
Month of Influenza Virus Vaccination Influences Antibody Responses in Children and Adults

 , , and
, , and 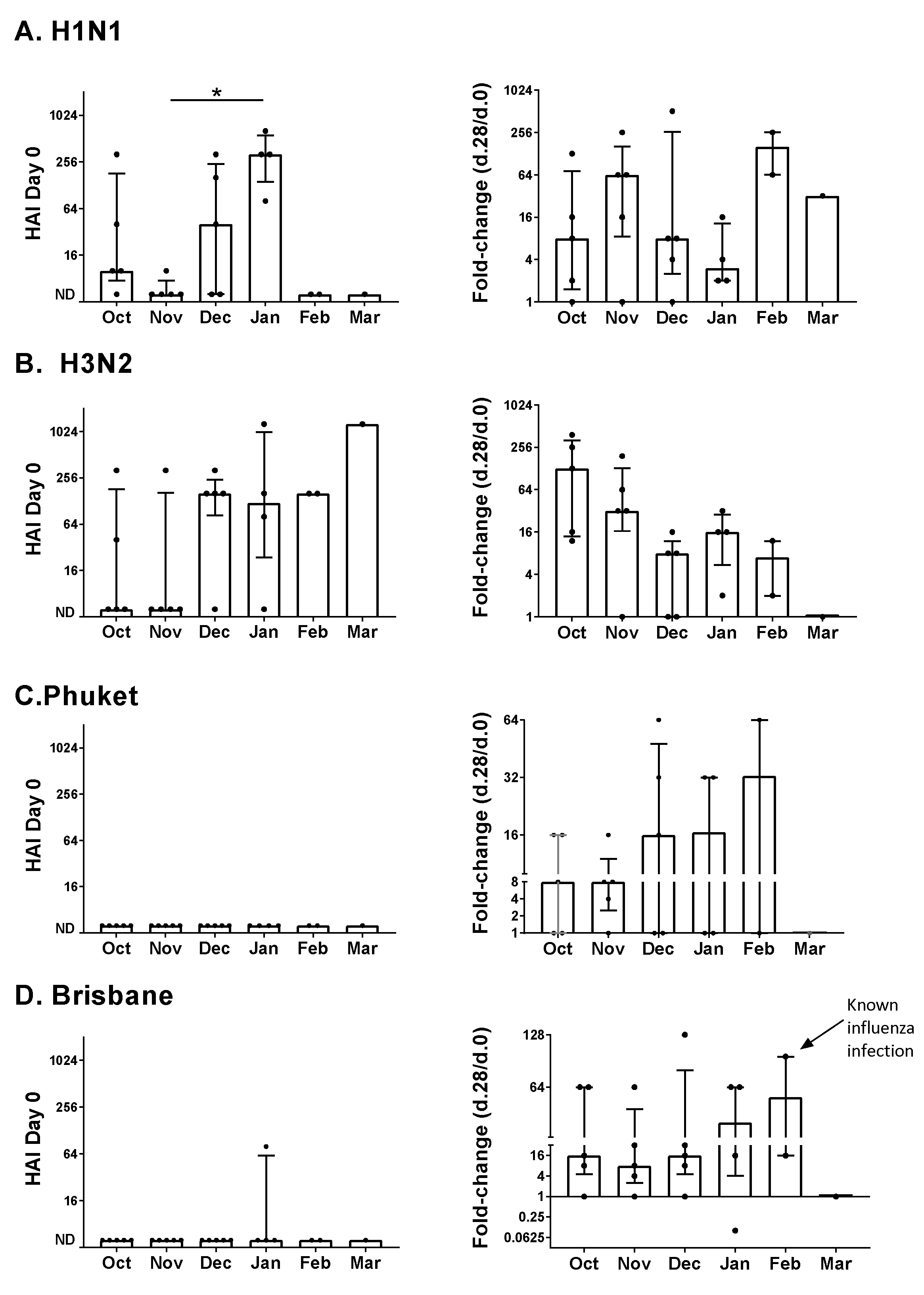{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. 2016–2017 Study
2.2. 2017–2018 Study
2.3. HAI Assays
2.4. Statistical Analyses
3. Results
3.1. 2016–2017 Vaccine Study
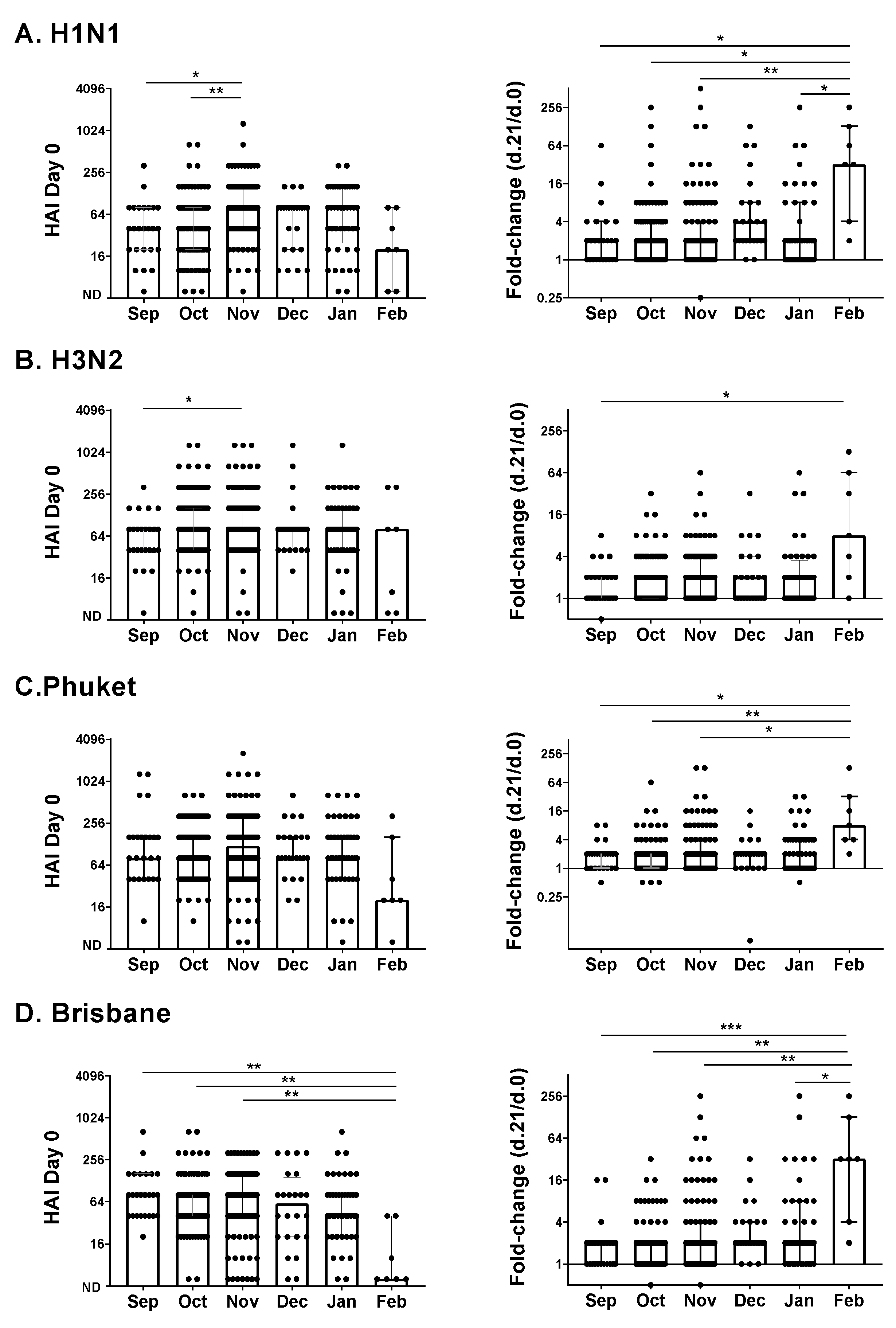
3.2. 2017–2018 Vaccine Study
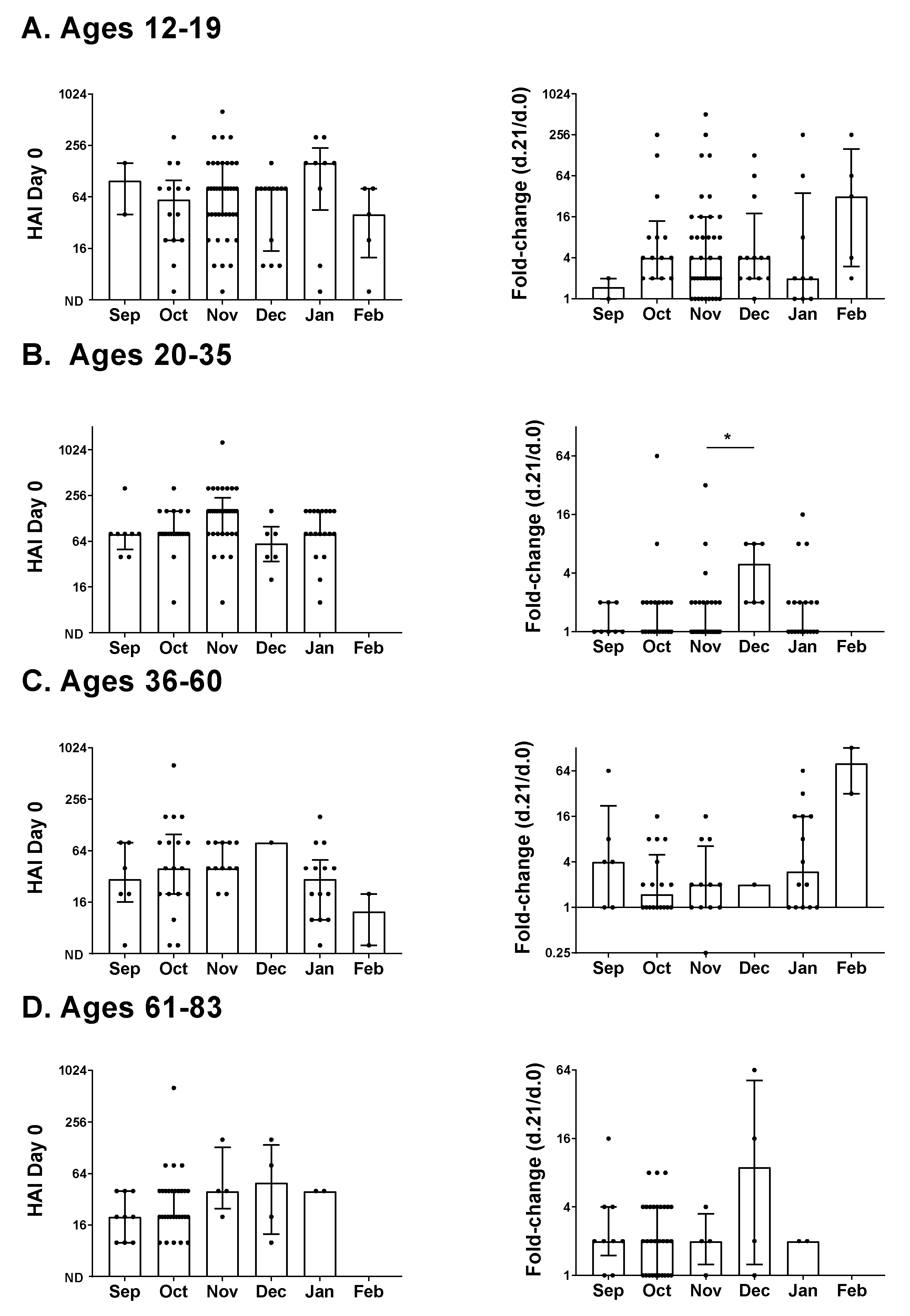
3.3. Age and Responses to the Influenza Vaccine
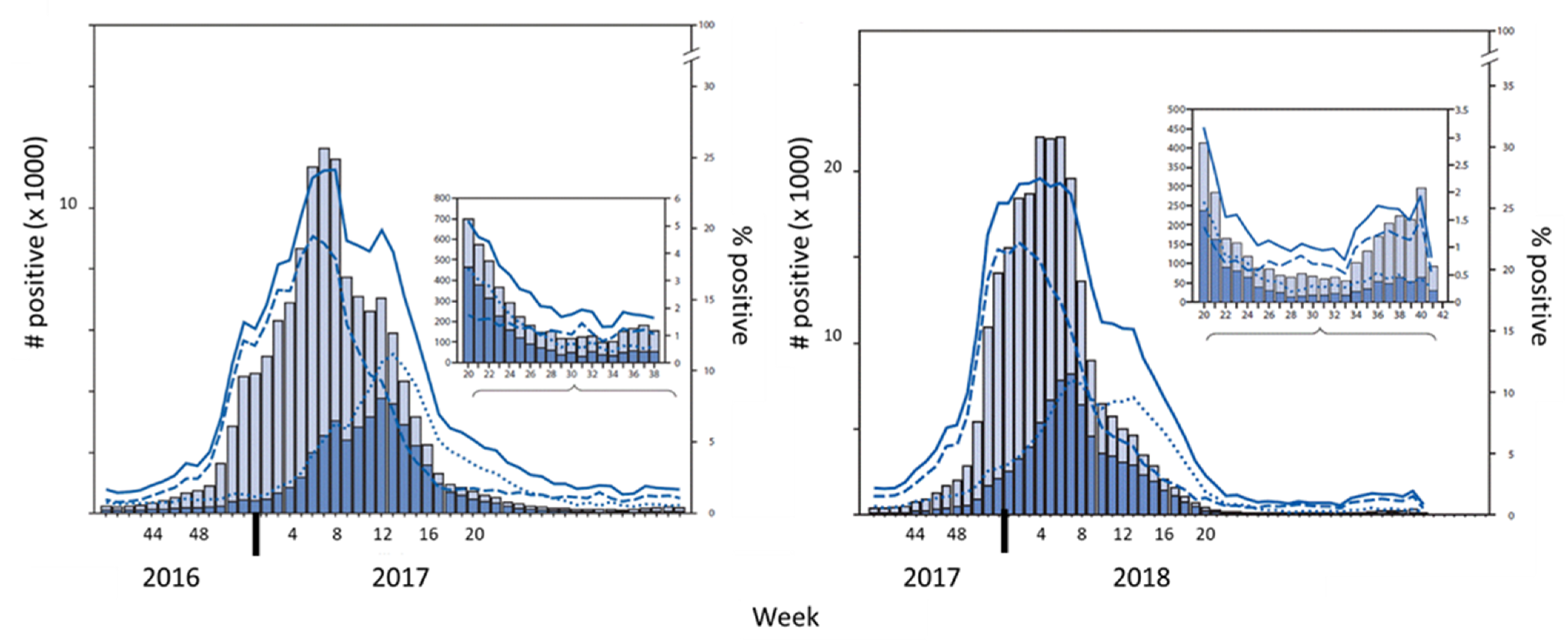
3.4. Circulating Influenza Viruses during the 2016–2017 and 2017–2018 Influenza Seasons
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HA | Hemagglutinin |
| HAI | hemagglutination inhibition |
| IM | Intramuscular |
| RBC | red blood cells |
References
- Erbelding, E.J.; Post, D.J.; Stemmy, E.J.; Roberts, P.C.; Augustine, A.D.; Ferguson, S.; Paules, C.I.; Graham, B.S.; Fauci, A.S. A Universal