
In Vitro and In Vivo Feasibility Study for a Portable VV-ECMO and ECCO2R System

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
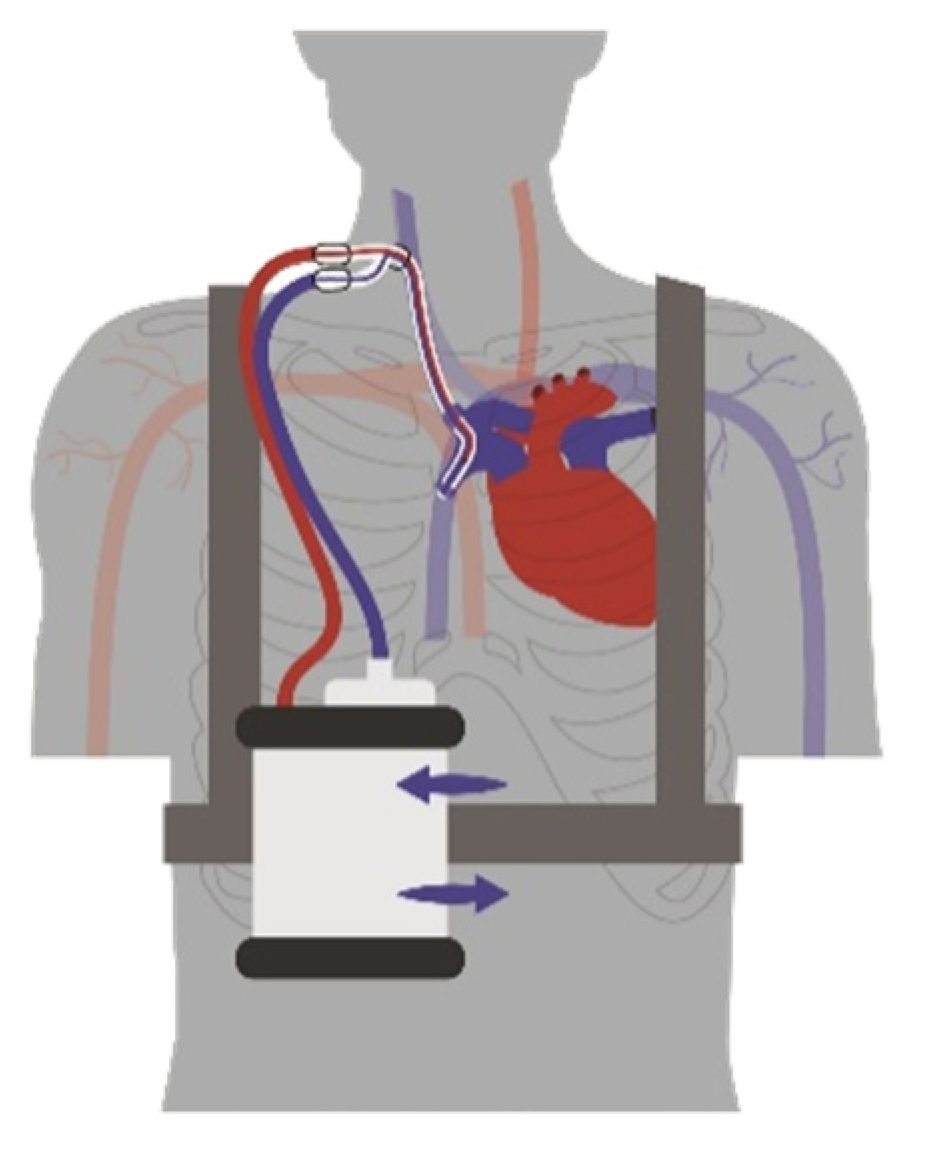
2.1. System Components
2.2. In Vitro Evaluation
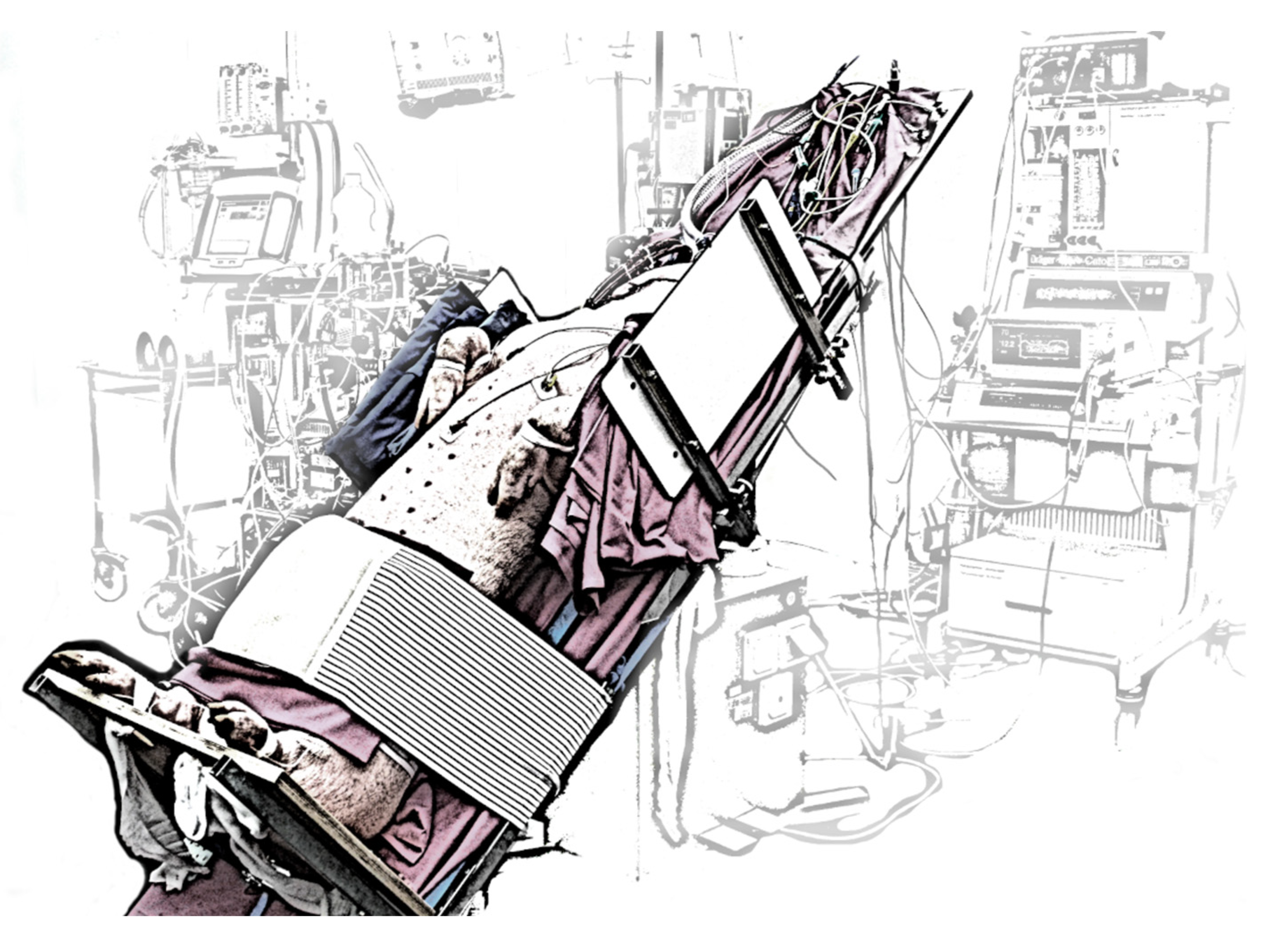
2.3. In Vivo Evaluation

2.4. Statistical Analysis
3. Results
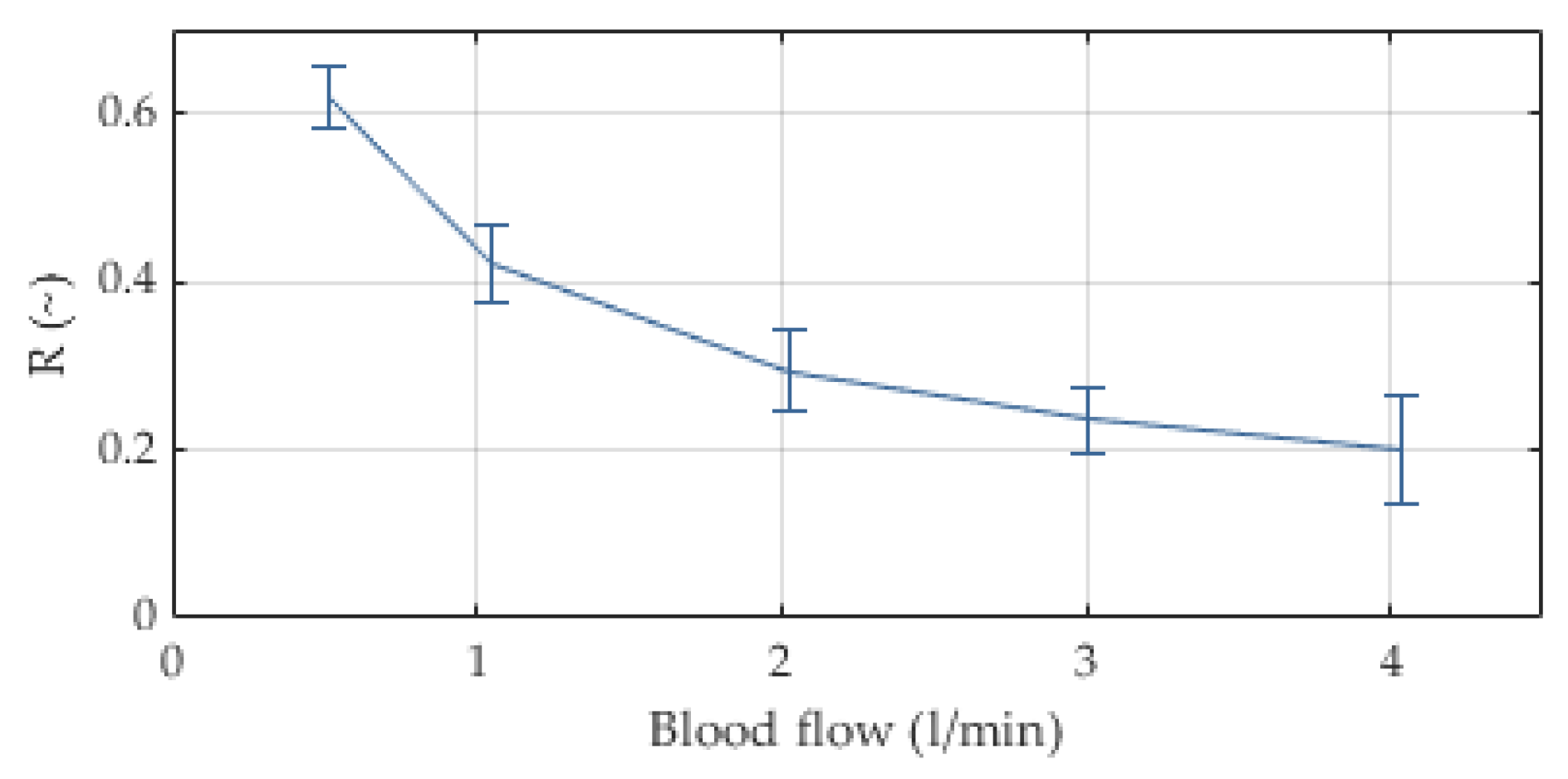
3.1. In Vitro Evaluation
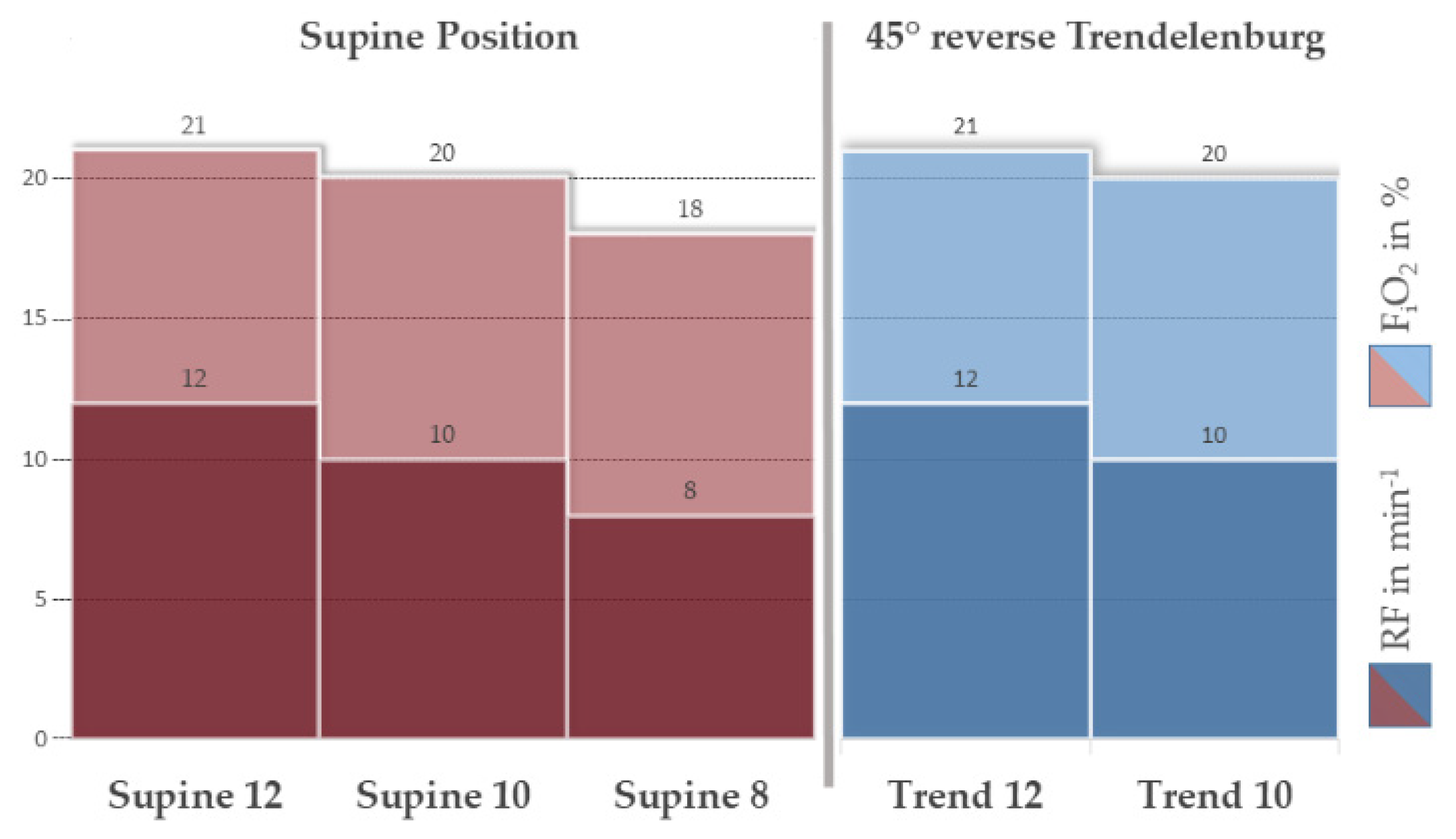
3.2. In Vivo Evaluation

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Supine 12 | Supine 10 | Supine 8 | Trend 12 | Trend 10 | p-Value | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Unit | Mean | Median | SD | Mean | Median | SD | Mean | Median | SD | Mean | Median | SD | Mean | Median | SD | |
| RMV | L/min | 4 | 5 | 2 | 4 | 4 | 1 | 3 | 3 | 2 | 5 | 5 | 1 | 5 | 4 | 1 | 0.040 *, (0) |
| FiO2 | % | 21 | 21 | 1 | 20 | 20 | 3 | 18 | 18 | 0 | 21 | 21 | 1 | 20 | 19 | 1 | 0.004 *, (1) |
| HF | 1/min | 119 | 111 | 34 | 119 | 121 | 51 | 151 | 169 | 56 | 166 | 168 | 40 | 171 | 171 | 36 | 0.035 *, (0) |
| MAP | mmHg | 75 | 71 | 14 | 105 | 94 | 38 | 94 | 84 | 18 | 79 | 75 | 20 | 71 | 71 | 15 | 0.040 *, (0) |
| MPAP | mmHg | 22 | 20 | 8 | 24 | 21 | 10 | 24 | 23 | 5 | 14 | 14 | 12 | 17 | 15 | 16 | 0.355 *, (0) |
| SaO2 | % | 84 | 87 | 11 | 80 | 85 | 14 | 73 | 77 | 24 | 83 | 87 | 10 | 73 | 74 | 11 | 0.483 † |
| ScvO2 | % | 71 | 72 | 10 | 61 | 67 | 13 | 52 | 61 | 17 | 56 | 56 | 7 | 57 | 54 | 11 | 0.235 † |
| SvO2 | % | 65 | 67 | 6 | 68 | 72 | 13 | 55 | 62 | 18 | 57 | 58 | 5 | 56 | 55 | 4 | 0.231 † |
| paO2 | mmHg | 66 | 64 | 15 | 67 | 67 | 19 | 54 | 50 | 19 | 62 | 65 | 10 | 52 | 50 | 8 | 0.311 † |
| pcvO2 | mmHg | 49 | 47 | 6 | 43 | 43 | 5 | 60 | 40 | 35 | 40 | 42 | 3 | 41 | 40 | 4 | 0.157 † |
