
Considerations on the Controlled Delivery of Bioactive Compounds through Hyaluronic Acid Membrane



 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of the Bioactive Formulation
2.2. Physicochemical Characterization of the Bioactive Formulation
2.3. Cytotoxicity Analysis
2.4. Microbiological Assessment
2.4.1. Reactivation of Microorganisms for the Minimum Inhibitory Concentration (MIC) Testing
2.4.2. The Minimum Inhibitory Concentration (MIC) Antibiogram
2.5. pH Influence on the Stability of the Active Compounds
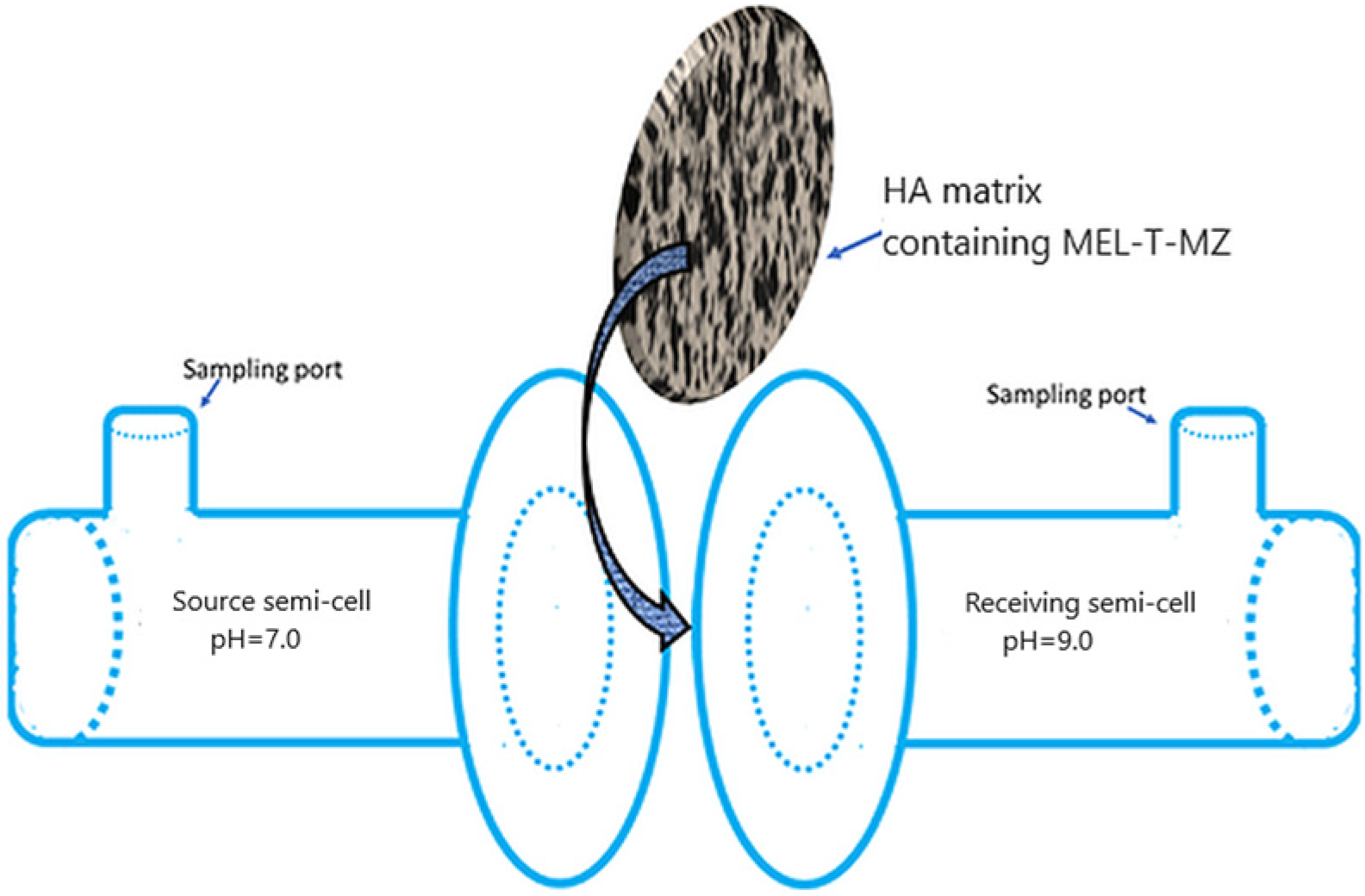
2.6. Release Profile Measurements
3. Results
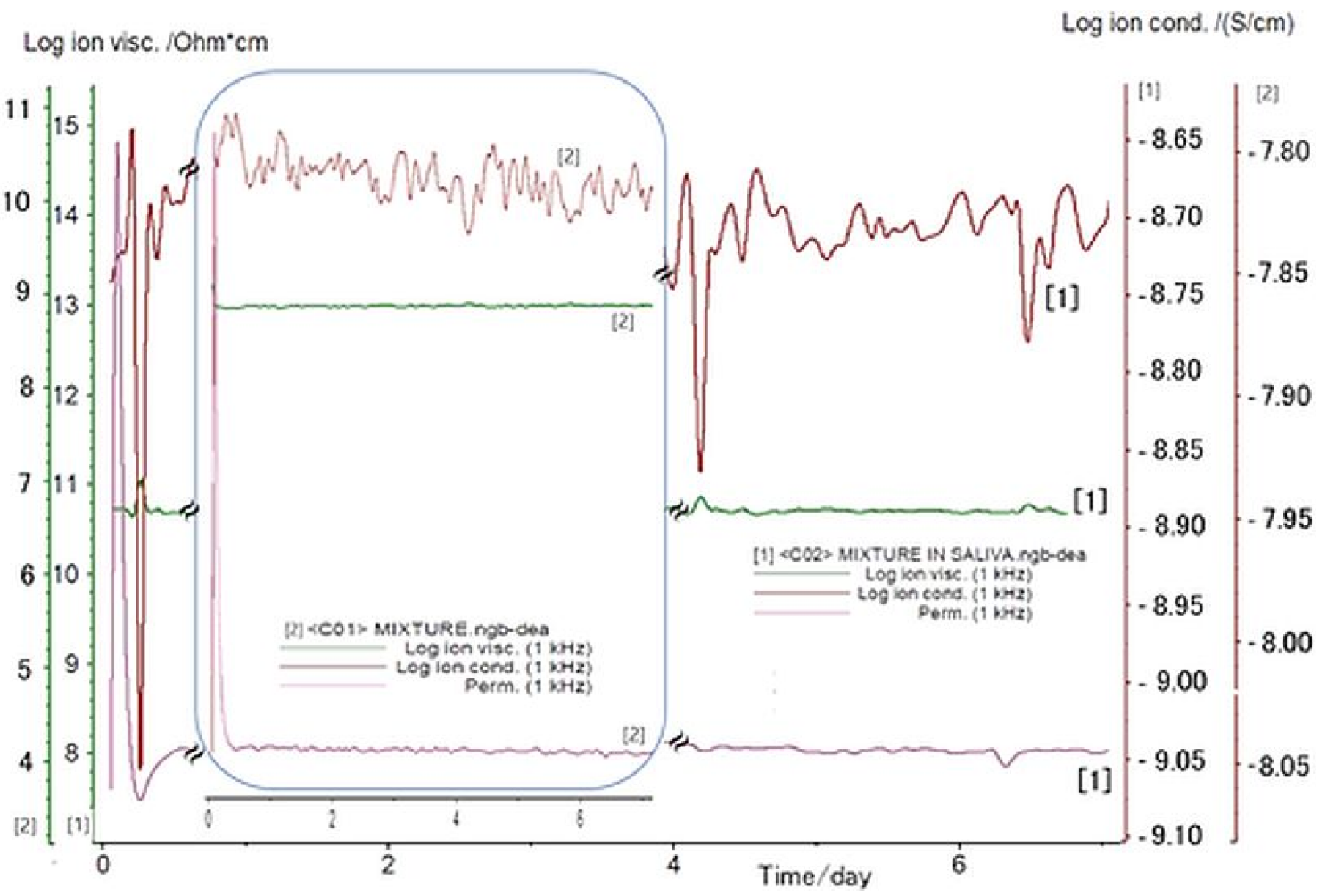
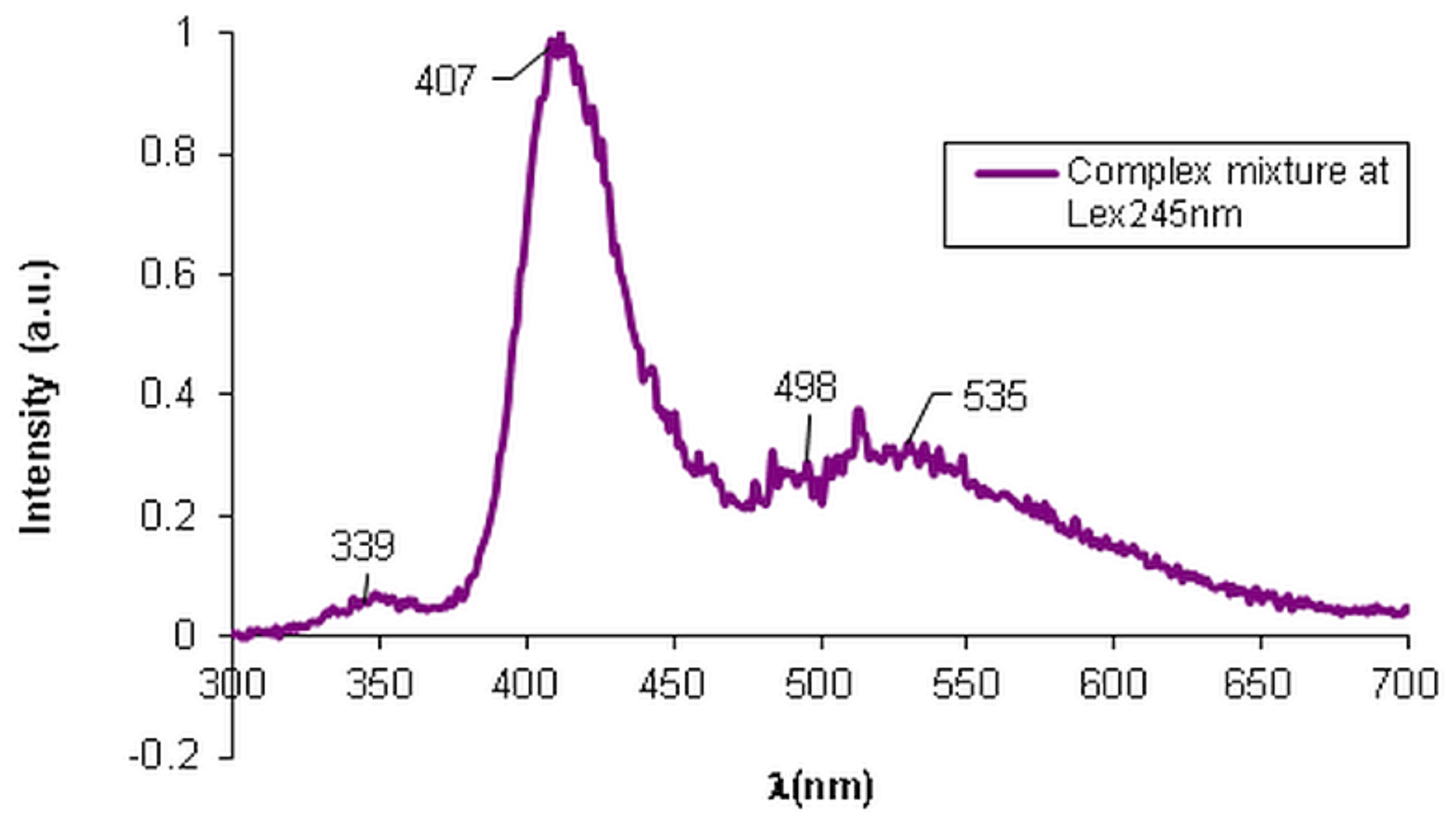
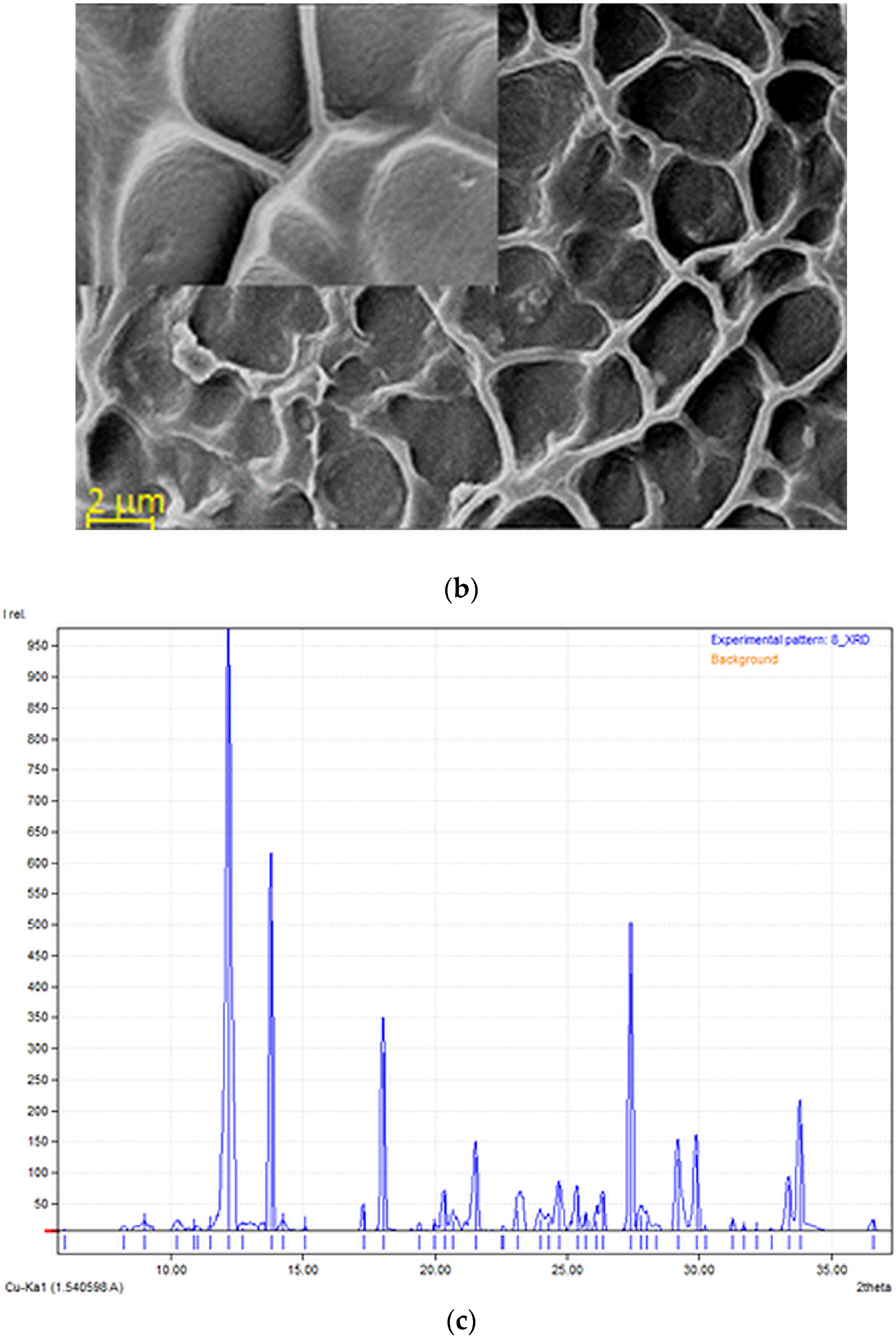
3.1. Physicochemical Characterization of the Bioactive Formulation
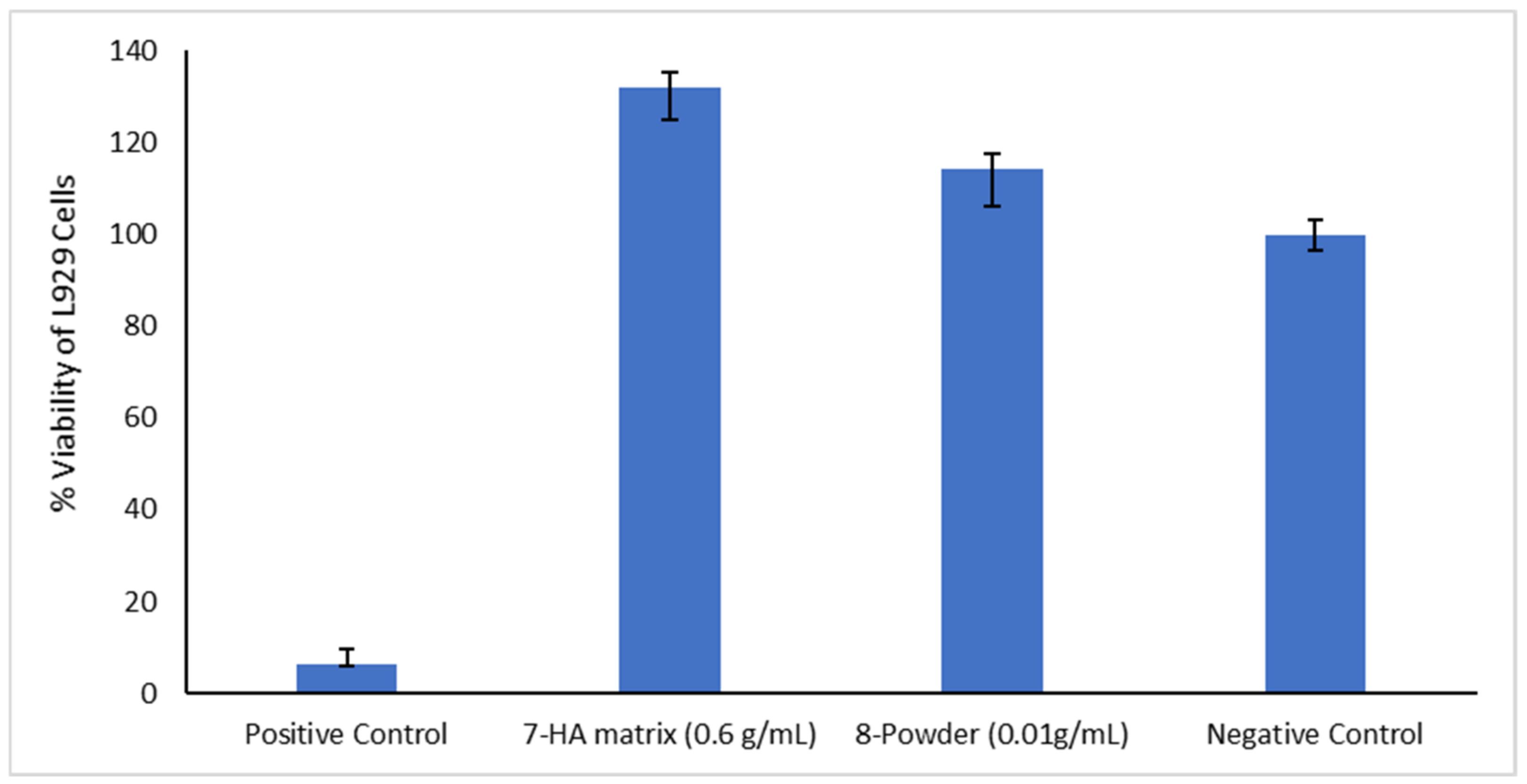
3.2. Cytotoxicity Analysis
3.3. Microbiological Assessment
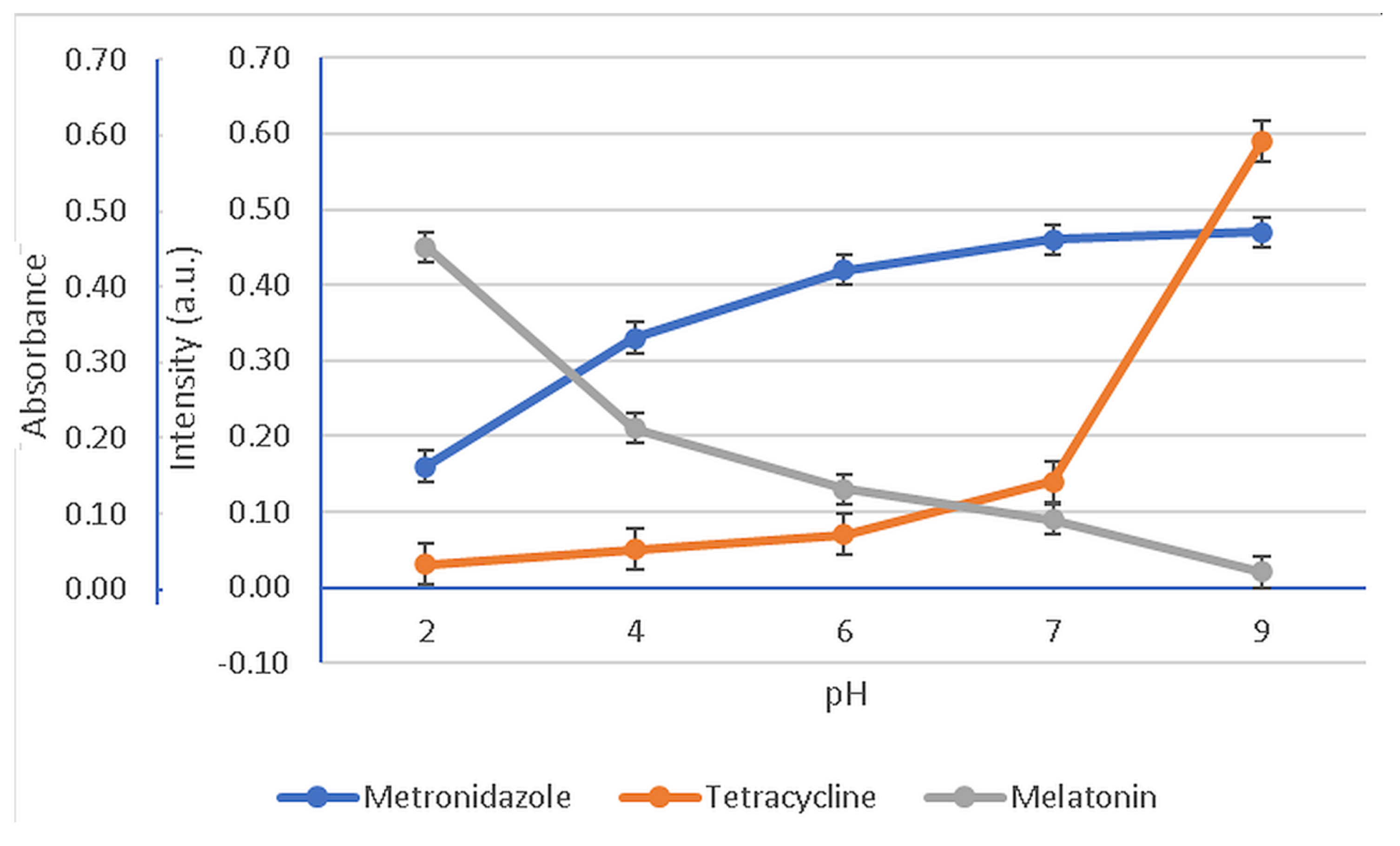
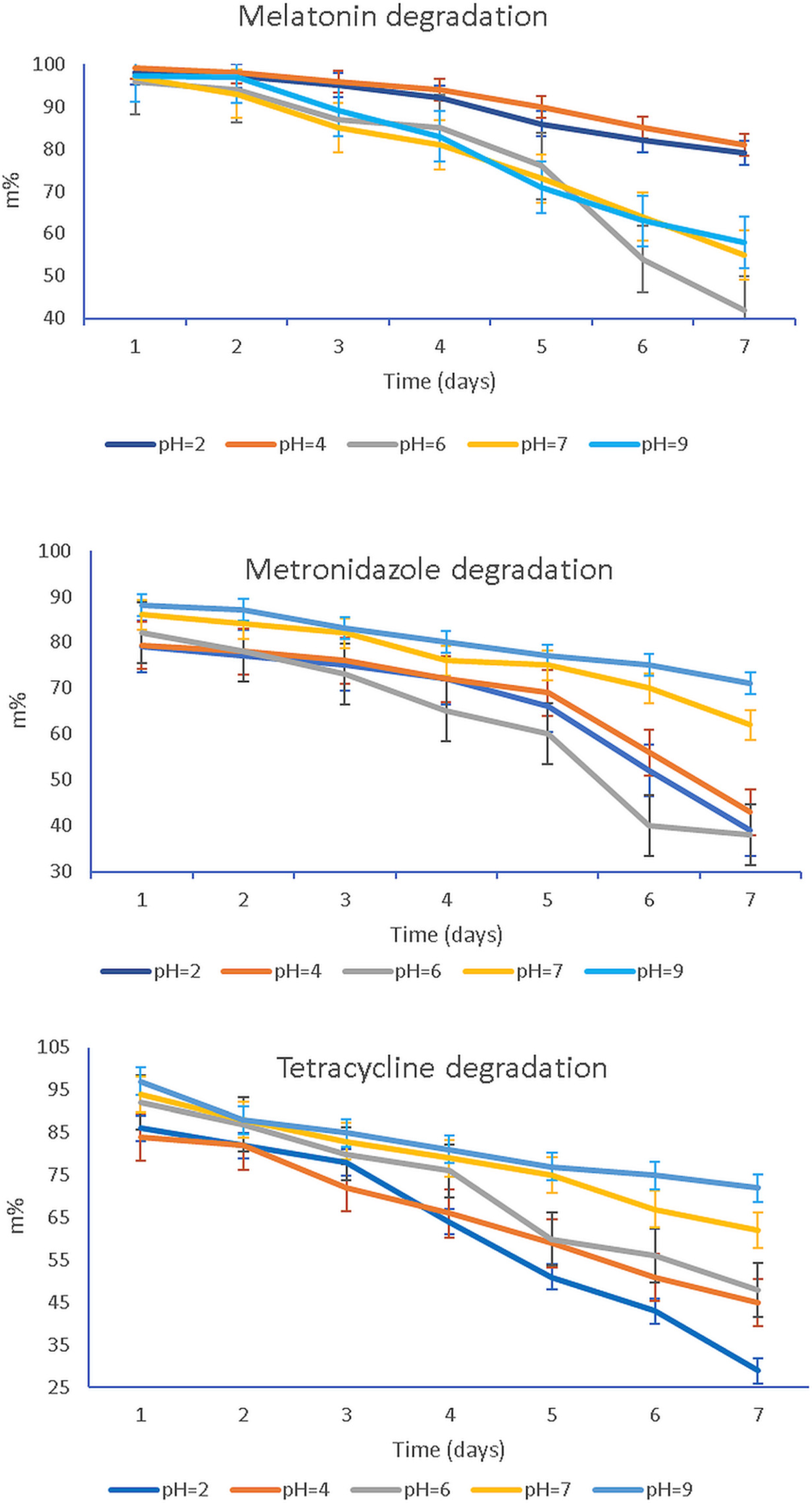
3.4. pH Influence
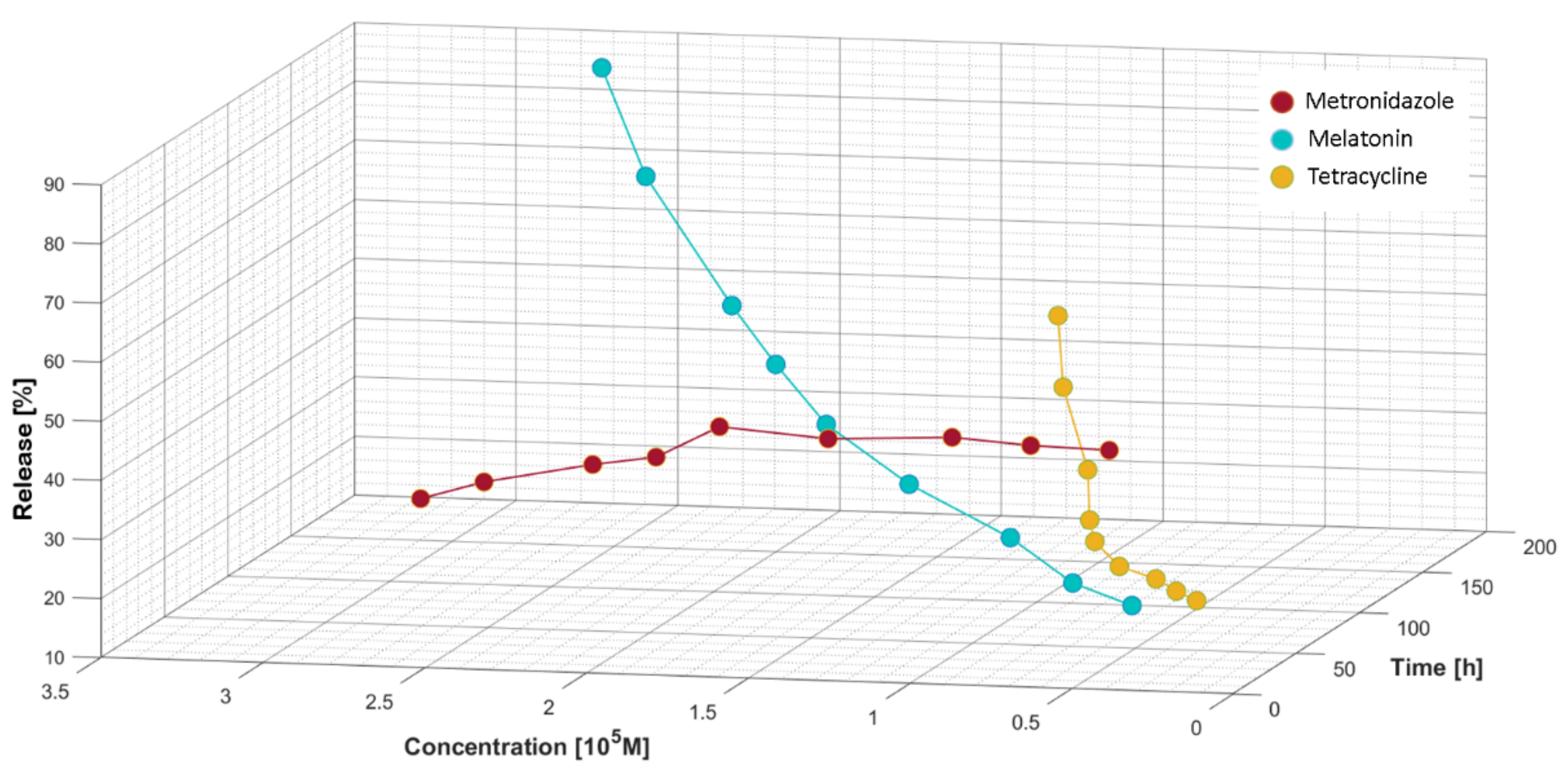
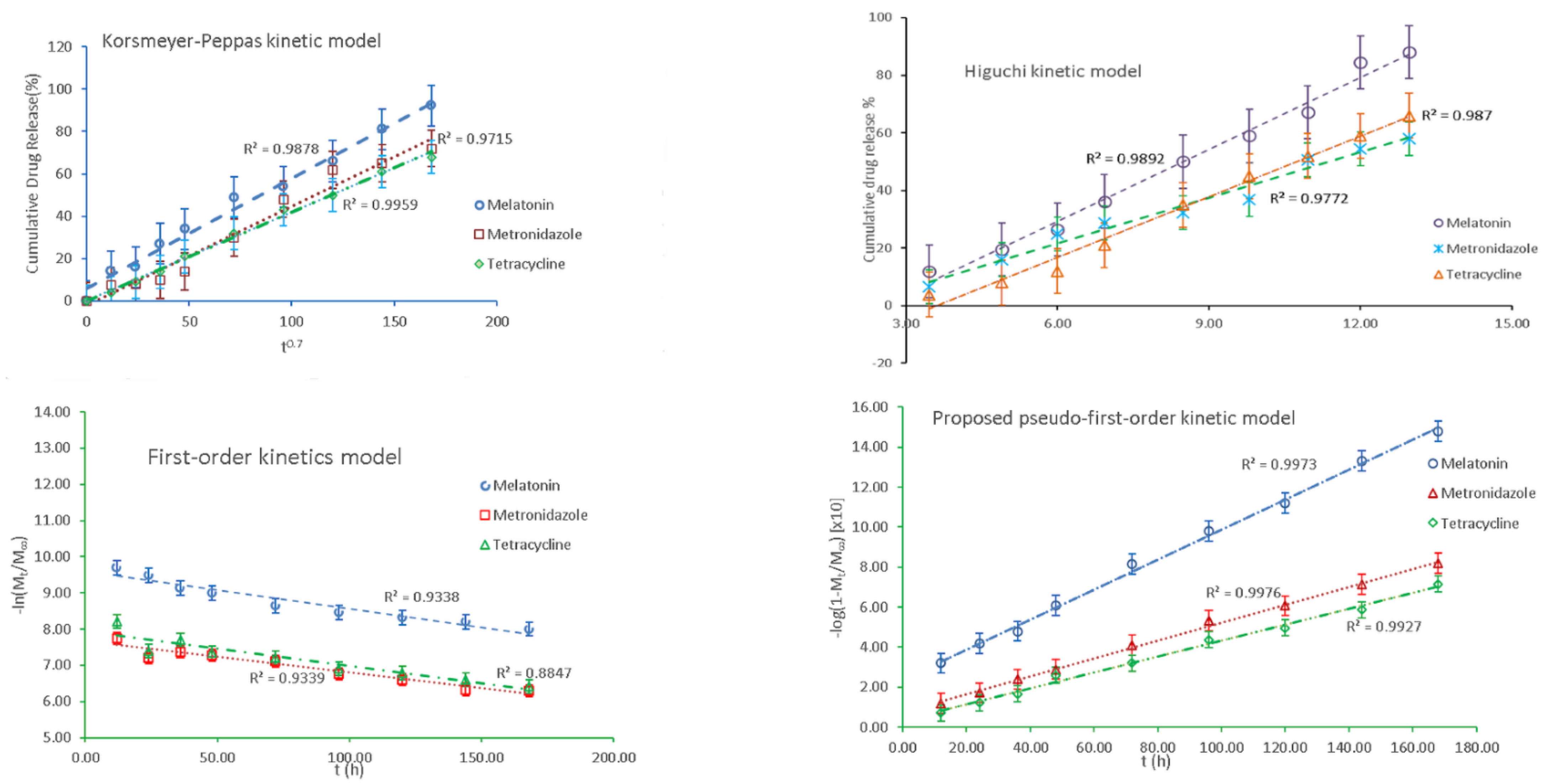
3.5. Release Profiles
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Seong, Y.-J.; Lin, G.; Kim, B.J.; Kim, H.-E.; Kim, S.; Jeong, S.-H. Hyaluronic Acid-Based Hybrid Hydrogel Microspheres with Enhanced Structural Stability and High Injectability. ACS Omega 2019, 4, 13834–13844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, B.; Zhang, M.; Shen, J.; He, Z.; Fatehi, P.; Ni, Y. Applications of cellulose-based materials in sustained drug delivery systems. Curr. Med. Chem. 2019, 26, 2485–2501. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Hui, P.C.-L.; Siu, W.S.; Kan, C.-W.; Leung, P.-C.; Wanxue, C.; Chiou, J.-C. Influence of pH-responsive compounds synthesized from chitosan and hyaluronic acid on dual-responsive (pH/temperature) hydrogel drug delivery systems of Cortex Moutan. Int. J. Biol. Macromol. 2021, 168, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Tang, X.; Jia, Y.; Ho, C.T.; Huang, Q. Applications and delivery mechanisms of hyaluronic acid used for topical/transdermal delivery—A review. Int. J. Pharm. 2020, 578, 119127. [Google Scholar] [CrossRef]
- Kim, H.S.; Yang, J.; Kim, K.; Shin, U.S. Biodegradable and injectable hydrogels as an immunosuppressive drug delivery system. Mater. Sci. Eng. C 2019, 98, 472–481. [Google Scholar] [CrossRef]
- Verhoef, J.J.F.; Anchordoquy, T.J. Questioning the use of PEGylation for drug delivery. Drug Deliv. Transl. Res. 2013, 3, 499–503. [Google Scholar] [CrossRef]
- Elashiry, M.; Meghil, M.M.; Arce, R.M.; Cutler, C.W. From manual periodontal probing to digital 3-D imaging to endoscopic capillaroscopy: Recent advances in periodontal disease diagnosis. J. Periodontal. Res. 2019, 54, 1–9. [Google Scholar] [CrossRef]
- Marsh, P.D.; Zaura, E. Dental biofilm: Ecological interactions in health and disease. J. Clin. Periodontol. 2017, 44, S12–S22. [Google Scholar] [CrossRef]
