
Unexpectedly High Efficacy of SARS-CoV-2 BNT162b2 Vaccine in Liver versus Kidney Transplant Recipients—Is It Related to Immunosuppression Only?

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Biochemical and Clinical Tests
2.3. Anti-S1 Ab Testing
2.4. Anti-Nucleocapsid Protein Ab Testing
3. Results
Immune Response in SOT Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mono-Therapy | Double-Therapy | Triple-Therapy | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n | MD (IQR) | n | MD (IQR) | n | MD (IQR) | ||
| KTRs | |||||||
| Δ anti-S1 Ab ‡ | n.a. | n.a. | 10 | 55.4 (1619.3) | 30 | 1722.3 (5014.6) | 0.54 * |
| Ab after 2nd dose | n.a. | n.a. | 11 | 99.5 (19,056.5) | 38 | 1434.3 (8823.5) | 0.52 * |
| Ab after 1st dose | n.a. | n.a. | 15 | 49.6 (3753.2) | 37 | 36.0 (5344.7) | 0.79 * |
| LTRs | |||||||
| Δ anti-S1 Ab ‡ | 17 | 1006.7 (4380.2) | 10 | 274.7 (3611.4) | 10 | 1412.5 (7708.6) | 0.76 † |
| Ab after 2nd dose | 20 | 4132.8 (12,768.8) | 14 | 4967.0 (21,904.5) | 12 | 6155.2 (21,904.5) | 0.98 † |
| Ab after 1st dose | 21 | 314.7 (3538.2) | 14 | 15.7 (10,404.8) | 11 | 263.0 (6192.0) | 0.68 † |
| Parameter | Sex | Blood Type | Autoimmune vs. Non-Autoimmune Cause of Liver Transplantation | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | KTRs | LTRs | KTRs | LTRs | LTRs | ||||||||||||||
| Mono-therapy | |||||||||||||||||||
| Variable | M (n = 0) | F (n = 0) | p-value * | M (n = 10) | F (n = 14) | p-value * | A (n = 0) | B (n = 0) | AB (n = 0) | O (n = 0) | p-value † | A (n = 4) | B (n = 8) | AB (n = 0) | O (n = 11) | p-value † | Yes (n = 3) | No (n = 21) | p-value * |
| Δ anti-S1 Ab ‡ | n.a. | n.a. | n.a. | 2370.4 (3826.6) | 590.7 (4684.3) | 0.65 | n.a. | n.a. | n.a. | n.a. | n.a. | 2384.4 (9504.6) | 232 (351.4) | n.a. | 4173.1 (4180.3) | 0.031 | 1236.7 (27,619.1) | 684.35 (4612.2) | 0.34 |
| Ab after 2nd dose | n.a. | n.a. | n.a. | 1593.3 (3372.5) | 7116.2 (28,621.3) | 0.132 | n.a. | n.a. | n.a. | n.a. | n.a. | 6726.9 (21,715.9) | 1210.2 (32,756.8) | n.a. | 3887.1 (4328.1) | 0.53 | 2500 (31,223.5) | 4378.4 (8028.6) | 1 |
| Ab after 1st dose | n.a. | n.a. | n.a. | 137.8 (275.8) | 1034.9 (7418) | 0.180 | n.a. | n.a. | n.a. | n.a. | n.a. | 307.9 (17,748) | 94.3 (7566) | n.a. | 349.8 (3456.4) | 0.59 | 1263 (3604.4) | 257.55 (7499.8) | 1 |
| Double-therapy | |||||||||||||||||||
| Variable | M (n = 6) | F (n = 10) | p-value * | M (n = 4) | F (n = 14) | p-value * | A (n = 4) | B (n = 4) | AB (n = 1) | O (n = 6) | p-value † | A (n = 7) | B (n = 3) | AB (n = 2) | O (n = 5) | p-value † | Yes (n = 8) | No (n = 9) | p-value * |
| Δ anti-S1 Ab ‡ | 1619.3 (17,595.2) | 11.3 (99.5) | 0.30 | 2662.5 (5030.4) | 271.6 (2240.4) | 0.51 | 52.2 (856.9) | 8791.5 (17,617.4) | n.a. | 11.3 (49,526.5) | 0.96 | 869.4 (3231.6) | n.a. | n.a. | 84.8 (125) | 0.088 | 144.15 (193.1) | 2251.6 (5177.7) | 0.46 |
| Ab after 2nd dose | 4969.1 (19,037.8) | 99.5 (846.3) | 0.65 | 1013 (8766.7) | 14160.4 (24,085.9) | 0.53 | 52.3 (4986.1) | 9551.3 (19,037.8) | n.a. | 10560.6 (30,493.3) | 0.61 | 9555.3 (21,904.5) | 8920.9 (33,722.2) | n.a. | 154.2 (414.9) | 0.118 | 402.1 (22,165.6) | 14,160.4 (23,475) | 0.096 |
| Ab after 1st dose | 1470 (8208.8) | 2.7 (1632.3) | 0.24 | 6.9 (3743.2) | 24.5 (14,939.5) | 0.69 | 0.015 (4129.2) | 62.8 (748.2) | n.a. | 2692.8 (9409.9) | 0.21 | 2832.2 (10,404.8) | n.a. | n.a. | 0 (3.5) | 0.088 | 0 (6.9) | 4691.6 (17,884.7) | 0.153 |
| Triple-therapy | |||||||||||||||||||
