
MiR-126 Is an Independent Predictor of Long-Term All-Cause Mortality in Patients with Type 2 Diabetes Mellitus

 , ,
, ,  ,
,  ,
,  ,
, 
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Endpoints
2.3. RNA Preparation and Detection and Quantification of miRNAs by Quantitative PCR
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
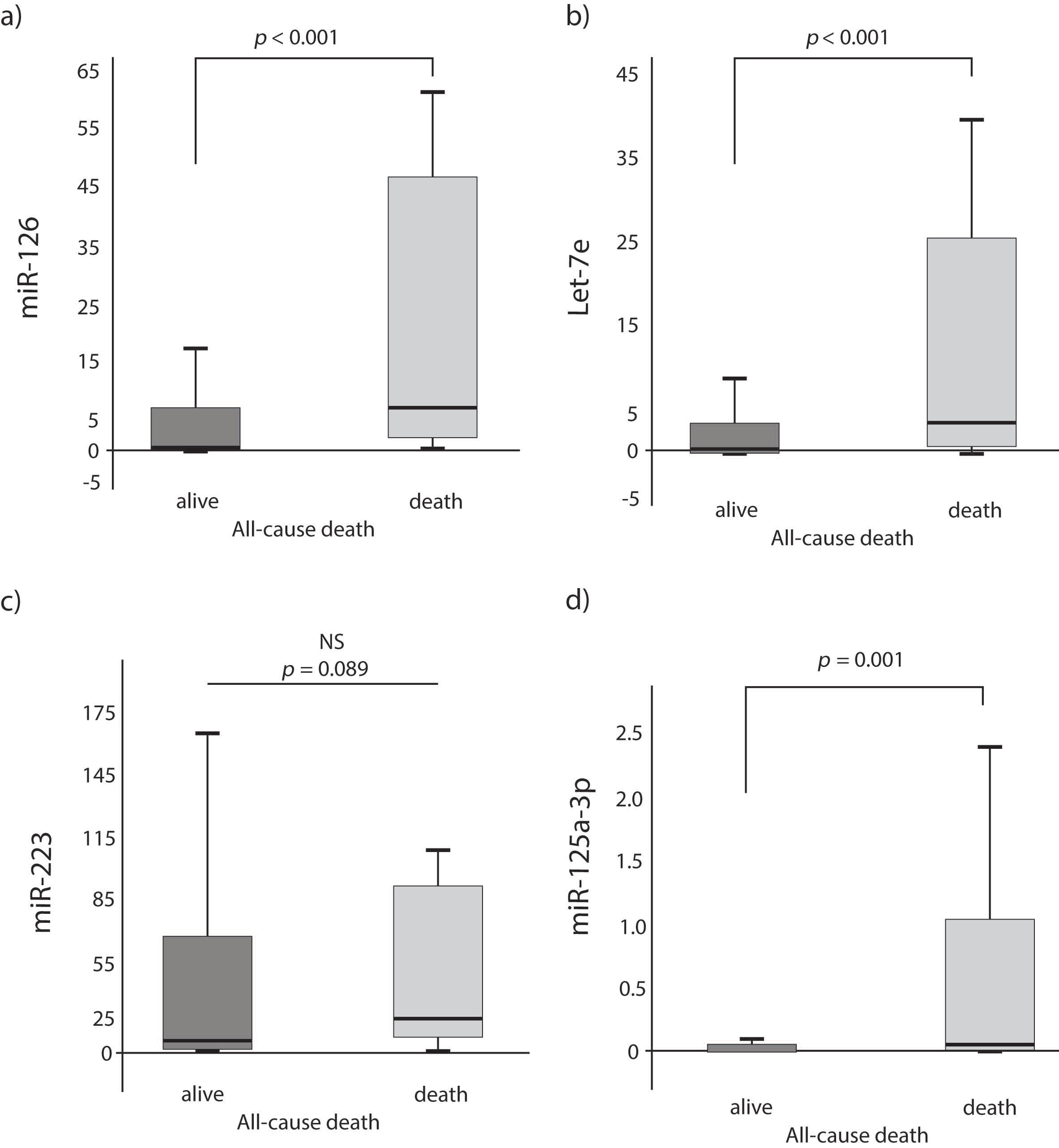
3.2. Circulating miRNA Levels Predict Long-Term All-Cause Death
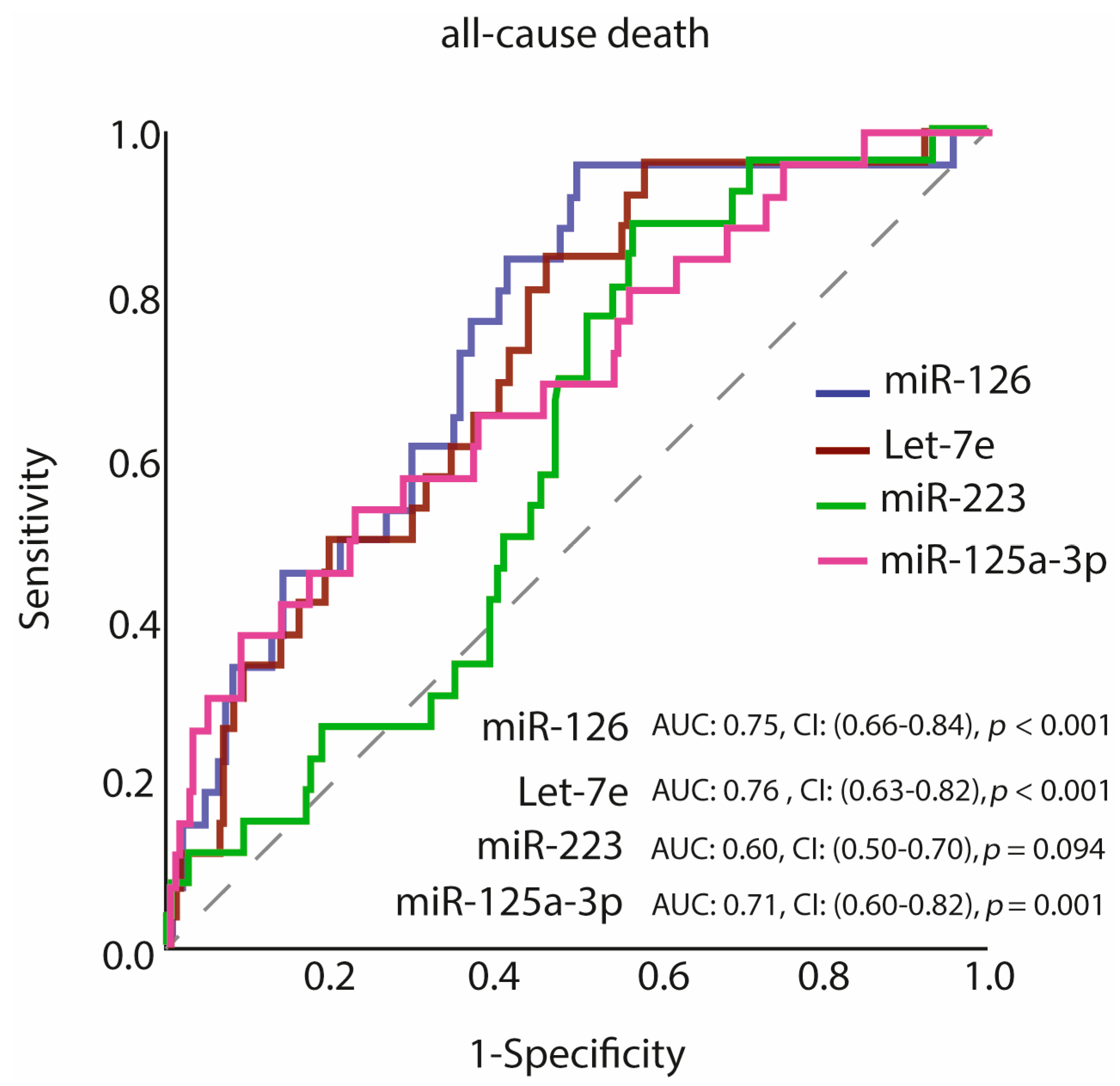
3.3. Predictive Value of miR-126, Let-7e, miR-223 and miR-125a-3p of Long-Term All-Cause Mortality
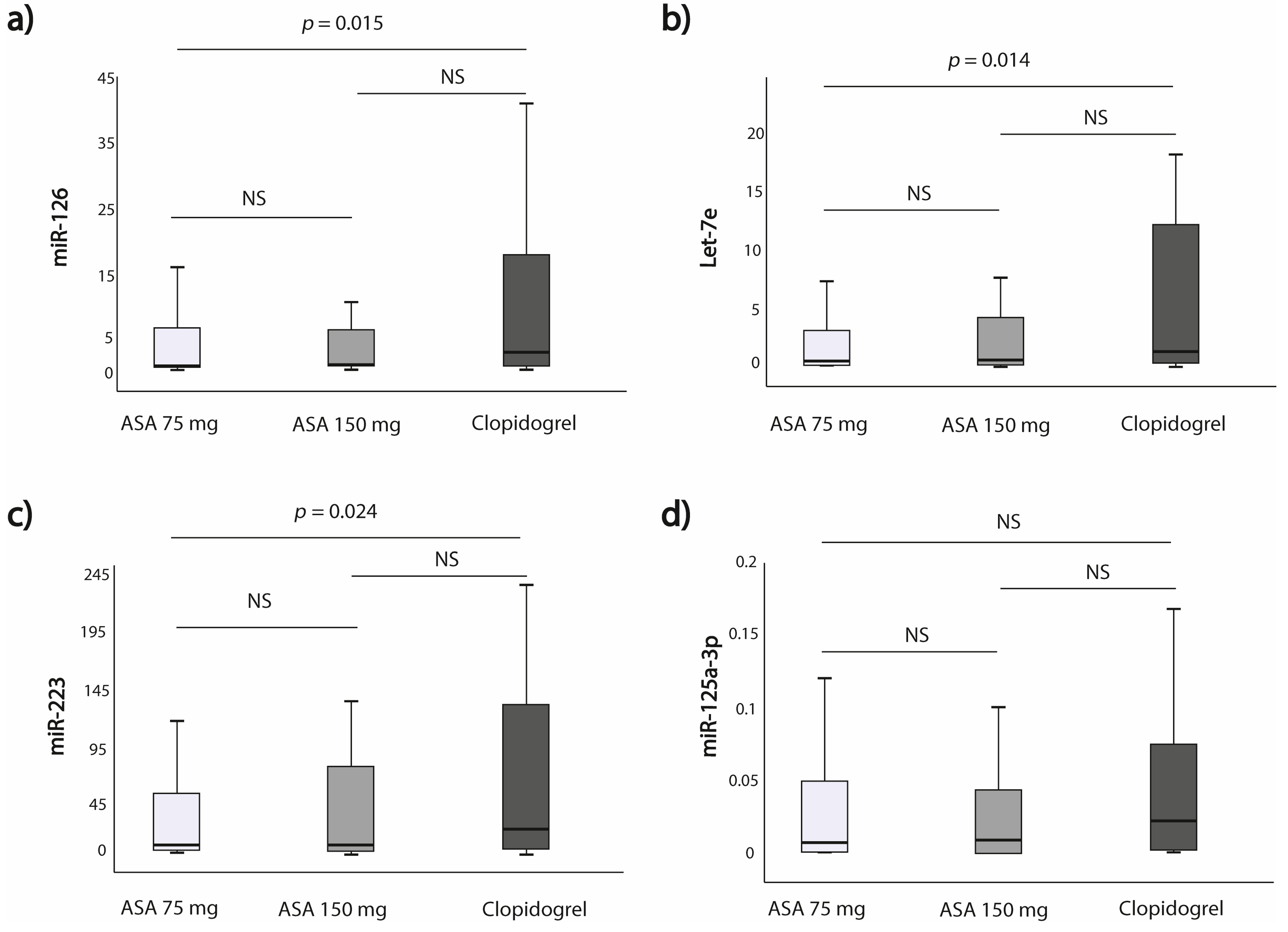
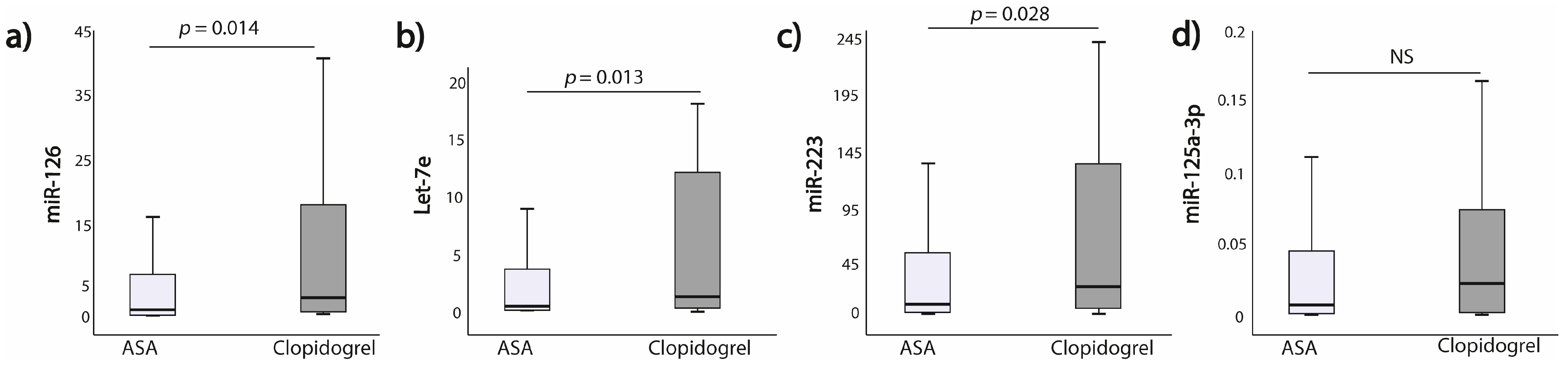
3.4. Expression of miRNAs According to the Allocation to the Antiplatelet Treatment Strategy
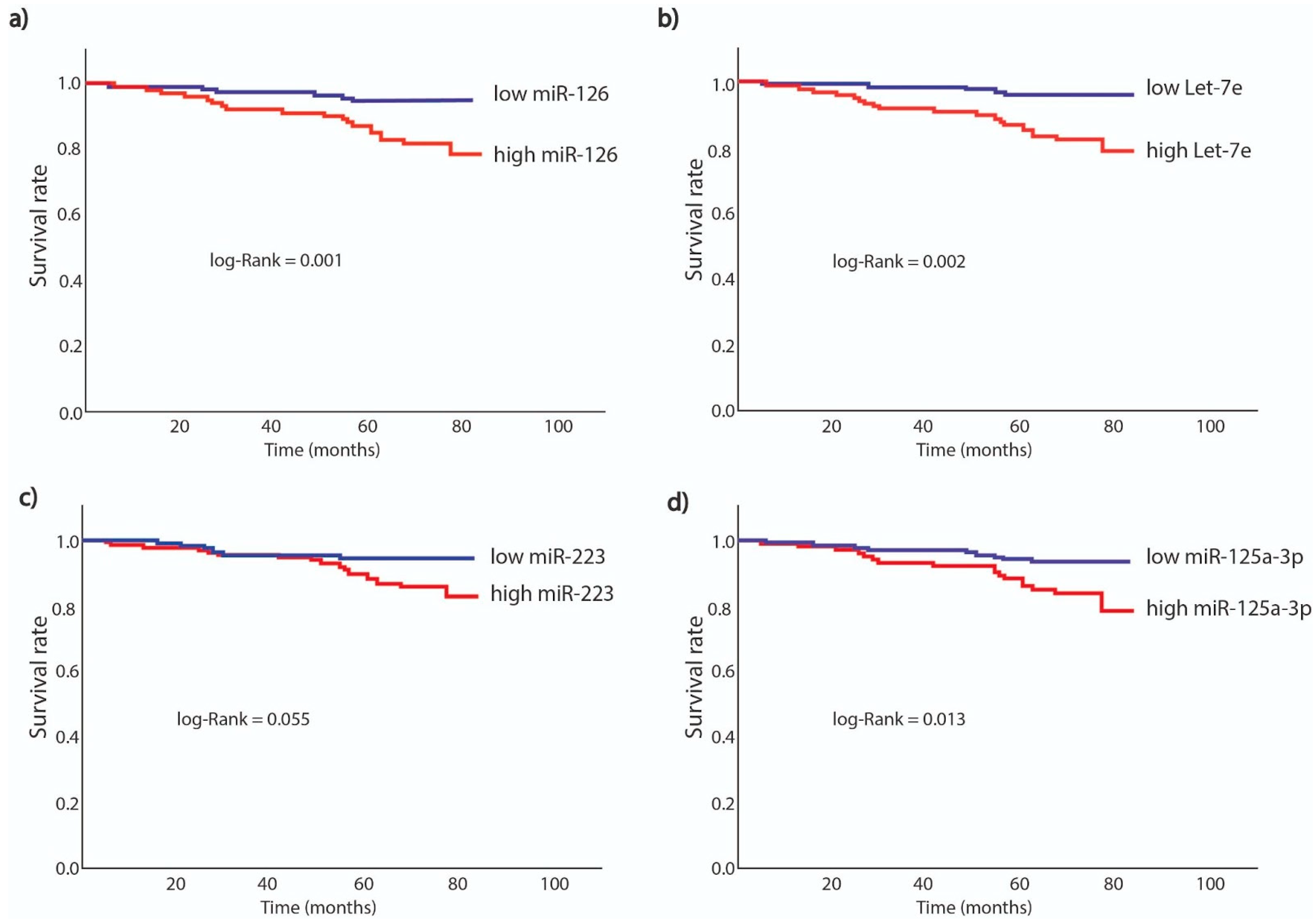
3.5. Survival Analysis According to miRNAs Expression
4. Discussion
5. Conclusions
6. Study Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Vaidya, V.; Gangan, N.; Sheehan, J. Impact of Cardiovascular Complications among Patients with Type 2 Diabetes Mellitus: A Systematic Review. Expert Rev. Pharm. Outcomes Res. 2015, 15, 487–497. [Google Scholar] [CrossRef]
- Pretorius, L.; Thomson, G.J.A.; Adams, R.C.M.; Nell, T.A.; Laubscher, W.A.; Pretorius, E. Platelet Activity and Hypercoagulation in Type 2 Diabetes. Cardiovasc. Diabetol. 2018, 17, 141. [Google Scholar] [CrossRef] [Green Version]
- Postula, M.; Janicki, P.K.; Eyileten, C.; Rosiak, M.; Kaplon-Cieslicka, A.; Sugino, S.; Wilimski, R.; Kosior, D.A.; Opolski, G.; Filipiak, K.J.; et al. Next-Generation Re-Sequencing of Genes Involved in Increased Platelet Reactivity in Diabetic Patients on Acetylsalicylic Acid. Platelets 2016, 27, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Postula, M.; Janicki, P.K.; Rosiak, M.; Kaplon-Cieslicka, A.; Trzepla, E.; Filipiak, K.J.; Kosior, D.A.; Czlonkowski, A.; Opolski, G. New Single Nucleotide Polymorphisms Associated with Differences in Platelets Reactivity in Patients with Type 2 Diabetes Treated with Acetylsalicylic Acid: Genome-Wide Association Approach and Pooled DNA Strategy. J. Thromb. Thrombolysis 2013, 36, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Postula, M.; Kaplon-Cieslicka, A.; Rosiak, M.; Kondracka, A.; Serafin, A.; Filipiak, K.J.; Czlonkowski, A.; Opolski, G.; Janicki, P.K. Genetic Determinants of Platelet Reactivity during Acetylsalicylic Acid Therapy in Diabetic Patients: Evaluation of 27 Polymorphisms within Candidate Genes. J. Thromb. Haemost. 2011, 9, 2291–2301. [Google Scholar] [CrossRef]
