report of 26 cases. Clin. Infect. Dis. 2004, 38, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Birrenbach, T.; Bertschy, S.; Aebersold, F.; Mueller, N.J.; Achermann, Y.; Muehlethaler, K.; Zimmerli, S. Emergence of Blastoschizomyces capitatus yeast infections, Central Europe. Emerg. Infect. Dis. 2012, 18, 98–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saghrouni, F.; Abdeljelil, J.B.; Youssef, Y.B.; Abdeljelil, N.B.; Gheith, S.; Fathallah, A.; Said, M.B. Geotrichum capitatum septicemia in patients with acute myeloid leukemia. Report of three cases. Med. Mycol. Case Rep. 2012, 1, 88–90. [Google Scholar] [CrossRef]
- Subramanya Supram, H.; Gokhale, S.; Chakrabarti, A.; Rudramurthy, S.M.; Gupta, S.; Honnavar, P. Emergence of Magnusiomyces capitatus infections in western Nepal. Med. Mycol. 2016, 54, 103–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arrieta-Aguirre, I.; Menendez-Manjon, P.; Cuétara, M.S.; de Larrinoa, I.F.; Garcia-Ruiz, J.C.; Moragues, M.D. Sequencing of FKS hot spot 1 from Saprochaete capitate to search a relationship to reduced echinocandin susceptibility. Antimicrob. Agents Chemother. 2018, 62, e01246-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Drugs (μg/mL) | Patient 1 | Patient 2 |
|---|---|---|
| 5-Fluorocytosine | 16 | 16 |
| Amphotericin B | 1 | 1 |
| Anidulafungin | 2 | 2 |
| Caspofungin | 8 | 8 |
| Fluconazole | 8 | 8 |
| Itraconazole | 0.25 | 0.5 |
| Micafungin | 2 | 8 |
| Posaconazole | 0.5 | 1 |
| Voriconazole | 0.12 | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gurrieri, F.; Corbellini, S.; Piccinelli, G.; Turra, A.; Morello, E.; Malagola, M.; Russo, D.; Caruso, A.; De Francesco, M.A. Management of Invasive Infections due to a Rare Arthroconidial Yeast, Saprochaete capitata, in Two Patients with Acute Hematological Malignancies. Vaccines 2021, 9, 1289. https://doi.org/10.3390/vaccines9111289
Gurrieri F, Corbellini S, Piccinelli G, Turra A, Morello E, Malagola M, Russo D, Caruso A, De Francesco MA. Management of Invasive Infections due to a Rare Arthroconidial Yeast, Saprochaete capitata, in Two Patients with Acute Hematological Malignancies. Vaccines. 2021; 9(11):1289. https://doi.org/10.3390/vaccines9111289
Chicago/Turabian StyleGurrieri, Francesca, Silvia Corbellini, Giorgio Piccinelli, Alessandro Turra, Enrico Morello, Michele Malagola, Domenico Russo, Arnaldo Caruso, and Maria Antonia De Francesco. 2021. "Management of Invasive Infections due to a Rare Arthroconidial Yeast, Saprochaete capitata, in Two Patients with Acute Hematological Malignancies" Vaccines 9, no. 11: 1289. https://doi.org/10.3390/vaccines9111289
APA StyleGurrieri, F., Corbellini, S., Piccinelli, G., Turra, A., Morello, E., Malagola, M., Russo, D., Caruso, A., & De Francesco, M. A. (2021). Management of Invasive Infections due to a Rare Arthroconidial Yeast, Saprochaete capitata, in Two Patients with Acute Hematological Malignancies. Vaccines, 9(11), 1289. https://doi.org/10.3390/vaccines9111289