
The Peritoneal Membrane—A Potential Mediator of Fibrosis and Inflammation among Heart Failure Patients on Peritoneal Dialysis

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Dialytic Procedure
3. Peritoneum
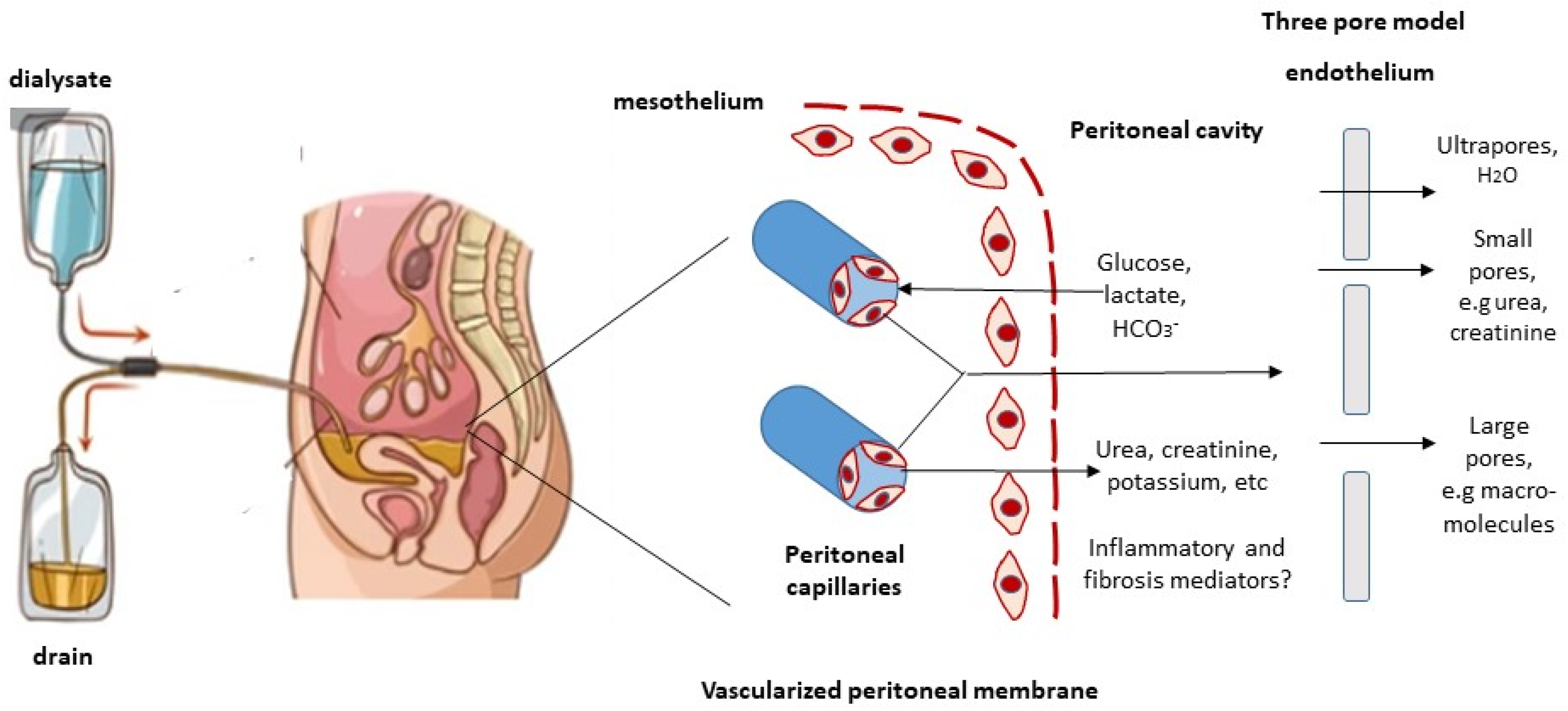
4. Peritoneal Transport
4.1. The Three-Pore Model
4.2. Removal of Middle Molecules and Protein-Bound Solutes
5. Molecular and Genetic Studies
6. Peritoneal Membrane Preservation
6.1. Glucose-Sparing Strategies
6.2. Encapsulating Peritoneal Sclerosis
7. Peritoneal Dialysis in Congestive Heart Failure
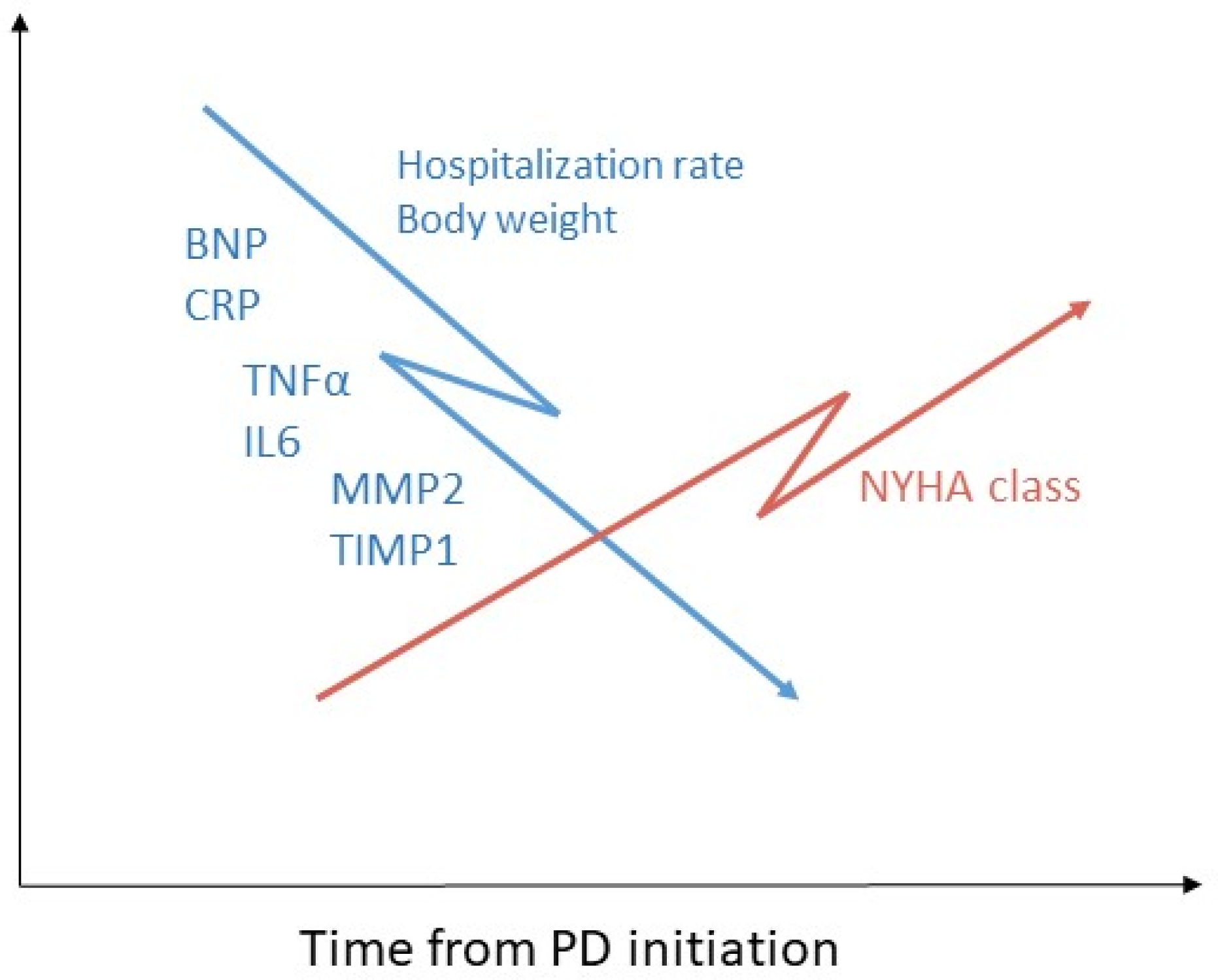
7.1. Inflammation
7.2. Fibrosis
8. Conclusions and Future Research
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cho, Y.; Bello, A.K.; Levin, A.; Lunney, M.; Osman, M.A.; Ye, F.; Ashuntantang, G.E.; Bellorin-Font, E.; Gharbi, M.B.; Davison, S.N.; et al. Peritoneal dialysis use and practice patterns: An international survey study. Am. J. Kidney Dis. 2021, 77, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, R.; Devuyst, O.; Davies, S.J.; Johnson, D.W. The current state of peritoneal dialysis. J. Am. Soc. Nephrol. 2016, 27, 3238–3252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, P.K.-T.; Chow, K.M.; Van de Luijtgaarden, M.W.M.; Jager, K.J.; Mehrotra, R.; Naicker, S.; Pecoits-Filho, R.; Yu, X.Q.; Lameire, N. Changes in the worldwide epidemiology of peritoneal dialysis. Nat. Rev. Nephrol. 2017, 13, 90–103. [Google Scholar] [CrossRef] [PubMed]
- Tam, P. Peritoneal dialysis and preservation of residual renal function. Perit. Dial. Int. 2009, 29, S108–S110. [Google Scholar] [CrossRef]
- Van Biesen, W.; Verbeke, F.; Vanholder, R. Cardiovascular disease in haemo-dialysis and peritoneal dialysis: Arguments pro peritoneal dialysis. Nephrol. Dial. Transpl. 2007, 22, 53–584. [Google Scholar] [CrossRef] [Green Version]
- Theofilou, P. Quality of Life in Patients Undergoing Hemodialysis or Peritoneal Dialysis Treatment. J. Clin. Med. Res. 2011, 3, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Crabtree, J.H.; Burchette, R.J. Effective use of laparoscopy for long-term peritoneal dialysis access. Am. J. Surg. 2009, 198, 135–141. [Google Scholar] [CrossRef]
- Heaf, J.G.; Wehberg, S. Relative survival of peritoneal dialysis and haemodialysis patients: Effect of cohort and mode of dialysis initiation. PLoS ONE 2014, 9, e90119. [Google Scholar] [CrossRef] [Green Version]
- Mehrotra, R.; Chiu, Y.-W.; Kalantar-Zadeh, K.; Bargman, J.; Vonesh, E. Similar outcomes with hemodialysis and peritoneal dialysis in patients with end-stage renal disease. Arch. Intern. Med. 2011, 171, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Ryu, J.-H.; Kim, H.; Kim, K.H.; Hann, H.J.; Ahn, H.S.; Lee, S.; Kim, S.-J.; Kang, D.-H.; Choi, K.B.; Ryu, D.-R. Improving survival rate of Korean patients initiating dialysis. Yonsei Med. J. 2015, 56, 666–675. [Google Scholar] [CrossRef] [Green Version]