- Beckman, J.A.; Creager, M.A.; Libby, P. Diabetes and Atherosclerosis: Epidemiology, Pathophysiology, and Management. JAMA 2002, 287, 2570–2581. [Google Scholar] [CrossRef] [PubMed]
- Pordzik, J.; Jakubik, D.; Jarosz-Popek, J.; Wicik, Z.; Eyileten, C.; De Rosa, S.; Indolfi, C.; Siller-Matula, J.M.; Czajka, P.; Postula, M. Significance of Circulating microRNAs in Diabetes Mellitus Type 2 and Platelet Reactivity: Bioinformatic Analysis and Review. Cardiovasc. Diabetol. 2019, 18, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Natarajan, A.; Zaman, A.G.; Marshall, S.M. Platelet Hyperactivity in Type 2 Diabetes: Role of Antiplatelet Agents. Diab. Vasc. Dis. Res. 2008, 5, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.; Rao, X.; Zhong, J. Role of T Lymphocytes in Type 2 Diabetes and Diabetes-Associated Inflammation. J. Diabetes Res. 2017, 2017, 6494795. [Google Scholar] [CrossRef]
- Dangwal, S.; Thum, T. MicroRNAs in Platelet Biogenesis and Function. Thromb. Haemost. 2012, 108, 599–604. [Google Scholar] [CrossRef]
- De Rosa, S.; Indolfi, C. Circulating microRNAs as Biomarkers in Cardiovascular Diseases. Exp. Suppl. 2015, 106, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.A.; Baxter, D.H.; Zhang, S.; Huang, D.Y.; Huang, K.H.; Lee, M.J.; Galas, D.J.; Wang, K. The microRNA Spectrum in 12 Body Fluids. Clin. Chem. 2010, 56, 1733–1741. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.A.; Ludwig, R.G.; Garcia-Martin, R.; Brandão, B.B.; Kahn, C.R. Extracellular miRNAs: From Biomarkers to Mediators of Physiology and Disease. Cell Metab. 2019, 30, 656–673. [Google Scholar] [CrossRef] [PubMed]
- Fish, J.E.; Santoro, M.M.; Morton, S.U.; Yu, S.; Yeh, R.-F.; Wythe, J.D.; Ivey, K.N.; Bruneau, B.G.; Stainier, D.Y.R.; Srivastava, D. miR-126 Regulates Angiogenic Signaling and Vascular Integrity. Dev. Cell 2008, 15, 272–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayés-Genis, A.; Lanfear, D.E.; de Ronde, M.W.J.; Lupón, J.; Leenders, J.J.; Liu, Z.; Zuithoff, N.P.A.; Eijkemans, M.J.C.; Zamora, E.; De Antonio, M.; et al. Prognostic Value of Circulating microRNAs on Heart Failure-Related Morbidity and Mortality in Two Large Diverse Cohorts of General Heart Failure Patients. Eur. J. Heart Fail. 2018, 20, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Willeit, P.; Zampetaki, A.; Dudek, K.; Kaudewitz, D.; King, A.; Kirkby, N.S.; Crosby-Nwaobi, R.; Prokopi, M.; Drozdov, I.; Langley, S.R.; et al. Circulating microRNAs as Novel Biomarkers for Platelet Activation. Circ. Res. 2013, 112, 595–600. [Google Scholar] [CrossRef] [Green Version]