| Variable | M (n = 22) | F (n = 23) | p-value * | M (n = 1) | F (n = 12) | p-value * | A (n = 15) | B (n = 5) | AB (n = 8) | O (n = 16) | p-value † | A (n = 5) | B (n = 3) | AB (n = 0) | O (n = 5) | p-value † | Yes (n = 10) | No (n = 3) | p-value * |
| Δ anti-S1 Ab ‡ | 3704.2 (8330.1) | 5.5 (2974.3) | 0.094 | n.a. | 1767.3 (7708.6) | n.a. | 347.9 (4256) | 1333.3 (2974.3) | 4009.6 (7024.2) | 0 (5014.6) | 0.64 | 3854.3 (12,117.7) | n.a. | n.a. | 1412.5 (1900.5) | 0.91 | 1767.3 (7708.6) | 385.5 (10,234.5) | 0.91 |
| Ab after 2nd dose | 4587.3 (28,130.5) | 3.7 (3016.5) | 0.012 | n.a. | 7959.3 (15130) | n.a. | 347.9 (13,235.4) | 1.1 (1357.1) | 4454.2 (10,470.6) | 779.9 (8823.5) | 0.20 | 10497.5 (25,602.7) | 296.8 (15,426.8) | n.a. | 2728.3 (5409.6) | 0.29 | 7959.3 (14,321.2) | 385.5 (10,497.5) | 0.36 |
| Ab after 1st dose | 93.4 (17,725.7) | 1.8 (1488.6) | 0.098 | n.a. | 329.8 (6144) | n.a. | 4 (8979.4) | 23.8 (42.2) | 2209.8 (17,725.7) | 33.3 (1045.7) | 0.77 | 20198.3 (39,670.3) | n.a. | n.a. | 48 (874.2) | 0.139 | 635.4 (23,036.8) | 0 (263) | 0.122 |
| Parameter | BMI | Time from Transplantation | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | KTRs | LTRs | KTRs | LTRs | ||||||||
| Variable | n | p-Value * | R | n | p-Value * | R | n | p-Value * | R | n | p-Value * | R |
| Mono-therapy | ||||||||||||
| Δ anti-S1 Ab † | n.a. | n.a. | n.a. | 17 | 0.48 | −0.184 | n.a. | n.a. | n.a. | 17 | 0.40 | 0.217 |
| Ab after 2nd dose | n.a. | n.a. | n.a. | 20 | 0.64 | −0.111 | n.a. | n.a. | n.a. | 20 | 0.37 | 0.213 |
| Ab after 1st dose | n.a. | n.a. | n.a. | 20 | 0.46 | −0.176 | n.a. | n.a. | n.a. | 21 | 0.50 | 0.154 |
| Double-therapy | ||||||||||||
| Δ anti-S1 Ab † | 10 | 0.73 | −0.127 | 10 | 0.83 | −0.079 | 10 | 0.37 | 0.321 | 10 | 0.75 | −0.117 |
| Ab after 2nd dose | 11 | 0.50 | −0.227 | 14 | 0.081 | 0.481 | 11 | 0.049 | 0.603 | 14 | 0.163 | −0.394 |
| Ab after 1st dose | 14 | 0.60 | −0.153 | 13 | 0.62 | 0.153 | 13 | 0.019 | 0.639 | 13 | 0.54 | −0.188 |
| Triple-therapy | ||||||||||||
| Δ anti-S1 Ab † | 30 | 0.48 | −0.134 | 10 | 0.062 | −0.608 | 30 | 0.84 | −0.038 | 10 | 0.51 | −0.238 |
| Ab after 2nd dose | 38 | 0.70 | 0.064 | 12 | 0.059 | −0.559 | 38 | 0.77 | 0.049 | 12 | 0.173 | −0.421 |
| Ab after 1st dose | 36 | 0.46 | 0.126 | 11 | 0.43 | −0.267 | 36 | 0.66 | 0.076 | 11 | 0.84 | 0.067 |
| KTRs | LTRs | p-Value * | |||
|---|---|---|---|---|---|
| Anti-N Ab S/CO | n | MD (IQR) | n | MD (IQR) | |
| After 1st dose | 53 | 0.06 (0.26) | 45 | 0.05 (0.77) | 0.946 |
| After 2nd dose | 25 | 0.0 (0.0) | 21 | 0.0 (0.31) | 0.067 |
References
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Katerinis, I.; Hadaya, K.; Duquesnoy, R.; Ferrari-Lacraz, S.; Meier, S.; van Delden, C.; Martin, P.Y.; Siegrist, C.A.; Villard, J. De novo anti-HLA antibody after pandemic H1N1 and seasonal influenza immunization in kidney transplant recipients. Am. J. Transplant. 2011, 11, 1727–1733. [Google Scholar] [CrossRef]
- Schaffer, S.A.; Husain, S.; Delgado, D.H.; Kavanaugh, L.; Ross, H.J. Impact of adjuvanted H1N1 vaccine on cell-mediated rejection in heart transplant recipients. Am. J. Transplant. 2011, 11, 2751–2754. [Google Scholar] [CrossRef]