- van de Luijtgaarden, M.W.M.; Jager, K.J.; Segelmark, M.; Pascual, J.; Collart, F.; Hemke, A.C.; Remón, C.; Metcalfe, W.; Miguel, A.; Kramar, R.; et al. Trends in dialysis modality choice and related patient survival in the ERA-EDTA Registry over a 20-year period. Nephrol. Dial. Transplant. 2016, 31, 120–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purnell, T.S.; Auguste, P.; Crews, D.C.; Lamprea-Montealegre, J.; Olufade, T.; Greer, R.; Ephraim, P.; Sheu, J.; Kostecki, D.; Powe, N.R.; et al. Comparison of life participation activities among adults treated by hemodialysis, peritoneal dialysis, and kidney transplantation: A systematic review. Am. J. Kidney Dis. 2013, 62, 953–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zazzeroni, L.; Pasquinelli, G.; Nanni, E.; Cremonini, V.; Rubbi, I. Comparison of quality of life in patients undergoing hemodialysis and peritoneal dialysis: A systematic review and meta-analysis. Kidney Blood Press. Res. 2017, 42, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Blake, P.G.; Daugirdas, J.T. Physiology of peritoneal dialysis. In Handbook of Dialysis, 5th ed.; Daugirdas, J.T., Blake, P.G., Ing, T.S., Eds.; Wolters Kluwer Health: Philadelphia, PA, USA, 2015; pp. 392–407. [Google Scholar]
- Flessner, M.F. Small-solute transport across specific peritoneal tissue surfaces in the rat. J. Am. Soc. Nephrol. 1996, 7, 225. [Google Scholar] [CrossRef]
- Di Paolo, N.; Sacchi, G. Atlas of peritoneal histology. Perit. Dial. Int. 2000, 20, S5–S96. [Google Scholar]
- Teitelbaum, I. Peritoneal dialysis. N. Engl. J. Med. 2021, 385, 1786–1795. [Google Scholar] [CrossRef]
- Flessner, M.F. The transport barrier in intraperitoneal therapy. Am. J. Physiol. Ren. Physiol. 2005, 288, F433–F442. [Google Scholar] [CrossRef]
- Rippe, B.; Haraldsson, B. Fluid and protein fluxes across small and large pores in the microvasculature. Application of two-pore equations. Acta Physiol. Scand. 1987, 131, 411–428. [Google Scholar] [CrossRef]
- Rippe, B.; Venturoli, D.; Simonsen, O.; de Arteaga, J. Fluid and electrolyte transport across the peritoneal membrane during CAPD according to the three-pore model. Perit. Dial. Int. 2004, 24, 10–27. [Google Scholar] [CrossRef]
- Davies, S.J.; Mushahar, L.; Yu, Z.; Lambie, M. Determinants of peritoneal membrane function over time. Semin. Nephrol. 2011, 31, 172–182. [Google Scholar] [CrossRef]
- Finkelstein, F.; Healy, H.; Abu-Alfa, A.; Ahmad, S.; Brown, F.; Gehr, T.; Nash, K.; Sorkin, M.; Mujais, S. Superiority of icodextrin compared with 4.25% dextrose for peritoneal ultrafiltration. J. Am. Soc. Nephrol. 2005, 16, 546–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkie, M.E.; Plant, M.J.; Edwards, L.; Brown, C.B. Icodextrin 7.5% dialysate solution (glucose polymer) in patients with ultrafiltration failure: Extension of CAPD technique survival. Perit. Dial. Int. 1997, 17, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Davies, S.J.; Woodrow, G.; Donovan, K.; Plum, J.; Williams, P.; Johansson, A.C.; Bosselmann, H.P.; Heimbürger, O.; Simonsen, O.; Davenport, A.; et al. Icodextrin improves the fluid status of peritoneal dialysis patients: Results of a double-blind randomized controlled trial. J. Am. Soc. Nephrol. 2003, 14, 2338–2344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Y.; Johnson, D.W.; Badve, S.; Craig, J.C.; Strippoli, G.F.; Wiggins, K.J. Impact of icodextrin on clinical outcomes in peritoneal dialysis: A systematic review of randomized controlled trials. Nephrol. Dial. Transplant. 2013, 28, 1899–1907. [Google Scholar] [CrossRef] [Green Version]