- Shi, R.; Zhou, X.; Ji, W.-J.; Zhang, Y.-Y.; Ma, Y.-Q.; Zhang, J.-Q.; Li, Y.-M. The Emerging Role of miR-223 in Platelet Reactivity: Implications in Antiplatelet Therapy. Biomed. Res. Int. 2015, 2015, 981841. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Lin, F.-Y.; Lin, Y.-W.; Cheng, S.-M.; Chang, C.-C.; Lin, R.-H.; Chuang, C.-L.; Sheu, J.-S.; Chen, S.-M.; Tsai, C.-S. Platelet MicroRNA 365-3p Expression Correlates with High On-Treatment Platelet Reactivity in Coronary Artery Disease Patients. Cardiovasc. Drugs Ther. 2019, 33, 129–137. [Google Scholar] [CrossRef]
- Yu, X.-Y.; Chen, J.-Y.; Zheng, Z.-W.; Wu, H.; Li, L.-W.; Zhang, Z.-W.; Chen, Z.-H.; Lin, Q.-X.; Han, Y.-L.; Zhong, S.-L. Plasma miR-126 as a Potential Marker Predicting Major Adverse Cardiac Events in Dual Antiplatelet-Treated Patients after Percutaneous Coronary Intervention. EuroIntervention 2013, 9, 546–554. [Google Scholar] [CrossRef]
- Stojkovic, S.; Wadowski, P.P.; Haider, P.; Weikert, C.; Pultar, J.; Lee, S.; Eichelberger, B.; Hengstenberg, C.; Wojta, J.; Panzer, S.; et al. Circulating MicroRNAs and Monocyte–Platelet Aggregate Formation in Acute Coronary Syndrome. Thromb. Haemost. 2021. [Google Scholar] [CrossRef]
- Kaudewitz, D.; Skroblin, P.; Bender, L.H.; Barwari, T.; Willeit, P.; Pechlaner, R.; Sunderland, N.P.; Willeit, K.; Morton, A.C.; Armstrong, P.C.; et al. Association of MicroRNAs and YRNAs With Platelet Function. Circ. Res. 2016, 118, 420–432. [Google Scholar] [CrossRef]
- Wang, Z.; Xia, L.; Xu, Q.; Ji, Q.; Yao, Z.; Lv, Q. MiR-223 Levels Predicting Perioperative Bleeding in off-Pump Coronary Artery Bypass Grafting. Ann. Transl. Med. 2020, 8, 1341. [Google Scholar] [CrossRef]