- Fairhead, T.; Hendren, E.; Tinckam, K.; Rose, C.; Sherlock, C.H.; Shi, L.; Crowcroft, N.S.; Gubbay, J.B.; Landsberg, D.; Knoll, G.; et al. Poor seroprotection but allosensitization after adjuvanted pandemic influenza H1N1 vaccine in kidney transplant recipients. Transpl. Infect. Dis. 2012, 14, 575–583. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Ou, M.T.; Greenberg, R.S.; Teles, A.T.; Werbel, W.A.; Avery, R.K.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Safety of the First Dose of SARS-CoV-2 Vaccination in Solid Organ Transplant Recipients. Transplantation 2021, 105, e56–e57. [Google Scholar] [CrossRef] [PubMed]
- Phadke, V.K.; Scanlon, N.; Jordan, S.C.; Rouphael, N.G. Immune Responses to SARS-CoV-2 in Solid Organ Transplant Recipients. Curr. Transplant. Rep. 2021, 8, 127–139. [Google Scholar] [CrossRef]
- Eckerle, I.; Rosenberger, K.D.; Zwahlen, M.; Junghanss, T. Serologic vaccination response after solid organ transplantation: A systematic review. PLoS ONE 2013, 8, e56974. [Google Scholar] [CrossRef] [Green Version]
- Korth, J.; Jahn, M.; Dorsch, O.; Anastasiou, O.E.; Sorge-Hädicke, B.; Eisenberger, U.; Gäckler, A.; Dittmer, U.; Witzke, O.; Wilde, B.; et al. Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech). Viruses 2021, 13, 756. [Google Scholar] [CrossRef]
- Rabinowich, L.; Grupper, A.; Baruch, R.; Ben-Yehoyada, M.; Halperin, T.; Turner, D.; Katchman, E.; Levi, S.; Houri, I.; Lubezky, N.; et al. Low immunogenicity to SARS-CoV-2 vaccination among liver transplant recipients. J. Hepatol. 2021, 75, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Rashidi-Alavijeh, J.; Frey, A.; Passenberg, M.; Korth, J.; Zmudzinski, J.; Anastasiou, O.E.; Saner, F.H.; Jahn, M.; Lange, C.M.; Willuweit, K. Humoral Response to SARS-Cov-2 Vaccination in Liver Transplant Recipients-A Single-Center Experience. Vaccines 2021, 9, 738. [Google Scholar] [CrossRef]
- Rusk, D.S.; Strachan, C.C.; Hunter, B.R. Lack of immune response after mRNA vaccination to SARS-CoV-2 in a solid organ transplant patient. J. Med. Virol. 2021, 93, 5623–5625. [Google Scholar] [CrossRef]
- Gobbi, F.; Buonfrate, D.; Moro, L.; Rodari, P.; Piubelli, C.; Caldrer, S.; Riccetti, S.; Sinigaglia, A.; Barzon, L. Antibody Response to the BNT162b2 mRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection. Viruses 2021, 13, 422. [Google Scholar] [CrossRef]
- Rabets, A.; Bila, G.; Grytsko, R.; Samborskyy, M.; Rebets, Y.; Vari, S.G.; Pagneux, Q.; Barras, A.; Boukherroub, R.; Szunerits, S.; et al. The Potential of Developing Pan-Coronaviral Antibodies to Spike Peptides in Convalescent COVID-19 Patients. Arch. Immunol. Ther. Exp. 2021, 69, 5. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Dagan, N.; Cohen, C.; Hernán, M.A.; Lipsitch, M.; Kohane, I.S.; Reis, B.Y.; Balicer, R.D. Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: An observational study. Lancet 2021, 398, 2093–2100. [Google Scholar] [CrossRef]
- Wise, J. Covid-19: UK will offer third vaccine dose to severely immunosuppressed people. Bmj 2021, 374, n2160. [Google Scholar] [CrossRef]
- Wheeler, S.E.; Shurin, G.V.; Yost, M.; Anderson, A.; Pinto, L.; Wells, A.; Shurin, M.R. Differential Antibody Response to mRNA COVID-19 Vaccines in Healthy Subjects. Microbiol. Spectr. 2021, 9, e0034121. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention Advisory Committee on Immunization Practices (ACIP); National Center for Immunization and Respiratory Diseases Centers for Disease Control and Prevention. Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Authorized in the United States. Available online: https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html (accessed on 23 November 2021).
