1. Introduction
As of 8 April 2021, Austria had 568,916 registered cases of COVID-19 with 9586 deaths, while 525,682 people have fully recovered and 2516 people are currently hospitalized, with 578 being treated in intensive units. As of 29 March 2021, a total of 1,569,200 vaccine doses have been administered [
1]. Austria was one of the first countries reporting COVID-19 cases, and complete lockdown measures were implemented in Austria for six weeks between 16 March and 25 April 2020, and again in December 2020 through to 8 February 2021. The current uptake in Austria stands at 20.96 doses of vaccine for every 100 people, which equals vaccination participation of 20% and ranks the country far behind states like Israel (117.72 doses/100 inhabitants), the United Kingdom (55.0), Hungary (38.49), and Morocco (22.89) [
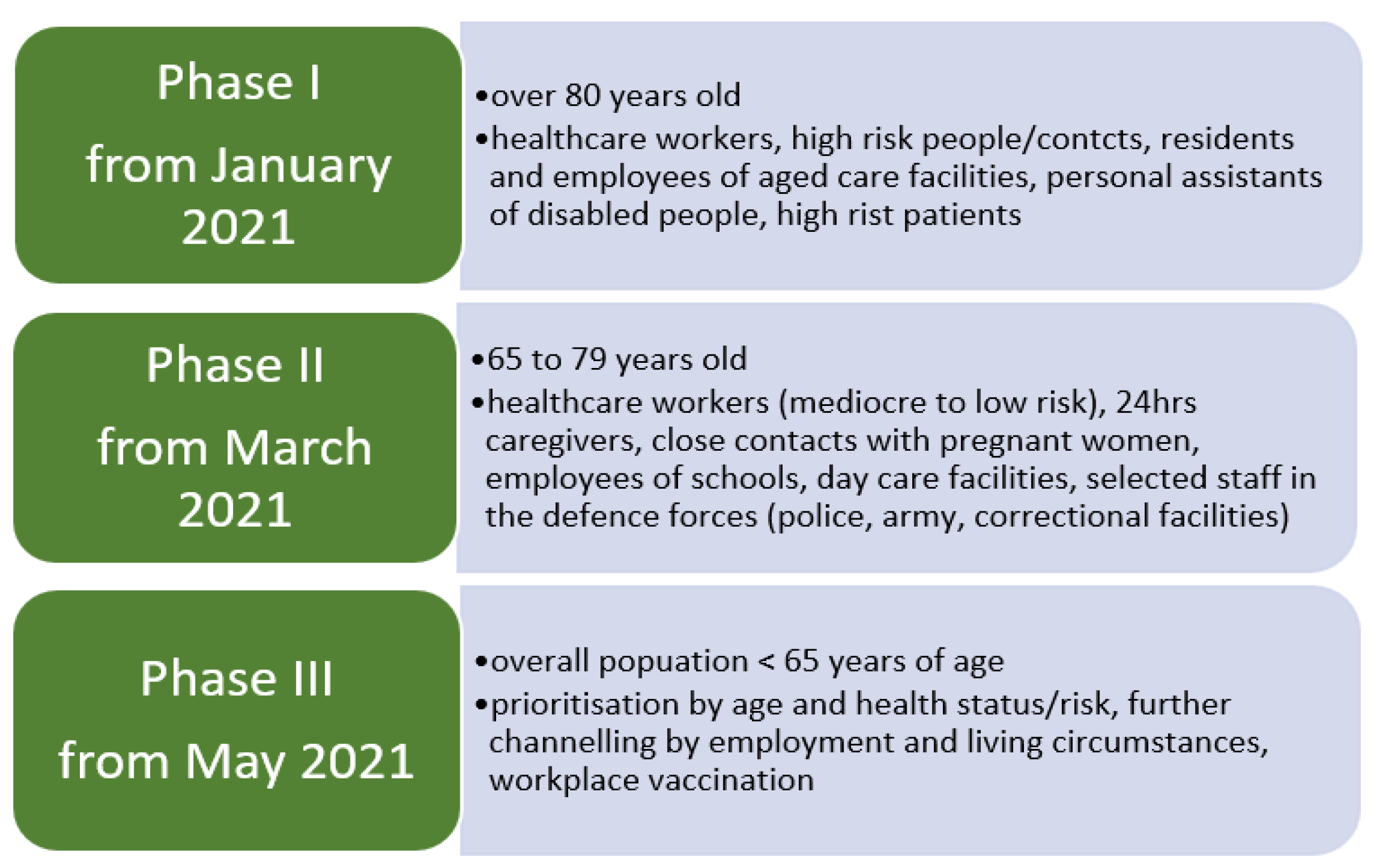
2]. As the situations have not shown significant progress, Austria is committed to developing an adequate vaccination strategy and course of action (see
Figure 1) to improve its vaccination uptake to protect its population in the best way possible. However, it is not yet possible to define an ultimate procedure for distributing and administering the COVID-19 vaccination. Vaccinations are one of the most important, influential, and preventive measures in medicine, and significant medical success could be achieved through vaccinations and countries have developed free vaccination programs to enable access to vaccinations that are important for public health. Therefore, Austria has included the new corona vaccination in the regulation on recommended vaccinations in Austria [
3].