- Abou Neel, E.A.; Aljabo, A.; Strange, A.; Ibrahim, S.; Coathup, M.; Young, A.M.; Bozec, L.; Mudera, V. Demineralization-remineralization dynamics in teeth and bone. Int. J. Nanomed. 2016, 11, 4743–4763. [Google Scholar] [CrossRef]
- Jepsen, K.; Jepsen, S. Antibiotics/antimicrobials: Systemic and local administration in the therapy of mild to moderately advanced periodontitis. Periodontology 2000 2016, 71, 82–112. [Google Scholar] [CrossRef]
- Pilloni, A.; Zeza, B.; Kuis, D.; Vrazic, D.; Domic, T.; Olszewska-Czyz, I.; Popova, C.; Kotsilkov, K.; Firkova, E.; Dermendzieva, Y.; et al. Treatment of Residual Periodontal Pockets Using a Hyaluronic Acid-Based Gel: A 12 Month Multicenter Randomized Triple-Blinded Clinical Trial. Antibiotics 2021, 10, 924. [Google Scholar] [CrossRef]
- Cho, Y.D.; Kim, K.H.; Lee, Y.M.; Ku, Y.; Seol, Y.J. Periodontal Wound Healing and Tissue Regeneration: A Narrative Review. Pharmaceuticals 2021, 14, 456. [Google Scholar] [CrossRef]
- Henskens, Y.M.; van der Weijden, F.A.; van den Keijbus, P.A.; Veerman, E.C.; Timmerman, M.F.; van der Velden, U.; Amerongen, A.V. Effect of periodontal treatment on the protein composition of whole and parotid saliva. J. Periodontol. 1996, 67, 205–212. [Google Scholar] [CrossRef]
- Galgut, P.N. The relevance of pH to gingivitis and periodontitis. J. Int. Acad. Periodontol. 2001, 3, 61–67. [Google Scholar]
- Muñoz-Carrillo, J.; Hernández-Reyes, V.E.; García-Huerta, O.E.; Chávez-Ruvalcaba, F.; Chávez-Ruvalcaba, M.I.; Chávez-Ruvalcaba, K.M.; Díaz-Alfaro, L. Pathogenesis of Periodontal Disease. In Periodontal Disease: Diagnostic and Adjunctive Non-surgical Considerations; Yussif, N.M.A., Ed.; IntechOpen: London, UK, 2019; pp. 848–865. [Google Scholar]
- Dahiya, P.; Kamal, R. Hyaluronic Acid: A boon in periodontal therapy. N. Am. J. Med. Sci. 2013, 5, 309–315. [Google Scholar] [CrossRef]
- Bonito, A.J.; Lux, L.; Lohr, K.N. Impact of local adjuncts to scaling and root planing in periodontal disease therapy: A systematic review. J. Periodontol. 2005, 76, 1227–1236. [Google Scholar] [CrossRef]
- Goldberg, M. Antibiotics and Antibacterial Medications for Endodontic Treatments. JSM Dent. 2020, 8, 1124. [Google Scholar]
- Passarelli, P.C.; Netti, A.; Lopez, M.A.; Giaquinto, E.F.; De Rosa, G.; Aureli, G.; Bodnarenko, A.; Papi, P.; Starzyńska, A.; Pompa, G.; et al. Local/Topical Antibiotics for Peri-Implantitis Treatment: A Systematic Review. Antibiotics 2021, 10, 1298. [Google Scholar] [CrossRef]
- Junmahasathien, T.; Panraksa, P.; Protiarn, P.; Hormdee, D.; Noisombut, R.; Kantrong, N.; Jantrawut, P. Preparation and Evaluation of Metronidazole-Loaded Pectin Films for Potentially Targeting a Microbial Infection Associated with Periodontal Disease. Polymers 2018, 10, 1021. [Google Scholar] [CrossRef] [Green Version]