- Kohmer, N.; Westhaus, S.; Rühl, C.; Ciesek, S.; Rabenau, H.F. Brief clinical evaluation of six high-throughput SARS-CoV-2 IgG antibody assays. J. Clin. Virol. 2020, 129, 104480. [Google Scholar] [CrossRef]
- World Health Organisation. Establishment of the WHO International Standard and Reference Panel for Anti-SARS-CoV-2 Antibody. Available online: https://www.who.int/publications/m/item/WHO-BS-2020.2403 (accessed on 23 November 2021).
- Galli, C.; Daghfal, D.; Averhoff, F. Antibody Testing for SARS-CoV-2 Infection, Quantitative Determination, Response to Vaccines and Viral Variability, Abbott Laboratories. Available online: https://www.corelaboratory.abbott/int/en/offerings/segments/infectious-disease/sars-cov-2- (accessed on 2 December 2021).
- Wei, J.; Stoesser, N.; Matthews, P.C.; Ayoubkhani, D.; Studley, R.; Bell, I.; Bell, J.I.; Newton, J.N.; Farrar, J.; Diamond, I.; et al. Antibody responses to SARS-CoV-2 vaccines in 45,965 adults from the general population of the United Kingdom. Nat. Microbiol. 2021, 6, 1140–1149. [Google Scholar] [CrossRef]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Am. J. Transplant. 2021, 21, 2719–2726. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Immunogenicity of a Single Dose of SARS-CoV-2 Messenger RNA Vaccine in Solid Organ Transplant Recipients. JAMA 2021, 325, 1784–1786. [Google Scholar] [CrossRef] [PubMed]
- Cornberg, M.; Eberhardt, C.S. Protected or not protected, that is the question-First data on COVID-19 vaccine responses in patients with NAFLD and liver transplant recipients. J. Hepatol. 2021, 75, 265–266. [Google Scholar] [CrossRef]
- Subesinghe, S.; Bechman, K.; Rutherford, A.I.; Goldblatt, D.; Galloway, J.B. A Systematic Review and Metaanalysis of Antirheumatic Drugs and Vaccine Immunogenicity in Rheumatoid Arthritis. J. Rheumatol. 2018, 45, 733–744. [Google Scholar] [CrossRef] [PubMed]
- Vassilaki, N.; Gargalionis, A.N.; Bletsa, A.; Papamichalopoulos, N.; Kontou, E.; Gkika, M.; Patas, K.; Theodoridis, D.; Manolis, I.; Ioannidis, A.; et al. Impact of Age and Sex on Antibody Response Following the Second Dose of COVID-19 BNT162b2 mRNA Vaccine in Greek Healthcare Workers. Microorganisms 2021, 9, 1725. [Google Scholar] [CrossRef] [PubMed]
- Deepak, P.; Kim, W.; Paley, M.A.; Yang, M.; Carvidi, A.B.; Demissie, E.G.; El-Qunni, A.A.; Haile, A.; Huang, K.; Kinnett, B.; et al. Effect of Immunosuppression on the Immunogenicity of mRNA Vaccines to SARS-CoV-2: A Prospective Cohort Study. Ann. Intern. Med. 2021, 174, 1572–1585. [Google Scholar] [CrossRef] [PubMed]