Experience of disease outbreaks over the past two decades, like SARS and influenza in 2009, Ebola3 in 2014, and the Zika virus, has substantiated rapid progress towards vaccines for COVID-19 [
4], and as it has become evident that an effective vaccine is required to bring the disease under control and prevent future outbreaks and global lockdowns. Moreover, introducing sensitive and robust disease severity measures encompassing the entire spectrum from mild to severe illness can support direct evidence-based diagnostic and therapeutic decisions [
5]. Our focus on vaccine-related attitudes and intentions is essential because experts agree that having enough people vaccinate against COVID-19 is key to stemming the pandemic [
6]. More broadly, negative attitudes towards vaccination in general and reduced vaccine uptake are an increasing public health concern and a seemingly emerging phenomenon, particularly in industrialized countries [
7]. In that matter, public health authorities aim for global coverage of the COVID-19 vaccine; however, vaccine uptake and acceptability require the public to place their trust in global health as well as in the country’s response to the pandemic and positive sentiment towards the vaccine is crucial for high coverage and clear guidelines and standard operating procedures need to be established [
5,
8]. The growing number of communities and individuals refusing or delaying recommended vaccinations despite their availability poses a severe threat to global health. The World Health Organization (WHO) has identified vaccine hesitancy as one of the top ten global health threats in 2020, and global concerns are growing [
9,
10]. Vaccine hesitancy is a complex multifactorial problem with several determinants: vaccine efficacy, convenience, confidence, and trust in healthcare professionals. It is the main reason for low vaccination coverages [
11,
12,
13]. Further, the accelerated pace of vaccine development has increased public anxiety and could adversely influence its acceptance [
14].
Numerous studies have addressed vaccine hesitancy and its change in response to the COVID-19 pandemic [
15]. There is only a little research on vaccine hesitancy in Austria to date, and further investigation into its contributing factors is necessary [
16]. In Austria, physicians and family doctors are the most trusted source of health information, and their recommendations can substantially impact people’s attitudes towards vaccines [
16]. This study aimed to understand better the factors contributing to vaccine reluctance in Austria to counteract and overcome obstacles that create uncertainty and skepticism and provide transparent and fact-based public health strategies to enhance immunization coverage. The objectives were to elicit the perceived efficacy of the new COVID-19 vaccine through research question 1: “Vaccination is a way of preventing and controlling COVID-19” (1), to elicit the acceptability and social approval of the rapid development of the new COVID-19 vaccine (2), to determine the willingness to get the COVID-19 vaccine (3), and to investigate influencing factors of COVID-19 vaccination acceptance among the Austrian population (4). We present findings from a survey of the likelihood of vaccine acceptance from a sample of 1350 respondents in Austria.
2. Methods
2.1. Survey Questionnaire and Participants
An anonymous cross-sectional study or transverse survey to assess the acceptability and factors influencing the attitude towards the COVID-19 vaccination in Austria was conducted. An online questionnaire in German was performed using the umfrageonline.com tool. The survey was modified from a questionnaire to be published in Malaysia. It comprised fifteen questions segmented into two parts, part A and part B. Part A contained nine questions about the sociodemographic profile of the participants, including age, gender, citizenship, marital status, annual household income, residential location setting (urban or rural), and educational level. Part B had six questions addressing acceptance, factors influencing the approval, and uptake of the COVID-19 vaccine. The link was distributed with an invitation to companies from various industries, e.g., the care sector, the business, the administration, the pedagogical sectors, non-profit organizations, nursing homes, and sports clubs.