- Carino, A.; De Rosa, S.; Sorrentino, S.; Polimeni, A.; Sabatino, J.; Caiazzo, G.; Torella, D.; Spaccarotella, C.; Mongiardo, A.; Strangio, A.; et al. Modulation of Circulating MicroRNAs Levels during the Switch from Clopidogrel to Ticagrelor. Biomed Res. Int. 2016, 2016, 3968206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benoit, C.; Ould-Hamouda, H.; Crepin, D.; Gertler, A.; Amar, L.; Taouis, M. Early Leptin Blockade Predisposes Fat-Fed Rats to Overweight and Modifies Hypothalamic microRNAs. J. Endocrinol. 2013, 218, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Bai, Y.; Liu, Y.; Wilfried Noel, S.; Yan, Q.; Pham Thi, H.; Sun, X.; Wei, W.; Ma, J.; Zheng, F. Plasma Exosomal miRNAs Involved in Endothelial Injury in Microscopic Polyangiitis Patients. FASEB J. 2020, 34, 6215–6228. [Google Scholar] [CrossRef] [Green Version]
- Deiuliis, J.A. MicroRNAs as Regulators of Metabolic Disease: Pathophysiologic Significance and Emerging Role as Biomarkers and Therapeutics. Int. J. Obes. 2016, 40, 88–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostrowska, M.; Kubica, J.; Adamski, P.; Kubica, A.; Eyileten, C.; Postula, M.; Toma, A.; Hengstenberg, C.; Siller-Matula, J.M. Stratified Approaches to Antiplatelet Therapies Based on Platelet Reactivity Testing. Front. Cardiovasc. Med. 2019, 6, 176. [Google Scholar] [CrossRef] [Green Version]
- Rosiak, M.; Postula, M.; Kaplon-Cieslicka, A.; Kondracka, A.; Trzepla, E.; Czlonkowski, A.; Janicki, P.K.; Filipiak, K.J.; Opolski, G. Effect of ASA Dose Doubling versus Switching to Clopidogrel on Plasma Inflammatory Markers Concentration in Patients with Type 2 Diabetes and High Platelet Reactivity: The AVOCADO Study. Cardiol. J. 2013, 20, 545–551. [Google Scholar] [CrossRef] [Green Version]
- Eyileten, C.; Zaremba, M.; Janicki, P.K.; Rosiak, M.; Cudna, A.; Kapłon-Cieślicka, A.; Opolski, G.; Filipiak, K.J.; Kosior, D.A.; Mirowska-Guzel, D.; et al. Serum Brain-Derived Neurotrophic Factor Is Related to Platelet Reactivity but Not to Genetic Polymorphisms within BDNF Encoding Gene in Patients with Type 2 Diabetes. Med. Sci. Monit. 2016, 22, 69–76. [Google Scholar] [CrossRef]
- Kapłon-Cieślicka, A.; Tymińska, A.; Rosiak, M.; Ozierański, K.; Peller, M.; Eyileten, C.; Kondracka, A.; Pordzik, J.; Mirowska-Guzel, D.; Opolski, G.; et al. Resistin Is a Prognostic Factor for Death in Type 2 Diabetes. Diabetes. Metab. Res. Rev. 2019, 35, e3098. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction (2018). Glob. Heart 2018, 13, 305–338. [Google Scholar] [CrossRef] [PubMed]