- Li, P.K.; Culleton, B.F.; Ariza, A.; Do, J.Y.; Johnson, D.W.; Sanabria, M.; Shockley, T.R.; Story, K.; Vatazin, A.; Verrelli, M.; et al. Randomized, controlled trial of glucose-sparing peritoneal dialysis in diabetic patients. J. Am. Soc. Nephrol. 2013, 24, 1889–1900. [Google Scholar] [CrossRef] [Green Version]
- Davies, S.J.; Brown, E.A.; Frandsen, N.E.; Rodrigues, A.S.; Rodriguez-Carmona, A.; Vychytil, A.; Macnamara, E.; Ekstrand, A.; Tranaeus, A.; Filho, J.C.; et al. Longitudinal membrane function in functionally anuric patients treated with APD: Data from EAPOS on the effects of glucose and icodextrin prescription. Kidney Int. 2005, 67, 1609–1615. [Google Scholar] [CrossRef] [Green Version]
- Venturoli, D.; Rippe, B. Transport asymmetry in peritoneal dialysis: Application of a serial heteroporous peritoneal membrane model. Am. J. Physiol. Ren. Physiol. 2001, 280, F599–F606. [Google Scholar] [CrossRef]
- Renkin, E.M. Relation of capillary morphology to transport of fluid and large molecules: A review. Acta Physiol. Scand. Suppl. 1979, 463, 81. [Google Scholar]
- Struijk, D.G.; Krediet, R.T.; Koomen, G.C.; Boeschoten, E.W.; vd Reijden, H.J.; Arisz, L. Indirect measurement of lymphatic absorption with inulin in continuous ambulatory peritoneal dialysis (CAPD) patients. Perit. Dial. Int. 1990, 10, 141. [Google Scholar] [CrossRef]
- Krediet, R.T.; Struijk, D.G.; Koomen, G.C.; Hoek, F.J.; Arisz, L. The disappearance of macromolecules from the peritoneal cavity during continuous ambulatory peritoneal dialysis (CAPD) is not dependent on molecular size. Perit. Dial. Int. 1990, 10, 147. [Google Scholar] [CrossRef]
- Bammens, B.; Evenepoel, P.; Verbeke, K.; Vanrenterghem, Y. Removal of middle molecules and protein-bound solutes by peritoneal dialysis and relation with uremic symptoms. Kidney Int. 2003, 64, 2238–2243. [Google Scholar] [CrossRef]
- Kim, D.J.; Do, J.H.; Huh, W.; Oh, H.Y. Dissociation between clearances of small and middle molecules in incremental peritoneal dialysis. Perit. Dial. Int. 2001, 21, 462–466. [Google Scholar] [CrossRef] [PubMed]
- Asano, M.; Ishii, T.; Hirayama, A.; Mizuno, M.; Suzuki, Y.; Sakata, F.; Akiyama, S.; Maruyama, S.; Soga, T.; Kinashi, H.; et al. Differences in peritoneal solute transport rates in peritoneal dialysis. Clin. Exp. Nephrol. 2019, 23, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Lai, K.N.; Lam, M.F.; Leung, J.C.; Chan, L.Y.; Lam, C.W.; Chan, I.H.; Chan, H.W.; Li, C.S.; Wong, S.S.; Ho, Y.W.; et al. A study of the clinical and biochemical profile of peritoneal dialysis fluid low in glucose degradation products. Perit. Dial. Int. 2012, 32, 280–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zemel, D.; Imholz, A.L.; de Waart, D.R.; Dinkla, C.; Struijk, D.G.; Krediet, R.T. Appearance of tumor necrosis factor-alpha and soluble TNF-receptors I and II in peritoneal effluent of CAPD. Kidney Int. 1994, 46, 1422–1430. [Google Scholar] [CrossRef] [Green Version]