| pvO2 | mmHg | 44 | 44 | 2 | 50 | 45 | 12 | 38 | 39 | 5 | 40 | 41 | 3 | 40 | 40 | 3 | 0.075 † |
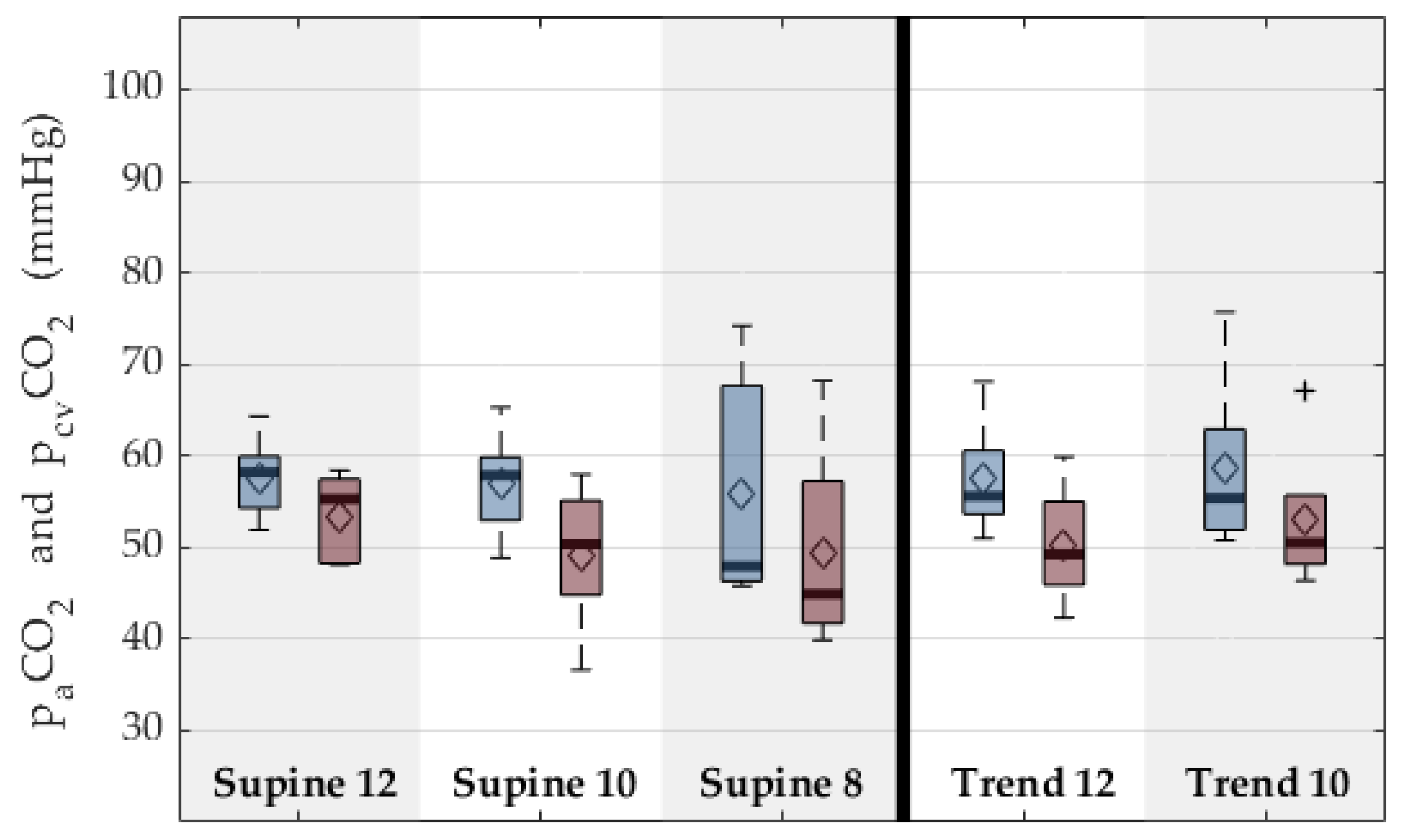
| paCO2 | mmHg | 53 | 55 | 5 | 49 | 50 | 8 | 49 | 45 | 13 | 50 | 49 | 7 | 53 | 51 | 8 | 0.556 † |
| pcvCO2 | mmHg | 58 | 58 | 5 | 57 | 58 | 6 | 56 | 48 | 16 | 57 | 56 | 6 | 59 | 55 | 10 | 0.873 † |
| pvCO2 | mmHg | 56 | 55 | 5 | 52 | 51 | 7 | 51 | 47 | 16 | 54 | 53 | 7 | 57 | 56 | 9 | 0.744 † |
| etCO2 | % | 7 | 6 | 1 | 6 | 7 | 2 | 7 | 6 | 1 | 7 | 7 | 1 | 7 | 7 | 1 | 0.747 * |
| Arterial lactate | mmol/L | 2.8 | 1.0 | 4.1 | 3.5 | 1.7 | 4.1 | 3.0 | 1.8 | 2.7 | 4.1 | 2.6 | 4.0 | 5.6 | 4.5 | 4.8 | 0.255 |
| Arterial pH | [] | 7.4 | 7.4 | 0.1 | 7.4 | 7.4 | 0.1 | 7.4 | 7.4 | 0.1 | 7.4 | 7.4 | 0.1 | 7.3 | 7.3 | 0.1 | 0.321 † |
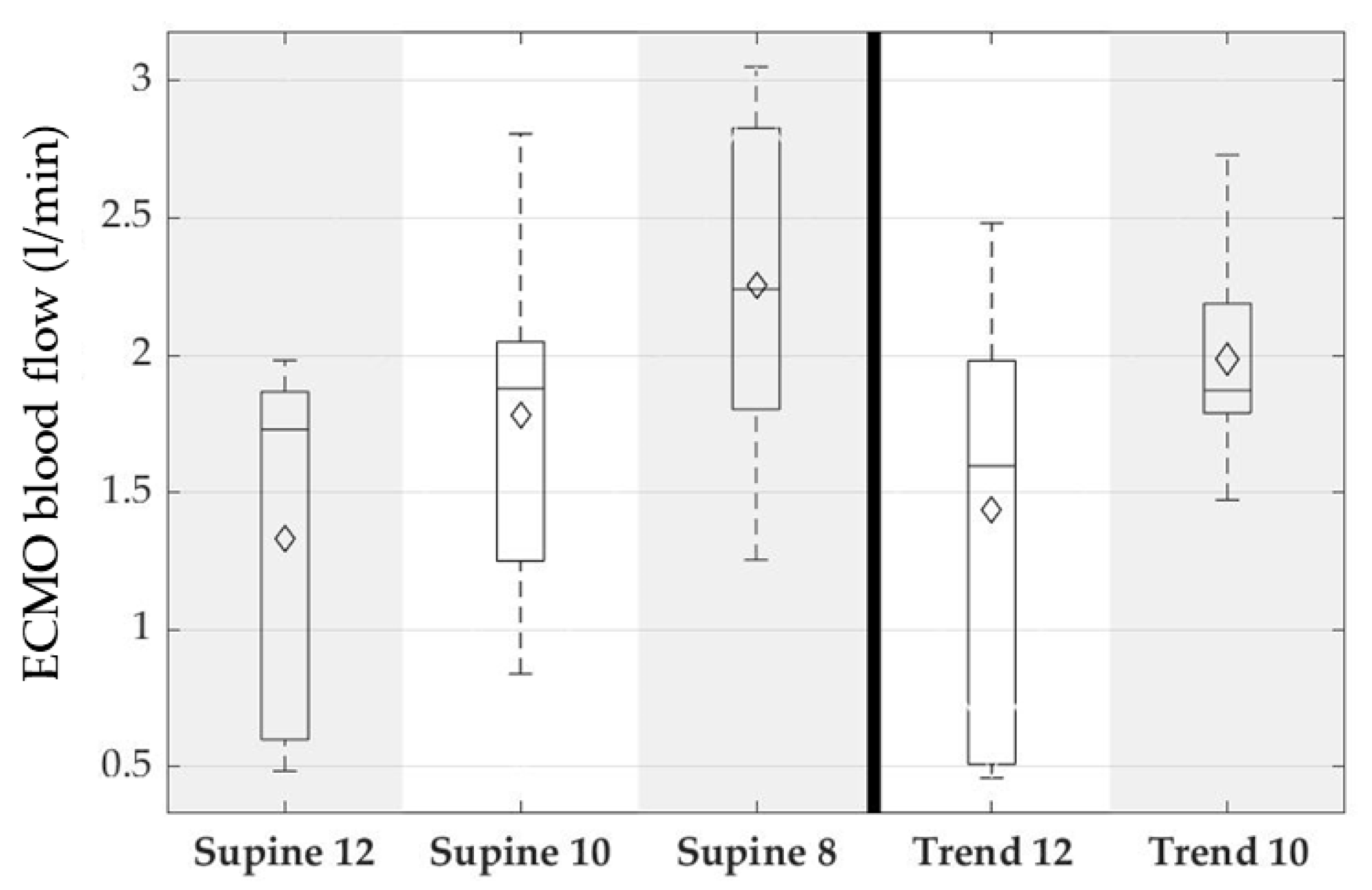
| Blood flow ECMO | L/min | 1.3 | 1.7 | 0.7 | 1.8 | 1.9 | 0.7 | 2.3 | 2.2 | 0.7 | 1.4 | 1.6 | 0.8 | 2.0 | 1.9 | 0.4 | 0.045 *, (0) |
| Pump speed | min−1 | 5470 | 5617 | 2878 | 6803 | 7188 | 2287 | 7457 | 7992 | 1774 | 5797 | 6967 | 2647 | 8097 | 8100 | 1581 | 0.082 * |
| Gas flow | L/min | 4 | 4 | 4 | 5 | 4 | 3 | 6 | 6 | 3 | 4 | 4 | 3 | 5 | 5 | 3 | 0.749 * |
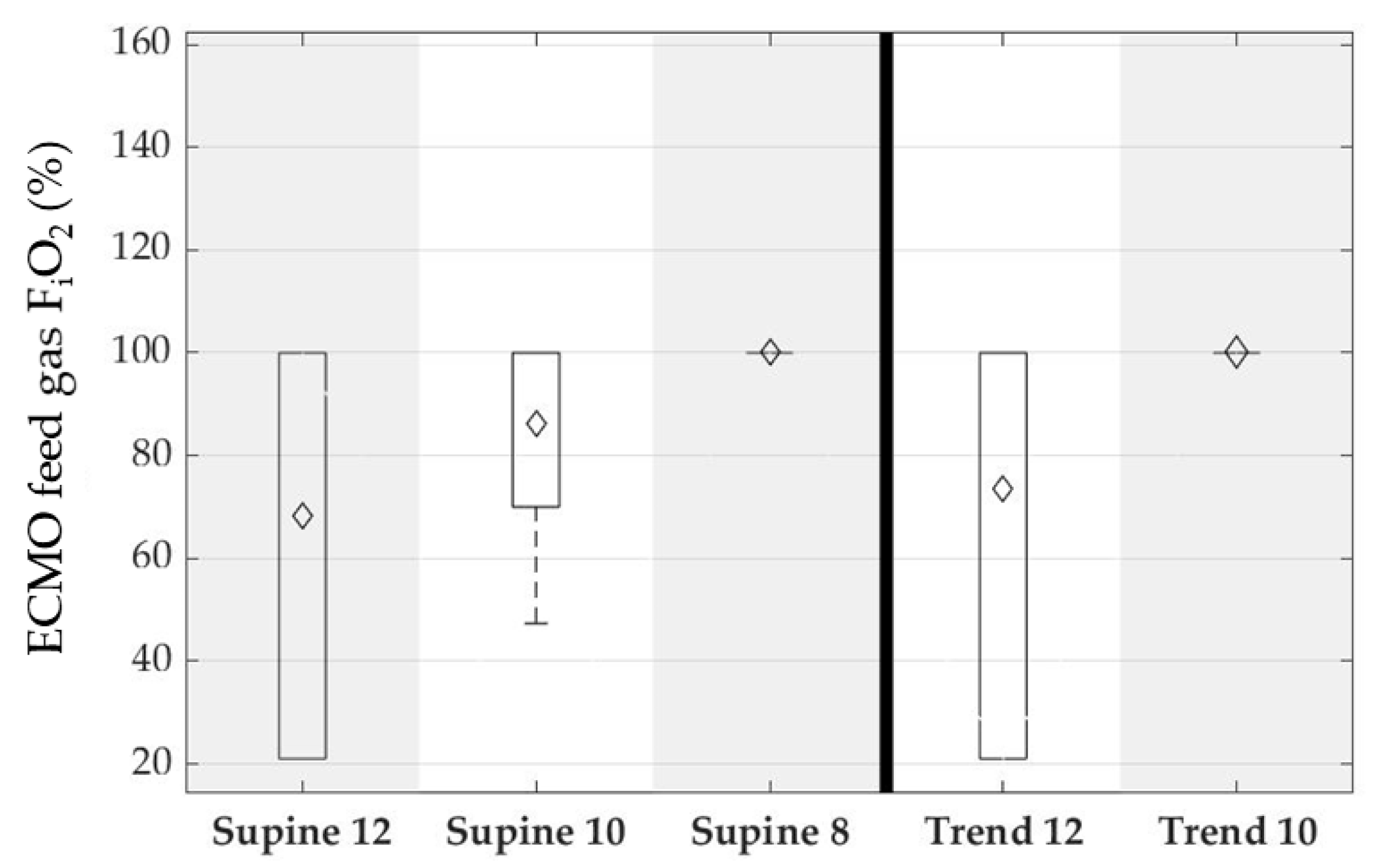
| FiO2 ECMO | % | 68 | 100 | 43 | 86 | 100 | 23 | 100 | 100 | 0 | 74 | 100 | 41 | 100 | 100 | 0 | 0.171 * |
| ΔP ECMO | mmHg | 7 | 7 | 13 | 18 | 20 | 14 | 30 | 28 | 16 | 12 | 16 | 15 | 23 | 26 | 10 | 0.075 * |
| fPHb | mg/dL | 15 | 13 | 6 | 12 | 12 | 7 | 12 | 12 | 7 | 14 | 12 | 4 | 13 | 14 | 6 | 0.920 * |
| SO2 post ECMO | % | 96 | 100 | 8 | 100 | 100 | 1 | 98 | 100 | 5 | 98 | 100 | 3 | 100 | 100 | 0 | 0.922 * |
| SO2 pre ECMO | % | 69 | 76 | 10 | 63 | 68 | 12 | 55 | 58 | 14 | 64 | 68 | 9 | 56 | 55 | 5 | 0.323 * |
| pO2 post ECMO | mmHg | 278 | 322 | 199 | 239 | 227 | 86 | 223 | 182 | 125 | 228 | 232 | 139 | 234 | 181 | 107 | 0.736 * |