- Fu, Y.; Rubio, A.H.; Gscheider, C.; du Teil Espina, M.; del Carmen Flores-Vallejo, R.; van Dijl, J.M.; Gabarrini, G. Oral and Dental Infections: Bacteria. Ref. Modul. Biomed. Sci. 2021. [Google Scholar] [CrossRef]
- Loesche, W.J.; Grossman, N.S. Periodontal Disease as a Specific, albeit Chronic, Infection: Diagnosis and Treatment. Clin. Microbiol. Rev. 2001, 14, 727–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitz-Mayfield, L.J.A. Systemic antibiotics in periodontal therapy. Aust. Dent. J. 2009, 54, S96–S101. [Google Scholar] [CrossRef] [PubMed]
- Matesanz-Pérez, P.; García-Gargallo, M.; Figuero, E.; Bascones-Martínez, A.; Sanz, M.; Herrera, D. A systematic review on the effects of local antimicrobials as adjuncts to subgingival debridement, compared with subgingival debridement alone, in the treatment of chronic periodontitis. J. Clin. Periodontol. 2013, 40, 227–241. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.K.C.; Ng, R.W.Y.; Leung, S.S.Y.; Hui, M.; Ip, M. Overcoming the rising incidence and evolving mechanisms of antibiotic resistance by novel drug delivery approaches—An overview. Adv. Drug Deliv. Rev. 2022, 181, 114078. [Google Scholar] [CrossRef]
- Kumar, M.; Sarma, D.K.; Shubham, S.; Kumawat, M.; Verma, V.; Nina, P.B.; Jp, D.; Kumar, S.; Singh, B.; Tiwari, R.R. Futuristic Non-antibiotic Therapies to Combat Antibiotic Resistance: A Review. Front. Microbiol. 2021, 12, 16. [Google Scholar] [CrossRef]
- Chandler, C.I.R. Current accounts of antimicrobial resistance: Stabilisation, individualisation and antibiotics as infrastructure. Palgrave Commun. 2019, 5, 6. [Google Scholar] [CrossRef] [Green Version]
- Vanić, Ž.; Jøraholmen, M.W.; Škalko-Basnet, N. Nanomedicines for the topical treatment of vulvovaginal infections: Addressing the challenges of antimicrobial resistance. Adv. Drug Deliv. Rev. 2021, 178, 113855. [Google Scholar] [CrossRef]
- Cristache, C.M.; Totu, E.E.; Burlibasa, M.; Tanase, G.; Iorgulescu, G.; Burlibasa, L. Preliminary Study on Genotoxicity Assessment of an Innovative Topical Treatment for Periodontal Disease. Rev. Chim. 2020, 71, 145–150. [Google Scholar] [CrossRef]
- Mhaske, N.; Sheker, A.; Marawar, P.; Mote, N. Evaluation of melatonin levels in saliva in periodontal health and disease: A clinico-biochemical study. J. Int. Clin. Dent. Res. Organ. 2010, 2, 119. [Google Scholar] [CrossRef]
- Marawar, A.; Marawar, P.; Nandal, D.H.; Kunkulol, R.; Narwane, S. Evaluation of Effect of Melatonin on Hematological Parameters in Patients of Periodontitis. Int. J. Clin. Biomed. Res. 2019, 5, 46–49. [Google Scholar] [CrossRef]
- Balaji, T.M.; Varadarajan, S.; Jagannathan, R.; Mahendra, J.; Fageeh, H.I.; Fageeh, H.N.; Mushtaq, S.; Baeshen, H.A.; Bhandi, S.; Gupta, A.A.; et al. Melatonin as a topical/systemic formulation for the management of periodontitis: A systematic review. Materials 2021, 14, 2417. [Google Scholar] [CrossRef]