- Hicks, K.A.; Mahaffey, K.W.; Mehran, R.; Nissen, S.E.; Wiviott, S.D.; Dunn, B.; Solomon, S.D.; Marler, J.R.; Teerlink, J.R.; Farb, A.; et al. 2017 Cardiovascular and Stroke Endpoint Definitions for Clinical Trials. Circulation 2018, 137, 961–972. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, S.; Eposito, F.; Carella, C.; Strangio, A.; Ammirati, G.; Sabatino, J.; Abbate, F.G.; Iaconetti, C.; Liguori, V.; Pergola, V.; et al. Transcoronary Concentration Gradients of Circulating microRNAs in Heart Failure. Eur. J. Heart Fail. 2018, 20, 1000–1010. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, R.; De Rosa, S.; Leistner, D.; Boeckel, J.-N.; Keller, T.; Fichtlscherer, S.; Dimmeler, S.; Zeiher, A.M. Transcoronary Concentration Gradient of microRNA-133a and Outcome in Patients With Coronary Artery Disease. Am. J. Cardiol. 2017, 120, 15–24. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Capodanno, D.; Danchin, N.; Simon, T.; Bergmeijer, T.O.; Ten Berg, J.M.; Sibbing, D.; Price, M.J. Derivation, Validation, and Prognostic Utility of a Prediction Rule for Nonresponse to Clopidogrel: The ABCD-GENE Score. JACC Cardiovasc. Interv. 2020, 13, 606–617. [Google Scholar] [CrossRef]
- Zampetaki, A.; Kiechl, S.; Drozdov, I.; Willeit, P.; Mayr, U.; Prokopi, M.; Mayr, A.; Weger, S.; Oberhollenzer, F.; Bonora, E.; et al. Plasma microRNA Profiling Reveals Loss of Endothelial miR-126 and Other microRNAs in Type 2 Diabetes. Circ. Res. 2010, 107, 810–817. [Google Scholar] [CrossRef]
- Mayer, O., Jr.; Seidlerová, J.; Černá, V.; Kučerová, A.; Vaněk, J.; Karnosová, P.; Bruthans, J.; Wohlfahrt, P.; Cífková, R.; Pešta, M.; et al. The Low Expression of Circulating microRNA-19a Represents an Additional Mortality Risk in Stable Patients with Vascular Disease. Int. J. Cardiol. 2019, 289, 101–106. [Google Scholar] [CrossRef]
- Schulte, C.; Molz, S.; Appelbaum, S.; Karakas, M.; Ojeda, F.; Lau, D.M.; Hartmann, T.; Lackner, K.J.; Westermann, D.; Schnabel, R.B.; et al. miRNA-197 and miRNA-223 Predict Cardiovascular Death in a Cohort of Patients with Symptomatic Coronary Artery Disease. PLoS ONE 2015, 10, e0145930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.; Yuan, Y.; Cho, J.-H.; McClarty, S.; Baxter, D.; Galas, D.J. Comparing the MicroRNA Spectrum between Serum and Plasma. PLoS ONE 2012, 7, e41561. [Google Scholar] [CrossRef] [PubMed]
- de Boer, H.C.; van Solingen, C.; Prins, J.; Duijs, J.M.G.J.; Huisman, M.V.; Rabelink, T.J.; van Zonneveld, A.J. Aspirin Treatment Hampers the Use of Plasma microRNA-126 as a Biomarker for the Progression of Vascular Disease. Eur. Heart J. 2013, 34, 3451–3457. [Google Scholar] [CrossRef]