| pO2 pre ECMO | mmHg | 48 | 50 | 5 | 48 | 45 | 11 | 52 | 40 | 27 | 45 | 46 | 4 | 41 | 40 | 2 | 0.171 * |
| pCO2 post ECMO | mmHg | 38 | 37 | 13 | 36 | 36 | 5 | 40 | 36 | 7 | 37 | 36 | 3 | 41 | 41 | 3 | 0.073 * |
| pCO2 pre ECMO | mmHg | 58 | 60 | 5 | 54 | 56 | 8 | 54 | 51 | 11 | 55 | 55 | 6 | 59 | 57 | 8 | 0.294 * |
| VCO2 ECMO | mL/min | 106 | 69 | 126 | 85 | 86 | 28 | 78 | 88 | 41 | 58 | 57 | 29 | 60 | 55 | 20 | 0.255 * |
| VO2 ECMO | mL/min | 56 | 57 | 48 | 90 | 93 | 49 | 122 | 133 | 45 | 69 | 74 | 46 | 116 | 123 | 32 | 0.220 * |
4. Discussion
4.1. In Vitro Evaluation
4.2. In Vivo Evaluation
4.3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Tramm, R.; Ilic, D.; Davies, A.R.; Pellegrino, V.A.; Romero, L.; Hodgson, C. Extracorporeal membrane oxygenation for critically ill adults. Cochrane Database Syst. Rev. 2015, 1, CD010381. [Google Scholar] [CrossRef]
- Weill, D.; Benden, C.; Corris, P.A.; Dark, J.H.; Davis, R.D.; Keshavjee, S.; Lederer, D.J.; Mulligan, M.J.; Patterson, G.A.; Singer, L.G.; et al. A consensus document for the selection of lung transplant candidates: 2014--An update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. 2015, 34, 1–15. [Google Scholar] [CrossRef]
- Benazzo, A.; Schwarz, S.; Frommlet, F.; Schweiger, T.; Jaksch, P.; Schellongowski, P.; Staudinger, T.; Klepetko, W.; Lang, G.; Hoetzenecker, K. Twenty-year experience with extracorporeal life support as bridge to lung transplantation. J. Thorac. Cardiovasc. Surg. 2019, 157, 2515–2525.e10. [Google Scholar] [CrossRef]