- Hardeland, R. Melatonin and inflammation—Story of a double-edged blade. J. Pineal Res. 2018, 65, e12525. [Google Scholar] [CrossRef] [Green Version]
- Nabavi, S.M.; Nabavi, S.F.; Sureda, A.; Xiao, J.; Dehpour, A.R.; Shirooie, S.; Silva, A.S.; Baldi, A.; Khan, H.; Daglia, M. Anti-inflammatory effects of Melatonin: A mechanistic review. Crit. Rev. Food Sci. Nutr. 2019, 59, S4–S16. [Google Scholar] [CrossRef]
- El-Sharkawy, H.; Elmeadawy, S.; Elshinnawi, U.; Anees, M. Is dietary melatonin supplementation a viable adjunctive therapy for chronic periodontitis?—A randomized controlled clinical trial. J. Periodontal Res. 2019, 54, 190–197. [Google Scholar] [CrossRef]
- Castro, M.M.L.; Duarte, N.N.; Nascimento, P.C.; Magno, M.B.; Fagundes, N.C.F.; Flores-Mir, C.; Monteiro, M.C.; Rösing, C.K.; Maia, L.C.; Lima, R.R. Antioxidants as Adjuvants in Periodontitis Treatment: A Systematic Review and Meta-Analysis. Oxid. Med. Cell. Longev. 2019, 2019, 9187978. [Google Scholar] [CrossRef]
- Bazyar, H.; Gholinezhad, H.; Moradi, L.; Salehi, P.; Abadi, F.; Ravanbakhsh, M.; Zare Javid, A. The effects of melatonin supplementation in adjunct with non-surgical periodontal therapy on periodontal status, serum melatonin and inflammatory markers in type 2 diabetes mellitus patients with chronic periodontitis: A double-blind, placebo-controlled t. Inflammopharmacology 2019, 27, 67–76. [Google Scholar] [CrossRef]
- Balaji, T.M.; Vasanthi, H.R.; Rao, S.R. Gingival, plasma and salivary levels of melatonin in periodontally healthy individuals and chronic periodontitis patients: A pilot study. J. Clin. Diagnostic Res. 2015, 9, ZC23–ZC25. [Google Scholar] [CrossRef]
- Balaji, T.M.; Varadarajan, S.; Jagannathan, R.; Gupta, A.A.; Raj, A.T.; Patil, S.; Fageeh, H.I.; Fageeh, H.N. Melatonin levels in periodontitis vs. the healthy state: A systematic review and meta-analysis. Oral Dis. 2020, 28, 284–306. [Google Scholar] [CrossRef]
- Tuncay Tanrıverdi, S.; Cheaburu-Yilmaz, C.N.; Carbone, S.; Özer, Ö.; Tuncay Tanrıverdi, S.; Cheaburu-Yilmaz, C.N.; Carbone, S.O. Preparation and in vitro evaluation of melatonin-loaded HA/PVA gel formulations. Pharm. Dev. Technol. 2018, 23, 815–825. [Google Scholar] [CrossRef]
- Kovacic, P.; Somanathan, R. Melatonin and Circadian Rhythm: Aging, Cancer, and Mechanism. Open J. Prev. Med. 2014, 4, 545–560. [Google Scholar] [CrossRef] [Green Version]
- Konečná, B.; Chobodová, P.; Janko, J.; Baňasová, L.; Bábíčková, J.; Celec, P.; Tóthová, Ľ. The Effect of Melatonin on Periodontitis. Int. J. Mol. Sci. 2021, 22, 2390. [Google Scholar] [CrossRef] [PubMed]
- Mayo, J.C.; Tan, D.X.; Sainz, R.M.; Lopez-Burillo, S.; Reiter, R.J. Oxidative damage to catalase induced by peroxyl radicals: Functional protection by melatonin and other antioxidants. Free Radic. Res. 2003, 37, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Idle, J.R.; Krausz, K.W.; Gonzalez, F.J. Metabolism of melatonin by human cytochromes P450. Drug Metab. Dispos. 2005, 33, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Yu, Y.; Shen, Y.; Liu, Q.; Zhao, Z.; Sharma, R.; Reiter, R.J. Melatonin Synthesis and Function: Evolutionary History in Animals and Plants. Front. Endocrinol. 2019, 10, 249. [Google Scholar] [CrossRef]