- Karl, Z.J.T.; Khanna, O.N.R.; Leonor, B.F.P.; Moore, H.L.; Nielsen, M.P. Peritoneal equilibration test. Perit. Dial. Int. 1987, 7, 138. [Google Scholar] [CrossRef]
- Brown, E.A.; Davies, S.J.; Rutherford, P.; Meeus, F.; Borras, M.; Riegel, W.; Filho, J.C.D.; Vonesh, E.; van Bree, M.; EAPOS Group. Survival of functionally anuric patients on automated peritoneal dialysis: The European APD Outcome Study. J. Am. Soc. Nephrol. 2003, 14, 2948–2957. [Google Scholar] [CrossRef] [Green Version]
- Brimble, K.S.; Walker, M.; Margetts, P.J.; Kundhal, K.K.; Rabbat, C.G. Meta-analysis: Peritoneal membrane transport, mortality, and technique failure in peritoneal dialysis. J. Am. Soc. Nephrol. 2006, 17, 2591–2598. [Google Scholar] [CrossRef] [Green Version]
- Morelle, J.; Stachowska-Pietka, J.; Öberg, C.; Gadola, L.; la Milia, V.; Yu, Z.; Lambie, M.; Mehrotra, R.; de Arteaga, J.; Davies, S. ISPD recommendations for the evaluation of peritoneal membrane dysfunction in adults: Classification, measurement, interpretation and rationale for intervention. Perit. Dial. Int. 2021, 41, 352–372. [Google Scholar] [CrossRef]
- Mehrotra, R.; Stanaway, I.B.; Jarvik, G.P.; Lambie, M.; Morelle, J.; Perl, J.; Himmelfarb, J.; Heimburger, O.; Johnson, D.W.; Imam, T.H.; et al. A genome-wide association study suggests correlations of common genetic variants with peritoneal solute transfer rates in patients with kidney failure receiving peritoneal dialysis. Kidney Int. 2021, 100, 1101–1111. [Google Scholar] [CrossRef]
- Morelle, J.; Marechal, C.; Yu, Z.; Debaix, H.; Corre, T.; Lambie, M.; Verduijn, M.; Dekker, F.; Bovy, P.; Evenepoel, P.; et al. AQP1 Promoter Variant, Water Transport, and Outcomes in Peritoneal Dialysis. N. Engl. J. Med. 2021, 385, 1570–1580. [Google Scholar] [CrossRef] [PubMed]
- Devuyst, O. Assessing transport across the peritoneal membrane: Precision medicine in dialysis. Perit. Dial. Int. 2021, 41, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Schricker, S.; Oberacker, T.; Fritz, P.; Ketteler, M.; Alscher, M.D.; Schanz, M. Peritoneal expression of SGLT-2, GLUT1 and GLUT3 in peritoneal dialysis patients. Kidney Blood Press. Res. 2022, 47, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Shi, Y.; Tao, M.; Zhuang, S.; Liu, N. Peritoneal fibrosis and epigenetic modulation. Perit. Dial. Int. 2021, 41, 168–178. [Google Scholar] [CrossRef]
- Holmes, C.; Mujais, S. Glucose spating in peritoneal dialysis: Implications and metrics. Kidney Int. Suppl. 2006, 103, S104–S109. [Google Scholar] [CrossRef] [Green Version]
- Pannekeet, M.M.; Imholz, A.L.; Struijk, D.G.; Koomen, G.C.; Langedijk, M.J.; Schouten, N.; de Waart, R.; Hiralall, J.; Krediet, R.T. The standard peritoneal permeability analysis: A tool for the assessment of peritoneal permeability characteristics in CAPD patients. Kidney Int. 1995, 48, 866. [Google Scholar] [CrossRef] [Green Version]