- Biscotti, M.; Gannon, W.D.; Agerstrand, C.; Abrams, D.; Sonett, J.; Brodie, D.; Bacchetta, M. Awake Extracorporeal Membrane Oxygenation as Bridge to Lung Transplantation: A 9-Year Experience. Ann. Thorac. Surg. 2017, 104, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuehner, T.; Kuehn, C.; Hadem, J.; Wiesner, O.; Gottlieb, J.; Tudorache, I.; Olsson, K.M.; Greer, M.; Sommer, W.; Welte, T.; et al. Extracorporeal membrane oxygenation in awake patients as bridge to lung transplantation. Am. J. Respir. Crit. Care Med. 2012, 185, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Hoetzenecker, K.; Donahoe, L.; Yeung, J.C.; Azad, S.; Fan, E.; Ferguson, N.D.; Del Sorbo, L.; de Perrot, M.; Pierre, A.; Yasufuku, K.; et al. Extracorporeal life support as a bridge to lung transplantation-experience of a high-volume transplant center. J. Thorac. Cardiovasc. Surg. 2018, 155, 1316–1328.e1. [Google Scholar] [CrossRef] [Green Version]
- Quaderi, S.A.; Hurst, J.R. The unmet global burden of COPD. Glob. Health Epidemiol. Genom. 2018, 3, e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varmaghani, M.; Dehghani, M.; Heidari, E.; Sharifi, F.; Moghaddam, S.S.; Farzadfar, F. Global prevalence of chronic obstructive pulmonary disease: Systematic review and meta-analysis. East. Mediterr. Health J. 2019, 25, 47–57. [Google Scholar] [CrossRef]
- Chambers, D.C.; Cherikh, W.S.; Harhay, M.O.; Hayes, D.; Hsich, E.; Khush, K.K.; Meiser, B.; Potena, L.; Rossano, J.W.; Toll, A.E.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-sixth adult lung and heart-lung transplantation Report-2019; Focus theme: Donor and recipient size match. J. Heart Lung Transplant. 2019, 38, 1042–1055. [Google Scholar] [CrossRef]
- Shah, R.J.; Kotloff, R.M. Lung transplantation for obstructive lung diseases. Semin. Respir. Crit. Care Med. 2013, 34, 288–296. [Google Scholar] [CrossRef]