- Carpentieri, A.R.; Oliva, C.; Díez-Noguera, A.; Cambras, T.; Carpentieri, A.R.; Oliva, C.; Díez-Noguera, A.C. Melatonin administration modifies circadian motor activity under constant light depending on the lighting conditions during suckling. Chronobiol. Int. 2015, 32, 994–1004. [Google Scholar] [CrossRef]
- Kim, T.K.; Kleszczynśki, K.; Janjetovic, Z.; Sweatman, T.; Lin, Z.; Li, W.; Reiter, R.J.; Fischer, T.W.; Slominski, A.T. Metabolism of melatonin and biological activity of intermediates of melatoninergic pathway in human skin cells. FASEB J. 2013, 27, 2742. [Google Scholar] [CrossRef]
- Ressmeyer, A.R.; Mayo, J.C.; Zelosko, V.; Sáinz, R.M.; Tan, D.X.; Poeggeler, B.; Antolín, I.; Zsizsik, B.K.; Reiter, R.J.; Hardeland, R. Antioxidant properties of the melatonin metabolite N1-acetyl-5-methoxykynuramine (AMK): Scavenging of free radicals and prevention of protein destruction. Redox Rep. 2003, 8, 205–213. [Google Scholar] [CrossRef] [Green Version]
- Cagnoli, C.M.; Atabay, C.; Kharlamova, E.; Manev, H. Melatonin protects neurons from singlet oxygen-induced apoptosis. J. Pineal Res. 1995, 18, 222–226. [Google Scholar] [CrossRef]
- Escames, G.; Guerrero, J.M.; Reiter, R.J.; Garcia, J.J.; Munoz-Hoyos, A.; Ortiz, G.G.; Oh, C.S. Melatonin and vitamin E limit nitric oxide-induced lipid peroxidation in rat brain homogenates. Neurosci. Lett. 1997, 230, 147–150. [Google Scholar] [CrossRef]
- Rodriguez, C.; Mayo, J.C.; Sainz, R.M.; Antolín, I.; Herrera, F.; Martín, V.; Reiter, R.J. Regulation of antioxidant enzymes: A significant role for melatonin. J. Pineal Res. 2004, 36, 1–9. [Google Scholar] [CrossRef]
- Wang, Y.; Andrukhov, O.; Rausch-Fan, X. Oxidative stress and antioxidant system in periodontitis. Front. Physiol. 2017, 8, 910. [Google Scholar] [CrossRef] [Green Version]
- Reiter, R.J.; Mayo, J.C.; Tan, D.X.; Sainz, R.M.; Alatorre-Jimenez, M.; Qin, L. Melatonin as an antioxidant: Under promises but over delivers. J. Pineal Res. 2016, 61, 253–278. [Google Scholar] [CrossRef]
- Galano, A.; Tan, D.X.; Reiter, R.J. Melatonin as a natural ally against oxidative stress: A physicochemical examination. J. Pineal Res. 2011, 51, 1–16. [Google Scholar] [CrossRef]
- Amstrup, A.K.; Sikjaer, T.; Mosekilde, L.; Rejnmark, L. Melatonin and the skeleton. Osteoporos. Int. 2013, 24, 2919–2927. [Google Scholar] [CrossRef]
- Olszewska-Czyz, I.; Kralik, K.; Prpic, J. Biomolecules in dental applications: Randomized, controlled clinical trial evaluating the influence of hyaluronic acid adjunctive therapy on clinical parameters of moderate periodontitis. Biomolecules 2021, 11, 1491. [Google Scholar] [CrossRef]