- Mehrotra, R.; Ravel, V.; Streja, E.; Kuttykrishnan, S.; Adams, S.V.; Katz, R.; Molnar, M.Z.; Kalantar-Zadeh, K. Peritoneal Equilibration Test and Patient Outcomes. Clin. J. Am. Soc. Nephrol. 2015, 10, 1990–2001. [Google Scholar] [CrossRef] [Green Version]
- Paniagua, R.; Ventura, M.-d.-J.; Avila-Díaz, M.; Cisneros, A.; Vicenté-Martínez, M.; Furlong, M.-D.-C.; García-González, Z.; Villanueva, D.; Orihuela, O.; Prado-Uribe, M.-D.-C.; et al. Icodextrin improves fluid and metabolic management in high and high-average transport patientds. Perit. Dial. Int. 2009, 29, 32–42. [Google Scholar] [CrossRef]
- Freida, P.; Wilkie, M.; Jenkins, S.; Dallas, F.; Issad, B. The contribution of combined crystalloid and colloid osmosis to fluid and sodium management in peritoneal dialysis. Kidney Int. 2008, 73, S102–S111. [Google Scholar] [CrossRef] [Green Version]
- Bonomini, M.; Masola, V.; Procino, G.; Zammit, V.; Divino-Filho, J.; Arduini, A.; Gambaro, G. How to Improve the Biocompatibility of Peritoneal Dialysis Solutions (without Jeopardizing the Patient’s Health). Int. J. Mol. Sci. 2021, 22, 7955. [Google Scholar] [CrossRef]
- Rago, C.; Lombardi, T.; Di Fulvio, G.; Di Liberato, L.; Arduini, A.; Divino-Filho, J.; Bonomini, M. A New Peritoneal Dialysis Solution Containing L-Carnitine and Xylitol for Patients on Continuous Ambulatory Peritoneal Dialysis: First Clinical Experience. Toxins 2021, 13, 174. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.J.; Yang, S.Y.; Wu, I.W.; Hsu, K.-H.; Sun, C.-Y.; Chen, C.-Y.; Lee, C.-C. Encapsulating peritoneal sclerosis in long-termed peritoneal dialysis patients. Biomed. Res. Int. 2018, 2018, 8250589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, B.; Bartosova, M.; Macher-Goeppinger, S.; Sallay, P.; Vörös, P.; Ranchin, B.; Vondrak, K.; Ariceta, G.; Zaloszyc, A.; Bayazit, A.K.; et al. Neutral pH and low–glucose degradation product dialysis fluids induce major early alterations of the peritoneal membrane in children on peritoneal dialysis. Kidney Int. 2018, 94, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Davies, S.J.; Phillips, L.; Griffiths, A.M.; Russell, L.H.; Naish, P.F.; Russell, G.I. What really happens to people on long-term peritoneal dialysis? Proc. Kidney Int. 1998, 54, 2207–2217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.M.; Yang, W.X. Epithelial-to-mesenchymal transition in the development of endometriosis. Oncotarget 2017, 8, 41679–41689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honda, K.; Oda, H. Pathology of encapsulating peritoneal sclerosis. Perit. Dial. Int. 2005, 25, S19–S29. [Google Scholar] [CrossRef] [PubMed]
- Augustine, T.; Brown, P.W.; Davies, S.D.; Summers, A.M.; Wilkie, M.E. Encapsulating peritoneal sclerosis: Clinical significance and implications. Nephron. Clin. Pract. 2009, 111, 149–154. [Google Scholar] [CrossRef]