Moreover, it was posted on social media and business platforms. A snowball sampling method was utilized. The survey was open from 18 February 2021 until 17 March 2021. The data collection began between Phase 1 and Phase 2 of the dissemination of the COVID-19 vaccination. Hence, our data span the early phase of the vaccination period and between lockdowns. The University Research Board approved the study. Participation in the survey was entirely voluntary, and participants gave their informed consent before answering the first question. No exclusion or inclusion criteria were defined, though the survey aimed to target people living in Austria to represent the country’s attitude. The primary measure of interest was the willingness of the participants to accept the vaccine as soon as it becomes available. Furthermore, the study focuses on the perceptions of the development of the COVID-19 vaccine and their vaccination attitudes in correlation with convenience and recommendations.
2.2. Data Analysis
The data obtained from the questionnaires were exported into Excel 2016, examined for errors, cleaned, shipped, and analyzed using IBM SPSS Statistics 27.0. Descriptive statistics were used as numbers and percentages to summarize the respondent’s sociodemographic characteristics. Cross-tabulations were performed to map the frequency distribution of selected variables in contingency tables to explore a potential relationship. A Chi-squared test was conducted to examine the significance of the association between demographics and factors influencing vaccine acceptance and determine whether there is a significant difference between expected frequencies and observed frequencies. A logistic regression model was employed on those variables that appeared to have a p-value < 0.05 in the multinominal analysis to identify determinants of participants’ acceptance of a COVID-19 vaccine. The significance of odds ratio (OR) in multivariate analyses was α = 0.05.
2.3. General Vaccine Hesitancy in Austria
Though data on vaccine hesitancy in Austria are limited, reviews of various papers and data reported by the WHO indicate a trend to increasing vaccine hesitancy and a declining child-vaccination rate [