- Jiang, D.; Liang, J.; Noble, P.W. Hyaluronan as an Immune Regulator in Human Diseases. Physiol. Rev. 2011, 91, 221. [Google Scholar] [CrossRef] [Green Version]
- David-Raoudi, M.; Tranchepain, F.; Deschrevel, B.; Vincent, J.C.; Bogdanowicz, P.; Boumediene, K.; Pujol, J.P. Differential effects of hyaluronan and its fragments on fibroblasts: Relation to wound healing. Wound Repair Regen. 2008, 16, 274–287. [Google Scholar] [CrossRef]
- Litwiniuk, M.; Krejner, A.; Grzela, T. Hyaluronic Acid in Inflammation and Tissue Regeneration. Wounds A Compend. Clin. Res. Pract. 2016, 28, 78–88. [Google Scholar]
- Gall, Y. Hyaluronic acid: Structure, metabolism and implication in cicatrisation. Ann. Dermatol. Venereol. 2010, 137, S30–S39. [Google Scholar] [CrossRef]
- Sierra-Sánchez, Á.; Fernández-González, A.; Lizana-Moreno, A.; Espinosa-Ibáñez, O.; Martinez-Lopez, A.; Guerrero-Calvo, J.; Fernández-Porcel, N.; Ruiz-García, A.; Ordóñez-Luque, A.; Carriel, V.; et al. Hyaluronic acid biomaterial for human tissue-engineered skin substitutes: Preclinical comparative in vivo study of wound healing. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2414–2427. [Google Scholar] [CrossRef]
- Asparuhova, M.B.; Chappuis, V.; Stähli, A.; Buser, D.; Sculean, A. Role of hyaluronan in regulating self-renewal and osteogenic differentiation of mesenchymal stromal cells and pre-osteoblasts. Clin. Oral Investig. 2020, 24, 3923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valachová, K.; Šoltés, L. Assessment of the Substance Antioxidative Profile by Hyaluronan, Cu(II) and Ascorbate. Pharmaceutics 2021, 13, 1815. [Google Scholar] [CrossRef] [PubMed]
- Pagnacco, A.; Vangelisti, R.; Erra, C.; Poma, A. Double-blind clinical trial vs. placebo of a new sodium-hyaluronate-based gingival gel. Attual. Ter. Internazionale 1997, 15, 1–7. [Google Scholar]
- Gontiya, G.; Galgali, S.R. Effect of hyaluronan on periodontitis: A clinical and histological study. J. Indian Soc. Periodontol. 2012, 16, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Eick, S.; Renatus, A.; Heinicke, M.; Pfister, W.; Stratul, S.-I.S.; Jentsch, H. Hyaluronic Acid as an Adjunct After Scaling and Root Planing: A Prospective Randomized Clinical Trial. J. Periodontol. 2013, 84, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Bansal, J.; Kedige, S.D.; Anand, S. Hyaluronic acid: A promising mediator for periodontal regeneration. Indian J. Dent. Res. 2010, 21, 575–578. [Google Scholar] [CrossRef] [PubMed]
- Bayer, I.S. Hyaluronic Acid and Controlled Release: A Review. Molecules 2020, 25, 2649. [Google Scholar] [CrossRef]
- Ma, X.; Liu, S.; Tang, H.; Yang, R.; Chi, B.; Ye, Z. In situ photocrosslinked hyaluronic acid and poly (γ-glutamic acid) hydrogels as injectable drug carriers for load-bearing tissue application. J. Biomater. Sci. Polym. Ed. 2018, 29, 2252–2266. [Google Scholar] [CrossRef]
