
Ocular Manifestations after Receiving COVID-19 Vaccine: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
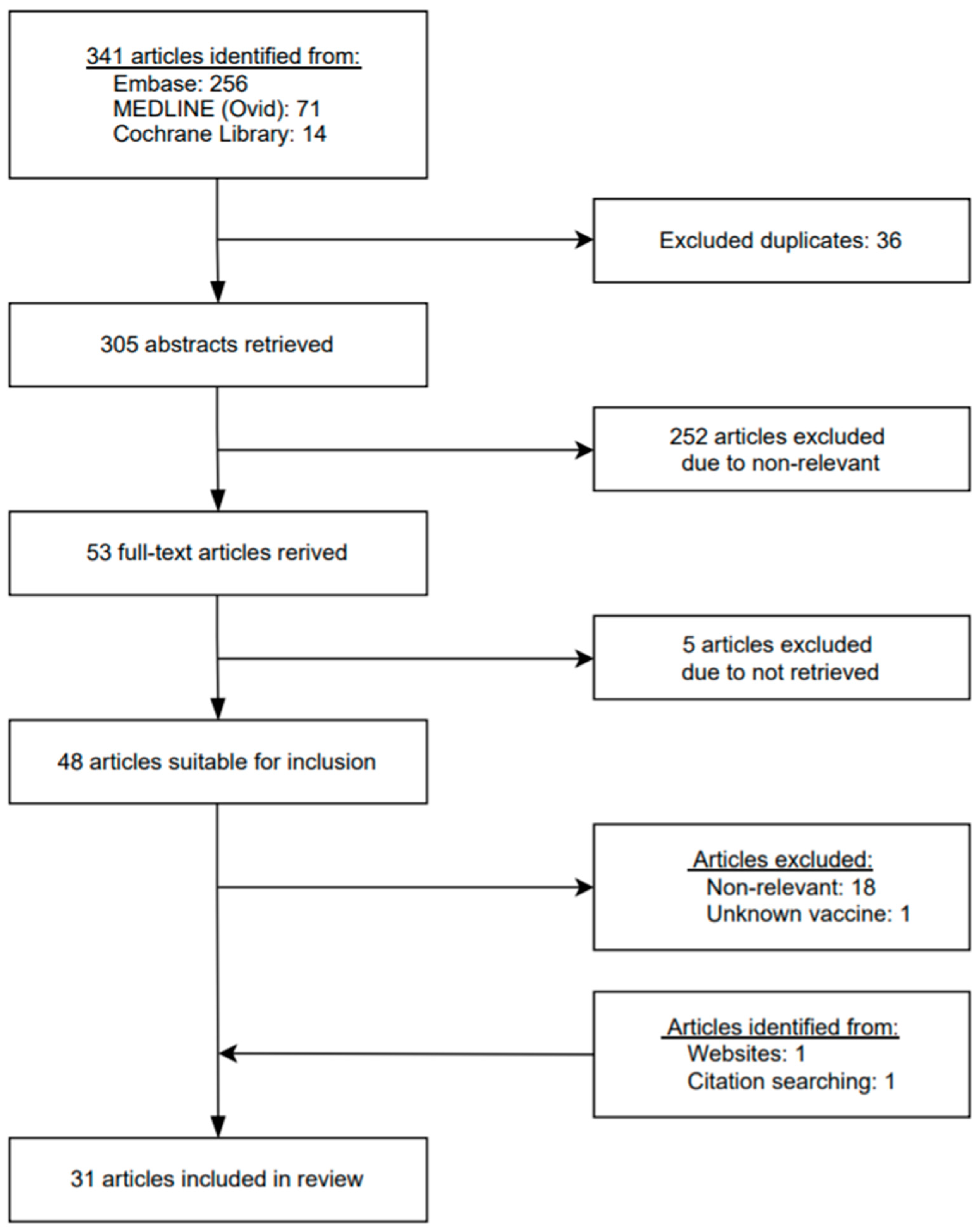
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Analysis
3. Results
3.1. Eyelid
- Eyelid swelling
- Eyelid purpuric lesions
- Herpes Zoster Ophthalmicus (HZO)
3.2. Cornea and Ocular Surface
- Corneal graft rejection after penetrating keratoplasty (PKP)
- Corneal graft rejection after Descemet membrane endothelial keratoplasty (DMEK)
3.3. Retina
- Acute Macular Neuroretinopathy (AMN)
- Central serous retinopathy
- Retinal detachment
3.4. Uvea
- Acute anterior uveitis
- Panuveitis
- Multifocal Choroiditis
- Acute zonal occult outer retinopathy (AZOOR)
- Reactivation of Vogt-Koyanagi-Harada (VKH) Disease
- Uveitis
3.5. Nerve
- Optic neuritis
- Arteritic anterior ischemic optic neuropathy (AAION)
- Abducens nerve palsy
3.6. Vascular Thrombosis
- Superior ophthalmic vein (SOV) thrombosis
- Cerebral venous sinus thrombosis (CVST)
- Thrombocytopenia with acute ischemic stroke and bleeding
3.7. Other Reports with Only Ocular Symptoms Mentioned
4. Discussion
4.1. mRNA Vaccines
4.2. Adenoviral Vector Vaccines
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Lundstrom, K.; Barh, D.; Uhal, B.D.; Takayama, K.; Aljabali, A.A.A.; Abd El-Aziz, T.M.; Lal, A.; Redwan, E.M.; Adadi, P.; Chauhan, G.; et al. COVID-19 Vaccines and Thrombosis-Roadblock or Dead-End Street? Biomolecules 2021, 11, 1020. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration—COVID-19 Vaccines. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/covid-19-vaccines (accessed on 21 September 2021).
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA Vaccine against SARS-CoV-2—Preliminary Report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef]
- Mercado, N.B.; Zahn, R.; Wegmann, F.; Loos, C.; Chandrashekar, A.; Yu, J.; Liu, J.; Peter, L.; McMahan, K.; Tostanoski, L.H.; et al. Single-shot Ad26 vaccine protects against SARS-CoV-2 in rhesus macaques. Nature 2020, 586, 583–588. [Google Scholar] [CrossRef]
- Arashkia, A.; Jalilvand, S.; Mohajel, N.; Afchangi, A.; Azadmanesh, K.; Salehi-Vaziri, M.; Fazlalipour, M.; Pouriayevali, M.H.; Jalali, T.; Mousavi Nasab, S.D.; et al. Severe acute respiratory syndrome-coronavirus-2 spike (S) protein based vaccine candidates: State of the art and future prospects. Rev. Med. Virol. 2021, 31, e2183. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- JAMA Network Open—Instructions for Authors: Ratings of the Quality of the Vidence. Available online: https://jamanetwork.com/journals/jamanetworkopen/pages/instructions-for-authors#SecRatingsofQuality (accessed on 21 September 2021).
- The Centre for Evidence-Based Medicine. Available online: https://www.cebm.net/ (accessed on 21 September 2021).