- Witkowski, M.; Tabaraie, T.; Steffens, D.; Friebel, J.; Dörner, A.; Skurk, C.; Witkowski, M.; Stratmann, B.; Tschoepe, D.; Landmesser, U.; et al. MicroRNA-19a Contributes to the Epigenetic Regulation of Tissue Factor in Diabetes. Cardiovasc. Diabetol. 2018, 17, 34. [Google Scholar] [CrossRef]
- Witkowski, M.; Weithauser, A.; Tabaraie, T.; Steffens, D.; Kränkel, N.; Witkowski, M.; Stratmann, B.; Tschoepe, D.; Landmesser, U.; Rauch-Kroehnert, U. Micro-RNA-126 Reduces the Blood Thrombogenicity in Diabetes Mellitus via Targeting of Tissue Factor. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 1263–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plé, H.; Landry, P.; Benham, A.; Coarfa, C.; Gunaratne, P.H.; Provost, P. The Repertoire and Features of Human Platelet microRNAs. PLoS ONE 2012, 7, e50746. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Ge, J.; Wang, Z.; Ren, J.; Wang, X.; Xiong, H.; Gao, J.; Zhang, Y.; Zhang, Q. Let-7e Modulates the Inflammatory Response in Vascular Endothelial Cells through ceRNA Crosstalk. Sci. Rep. 2017, 7, 42498. [Google Scholar] [CrossRef]
- Maués, J.H.D.S.; Aquino Moreira-Nunes, C.D.F.; Rodriguez Burbano, R.M. MicroRNAs as a Potential Quality Measurement Tool of Platelet Concentrate Stored in Blood Banks—A Review. Cells 2019, 8, 1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavarretta, E.; Chiariello, G.A.; Condorelli, G. Platelets, Endothelium, and Circulating microRNA-126 as a Prognostic Biomarker in Cardiovascular Diseases: Per Aspirin Ad Astra. Eur. Heart J. 2013, 34, 3400–3402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Rosa, S.; Fichtlscherer, S.; Lehmann, R.; Assmus, B.; Dimmeler, S.; Zeiher, A.M. Transcoronary Concentration Gradients of Circulating microRNAs. Circulation 2011, 124, 1936–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, L.; Liu, J.; Qin, L.; Liu, J.; Xi, S.; Lu, C.; Yin, T. Interaction between Platelet-Derived microRNAs and CYP2C19*2 Genotype on Clopidogrel Antiplatelet Responsiveness in Patients with ACS. Thromb. Res. 2017, 157, 97–102. [Google Scholar] [CrossRef]
- Parker, W.A.E.; Schulte, C.; Barwari, T.; Phoenix, F.; Pearson, S.M.; Mayr, M.; Grant, P.J.; Storey, R.F.; Ajjan, R.A. Aspirin, Clopidogrel and Prasugrel Monotherapy in Patients with Type 2 Diabetes Mellitus: A Double-Blind Randomised Controlled Trial of the Effects on Thrombotic Markers and microRNA Levels. Cardiovasc. Diabetol. 2020, 19, 3. [Google Scholar] [CrossRef]