- Malizos, K.; Blauth, M.; Danita, A.; Capuano, N.; Mezzoprete, R.; Logoluso, N.; Drago, L.; Romanò, C.L. Fast-resorbable antibiotic-loaded hydrogel coating to reduce post-surgical infection after internal osteosynthesis: A multicenter randomized controlled trial. J. Orthop. Traumatol. 2017, 18, 159–169. [Google Scholar] [CrossRef] [Green Version]
- Shoham, N.; Sasson, A.L.; Lin, F.H.; Benayahu, D.; Haj-Ali, R.; Gefen, A. The mechanics of hyaluronic acid/adipic acid dihydrazide hydrogel: Towards developing a vessel for delivery of preadipocytes to native tissues. J. Mech. Behav. Biomed. Mater. 2013, 28, 320–331. [Google Scholar] [CrossRef]
- Oliva, F.; Marsilio, E.; Asparago, G.; Frizziero, A.; Berardi, A.C.; Maffulli, N. The impact of hyaluronic acid on tendon physiology and its clinical application in tendinopathies. Cells 2021, 10, 3081. [Google Scholar] [CrossRef]
- Hahn, S.K.; Oh, E.J.; Miyamoto, H.; Shimobouji, T. Sustained release formulation of erythropoietin using hyaluronic acid hydrogels crosslinked by Michael addition. Int. J. Pharm. 2006, 322, 44–51. [Google Scholar] [CrossRef]
- Hsiao, M.Y.; Lin, A.C.; Liao, W.H.; Wang, T.G.; Hsu, C.H.; Chen, W.S.; Lin, F.H. Drug-loaded hyaluronic acid hydrogel as a sustained-release regimen with dual effects in early intervention of tendinopathy. Sci. Rep. 2019, 9, 4784. [Google Scholar] [CrossRef]
- Cristache, C.M.; Totu, E.E.; Petre, D.; Buga, R.; Cristache, G.; Totu, T. Melatonin and Hyaluronic Acid Mixture as a Possible Therapeutic Agent in Dental Medicine. Rev. Chim. Buchar. Orig. Ed. 2018, 69, 1996–1999. [Google Scholar] [CrossRef]
- Cristache, C.M.; Totu, E.E.; Cristache, G.; Nechifor, A.C.; Pintilie, I.I. Melatonin and Hyaluronic Acid in Periodontal Disease. Rev. Chim. 2019, 70, 1089–1093. [Google Scholar] [CrossRef]
- Totu, E.E.; Cristache, C.M.; Buga, R.; Dumitru, F.; Totu, T. A Card Double Face: Compounds’ Functionality and Synergy of a Topical Treatment Proposed for Oral Health Improvement in Periodontal Disease. Rev. Chim. 2019, 70, 1551–1557. [Google Scholar] [CrossRef]
- Cristache, C.M.; Totu, E.E.; Tanase, G.; Nechifor, A.C.; Petre, D.; Burlibasa, M. Innovative Complex Formulation as Topical Treatment for Oral Health Improvment in Periodontal Disease. Rev. Chim. 2019, 70, 2485–2490. [Google Scholar] [CrossRef]
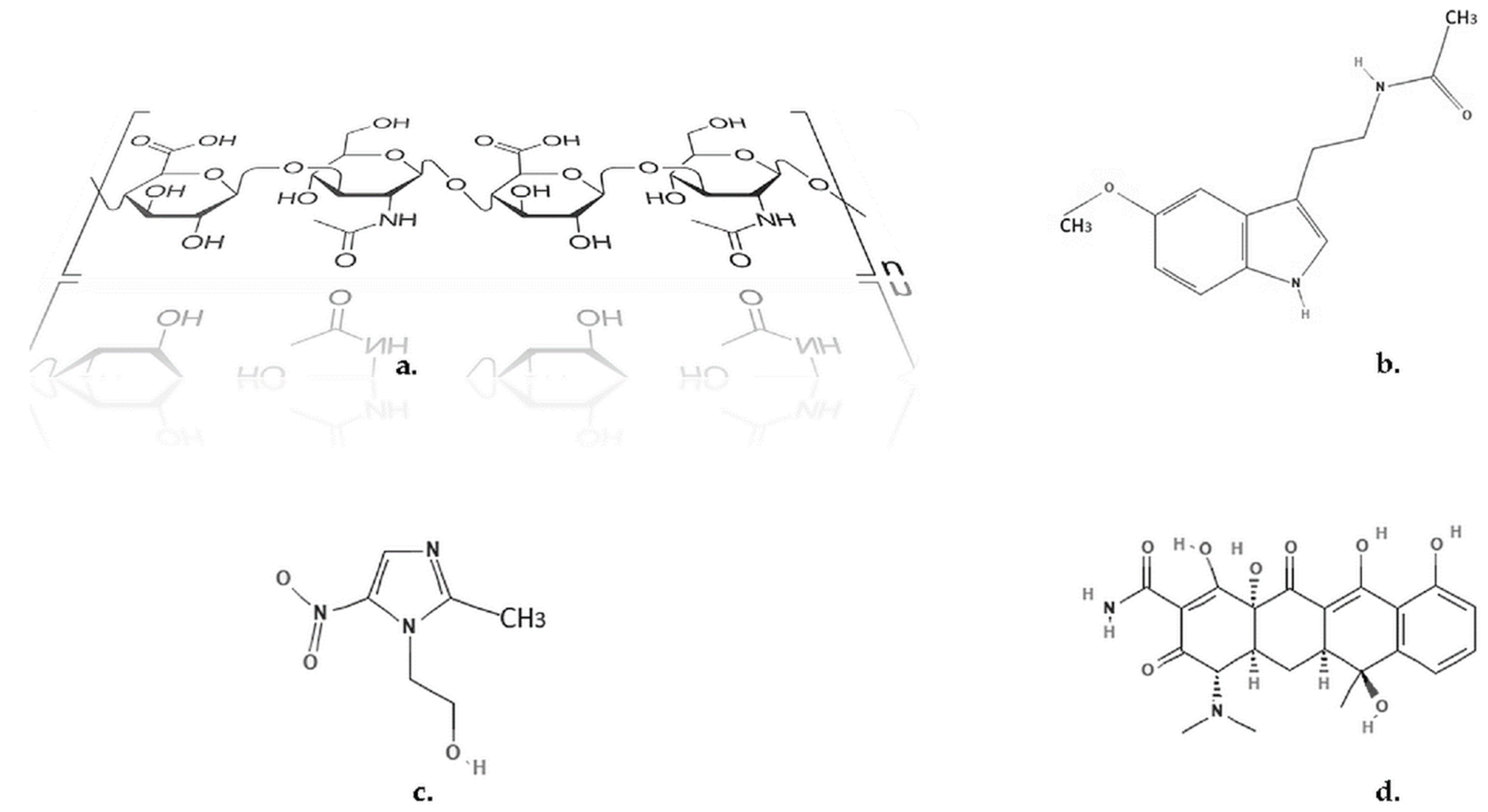
- National Center for Biotechnology Information. PubChem Compound Summary for CID 896, Melatonin. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Melatonin (accessed on 10 February 2022).
- National Center for Biotechnology Information. PubChem Compound Summary for CID 4173, Metronidazole. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Metronidazole (accessed on 10 February 2022).
- National Center for Biotechnology Information. PubChem Compound Summary for CID 54675776, Tetracycline. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Tetracycline (accessed on 10 February 2022).