- Al Khames Aga, Q.A.; Alkhaffaf, W.H.; Hatem, T.H.; Nassir, K.F.; Batineh, Y.; Dahham, A.T.; Shaban, D.; Al Khames Aga, L.A.; Agha, M.Y.R.; Traqchi, M. Safety of COVID-19 vaccines. J. Med. Virol. 2021, 93, 6588–6594. [Google Scholar] [CrossRef] [PubMed]
- Mazzatenta, C.; Piccolo, V.; Pace, G.; Romano, I.; Argenziano, G.; Bassi, A. Purpuric lesions on the eyelids developed after BNT162b2 mRNA COVID-19 vaccine: Another piece of SARS-CoV-2 skin puzzle? J. Eur. Acad. Dermatol. Venereol. 2021, 35, e543–e545. [Google Scholar] [CrossRef]
- Furer, V.; Zisman, D.; Kibari, A.; Rimar, D.; Paran, Y.; Elkayam, O. Herpes zoster following BNT162b2 mRNA Covid-19 vaccination in patients with autoimmune inflammatory rheumatic diseases: A case series. Rheumatology 2021, 12, 12. [Google Scholar] [CrossRef]
- Ravichandran, S.; Natarajan, R. Corneal graft rejection after COVID-19 vaccination. Indian J. Ophthalmol. 2021, 69, 1953–1954. [Google Scholar]
- Wasser, L.M.; Roditi, E.; Zadok, D.; Berkowitz, L.; Weill, Y. Keratoplasty Rejection After the BNT162b2 messenger RNA Vaccine. Cornea 2021, 40, 1070–1072. [Google Scholar] [CrossRef] [PubMed]
- Crnej, A.; Khoueir, Z.; Cherfan, G.; Saad, A. Acute corneal endothelial graft rejection following COVID-19 vaccination. J. Fr. Ophtalmol. 2021, 8, 8. [Google Scholar] [CrossRef] [PubMed]
- Phylactou, M.; Li, J.P.O.; Larkin, D.F.P. Characteristics of endothelial corneal transplant rejection following immunisation with SARS-CoV-2 messenger RNA vaccine. Br. J. Ophthalmol. 2021, 105, 893–896. [Google Scholar] [CrossRef] [PubMed]
- Mambretti, M.; Huemer, J.; Torregrossa, G.; Ullrich, M.; Findl, O.; Casalino, G. Acute Macular Neuroretinopathy following Coronavirus Disease 2019 Vaccination. Ocul. Immunol. Inflamm. 2021, 29, 730–733. [Google Scholar] [CrossRef]
- Bøhler, A.D.; Strøm, M.E.; Sandvig, K.U.; Moe, M.C.; Jørstad, Ø.K. Acute macular neuroretinopathy following COVID-19 vaccination. Eye 2021, 22, 1–2. [Google Scholar] [CrossRef]
- Gabka, K.; Groselli, S.; Ulbig, M. Flickering scotoma after COVID vaccination: A further possible side effect of vaccination? Ophthalmologe 2021, 118, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Book, B.A.J.; Schmidt, B.; Foerster, A.M.H. Bilateral Acute Macular Neuroretinopathy after Vaccination against SARS-CoV-2. JAMA Ophthalmol. 2021, 139, e212471. [Google Scholar] [CrossRef]
- Fowler, N.; Mendez Martinez, N.R.; Pallares, B.V.; Maldonado, R.S. Acute-onset central serous retinopathy after immunization with COVID-19 mRNA vaccine. Am. J. Ophthalmol. Case Rep. 2021, 23, 101136. [Google Scholar] [CrossRef]
- Subramony, R.; Lin, L.C.; Knight, D.K.; Aminlari, A.; Belovarski, I. Bilateral Retinal Detachments in a Healthy 22-year-old Female Following Moderna SARS-CoV-2 Vaccination. J. Emerg. Med. 2021, 16, S0736-4679. [Google Scholar] [CrossRef]