- Kozower, B.D.; Meyers, B.F.; Smith, M.A.; de Oliveira, N.C.; Cassivi, S.D.; Guthrie, T.J.; Wang, H.; Ryan, B.J.; Shen, K.R.; Daniel, T.M.; et al. The impact of the lung allocation score on short-term transplantation outcomes: A multicenter study. J. Thorac. Cardiovasc. Surg. 2008, 135, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Turner, D.A.; Cheifetz, I.M.; Rehder, K.J.; Williford, W.L.; Bonadonna, D.; Banuelos, S.V.J.; Peterson-Carmichael, S.; Lin, S.S.; Davis, R.D.; Zaas, D. Active rehabilitation and physical therapy during extracorporeal membrane oxygenation while awaiting lung transplantation: A practical approach. Crit. Care Med. 2011, 39, 2593–2598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cypel, M.; Keshavjee, S. Extracorporeal life support as a bridge to lung transplantation. Clin. Chest Med. 2011, 32, 245–251. [Google Scholar] [CrossRef] [PubMed]
- de Jonghe, B.; Sharshar, T.; Lefaucheur, J.-P.; Authier, F.-J.; Durand-Zaleski, I.; Boussarsar, M.; Cerf, C.; Renaud, E.; Mesrati, F.; Carlet, J.; et al. Paresis acquired in the intensive care unit: A prospective multicenter study. JAMA 2002, 288, 2859–2867. [Google Scholar] [CrossRef] [Green Version]
- Needham, D.M.; Korupolu, R.; Zanni, J.M.; Pradhan, P.; Colantuoni, E.; Palmer, J.B.; Brower, R.G.; Fan, E. Early physical medicine and rehabilitation for patients with acute respiratory failure: A quality improvement project. Arch. Phys. Med. Rehabil. 2010, 91, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Truong, A.D.; Fan, E.; Brower, R.G.; Needham, D.M. Bench-to-bedside review: Mobilizing patients in the intensive care unit--from pathophysiology to clinical trials. Crit. Care 2009, 13, 216. [Google Scholar] [CrossRef] [Green Version]