- Brown, E.A.; Bargman, J.; van Biesen, W.; Chang, M.Y.; Finkelstein, F.O.; Hurst, H.; Johnson, D.W.; Kawanishi, H.; Lambie, M.; de Moraes, T.P.; et al. Length of Time on Peritoneal Dialysis and Encapsulating Peritoneal Sclerosis—Position Paper for ISPD: 2017 Update. Perit. Dial. Int. 2017, 37, 362. [Google Scholar] [CrossRef]
- Barreto, D.L.; Sampimon, D.E.; Struijk, D.G.; Krediet, R.T. Early Detection of Imminent Encapsulating Peritoneal Sclerosis: Free Water Transport, Selected Effluent Proteins, or Both? Perit. Dial. Int. 2019, 39, 83. [Google Scholar] [CrossRef]
- Sajwani, S.H.; Bargman, J.M. Novel ways to preserve the peritoneal membrane. Adv. Perit. Dial. 2012, 28, 37–41. [Google Scholar]
- Korte, M.R.; Yo, M.; Betjes, M.G.; Fieren, M.W.; van Saase, J.C.; Boer, W.H.; Weimar, W.; Zietse, R. Increasing incidence of severe encapsulating peritoneal sclerosis after kidney transplantation. Nephrol. Dial Transplant. 2007, 22, 2412–2414. [Google Scholar] [CrossRef] [PubMed]
- Fieren, M.W.; Betjes, M.G.; Korte, M.R.; Boer, W.H. Posttransplant encapsulating peritoneal sclerosis: A worrying new trend? Perit. Dial. Int. 2007, 27, 619. [Google Scholar] [CrossRef] [PubMed]
- Pecoits-Filho, R.; Carvalho, M.J.; Stenvinkel, P.; Lindholm, B.; Heimbürger, O. Systemic and intraperitoneal interleukin-6 system during the first year of peritoneal dialysis. Perit. Dial. Int. 2006, 26, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.Y.H.; Szeto, C.C.; Szeto, C.Y.K.; Lai, K.B.; Chow, K.M.; Li, P.K.T. Association of ENOS polymorphism with basal peritoneal membrane function in uremic patients. Am. J. Kidney Dis. 2003, 42, 781–786. [Google Scholar] [CrossRef]
- Gillerot, G.; Goffin, E.; Michel, C.; Evenepoel, P.; Van Biesen, W.; Tintillier, M.; Stenvinkel, P.; Heimbürger, O.; Lindholm, B.; Nordfors, L.; et al. Genetic and clinical factors influence the baseline permeability of the peritoneal membrane. Kidney Int. 2005, 67, 2477–2487. [Google Scholar] [CrossRef]
- Nakamoto, H. Encapsulating peritoneal sclerosis—A clinician’s approach to diagnosis and medical treatment. Perit. Dial. Int. 2005, 25, S30–S38. [Google Scholar] [CrossRef]
- Hamada, C.; Tomino, Y. Recent Understanding of Peritoneal Pathology in Peritoneal Dialysis Patients in Japan. Blood Purif. 2021, 50, 719–728. [Google Scholar] [CrossRef]
- Tarzi, R.M.; Lim, A.; Moser, S.; Ahmad, S.; George, A.; Balasubramaniam, G.; Clutterbuck, E.J.; Gedroyc, W.; Brown, E.A. Assessing the validity of an abdominal CT scoring system in the diagnosis of encapsulating peritoneal sclerosis. Clin. J. Am. Soc. Nephrol. 2008, 3, 1702. [Google Scholar] [CrossRef] [Green Version]
- Kawanishi, K.; Honda, K.; Tsukada, M.; Oda, H.; Nitta, K. Neutral solution low in glucose degradation products is associated with less peritoneal fibrosis and vascular sclerosis in patients receiving peritoneal dialysis. Perit. Dial. Int. 2013, 33, 242–251. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, M.; Miyazaki, M.; Honda, K.; Kasai, K.; Tomo, T.; Nakamoto, H.; Kawanishi, H. Encapsulating peritoneal sclerosis in the era of a multi-disciplinary approach based on biocompatible solutions: The NEXT-PD study. Perit. Dial. Int. 2014, 34, 766–774. [Google Scholar] [CrossRef] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- François, K.; Ronco, C.; Bargman, J.M. Peritoneal Dialysis for Chronic Congestive Heart Failure. Blood Purif. 