- Renisi, G.; Lombardi, A.; Massimo, S.; Alessandro, I.; Bandera, A.; Gori, A. Anterior uveitis onset after bnt162b2 vaccination: Is this just a coincidence? Int. J. Infect. Dis. 2021, 18, 18. [Google Scholar] [CrossRef]
- Mudie, L.I.; Zick, J.D.; Dacey, M.S.; Palestine, A.G. Panuveitis following Vaccination for COVID-19. Ocul. Immunol. Inflamm. 2021, 29, 741–742. [Google Scholar] [CrossRef]
- Goyal, M.; Murthy, S.I.; Annum, S. Bilateral Multifocal Choroiditis following COVID-19 Vaccination. Ocul. Immunol. Inflamm. 2021, 29, 753–757. [Google Scholar] [CrossRef]
- Maleki, A.; Look-Why, S.; Manhapra, A.; Foster, C.S. COVID-19 Recombinant mRNA Vaccines and Serious Ocular Inflammatory Side Effects: Real or Coincidence? J. Ophthalmic. Vis. Res. 2021, 16, 490–501. [Google Scholar] [CrossRef]
- Papasavvas, I.; Herbort, C.P. Reactivation of Vogt-Koyanagi-Harada disease under control for more than 6 years, following anti-SARS-CoV-2 vaccination. J. Ophthalmic Inflamm. Infect. 2021, 11, 21. [Google Scholar] [CrossRef]
- Furer, V.; Eviatar, T.; Zisman, D.; Peleg, H.; Paran, D.; Levartovsky, D.; Zisapel, M.; Elalouf, O.; Kaufman, I.; Meidan, R.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann. Rheum. Dis. 2021, 80, 200–201. [Google Scholar] [CrossRef]
- Helmchen, C.; Buttler, G.M.; Markewitz, R.; Hummel, K.; Wiendl, H.; Boppel, T. Acute bilateral optic/chiasm neuritis with longitudinal extensive transverse myelitis in longstanding stable multiple sclerosis following vector-based vaccination against the SARS-CoV-2. J. Neurol. 2021, 15, 1–6. [Google Scholar] [CrossRef]
- Reyes-Capo, D.P.; Stevens, S.M.; Cavuoto, K.M. Acute abducens nerve palsy following COVID-19 vaccination. J. AAPOS 2021. [Google Scholar] [CrossRef]
- Panovska-Stavridis, I.; Pivkova-Veljanovska, A.; Trajkova, S.; Lazarevska, M.; Grozdanova, A.; Filipche, V. A rare case of superior ophthalmic vein thrombosis and thrombocytopenia following ChAdOx1 nCoV-19 vaccine against SARS-CoV-2. Mediterr. J. Hematol. Infect. Dis. 2021, 13, e2021048. [Google Scholar] [CrossRef]
- Bayas, A.; Menacher, M.; Christ, M.; Behrens, L.; Rank, A.; Naumann, M. Bilateral superior ophthalmic vein thrombosis, ischaemic stroke, and immune thrombocytopenia after ChAdOx1 nCoV-19 vaccination. Lancet 2021, 397, e11. [Google Scholar] [CrossRef]
- Castelli, G.P.; Pognani, C.; Sozzi, C.; Franchini, M.; Vivona, L. Cerebral venous sinus thrombosis associated with thrombocytopenia post-vaccination for COVID-19. Crit. Care 2021, 25, 137. [Google Scholar] [CrossRef]
- Wolf, M.E.; Luz, B.; Niehaus, L.; Bhogal, P.; Bäzner, H.; Henkes, H. Thrombocytopenia and intracranial venous sinus thrombosis after “covid-19 vaccine astrazeneca” exposure. J. Clin. Med. 2021, 10, 1599. [Google Scholar] [CrossRef]
- Suresh, P.; Petchey, W. ChAdOx1 nCOV-19 vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis (CVST). BMJ Case Rep. 2021, 14, e243931. [Google Scholar] [CrossRef]