- Crotti, S.; Iotti, G.A.; Lissoni, A.; Belliato, M.; Zanierato, M.; Chierichetti, M.; Di Meo, G.; Meloni, F.; Pappalettera, M.; Nosotti, M.; et al. Organ allocation waiting time during extracorporeal bridge to lung transplant affects outcomes. Chest 2013, 144, 1018–1025. [Google Scholar] [CrossRef]
- Lehr, C.J.; Zaas, D.W.; Cheifetz, I.M.; Turner, D.A. Ambulatory extracorporeal membrane oxygenation as a bridge to lung transplantation: Walking while waiting. Chest 2015, 147, 1213–1218. [Google Scholar] [CrossRef]
- Abrams, D.; Combes, A.; Brodie, D. Extracorporeal membrane oxygenation in cardiopulmonary disease in adults. J. Am. Coll. Cardiol. 2014, 63, 2769–2778. [Google Scholar] [CrossRef] [Green Version]
- Abrams, D.; Javidfar, J.; Farrand, E.; Mongero, L.B.; Agerstrand, C.L.; Ryan, P.; Zemmel, D.; Galuskin, K.; Morrone, T.M.; Boerem, P.; et al. Early mobilization of patients receiving extracorporeal membrane oxygenation: A retrospective cohort study. Crit. Care 2014, 18, R38. [Google Scholar] [CrossRef] [Green Version]
- Abrams, D.; Madahar, P.; Eckhardt, C.M.; Short, B.; Yip, N.H.; Parekh, M.; Serra, A.; Dubois, R.L.; Saleem, D.; Agerstrand, C.; et al. Early Mobilization during ECMO for Cardiopulmonary Failure in Adults: Factors Associated with Intensity of Treatment. Ann. Am. Thorac. Soc. 2021, 19, 90–98. [Google Scholar] [CrossRef]
- Ko, Y.; Cho, Y.H.; Park, Y.H.; Lee, H.; Suh, G.Y.; Yang, J.H.; Park, C.-M.; Jeon, K.; Chung, C.R. Feasibility and Safety of Early Physical Therapy and Active Mobilization for Patients on Extracorporeal Membrane Oxygenation. ASAIO J. 2015, 61, 564–568. [Google Scholar] [CrossRef]
- Pruijsten, R.; van Thiel, R.; Hool, S.; Saeijs, M.; Verbiest, M.; Reis Miranda, D. Mobilization of patients on venovenous extracorporeal membrane oxygenation support using an ECMO helmet. Intensive Care Med. 2014, 40, 1595–1597. [Google Scholar] [CrossRef] [PubMed]