2015, 40, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Kunin, M.; Carmon, V.; Arad, M.; Levin-Iaina, N.; Freimark, D.; Holtzman, E.J.; .Dinour, D. Inflammatory biomarkers in refractory congestive heart failure patients treated with peritoneal dialysis. Biomed. Res. Int. 2015, 2015, 590851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selby, N.M.; McIntyre, C.W. Peritoneal dialysis is not associated with myocardial stunning. Perit. Dial. Int. J. Int. Soc. 2011, 31, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Cnossen, T.T.; Kooman, J.P.; Konings, C.J.A.M.; Uszko-Lencer, N.H.M.K.; Leunissen, K.M.L.; van der Sande, F.M. Peritoneal dialysis in patients with primary cardiac failure complicated by renal failure. Blood Purif. 2010, 30, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, J.E.; Ortega, T.; Rodriguez, C.; Diaz-Molina, B.; Martin, M.; Garcia-Cueto, C.; Vidau, P.; Gago, E.; Ortega, F. Efficacy of peritoneal ultrafiltration in the treatment of refractory congestive heart failure. Nephrol. Dial Transpl. 2010, 25, 605–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sotirakopoulos, N.G.; Kalogiannidou, I.M.; Tersi, M.E.; Mavromatidis, K.S. Peritoneal dialysis for patients suffering from severe heart failure. Clin. Nephrol. 2011, 76, 124–129. [Google Scholar] [CrossRef]
- Kunin, M.; Arad, M.; Dinour, D.; Freimark, D.; Holtzman, E.J. Peritoneal Dialysis in Patients with Refractory Congestive Heart Failure: Potential Prognostic Factors. Blood Purif. 2013, 35, 285–294. [Google Scholar] [CrossRef]
- Kunin, M.; Klempfner, R.; Beckerman, P.; Rott, D.; Dinour, D. Congestive heart failure treated with peritoneal dialysis or hemodialysis: Typical patient profile and outcomes in real-world setting. Int. J. Clin. Pract. 2021, 75, e13727. [Google Scholar] [CrossRef]
- Cheetham, M.S.; Cho, Y.; Krishnasamy, R.; Jain, A.K.; Boudville, N.; Johnson, D.; Huang, L.L. Incremental Versus Standard (Full-Dose) Peritoneal Dialysis. Kidney Int. Rep. 2022, 7, 165–176. [Google Scholar] [CrossRef]
- Kunin, M.; Mini, S.; Abu-Amer, N.; Beckerman, P. Regular at-home abdominal paracentesis via Tenckhoff catheter in patients with refractory congestive heart failure. Int. J. Clin. Pract. 2021, 75, e14924. [Google Scholar] [CrossRef] [PubMed]
- Mullens, W.; Abrahams, Z.; Francis, G.S.; Taylor, D.O.; Starling, R.C.; Tang, W. Prompt Reduction in Intra-Abdominal Pressure Following Large-Volume Mechanical Fluid Removal Improves Renal Insufficiency in Refractory Decompensated Heart Failure. J. Card. Fail. 2008, 14, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Polese, A.; Magrini, F.; Fiorentini, C.; Olivari, M.T. Negative influences of ascites on the cardiac function of cirrhotic patients. Am. J. Med. 1975, 59, 165–170. [Google Scholar] [CrossRef]
- Mann, D.L. Inflammatory mediators and the failing heart: Past, present, and the foreseeable future. Circ. Res. 2002, 91, 988–998. [Google Scholar] [CrossRef] [PubMed]