- Dias, L.; Soares-dos-Reis, R.; Meira, J.; Ferrão, D.; Soares, P.R.; Pastor, A.; Gama, G.; Fonseca, L.; Fagundes, V.; Carvalho, M. Cerebral Venous Thrombosis after BNT162b2 mRNA SARS-CoV-2 vaccine. J. Stroke Cerebrovasc. Dis. 2021, 30, 105906. [Google Scholar] [CrossRef]
- See, I.; Su, J.R.; Lale, A.; Woo, E.J.; Guh, A.Y.; Shimabukuro, T.T.; Streiff, M.B.; Rao, A.K.; Wheeler, A.P.; Beavers, S.F.; et al. US Case Reports of Cerebral Venous Sinus Thrombosis With Thrombocytopenia After Ad26.COV2.S Vaccination, 2 March to 21 April 2021. JAMA 2021, 325, 2448–2456. [Google Scholar] [CrossRef]
- Blauenfeldt, R.A.; Kristensen, S.R.; Ernstsen, S.L.; Kristensen, C.C.H.; Simonsen, C.Z.; Hvas, A.M. Thrombocytopenia with acute ischemic stroke and bleeding in a patient newly vaccinated with an adenoviral vector-based COVID-19 vaccine. J. Thromb. Haemost. 2021, 19, 1771–1775. [Google Scholar] [CrossRef]
- Santovito, L.S.; Pinna, G. Acute reduction of visual acuity and visual field after Pfizer-BioNTech COVID-19 vaccine 2nd dose: A case report. Inflamm. Res. 2021, 70, 931–933. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef]
- Heinz, F.X.; Stiasny, K. Distinguishing features of current COVID-19 vaccines: Knowns and unknowns of antigen presentation and modes of action. NPJ Vaccines 2021, 6, 104. [Google Scholar] [CrossRef]
- Cunningham, E.T., Jr.; Moorthy, R.S.; Fraunfelder, F.W.; Zierhut, M. Vaccine-Associated Uveitis. Ocul. Immunol. Inflamm. 2019, 27, 517–520. [Google Scholar] [CrossRef]
- Dicks, M.D.; Spencer, A.J.; Edwards, N.J.; Wadell, G.; Bojang, K.; Gilbert, S.C.; Hill, A.V.; Cottingham, M.G. A novel chimpanzee adenovirus vector with low human seroprevalence: Improved systems for vector derivation and comparative immunogenicity. PLoS ONE 2012, 7, e40385. [Google Scholar] [CrossRef] [Green Version]
- Logunov, D.Y.; Dolzhikova, I.V.; Zubkova, O.V.; Tukhvatulin, A.I.; Shcheblyakov, D.V.; Dzharullaeva, A.S.; Grousova, D.M.; Erokhova, A.S.; Kovyrshina, A.V.; Botikov, A.G.; et al. Safety and immunogenicity of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine in two formulations: Two open, non-randomised phase 1/2 studies from Russia. Lancet 2020, 396, 887–897. [Google Scholar] [CrossRef]
- Eric, K.; Lea, K.; Jenny, R.; Silvia, B.; Stefan, K.; Rolf, M. “Vaccine-Induced Covid-19 Mimicry” Syndrome: Splice reactions within the SARS-CoV-2 Spike open reading frame result in Spike protein variants that may cause thromboembolic events in patients immunized with vector-based vaccines. Res. Sq. 2021. [Google Scholar] [CrossRef]
- MacIntyre, C.R.; Veness, B.; Berger, D.; Hamad, N.; Bari, N. Thrombosis with Thrombocytopenia Syndrome (TTS) following AstraZeneca ChAdOx1 nCoV-19 (AZD1222) COVID-19 vaccination—A risk-benefit analysis for people <60 years in Australia. Vaccine 2021, 39, 4784–4787. [Google Scholar] [CrossRef]