- Jalkanen, P.; Kolehmainen, P.; Häkkinen, H.K.; Huttunen, M.; Tähtinen, P.A.; Lundberg, R.; Maljanen, S.; Reinholm, A.; Tauriainen, S.; Pakkanen, S.H.; et al. COVID-19 mRNA vaccine induced antibody responses against three SARS-CoV-2 variants. Nat. Commun. 2021, 12, 3991. [Google Scholar] [CrossRef]
- Krause, P.R.; Fleming, T.R.; Peto, R.; Longini, I.M.; Figueroa, J.P.; Sterne, J.A.C.; Cravioto, A.; Rees, H.; Higgins, J.P.T.; Boutron, I.; et al. Considerations in boosting COVID-19 vaccine immune responses. Lancet 2021, 398, 1377–1380. [Google Scholar] [CrossRef]
- Masset, C.; Kerleau, C.; Garandeau, C.; Ville, S.; Cantarovich, D.; Hourmant, M.; Kervella, D.; Houzet, A.; Guillot-Gueguen, C.; Guihard, I.; et al. A third injection of the BNT162b2 mRNA COVID-19 vaccine in kidney transplant recipients improves the humoral immune response. Kidney Int. 2021, 100, 1132–1135. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 Vaccine Booster against Covid-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Werbel, W.A.; Boyarsky, B.J.; Ou, M.T.; Massie, A.B.; Tobian, A.A.R.; Garonzik-Wang, J.M.; Segev, D.L. Safety and Immunogenicity of a Third Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Case Series. Ann. Intern. Med. 2021, 174, 1330–1332. [Google Scholar] [CrossRef] [PubMed]
- Del Bello, A.; Abravanel, F.; Marion, O.; Couat, C.; Esposito, L.; Lavayssière, L.; Izopet, J.; Kamar, N. Efficiency of a boost with a third dose of anti-SARS-CoV-2 messenger RNA-based vaccines in solid organ transplant recipients. Am. J. Transplant. 2021. [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- Yan, S.; Sun, H.; Bu, X.; Wan, G. New Strategy for COVID-19: An Evolutionary Role for RGD Motif in SARS-CoV-2 and Potential Inhibitors for Virus Infection. Front. Pharmacol. 2020, 11, 912. [Google Scholar] [CrossRef] [PubMed]
- Rivas-Santiago, B.; Jacobo-Delgado, Y.; Rodriguez-Carlos, A. Are Host Defense Peptides and Their Derivatives Ready to be Part of the Treatment of the Next Coronavirus Pandemic? Arch. Immunol. Ther. Exp. 2021, 69, 25. [Google Scholar] [CrossRef]





| Characteristics | KTRs (n = 61) | LTRs (n = 55) |
|---|---|---|
| Mean age (SD), years | 54.4 (12.9) | 58.4 (13.3) |
| Median age (Range), years | ||
| Female | 61 (31–77) | 60 (26–82) |
| Male | 53.5 (18–71) | 65 (50–71) |
| Gender, n (%) | ||
| Female | 33 (54.1) | 21 (43.6) |
| Male | 28 (45.9) | 44 (80) |
| Mean BMI (SD), kg/m2 | 25.1 (3.9) | 25.7 (4.0) |
| Mean time since transplantation (SD), years | 13 (7.1) | 14.8 (3.8) |
| History of COVID-19 infection, n (%) | ||
| Infection confirmed by PCR | 5 (8.2) | 5 (9.1) |
| Hospitalization due to COVID-19 | 3 (60) † | 1 (20) † |
| Symptoms: | ||
| Fever >38 °C | 3 (60) | 4 (80) |
| Loss of smell and/or taste | 0 (0) | 3 (60) |
| Dyspnea | 2 (40) | 2 (40) |
| Sore throat | 1 (20) | 1 (20) |