Influenza Vaccine: The Strategic Plan for the National Institute of Allergy and Infectious Diseases. J. Infect. Dis. 2018, 218, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Lopez, C.E.; Legge, K.L. Influenza A Virus Vaccination: Immunity, Protection, and Recent Advances Toward A Universal Vaccine. Vaccines 2020, 8, 434. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Penkert, R.R.; Jones, B.G.; Sealy, R.E.; Surman, S.L.; Sun, Y.; Tang, L.; DeBeauchamp, J.; Webb, A.; Richardson, J.; et al. Baseline Serum Vitamin A and D Levels Determine Benefit of Oral Vitamin A&D Supplements to Humoral Immune Responses Following Pediatric Influenza Vaccination. Viruses 2019, 11, 907. [Google Scholar] [CrossRef] [Green Version]
- De Bourcy, C.F.; Angel, C.J.; Vollmers, C.; Dekker, C.L.; Davis, M.M.; Quake, S.R. Phylogenetic analysis of the human antibody repertoire reveals quantitative signatures of immune senescence and aging. Proc. Natl. Acad. Sci. USA 2017, 114, 1105–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanton, L.; Alabi, N.; Mustaquim, D.; Taylor, C.; Kniss, K.; Kramer, N.; Budd, A.; Garg, S.; Cummings, C.N.; Chung, J.; et al. Update: Influenza Activity in the United States During the 2016-17 Season and Composition of the 2017-18 Influenza Vaccine. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 668–676. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.J.; Davis, C.T.; Elal, A.I.A.; Alabi, N.; Azziz-Baumgartner, E.; Barnes, J.; Blanton, L.; Brammer, L.; Budd, A.P.; Burns, E.; et al. Update: Influenza activity-United States and worldwide, May 20–October 13, 2018. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1178–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayward, A.C.; Fragaszy, E.B.; Bermingham, A.; Wang, L.; Copas, A.; Edmunds, W.J.; Ferguson, N.; Goonetilleke, N.; Harvey, G.; Kovar, J.; et