4,
17,
18,
19]. For example, a survey on vaccine hesitancy in Austria, published in 2017, reported that, out of their 350 participants, 40 (11.4%) stated that they deliberately refused vaccinations, with fear of adverse effects, doubt of vaccine effectiveness, and distrust in the pharmaceutical industry being the main reasons for their reluctancy [
17]. To give an example, in Austria, the vaccination coverage for measles and influence do not reach the recommended levels of vaccination by the WHO [
17].
4. Discussion
Since the first diagnosed case of COVID-19 in December 2019, the number of new infections and fatalities in Austria has been increasing rapidly. National authorities are urged to respond to the pandemic appropriately. The World Health Organization (WHO) is yet to confirm and enhance treatment of the disease, which requires the administration of the newly developed vaccine. The rapid approval of the COVID-19 vaccine raises public concerns about its safety, and international surveys have suggested that general hesitancy to a COVID-19 vaccine has grown since its first release. The current willingness to accept a COVID-19 vaccine is insufficient to meet the requirements for community immunity [
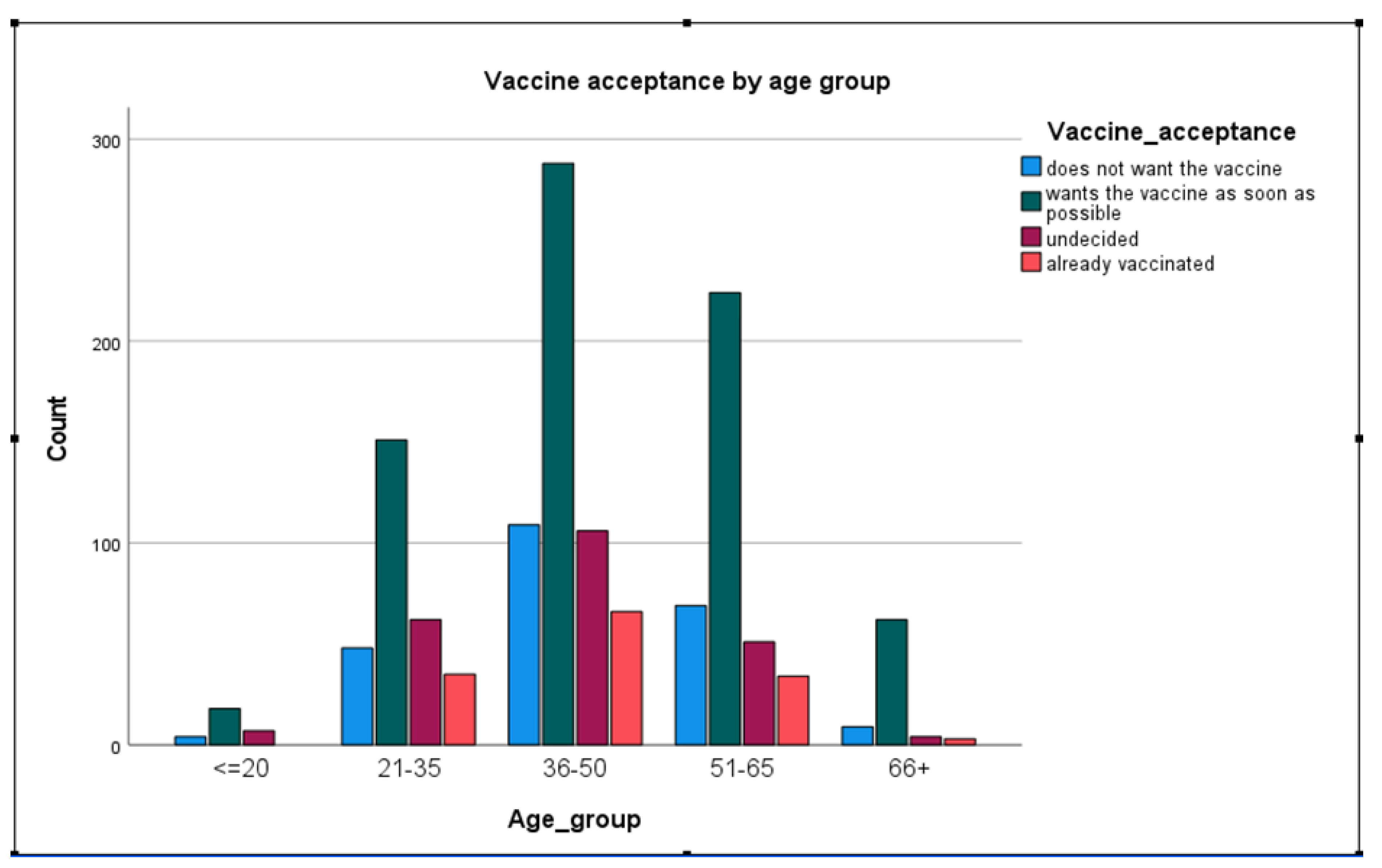
10]. Here, we report the findings of a brief survey addressing the attitude and openness towards the COVID-19 vaccine among Austrian citizens during stage one of the vaccination plan. The results showed that 23.4% of the people who already received their vaccine were aged between 35 and 50 years, estimating that those people were prioritized to be vaccinated owing to their professional background. Though the Austrian vaccination plan (
Figure 1) aims to vaccinate older people and high-risk groups first, the ratio seems unbalanced. For a better understanding of these numbers, our survey could have included a question about the professional area of the participants. In this questionnaire study, a significantly lower response rate for male participants was obtained, which proposes the risk of gender-dependent errors in the analysis of the