- MacNeil, J.R.; Su, J.R.; Broder, K.R.; Guh, A.Y.; Gargano, J.W.; Wallace, M.; Hadler, S.C.; Scobie, H.M.; Blain, A.E.; Moulia, D.; et al. Updated Recommendations from the Advisory Committee on Immunization Practices for Use of the Janssen (Johnson & Johnson) COVID-19 Vaccine After Reports of Thrombosis with Thrombocytopenia Syndrome Among Vaccine Recipients—United States, April 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 651–656. [Google Scholar] [CrossRef]
- Douxfils, J.; Favresse, J.; Dogne, J.M.; Lecompte, T.; Susen, S.; Cordonnier, C.; Lebreton, A.; Gosselin, R.; Sie, P.; Pernod, G.; et al. Hypotheses behind the very rare cases of thrombosis with thrombocytopenia syndrome after SARS-CoV-2 vaccination. Thromb. Res. 2021, 203, 163–171. [Google Scholar] [CrossRef]
- Bhavsar, K.V.; Lin, S.; Rahimy, E.; Joseph, A.; Freund, K.B.; Sarraf, D.; Cunningham, E.T. Acute macular neuroretinopathy: A comprehensive review of the literature. Surv. Ophthalmol. 2016, 61, 538–565. [Google Scholar] [CrossRef]
- Ng, X.L.; Betzler, B.K.; Testi, I.; Ho, S.L.; Tien, M.; Ngo, W.K.; Zierhut, M.; Chee, S.P.; Gupta, V.; Pavesio, C.E.; et al. Ocular Adverse Events After COVID-19 Vaccination. Ocul. Immunol. Inflamm. 2021, 1–9. [Google Scholar] [CrossRef]
- Sopp, N.M.; Sharda, V. An Eye on COVID-19: A Meta-analysis of Positive Conjunctival Reverse Transcriptase-Polymerase Chain Reaction and SARS-CoV-2 Conjunctivitis Prevalence. Optom. Vis. Sci. 2021, 98, 429–436. [Google Scholar] [CrossRef]


{kind=link}
| Study | Type | Rating Score * | Age (Years) | Sex | Vaccine | Dose | Duration between Vaccine and Ocular Symptoms (Days) | Diagnosis |
|---|---|---|---|---|---|---|---|---|
| Al Khames Aga et al. [10] | Retrospective cohort | 3 | N.A. | N.A. | BNT162B2 | N.A. | 1 | Eyelid swelling and allergy |
| Mazzatenta et al. [11] | Letter to editor | 5 | 44 63 67 | F M F | BNT162B2 BNT162B2 BNT162B2 | 2nd 2nd 1st | 21–25 21 10 | Eyelid purpuric lesions Eyelid purpuric lesions Eyelid ecchymotic lesions |
| Furer et al. [12] | Case series | 4 | 56 | F | BNT162B2 | 1st | 4 | Herpes zoster ophthalmicus |
| Ravichandran et al. [13] | Case report | 5 | 62 | M | ChAdOx1 | 1st | 21 | Corneal graft rejection |
| Wasser et al. [14] | Case report | 5 | 73 56 | M M | BNT162B2 BNT162B2 | 1st 1st | 14 14 | Corneal graft rejection Corneal graft rejection |
| Crnej et al. [15] | Letter to editor | 5 | 71 | M | BNT162B2 | 1st | 7 | Corneal graft rejection |
| Phylactou et al. [16] | Case report | 5 | 66 83 | F F | BNT162B2 BNT162B2 | 1st 2nd | 7 21 | Corneal graft rejection Corneal graft rejection |
| Mambretti et al. [17] | Case report | 5 | 22 28 | F F | ChAdOx1 ChAdOx1 | N.A. N.A. | 2 2 | Acute macular neuroretinopathy Acute macular neuroretinopathy |
| Bøhler et al. [18] | Letter to editor | 5 | 27 | F | ChAdOx1 | 1st | 2 | Acute macular neuroretinopathy |
| Gabka et al. [19] | Case report | 5 | 20 | F | ChAdOx1 | N.A. | 1 | Acute macular neuroretinopathy |
| Book et al. [20] | Images | 5 | 21 | F | ChAdOx1 | 1st | 3 | Acute macular neuroretinopathy |