| Myalgia | 2 (40) | 3 (60) |
| Cough | 2 (40) | 2 (40) |
| Pneumoniae | 2 (40) | 2 (40) |
| Tachycardia/arrythmia | 0 | 3 (40) |
| Diarrhea | 1 (20) | 3 (40) |
| Other | 1 (20) | 2 (40) |
| Induction therapy, n (%) | ||
| Anti-thymocyte globulin | 0 | 0 |
| Anti-interleukin-2 receptor | 0 | 30 (54.5) |
| Immunosuppression, n (%) | ||
| Steroids | 52 (85.2) | 20 (36.4) |
| Mycophenolate mofetil | 47 (77.1) | 16 (29.1) |
| Azathioprine | 7 (11.5) | 5 (9.1) |
| Cyclosporine | 25 (41) | 11 (20) |
| Tacrolimus | 33 (54.1) | 43 (78.2) |
| Sirolimus | 2 (3.3) | 2 (3.6) |
| Everolimus | 1 (1.6) | 2 (3.6) |
| Immunosuppression, n (%) | ||
| Mono-therapy (CNI/MMF) | 0 | 24 (43.6) |
| Dual-therapy (CNI + GKS/MMF/AZA/mTORI) | 16 (26.3) | 18 (32.7) |
| Triple-therapy (CNI/mTORi +GKS + MMF/AZA) | 45 (73.8) | 13 (23.6) |
| Mean laboratory data (SD) | ||
| Serum creatinine, mg/dL | 1.4 (0.5) | 1 (0.3) |
| eGFR, mL/min * 1.73 m2 | 51.3 (16.8) | 58.4 (19.1) |
| ALT, IU/L | 18.6 (10.5) | 25.1 (17.7) |
| AST, IU/L | n.a. | 26.4 (15.4) |
| GGTP, IU/L | n.a. | 70 (78.3) |
| ALP, IU/L | n.a. | 109.4 (65.4) |
| Bil, mg/dL | n.a. | 1.3 (2.4) |
| Complement component | ||
| C3 G/L | 1.2 (0.3) | 1.3 (0.3) |
| C4 G/L | 0.2 (0.1) | 0.2 (0.1) |
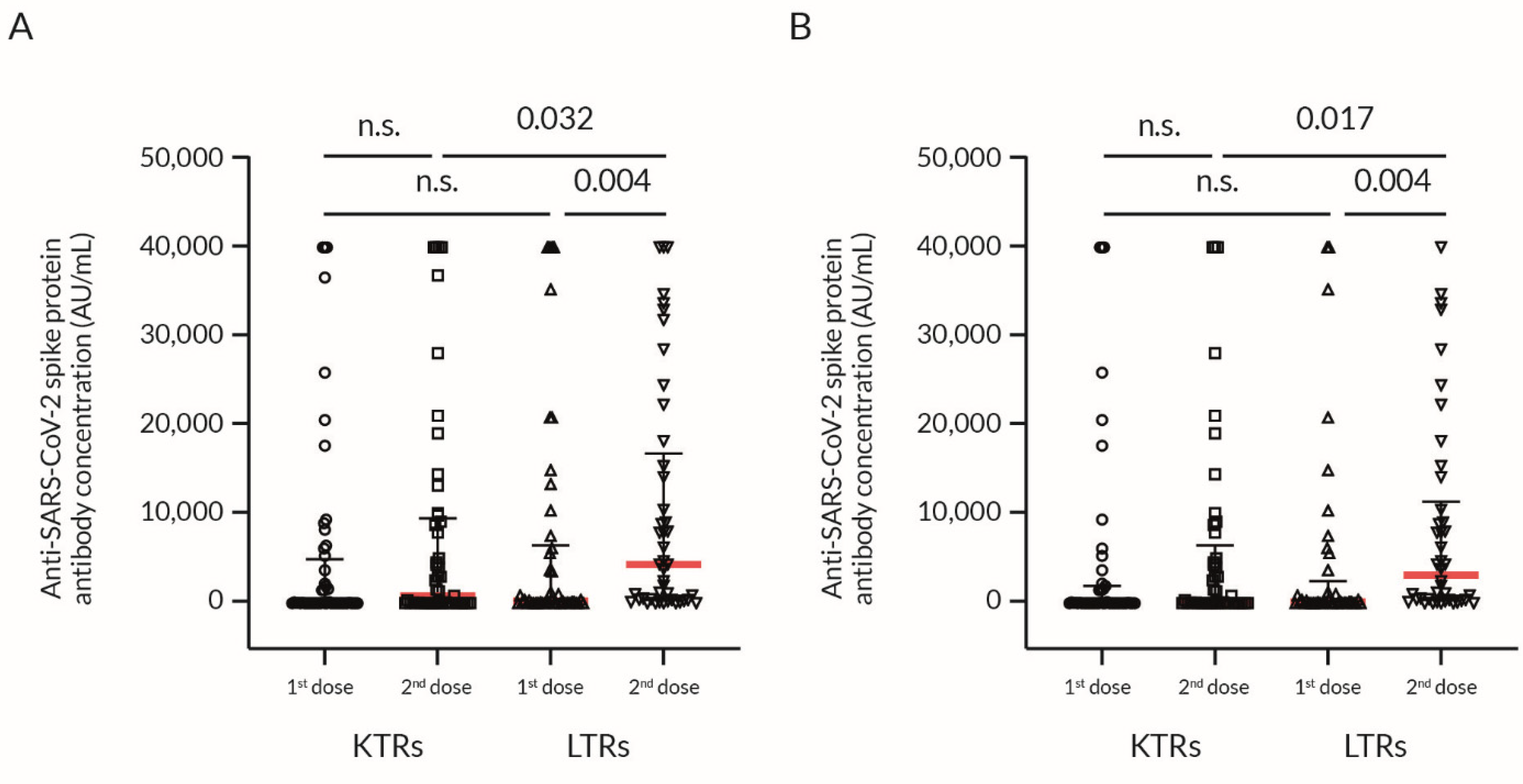
| Parameter | KTRs + LTRs (n) | MD (IQR) | KTRs (n) | MD (IQR) | LTRs (n) | MD (IQR) | p-Value * |
|---|---|---|---|---|---|---|---|
| All patients: positive history of COVID-19 disease (confirmed by PCR test) included | |||||||
| Δ anti-S1 Ab † | 76 | 725.4 (4434.4) | 40 | 604 (4635.6) | 36 | 730.1 (4384) | 0.84 |
| Ab after the 2nd dose | 94 | 2238.2 (10,475.2) | 49 | 860 (9198.9) | 45 | 4351 (15,024.7) | 0.032 |
| Ab after the 1st dose | 98 | 73.2 (5639.9) | 52 | 39.1 (4549) | 46 | 231.7 (6192) | 0.197 |
| Patients without a positive history of COVID-19 disease | |||||||
| Δ anti-S1 Ab † | 69 | 402.1 (4178) | 36 | 55.4 (4512.1) | 33 | 869.4 (4037) | 0.477 |
| Ab after the 2nd dose | 87 | 1210.2 (8910.5) | 45 | 99.5 (5077.6) | 42 | 3193.55 (10,112) | 0.017 |
| Ab after the 1st dose | 88 | 48.8 (1788.8) | 47 | 23.8 (1945.3) | 41 | 148 (1263.3) | 0.266 |
| Parameter | All Patients | KTRs | LTRs | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | p-Value * | R | n | p-Value * | R | n | p-Value * | R | |
| Correlations with Δ anti-S1 Ab † | |||||||||
| Anti-N Ab ‡, S/CO | 75 | 0.103 | 0.190 | 40 | 0.43 | 0.006 | 35 | 0.64 | −0.082 |
| Age, years | 76 | 0.005 | −0.317 | 40 | 0.004 | −0.447 | 36 | 0.31 | −0.174 |
| BMI, kg/m2 | 76 | 0.071 | −0.208 | 40 | 0.29 | −0.170 | 36 | 0.148 | −0.246 |
| Time from transplantation, years | 76 | 0.87 | 0.020 | 40 | 0.99 | 0.002 | 36 | 0.80 | −0.043 |