collected data—a reflection on a potential methodological bias has to be considered and improved in further studies. This apparent gender disparity results in the main limitation of this study. In Austria, insufficient vaccination promotion activity has been reported in the past, and stakeholders face complex challenges regarding the current events of the pandemic [
16]. Furthermore, vaccination records are primarily paper-based and poorly standardized, if at all. Individuals moving from one region to another often face difficulties keeping vaccination records in place and up to date [
21]. Although a national approach for vaccine administration is in place [
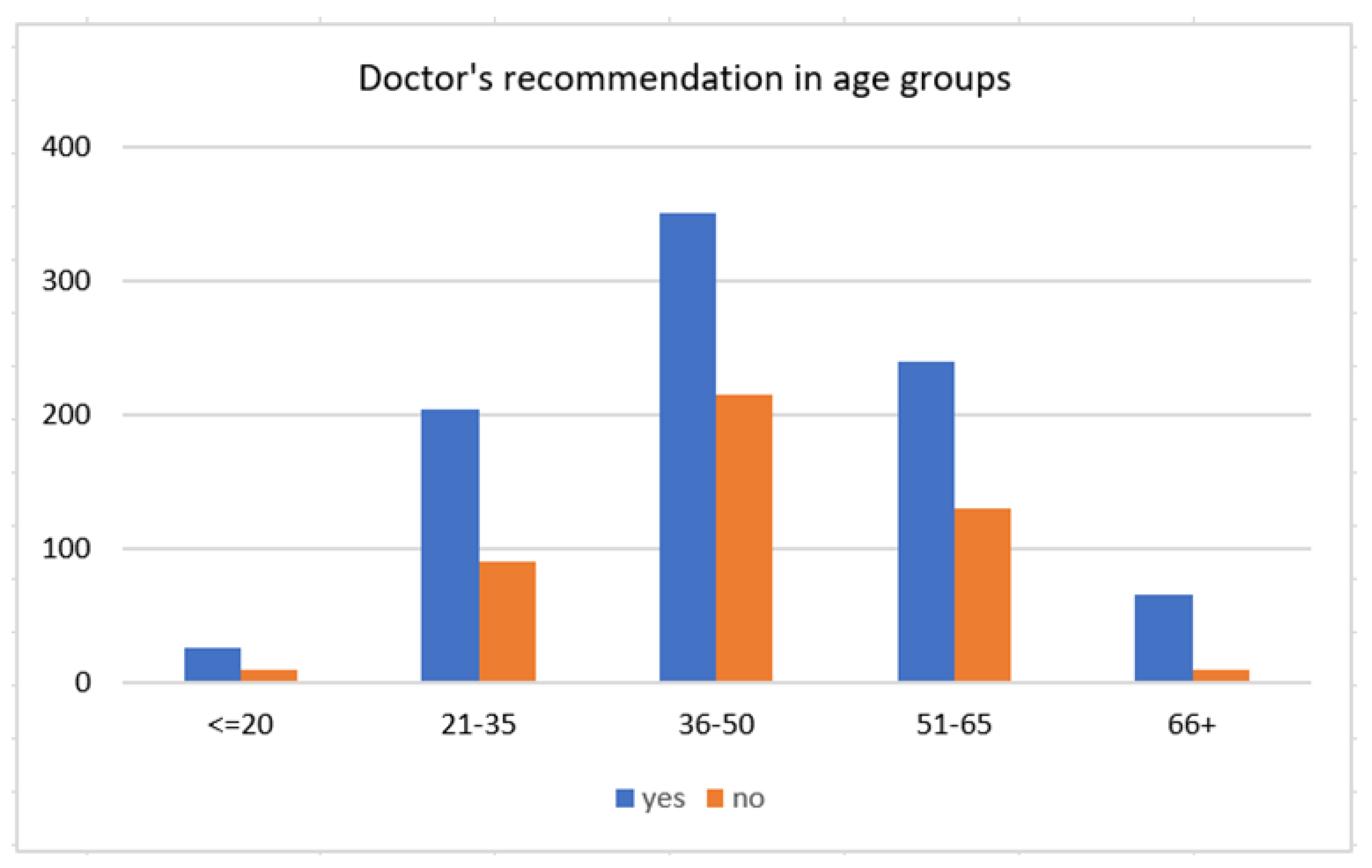
3], greater effort has to be made towards promoting the new vaccine and must reach further than just supplying a free vaccine. Our results show that doctors significantly impact peoples’ decision making and the potential acceptance of the vaccine. Especially, older people might have higher trust in their physician owing to more frequent consultations for other health problems. Therefore, physicians should be made aware and work closely and synergetically with national health authorities in promoting vaccinations.
This study had several limitations, mainly selection biases. Firstly, the fact that 80% of the respondents were females raises several presumptions. Females may have been more inclined to agree to participate in our research, while males were more reluctant. Moreover, women have historically played a crucial role in the research and development of vaccinations. Women are more exposed to vaccinations and more involved in the vaccination status of their children [
22,
23]. Because of the small sample size of men (
n = 241), the number is too small to test differences between men and women. Although the uneven distribution of men and women might be helpful to address the research questions, it may come at the cost of representativeness. Because the sampling method was snowball sampling, further studies should aim to recruit both genders and monitor the information while collecting closer or using a different sampling method.