| Fowler et al. [21] | Case report | 5 | 33 | M | BNT162B2 | N.A. | 3 | Central serous retinopathy |
| Subramony et al. [22] | Case report | 5 | 22 | F | mRNA-1273 | 2nd | 15 | Retinal detachment |
| Renisi et al. [23] | Case report | 5 | 23 | M | BNT162B2 | 2nd | 14 | Acute anterior uveitis |
| Mudie et al. [24] | Case report | 5 | 43 | F | BNT162B2 | 2nd | 3 | Panuveitis |
| Goyal et al. [25] | Case report | 5 | 34 | M | ChAdOx1 | 2nd | 7 | Multifocal choroiditis |
| Maleki et al. [26] | Case report | 5 | 33 79 | F F | mRNA-1273 BNT162B2 | 2nd 2nd | 10 2 | Acute zonal occult outer retinopathy Arteritic anterior ischemic optic neuropathy |
| Papasavvas et al. [27] | Case report | 5 | 43 | F | BNT162B2 | 2nd | 42 | Reactivation of Vogt-Koyanagi-Harada disease |
| Furer et al. [28] | Case-control study | 3 | N.A. | N.A. | BNT162B2 | 1st/2nd | N.A. | Uveitis |
| Helmchen et al. [29] | Letter to editor | 5 | 40 | F | ChAdOx1 | 1st | 14 | Optic/chiasm neuritis with longitudinal extensive transverse myelitis |
| Reyes-Capo et al. [30] | Case report | 5 | 59 | F | BNT162B2 | N.A. | 2 | Abducens nerve palsy |
| Panovska-Stavridis et al. [31] | Letter to editor | 5 | 29 | F | ChAdOx1 | 1st | 9 | Superior ophthalmic vein thrombosis |
| Bayas et al. [32] | Images | 5 | 55 | F | ChAdOx1 | 1st | 10 | Superior ophthalmic vein thrombosis |
| Castelli et al. [33] | Letter to editor | 5 | 50 | M | ChAdOx1 | 1st | 11 | Cerebral venous sinus thrombosis |
| Wolf et al. [34] | Case series | 4 | 46 | F | ChAdOx1 | 1st | 13 | Cerebral venous sinus thrombosis |
| Suresh et al. [35] | Case report | 5 | 27 | M | ChAdOx1 | 1st | 2 | Cerebral venous sinus thrombosis |
| Dias et al. [36] | Case report | 5 | 47 | F | BNT162B2 | 1st | 6 | Cerebral venous sinus thrombosis |
| See et al. [37] | Case series | 4 | 18–39 | N.A. | Ad26.COV2.S | 1st | 6 | Cerebral venous sinus thrombosis |
| Blauenfeldt et al. [38] | Case report | 5 | 60 | F | ChAdOx1 | 1st | 8 | Acute ischemic stroke and bleeding |
| Santovito et al. [39] | Letter to editor | 5 | middle-aged | M | BNT162B2 | 2nd | 3 | N.A. |
| Kadali et al. [40] | Cross sectional study | 4 | N.A. | N.A. | BNT162B2 | N.A. | 1–42 | N.A. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-K.; Huang, Y.-H. Ocular Manifestations after Receiving COVID-19 Vaccine: A Systematic Review. Vaccines 2021, 9, 1404. https://doi.org/10.3390/vaccines9121404
Lee Y-K, Huang Y-H. Ocular Manifestations after Receiving COVID-19 Vaccine: A Systematic Review. Vaccines. 2021; 9(12):1404. https://doi.org/10.3390/vaccines9121404
Chicago/Turabian StyleLee, Yu-Kuei, and Yi-Hsun Huang. 2021. "Ocular Manifestations after Receiving COVID-19 Vaccine: A Systematic Review" Vaccines 9, no. 12: 1404. https://doi.org/10.3390/vaccines9121404
APA StyleLee, Y. -K., & Huang, Y. -H. (2021). Ocular Manifestations after Receiving COVID-19 Vaccine: A Systematic Review. Vaccines, 9(12), 1404. https://doi.org/10.3390/vaccines9121404