| CSA | |||||||||
| daily dose, mg | 21 | 0.70 | 0.089 | 13 | 0.74 | 0.100 | 8 | 0.47 | 0.299 |
| Concentration ‡, ng/mL | 21 | 0.48 | −0.163 | 13 | 0.61 | −0.156 | 8 | 0.74 | −0.143 |
| TAC | |||||||||
| daily dose, mg | 53 | 0.22 | 0.171 | 25 | 0.50 | 0.142 | 28 | 0.37 | 0.200 |
| Concentration ‡, ng/mL | 52 | 0.30 | −0.148 | 24 | 0.46 | −0.158 | 28 | 0.23 | −0.233 |
| Graft function | |||||||||
| Cr, mg/dL | 65 | 0.26 | −0.141 | 37 | 0.59 | −0.090 | 28 | 0.145 | −0.282 |
| GFR, mL/min × 1.73 m2 | 66 | 0.036 | 0.259 | 37 | 0.102 | 0.273 | 29 | 0.35 | 0.179 |
| AST, IU/L | 67 | 0.41 | 0.102 | 34 | 0.82 | 0.039 | 33 | 0.124 | 0.273 |
| ALT, IU/L | 37 | 0.56 | 0.100 | 5 | 0.39 | −0.500 | 32 | 0.32 | 0.183 |
| ALP, IU/L | 35 | 0.41 | 0.144 | 4 | 0.37 | −0.632 | 31 | 0.31 | 0.189 |
| Bil, mg/dL | 35 | 0.51 | −0.115 | 3 | n.a. | n.a. | 32 | 0.79 | −0.050 |
| GGTP, IU/L | 30 | 0.115 | −0.294 | 1 | n.a. | n.a. | 29 | 0.188 | −0.252 |
| Complement component, G/L | |||||||||
| C3 | 56 | 0.54 | −0.084 | 30 | 0.96 | 0.010 | 26 | 0.25 | −0.235 |
| C4 | 55 | 0.26 | −0.155 | 30 | 0.52 | −0.123 | 25 | 0.43 | −0.166 |
| Correlations with anti-S1 Ab after the 2nd dose | |||||||||
| Anti-N Ab §, S/CO | 35 | 0.040 | 0.409 | 25 | 0.106 | 0.331 | 20 | 0.41 | 0.194 |
| Age, years | 94 | 0.014 | −0.253 | 49 | <0.001 | −0.467 | 45 | 0.62 | −0.076 |
| BMI, kg/m2 | 94 | 0.74 | 0.034 | 49 | 0.77 | 0.042 | 45 | 0.96 | 0.008 |
| Time from transplantation, years | 94 | 0.32 | 0.104 | 49 | 0.25 | 0.169 | 45 | 0.25 | −0.174 |
| CSA | |||||||||
| daily dose, mg | 30 | 0.27 | 0.209 | 20 | 0.062 | 0.425 | 10 | 0.45 | 0.271 |
| Concentration §, ng/mL | 28 | 0.81 | 0.049 | 20 | 0.63 | 0.114 | 8 | 0.46 | 0.310 |
| TAC | |||||||||
| daily dose, mg | 62 | 0.119 | 0.200 | 27 | 0.69 | 0.080 | 35 | 0.040 | 0.349 |
| Concentration §, ng/mL | 57 | 0.180 | −0.180 | 26 | 0.87 | 0.033 | 31 | 0.162 | −0.257 |
| Correlations with anti-S1 Ab after the 1st dose | |||||||||
| Anti-N Ab ‡, S/CO | 97 | <0.001 | 0.671 | 52 | <0.001 | 0.632 | 45 | <0.001 | 0.711 |
| Age, years | 97 | <0.001 | −0.346 | 52 | <0.001 | −0.462 | 45 | 0.139 | −0.224 |
| BMI, kg/m2 | 94 | 0.86 | 0.018 | 50 | 0.51 | 0.096 | 44 | 0.86 | −0.027 |
| Time from transplantation, years | 94 | 0.181 | 0.139 | 49 | 0.23 | 0.173 | 45 | 0.96 | −0.007 |
| CSA | |||||||||
| daily dose, mg | 27 | 0.188 | 0.261 | 18 | 0.33 | 0.245 | 9 | 0.24 | 0.434 |
| Concentration ‡, ng/mL | 27 | 0.088 | 0.335 | 18 | 0.28 | 0.270 | 9 | 0.081 | 0.610 |
| TAC | |||||||||
| daily dose, mg | 67 | 0.057 | 0.234 | 31 | 0.163 | 0.257 | 36 | 0.26 | 0.194 |
| Concentration ‡, ng/mL | 65 | 0.56 | −0.074 | 29 | 0.68 | −0.080 | 36 | 0.38 | −0.152 |
| Parameter | All Patients | KTRs | LTRs | ||||