al. Comparative community burden and severity of seasonal and pandemic influenza: Results of the Flu Watch cohort study. Lancet Respir. Med. 2014, 2, 445–454. [Google Scholar] [CrossRef]
- Furuya-Kanamori, L.; Yakob, L. Heterogeneous and Dynamic Prevalence of Asymptomatic Influenza Virus Infections. Emerg. Infect. Dis. 2018, 24, 951. [Google Scholar] [CrossRef] [PubMed]
- Scaggs Huang, F.; Bernstein, D.I.; Slobod, K.S.; Portner, A.; Takimoto, T.; Russell, C.J.; Meagher, M.; Jones, B.G.; Sealy, R.E.; Coleclough, C.; et al. Safety and immunogenicity of an intranasal sendai virus-based vaccine for human parainfluenza virus type I and respiratory syncytial virus (SeVRSV) in adults. Hum. Vaccines Immunother 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Chesney, R.W. Vitamin D and The Magic Mountain: The anti-infectious role of the vitamin. J. Pediatr. 2010, 156, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Penkert, R.R.; Patel, N.; Webby, R.J.; Ross, T.M.; Hurwitz, J.L. Month of Influenza Virus Vaccination Influences Antibody Responses in Children and Adults. Vaccines 2021, 9, 68. https://doi.org/10.3390/vaccines9020068
Penkert RR, Patel N, Webby RJ, Ross TM, Hurwitz JL. Month of Influenza Virus Vaccination Influences Antibody Responses in Children and Adults. Vaccines. 2021; 9(2):68. https://doi.org/10.3390/vaccines9020068
Chicago/Turabian StylePenkert, Rhiannon R., Nehali Patel, Richard J. Webby, Ted M. Ross, and Julia L. Hurwitz. 2021. "Month of Influenza Virus Vaccination Influences Antibody Responses in Children and Adults" Vaccines 9, no. 2: 68. https://doi.org/10.3390/vaccines9020068
APA StylePenkert, R. R., Patel, N., Webby, R. J., Ross, T. M., & Hurwitz, J. L. (2021). Month of Influenza Virus Vaccination Influences Antibody Responses in Children and Adults. Vaccines, 9(2), 68. https://doi.org/10.3390/vaccines9020068