- Van Meerloo, J.; Kaspers, G.J.L.; Cloos, J. Cell sensitivity assays: The MTT assay. Methods Mol. Biol. 2011, 731, 237–245. [Google Scholar] [CrossRef]
- Othersen, O.G.; Beierlein, F.; Lanig, H.; Clark, T. Conformations and tautomers of tetracycline. J. Phys. Chem. B 2003, 107, 13743–13749. [Google Scholar] [CrossRef]
- Stando, K.; Kasprzyk, P.; Felis, E.; Bajkacz, S. Heterogeneous Photocatalysis of Metronidazole in Aquatic Samples. Molecules 2021, 26, 7612. [Google Scholar] [CrossRef]
- Bickel, M.; Munoz, J.L.; Giovannini, P. Acid-base properties of human gingival crevicular fluid. J. Dent. Res. 1985, 64, 1218–1220. [Google Scholar] [CrossRef]
- Pimenta, A.F.R.; Serro, A.P.; Colaço, R.; Chauhan, A. Optimization of intraocular lens hydrogels for dual drug release: Experimentation and modelling. Eur. J. Pharm. Biopharm. 2019, 141, 51–57. [Google Scholar] [CrossRef]
- Toffoletto, N.; Saramago, B.; Serro, A.P. Therapeutic Ophthalmic Lenses: A Review. Pharmaceutics 2020, 13, 36. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.B.; Jones, S.A. Hyaluronic acid: A unique topical vehicle for the localized delivery of drugs to the skin. J. Eur. Acad. Dermatol. Venereol. 2005, 19, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Korsmeyer, R.W.; Peppas, N.A. Effect of the morphology of hydrophilic polymeric matrices on the diffusion and release of water soluble drugs. J. Memb. Sci. 1981, 9, 211–227. [Google Scholar] [CrossRef]
- Kodavaty, J.; Deshpande, A.P. Evaluation of solute diffusion and polymer relaxation in cross-linked hyaluronic acid hydrogels: Experimental measurement and relaxation modeling. Polym. Bull. 2020, 78, 2605–2626. [Google Scholar] [CrossRef]
- Yotsuyanagi, T.; Higuchi, W.I.; Ghanem, A.H. Theoretical treatment of diffusional transport into and through an oil-water emulsion with an interfacial barrier at the oil-water interface. J. Pharm. Sci. 1973, 62, 40–43. [Google Scholar] [CrossRef]
- Mircioiu, C.; Voicu, V.; Anuta, V.; Tudose, A.; Celia, C.; Paolino, D.; Fresta, M.; Sandulovici, R.; Mircioiu, I. Mathematical Modeling of Release Kinetics from Supramolecular Drug Delivery Systems. Pharmaceutics 2019, 11, 140. [Google Scholar] [CrossRef] [Green Version]
- Vigata, M.; Meinert, C.; Hutmacher, D.W.; Bock, N. Hydrogels as Drug Delivery Systems: A Review of Current Characterization and Evaluation Techniques. Pharmaceutics 2020, 12, 1188. [Google Scholar] [CrossRef]
- Kim, S.J.; Shin, S.R.; Lee, S.M.; Kim, I.Y.; Kim, S.I. Thermal characteristics of polyelectrolyte complexes composed of chitosan and hyaluronic acid. J. Macromol. Sci. Pure Appl. Chem. 2003, 40, 807–815. [Google Scholar] [CrossRef]
- Fukumoto, K.; Yoshizawa, M.; Ohno, H. Room temperature ionic liquids from 20 natural amino acids. J. Am. Chem. Soc. 2005, 127, 2398–2399. [Google Scholar] [CrossRef]
- Singh, G.; Abbas, J.M.; Dogra, S.D.; Sachdeva, R.; Rai, B.; Tripathi, S.K.; Prakash, S.; Sathe, V.; Saini, G.S.S. Vibrational and electronic spectroscopic studies of melatonin. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2014, 118, 73–81. [Google Scholar] [CrossRef]
- Zafra-Roldán, A.; Corona-Avendaño, S.; Montes-Sánchez, R.; Palomar-Pardavé, M.; Romero-Romo, M.; Ramírez-Silva, M.T. New insights on the spectrophotometric determination of melatonin pK a values and melatonin-βCD inclusion complex formation constant. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2018, 190, 442–449. [Google Scholar] [CrossRef]
- Wu, Y. Preparation of low-molecular-weight hyaluronic acid by ozone treatment. Carbohydr. Polym. 2012, 89, 709–712. [Google Scholar] [CrossRef]
- Minaberry, Y.; Chiappetta, D.A.; Sosnik, A.; Jobbágy, M. Micro/nanostructured hyaluronic acid matrices with tuned swelling and drug release properties. Biomacromolecules 2013, 14, 1–9. [Google Scholar] [CrossRef]
- Topal, B.; Çetin Altindal, D.; Gümüsderelioglu, M. Melatonin/HPβCD complex: Microwave synthesis, integration with chitosan scaffolds and inhibitory effects on MG-63CELLS. Int. J. Pharm. 2015, 496, 801–811. [Google Scholar] [CrossRef]
- Yousaf, A.M.; Ramzan, M.; Shahzad, Y.; Mahmood, T.; Jamshaid, M. Fabrication and in vitro characterization of fenofibric acid-loaded hyaluronic acid–polyethylene glycol polymeric composites with enhanced drug solubility and dissolution rate. Int. J. Polym. Mater. Polym. Biomater. 2018, 68, 510–515. [Google Scholar] [CrossRef]
- Kader Sabbagh, H.A.; Hussein-Al-Ali, S.H.; Hussein, M.Z.; Abudayeh, Z.; Ayoub, R.; Abudoleh, S.M. A Statistical Study on the Development of Metronidazole-Chitosan-Alginate Nanocomposite Formulation Using the Full Factorial Design. Polymers 2020, 12, 772. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Kolb, V.M.K.; Jiang, W.T.; Hong, H. FTIR and XRD Investigations of Tetracycline Intercalation in Smectites. Clays Clay Miner. 2010, 58, 462–474. [Google Scholar] [CrossRef]
- Tran, T.H.; Choi, J.Y.; Ramasamy, T.; Truong, D.H.; Nguyen, C.N.; Choi, H.G.; Yong, C.S.; Kim, J.O. Hyaluronic acid-coated solid lipid nanoparticles for targeted delivery of vorinostat to CD44 overexpressing cancer cells. Carbohydr. Polym. 2014, 114, 407–415. [Google Scholar] [CrossRef]
- Dovedytis, M.; Liu, Z.J.; Bartlett, S. Hyaluronic acid and its biomedical applications: A review. Eng. Regen. 2020, 1, 102–113. [Google Scholar] [CrossRef]
- Caccavo, D.; Barba, A.A.; d’Amore, M.; De Piano, R.; Lamberti, G.; Rossi, A.; Colombo, P. Modeling the modified drug release from curved shape drug delivery systems—Dome Matrix®. Eur. J. Pharm. Biopharm. 2017, 121, 24–31. [Google Scholar] [CrossRef]
- Nechifor, G.; Totu, E.E.; Nechifor, A.C.; Isildak, I.; Oprea, O.; Cristache, C.M. Non-resorbable nanocomposite membranes for guided bone regeneration based on polysulfone-quartz fiber grafted with nano-TiO2. Nanomaterials 2019, 9, 985. [Google Scholar] [CrossRef] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Mean Absorbance | % Viability |
|---|---|---|
| 7-HA matrix (0.6 g/mL) | 2.443 ± 0.070 | 132.09 |
| 8-Powder (0.01 g/mL) | 2.112 ± 0.081 | 114.19 |
| Negative control | 1.850 ± 0.033 | 100.00 |
| Positive control | 0.117 ± 0.005 | 6.34 |
| No. | Sample/ AS Concentration µg/mL | Microbial Strains | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Staphylococcus spp. | Streptococcus spp. | ||||||||||
| 2500 | 1250 | 625 | 312.5 | 156.25 | 2500 | 1250 | 625 | 312.5 | 156.25 | ||
| 1 | T, MZ, Soft paraffin | S | S | R | R | R | S | S | S | S | S |
| 2 | MEL, HA, Soft paraffin | S | R | R | R | R | S | R | R | R | R |
| 3 | MEL, HA—solid sample | S | S | S | R | R | S | R | R | R | R |
| 4 | MZ, T, MEL, HA matrix | S | S | S | S | R | S | S | S | S | S |
| 5 | Soft paraffin | S | R | R | R | R | S | R | R | R | R |
| 6 | HA | S | S | R | R | R | R | R | R | R | R |
| 7 | MEL | S | S | S | R | R | S | R | R | R | R |
| 8 | MZ | S | S | R | R | R | S | S | S | R | R |
| 9 | T | S | S | S | S | S | S | S | S | S | S |
| 10 | Control | + | + | + | + | + | + | + | + | + | + |
| Kinetic Model | Parameter | Analyte | ||
|---|---|---|---|---|
| MEL | MZ | T | ||
| Higuchi | k | 3.79 × 10−4 ± 0.84 | 2.26 × 10−4 ± 0.72 | 1.49 × 10−4 ± 0.21 |
| R2 | 0.9892 | 0.9870 | 0.9772 | |
| Korsmeyer–Peppas | k | 2.37 × 10−2 ± 0.14 | 4.36 × 10−2 ± 0.51 | 7.27 × 10−2 ± 0.77 |
| R2 | 0.9843 | 0.9787 | 0.9793 | |
| Pseudo-first-order | k | 1.62 × 10−3 ± 0.35 | 0.88 × 10−3 ± 0.47 | 0.73 × 10−3 ± 0.31 |
| R2 | 0.9976 | 0.9973 | 0.9927 | |
| First-order | k | 2.06 × 10−3 ± 0.49 | 0.66 × 10−3 ± 0.55 | 0.60 × 10−3 ± 0.14 |
| R2 | 0.9338 | 0.8847 | 0.9339 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eftimie Totu, E.; Mănuc, D.; Totu, T.; Cristache, C.M.; Buga, R.-M.; Erci, F.; Cristea, C.; Isildak, I. Considerations on the Controlled Delivery of Bioactive Compounds through Hyaluronic Acid Membrane. Membranes 2022, 12, 303. https://doi.org/10.3390/membranes12030303
Eftimie Totu E, Mănuc D, Totu T, Cristache CM, Buga R-M, Erci F, Cristea C, Isildak I. Considerations on the Controlled Delivery of Bioactive Compounds through Hyaluronic Acid Membrane. Membranes. 2022; 12(3):303. https://doi.org/10.3390/membranes12030303
Chicago/Turabian StyleEftimie Totu, Eugenia, Daniela Mănuc, Tiberiu Totu, Corina Marilena Cristache, Roxana-Mădălina Buga, Fatih Erci, Camelia Cristea, and Ibrahim Isildak. 2022. "Considerations on the Controlled Delivery of Bioactive Compounds through Hyaluronic Acid Membrane" Membranes 12, no. 3: 303. https://doi.org/10.3390/membranes12030303
APA StyleEftimie Totu, E., Mănuc, D., Totu, T., Cristache, C. M., Buga, R. -M., Erci, F., Cristea, C., & Isildak, I. (2022). Considerations on the Controlled Delivery of Bioactive Compounds through Hyaluronic Acid Membrane. Membranes, 12(3), 303. https://doi.org/10.3390/membranes12030303