- Haji, J.Y.; Mehra, S.; Doraiswamy, P. Awake ECMO and mobilizing patients on ECMO. Indian J. Thorac. Cardiovasc. Surg. 2021, 37, 1–10. [Google Scholar] [CrossRef]
- ISO 7199:2016; Cardiovascular Implants and Artificial Organs: Cardiovascular Implants and Artificial Organs—Blood-Gas Exchangers (Oxygenators), 11.040.40 Implants for Surgery, Prosthetics and Orthotics (7199:2016). International Organization for Standardization: Geneva, Switzerland, 2016.
- Food and Drug Administration. Guidance for Cardiopulmonary Bypass Oxygenators 510 (k) Submissions: Final Guidance for Industry and FDA Staff; Food and Drug Administration: Washington, DC, USA, 2010.
- Hesselmann, F.; Focke, J.M.; Schlanstein, P.C.; Steuer, N.B.; Kaesler, A.; Reinartz, S.D.; Schmitz-Rode, T.; Steinseifer, U.; Jansen, S.V.; Arens, J. Introducing 3D-potting: A novel production process for artificial membrane lungs with superior blood flow design. Bio-Des. Manuf. 2021. [Google Scholar] [CrossRef]
- Kopp, R.; Bensberg, R.; Stollenwerk, A.; Arens, J.; Grottke, O.; Walter, M.; Rossaint, R. Automatic Control of Veno-Venous Extracorporeal Lung Assist. Artif. Organs 2016, 40, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Douglas, A.R.; Jones, N.L.; Reed, J.W. Calculation of whole blood CO2 content. J. Appl. Physiol. (1985) 1988, 65, 473–477. [Google Scholar] [CrossRef]
- Leach, R.M.; Treacher, D.F. The pulmonary physician in critical care * 2: Oxygen delivery and consumption in the critically ill. Thorax 2002, 57, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Maquet Cardiopulmonary GmbH. Instructions for Use: HLS Set Advanced 5.0 | HLS Set Advanced 7.0 1.4|G-270|01; Maquet Cardiopulmonary GmbH: Rastatt, Germany.
- Xenios AG. Data Sheet: Novalung iLA Membrane Ventilator; Xenios AG: Heilbronn, Germany.