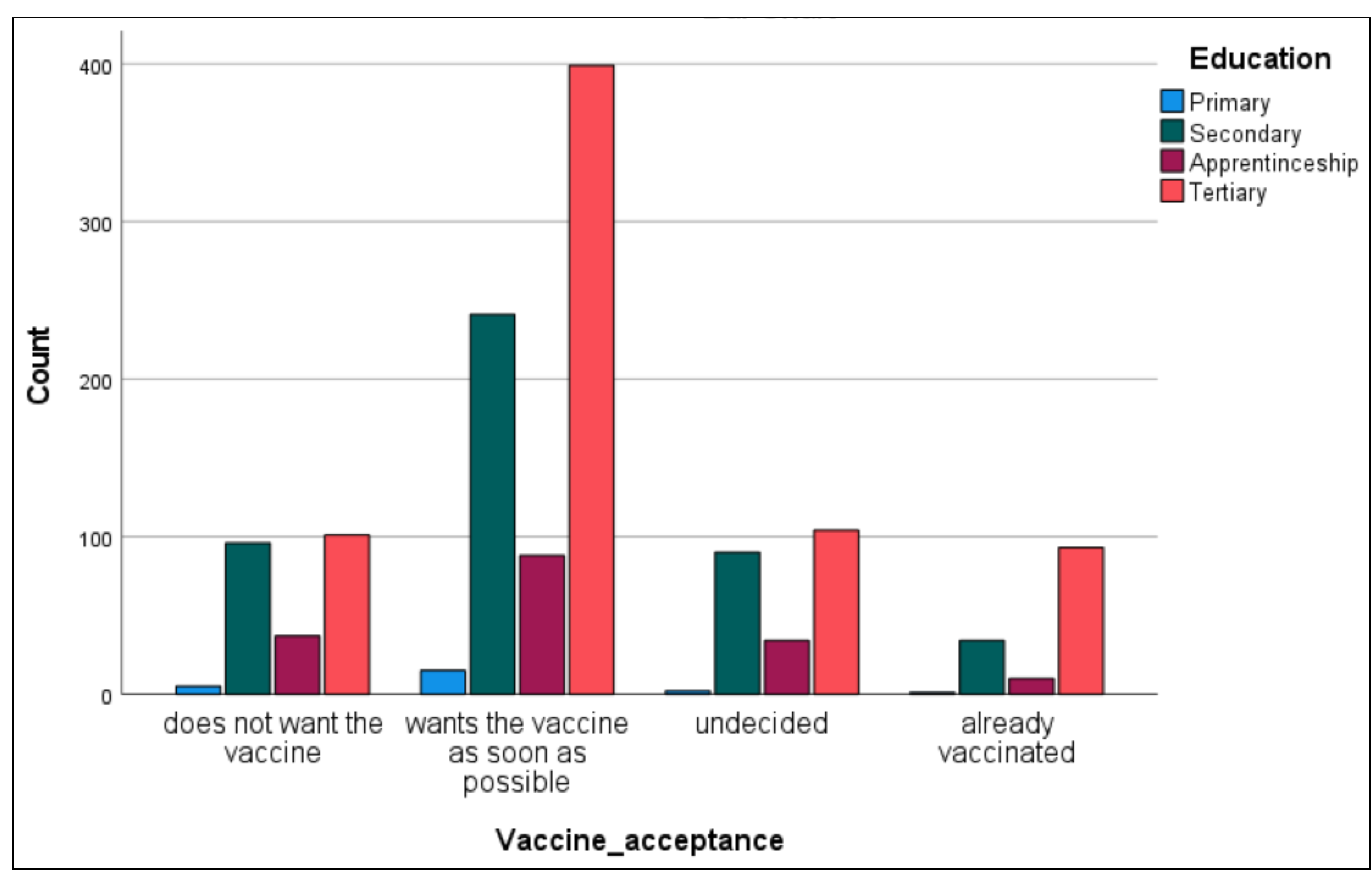
Another limitation, namely the selection bias regarding education, was recognized. This might have occurred because the link was distributed via e-mail to educational institutions and on social media.