- Chyrchel, B.; Totoń-Żurańska, J.; Kruszelnicka, O.; Chyrchel, M.; Mielecki, W.; Kołton-Wróż, M.; Wołkow, P.; Surdacki, A. Association of Plasma miR-223 and Platelet Reactivity in Patients with Coronary Artery Disease on Dual Antiplatelet Therapy: A Preliminary Report. Platelets 2015, 26, 593–597. [Google Scholar] [CrossRef]
- Xie, W.; Yin, Q.; Zhang, M.; Li, S.; Chen, S. Leukocyte miR-223-3p Is Not Associated with Altered Platelet Responses to Clopidogrel in Patients with Coronary Artery Disease. Zhong Nan Da Xue Xue Bao Yi Xue Ban. J. Cent. South Univ. Med. Sci. 2018, 43, 421–427. [Google Scholar] [CrossRef]
- Maitrias, P.; Metzinger-Le Meuth, V.; Massy, Z.A.; M’Baya-Moutoula, E.; Reix, T.; Caus, T.; Metzinger, L. MicroRNA Deregulation in Symptomatic Carotid Plaque. J. Vasc. Surg. 2015, 62, 1245–1250. [Google Scholar] [CrossRef] [Green Version]
- Hijmans, J.G.; Levy, M.A.; Garcia, V.; Lincenberg, G.M.; Diehl, K.J.; Greiner, J.J.; Stauffer, B.L.; DeSouza, C.A. Insufficient Sleep Is Associated with a pro-Atherogenic Circulating microRNA Signature. Exp. Physiol. 2019, 104, 975–982. [Google Scholar] [CrossRef] [PubMed]
- Bhatlekar, S.; Manne, B.K.; Basak, I.; Edelstein, L.C.; Tugolukova, E.; Stoller, M.L.; Cody, M.J.; Morley, S.C.; Nagalla, S.; Weyrich, A.S.; et al. miR-125a-5p Regulates Megakaryocyte Proplatelet Formation Via the Actin Bundling Protein L-Plastin. Blood 2020. [Google Scholar] [CrossRef] [PubMed]
- Villmann, J.-M.; Burkhardt, R.; Teren, A.; Villmann, T.; Thiery, J.; Drogies, T. Atherosclerosis, Myocardial Infarction and Primary Hemostasis: Impact of Platelets, von Willebrand Factor and Soluble Glycoprotein VI. Thromb. Res. 2019, 180, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Sangkuhl, K.; Klein, T.E.; Altman, R.B. Clopidogrel Pathway. Pharmacogenet. Genomics 2010, 20, 463–465. [Google Scholar] [CrossRef]
- Pereira, N.L.; Rihal, C.S.; So, D.Y.F.; Rosenberg, Y.; Lennon, R.J.; Mathew, V.; Goodman, S.G.; Weinshilboum, R.M.; Wang, L.; Baudhuin, L.M.; et al. Clopidogrel Pharmacogenetics. Circ. Cardiovasc. Interv. 2019, 12, e007811. [Google Scholar] [CrossRef] [PubMed]