|---|---|---|---|---|---|---|---|
| n | MD (IQR) | n | MD (IQR) | n | MD (IQR) | p-Value * | |
| Comparison to Δ anti-S1 Ab † | |||||||
| Gender | |||||||
| M | 30 | 2509 (7408.8) | 21 | 3398.7 (9104.1) | 9 | 1006.7 (3826.6) | 0.86 |
| F | 46 | 251.5 (3476.8) | 19 | 10.4 (2931.4) | 27 | 590.7 (4612.2) | 0.35 |
| Blood type | |||||||
| A | 29 | 402.1 (4177.5) | 16 | 55 (3164.8) | 13 | 869.4 (7567.6) | 0.32 |
| B | 13 | 351.4 (2974.3) | 5 | 1333.3 (2974.3) | 8 | 291.7 (2769.9) | 0.88 |
| AB | 8 | 1485.7 (6572.6) | 6 | 3060.5 (8275.5) | 2 | −389.6 (779.1) | 0.094 |
| O | 24 | 1147.2 (4813.4) | 11 | 0 (6878.2) | 13 | 1236.7 (3348.5) | 0.64 |
| Comparison to Ab after the 2nd dose | |||||||
| Gender | |||||||
| M | 37 | 2583.7 (9723.5) | 25 | 4587.3 (19,037.8) | 12 | 1128.5 (3824) | 0.26 |
| F | 57 | 1511.5 (10,487.1) | 24 | 12.1 (2996.3) | 33 | 7928 (24,050.8) | <0.001 |
| Comparison to Ab after the 1st dose | |||||||
| Gender | |||||||
| M | 36 | 107.9 (7375.3) | 24 | 119.7 (9196.1) | 12 | 81.2 (304.5) | 0.45 |
| F | 62 | 68.3 (3753.2) | 28 | 2.7 (1560.5) | 34 | 390.7 (10,404.8) | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nazaruk, P.; Monticolo, M.; Jędrzejczak, A.M.; Krata, N.; Moszczuk, B.; Sańko-Resmer, J.; Pilecki, T.; Urbanowicz, A.; Florczak, M.; Pączek, L.; et al. Unexpectedly High Efficacy of SARS-CoV-2 BNT162b2 Vaccine in Liver versus Kidney Transplant Recipients—Is It Related to Immunosuppression Only? Vaccines 2021, 9, 1454. https://doi.org/10.3390/vaccines9121454
Nazaruk P, Monticolo M, Jędrzejczak AM, Krata N, Moszczuk B, Sańko-Resmer J, Pilecki T, Urbanowicz A, Florczak M, Pączek L, et al. Unexpectedly High Efficacy of SARS-CoV-2 BNT162b2 Vaccine in Liver versus Kidney Transplant Recipients—Is It Related to Immunosuppression Only? Vaccines. 2021; 9(12):1454. https://doi.org/10.3390/vaccines9121454
Chicago/Turabian StyleNazaruk, Paulina, Marta Monticolo, Anna Maria Jędrzejczak, Natalia Krata, Barbara Moszczuk, Joanna Sańko-Resmer, Tomasz Pilecki, Arkadiusz Urbanowicz, Michał Florczak, Leszek Pączek, and et al. 2021. "Unexpectedly High Efficacy of SARS-CoV-2 BNT162b2 Vaccine in Liver versus Kidney Transplant Recipients—Is It Related to Immunosuppression Only?" Vaccines 9, no. 12: 1454. https://doi.org/10.3390/vaccines9121454
APA StyleNazaruk, P., Monticolo, M., Jędrzejczak, A. M., Krata, N., Moszczuk, B., Sańko-Resmer, J., Pilecki, T., Urbanowicz, A., Florczak, M., Pączek, L., Foroncewicz, B., & Mucha, K. (2021). Unexpectedly High Efficacy of SARS-CoV-2 BNT162b2 Vaccine in Liver versus Kidney Transplant Recipients—Is It Related to Immunosuppression Only? Vaccines, 9(12), 1454. https://doi.org/10.3390/vaccines9121454