In adults, tertiary education appeared to be correlated with a more positive attitude towards vaccination. People with primary education were more likely to be skeptical than people of more mature age. These findings are not entirely in line with other research on vaccine hesitancy and its impact factors. Several studies found that people with higher education were more likely to report vaccine hesitancy and identified higher education as a potential barrier to vaccine acceptance in specific settings [
24,
25,
26], while in other findings, education was a significant factor in desire for COVID-19 vaccine [
27,
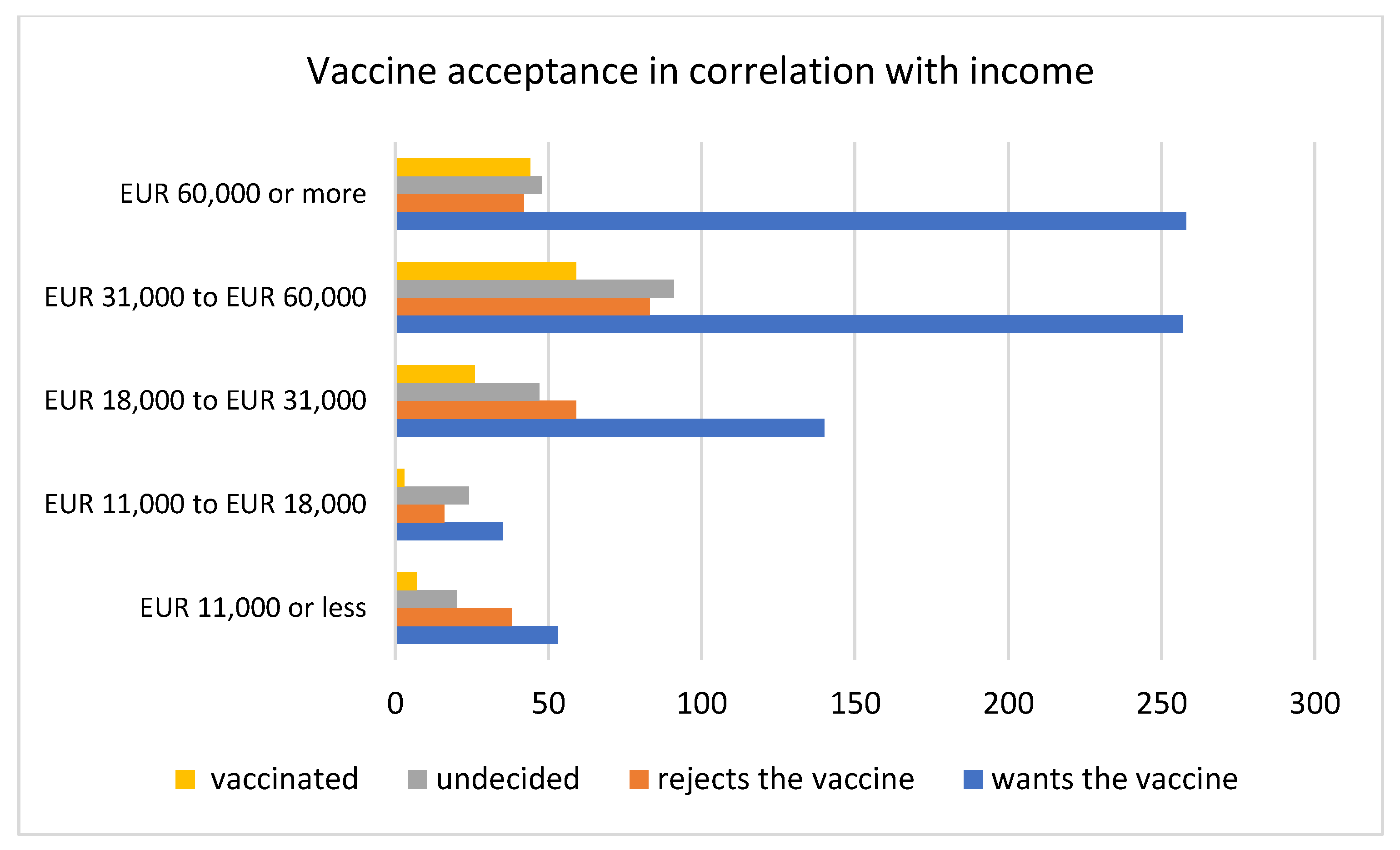
28]. COVID-19 vaccine acceptance increased with increasing age, income, and education level. These findings mirror the trends seen in other studies which surveyed the general population, for example, in the United States [
29,
30].











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}