- Pecoits-Filho, R.; Stenvinkel, P.; Wang, A.Y.; Heimburger, O.; Lindholm, B. Chronic inflammation in peritoneal dialysis: The search for the holy grail? Perit. Dial. Int. 2004, 24, 327–339. [Google Scholar] [CrossRef]
- Fiaccadori, E.; Regolisti, G.; Maggiore, U.; Parenti, E.; Cremaschi, E.; Detrenis, S.; Caiazza, A.; Cabassi, A. Ultrafiltration in heart failure. Am. Heart J. 2011, 161, 439–449. [Google Scholar] [CrossRef]
- Takawale, A.; Sakamuri, S.S.; Kassiri, Z. Extracellular matrix communication and turnover in cardiac physiology and pathology. Compr. Physiol. 2015, 5, 687–719. [Google Scholar]
- Quilliot, D.; Alla, F.; Bohme, P.; Bruntz, J.-F.; Hammadi, M.; Dousset, B.; Ziegler, O.; Zannad, F. Myocardial collagen turnover in normotensive obese patients: Relation to insulin resistance. Int. J. Obes. 2005, 29, 1321–1328. [Google Scholar] [CrossRef]
- Kunin, M.; Carmon, V.; Beckerman, P.; Dinour, D. Effect of Peritoneal Dialysis on Serum Fibrosis Biomarkers in Patients with Refractory Congestive Heart Failure. Int. J. Mol. Sci. 2019, 20, 2610. [Google Scholar] [CrossRef] [Green Version]
- Funck, R.C.; Wilke, A.; Rupp, H.; Brilla, C.G. Regulation and role of myocardial collagen matrix remodeling in hypertensive heart disease. Adv. Exp. Med. Biol. 1997, 432, 35–44. [Google Scholar]
- Chua, C.C.; Hamdy, R.C.; Cha, B.H. Angiotensin II induces TIMP-1 production in rat heart endothelial cells. Biochim. Biophys. Acta 1996, 1311, 175–180. [Google Scholar] [CrossRef] [Green Version]
- Varo, N.; Iraburu, M.J.; Varela, M.; Lopez, B.; Etayo, J.C.; Diez, J. Chronic AT1 blockade stimulates extracellular collagen type I degradation and reverses myocardial fibrosis in spontaneously hypertensive rats. Hypertension 2000, 35, 1197–11202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murtha, L.A.; Schullga, M.J.; Mabotuwana, N.S.; Hardy, S.A.; Waters, D.W.; Burgess, J.K.; Knight, D.A.; Boyle, A.J. The Processes and Mechanisms of Cardiac and Pulmonary Fibrosis. Front. Physiol. 2017, 8, 777. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kunin, M.; Beckerman, P. The Peritoneal Membrane—A Potential Mediator of Fibrosis and Inflammation among Heart Failure Patients on Peritoneal Dialysis. Membranes 2022, 12, 318. https://doi.org/10.3390/membranes12030318
Kunin M, Beckerman P. The Peritoneal Membrane—A Potential Mediator of Fibrosis and Inflammation among Heart Failure Patients on Peritoneal Dialysis. Membranes. 2022; 12(3):318. https://doi.org/10.3390/membranes12030318
Chicago/Turabian StyleKunin, Margarita, and Pazit Beckerman. 2022. "The Peritoneal Membrane—A Potential Mediator of Fibrosis and Inflammation among Heart Failure Patients on Peritoneal Dialysis" Membranes 12, no. 3: 318. https://doi.org/10.3390/membranes12030318
APA StyleKunin, M., & Beckerman, P. (2022). The Peritoneal Membrane—A Potential Mediator of Fibrosis and Inflammation among Heart Failure Patients on Peritoneal Dialysis. Membranes, 12(3), 318. https://doi.org/10.3390/membranes12030318