- Ficial, B.; Vasques, F.; Zhang, J.; Whebell, S.; Slattery, M.; Lamas, T.; Daly, K.; Agnew, N.; Camporota, L. Physiological Basis of Extracorporeal Membrane Oxygenation and Extracorporeal Carbon Dioxide Removal in Respiratory Failure. Membranes 2021, 11, 225. [Google Scholar] [CrossRef]
- von Petersdorff-Campen, K.; Abeken, J.; de Zélicourt, D.; Kurtcuoglu, V.; Meboldt, M.; Schmid Daners, M. In Vitro Testing and Comparison of Additively Manufactured Polymer Impellers for the CentriMag Blood Pump. ASAIO J. 2021, 67, 306–313. [Google Scholar] [CrossRef]
- Kopp, R.; Bensberg, R.; Arens, J.; Steinseifer, U.; Schmitz-Rode, T.; Rossaint, R.; Henzler, D. A miniaturized extracorporeal membrane oxygenator with integrated rotary blood pump: Preclinical in vivo testing. ASAIO J. 2011, 57, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Madhani, S.P.; Frankowski, B.J.; Ye, S.-H.; Burgreen, G.W.; Wagner, W.R.; Kormos, R.; D’Cunha, J.; Federspiel, W.J. In Vivo 5 Day Animal Studies of a Compact, Wearable Pumping Artificial Lung. ASAIO J. 2019, 65, 94–100. [Google Scholar] [CrossRef]
- Kopp, R.; Mottaghy, K.; Kirschfink, M. Mechanism of complement activation during extracorporeal blood-biomaterial interaction: Effects of heparin coated and uncoated surfaces. ASAIO J. 2002, 48, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Lappa, A.; Cottini, M.; Ranocchi, S.D.F.; Luzi, G.; Montalto, A.; Contento, C.; Bruno, A.; Pisani, P.; Antonio, P.; Emiliano, V.; et al. Single or Double Site Cannuation for Veno-Venous Ecmo in Severe Obese Patient? ARC J. Anesthesiol. 2016, 1, 19–24. [Google Scholar] [CrossRef]
- Chen, R.H.-S.; Yam, N.; Lun, K.-S.; Au, T.W.-K. Migrated Avalon-Elite cannula in an infant transcatheter repositioning without interruption of ECMO flow. J. Artif. Organs 2021, 24, 382–386. [Google Scholar] [CrossRef]
- Kalbhenn, J.; Maier, S.; Heinrich, S.; Schallner, N. Bedside repositioning of a dislocated Avalon-cannula in a running veno-venous ECMO. J. Artif. Organs 2017, 20, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Simons, A.P.; Donker, D.W.; Weerwind, P.W. Optimized safety and function of the bicaval dual-lumen cannula by refined positioning and bedside management. Intensive Care Med. 2013, 39, 984–985. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, D.; Pitcher, H.T.; Cavarocchi, N.; Hirose, H. Migrated Avalon Veno-Venous Extracorporeal Membrane Oxygenation Cannula: How to Adjust Without Interruption of Flow. J. Card. Surg. 2015, 30, 865–868. [Google Scholar] [CrossRef] [Green Version]
- Betancor, J.; Xu, B.; Rehman, K.A.; Rivas, C.G.; Patel, K.; Tong, M.Z.; Rodriguez, L.L. Transesophageal Echocardiographic Guidance of Venovenous Extracorporeal Membrane Oxygenation Cannula (Avalon Cannula) Repositioning. CASE 2017, 1, 150–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reis Miranda, D.; Dabiri Abkenari, L.; Nieman, K.; Dijkshoorn, M.; Duckers, E.; Gommers, D. Myocardial infarction due to malposition of ECMO cannula. Intensive Care Med. 2012, 38, 1233–1234. [Google Scholar] [CrossRef] [Green Version]
- Steuer, N.B.; Hugenroth, K.; Beck, T.; Spillner, J.; Kopp, R.; Reinartz, S.; Schmitz-Rode, T.; Steinseifer, U.; Wagner, G.; Arens, J. Long-Term Venovenous Connection for Extracorporeal Carbon Dioxide Removal (ECCO2R)-Numerical Investigation of the Connection to the Common Iliac Veins. Cardiovasc. Eng. Technol. 2020, 11, 362–380. [Google Scholar] [CrossRef] [PubMed]
- Palmér, O.; Palmér, K.; Hultman, J.; Broman, M. Cannula Design and Recirculation During Venovenous Extracorporeal Membrane Oxygenation. ASAIO J. 2016, 62, 737–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conrad, S.A.; Wang, D. Evaluation of Recirculation During Venovenous Extracorporeal Membrane Oxygenation Using Computational Fluid Dynamics Incorporating Fluid-Structure Interaction. ASAIO J. 2021, 67, 943–953. [Google Scholar] [CrossRef] [PubMed]
- Broman, M.; Frenckner, B.; Bjällmark, A.; Broomé, M. Recirculation during veno-venous extra-corporeal membrane oxygenation--a simulation study. Int. J. Artif. Organs 2015, 38, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Müller, T.; Lubnow, M.; Philipp, A.; Bein, T.; Jeron, A.; Luchner, A.; Rupprecht, L.; Reng, M.; Langgartner, J.; Wrede, C.E.; et al. Extracorporeal pumpless interventional lung assist in clinical practice: Determinants of efficacy. Eur. Respir. J. 2009, 33, 551–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp, R.; Bensberg, R.; Wardeh, M.; Rossaint, R.; Kuhlen, R.; Henzler, D. Pumpless arterio-venous extracorporeal lung assist compared with veno-venous extracorporeal membrane oxygenation during experimental lung injury. Br. J. Anaesth. 2012, 108, 745–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]














Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strudthoff, L.J.; Lüken, H.; Jansen, S.V.; Petran, J.; Schlanstein, P.C.; Schraven, L.; Schürmann, B.J.; Steuer, N.B.; Wagner, G.; Schmitz-Rode, T.; et al. In Vitro and In Vivo Feasibility Study for a Portable VV-ECMO and ECCO2R System. Membranes 2022, 12, 133. https://doi.org/10.3390/membranes12020133
Strudthoff LJ, Lüken H, Jansen SV, Petran J, Schlanstein PC, Schraven L, Schürmann BJ, Steuer NB, Wagner G, Schmitz-Rode T, et al. In Vitro and In Vivo Feasibility Study for a Portable VV-ECMO and ECCO2R System. Membranes. 2022; 12(2):133. https://doi.org/10.3390/membranes12020133
Chicago/Turabian StyleStrudthoff, Lasse J., Hannah Lüken, Sebastian V. Jansen, Jan Petran, Peter C. Schlanstein, Lotte Schraven, Benjamin J. Schürmann, Niklas B. Steuer, Georg Wagner, Thomas Schmitz-Rode, and et al. 2022. "In Vitro and In Vivo Feasibility Study for a Portable VV-ECMO and ECCO2R System" Membranes 12, no. 2: 133. https://doi.org/10.3390/membranes12020133
APA StyleStrudthoff, L. J., Lüken, H., Jansen, S. V., Petran, J., Schlanstein, P. C., Schraven, L., Schürmann, B. J., Steuer, N. B., Wagner, G., Schmitz-Rode, T., Steinseifer, U., Arens, J., & Kopp, R. (2022). In Vitro and In Vivo Feasibility Study for a Portable VV-ECMO and ECCO2R System. Membranes, 12(2), 133. https://doi.org/10.3390/membranes12020133