- Brandt, J.T.; Close, S.L.; Iturria, S.J.; Payne, C.D.; Farid, N.A.; Ernest, C.S., 2nd; Lachno, D.R.; Salazar, D.; Winters, K.J. Common Polymorphisms of CYP2C19 and CYP2C9 Affect the Pharmacokinetic and Pharmacodynamic Response to Clopidogrel but Not Prasugrel. J. Thromb. Haemost. 2007, 5, 2429–2436. [Google Scholar] [CrossRef]
- Grines, C.L.; Marshall, J.J. Short DAPT after DES: P2Y12 Monotherapy Is In, Aspirin Is Out! Eur. Heart J. 2019, 40, 2605–2606. [Google Scholar] [CrossRef]
- Vranckx, P.; Valgimigli, M.; Jüni, P.; Hamm, C.; Steg, P.G.; Heg, D.; van Es, G.A.; McFadden, E.P.; Onuma, Y.; van Meijeren, C.; et al. Ticagrelor plus Aspirin for 1 Month, Followed by Ticagrelor Monotherapy for 23 Months vs Aspirin plus Clopidogrel or Ticagrelor for 12 Months, Followed by Aspirin Monotherapy for 12 Months after Implantation of a Drug-Eluting Stent: A Multicentre, Open-Label, Randomised Superiority Trial. Lancet 2018, 392, 940–949. [Google Scholar] [CrossRef]
- Hahn, J.-Y.; Song, Y.B.; Oh, J.-H.; Chun, W.J.; Park, Y.H.; Jang, W.J.; Im, E.-S.; Jeong, J.-O.; Cho, B.R.; Oh, S.K.; et al. Effect of P2Y12 Inhibitor Monotherapy vs Dual Antiplatelet Therapy on Cardiovascular Events in Patients Undergoing Percutaneous Coronary Intervention: The SMART-CHOICE Randomized Clinical Trial. JAMA 2019, 321, 2428–2437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehran, R.; Baber, U.; Sharma, S.K.; Cohen, D.J.; Angiolillo, D.J.; Briguori, C.; Cha, J.Y.; Collier, T.; Dangas, G.; Dudek, D.; et al. Ticagrelor with or without Aspirin in High-Risk Patients after PCI. N. Engl. J. Med. 2019, 381, 2032–2042. [Google Scholar] [CrossRef] [PubMed]
- Guedeney, P.; Mesnier, J.; Sorrentino, S.; Abcha, F.; Zeitouni, M.; Lattuca, B.; Silvain, J.; De Rosa, S.; Indolfi, C.; Collet, J.-P.; et al. Early Aspirin Discontinuation Following Acute Coronary Syndrome or Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. Res. 2020, 9, 680. [Google Scholar] [CrossRef] [Green Version]
- Michelson, A.D. Methods for the Measurement of Platelet Function. Am. J. Cardiol. 2009, 103, 20A–26A. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Demographics | Overall 252 (100%) | Patients Who Died * (N = 26) | Patients Who Survived * (N = 226) | p |
|---|---|---|---|---|
| Age (years) mean ± SD | 67.1 ± 8.5 | 70.52 ± 1.80 | 66.61 ± 0.60 | 0.019 |
| Sex (female) n (%) | 117 (46%) | 111 (49%) | 6 (23%) | 0.012 |
| Body mass index (BMI) | 31.5 ± 12.7 | 30.21 ± 0.80 | 31.81 ± 0.99 | 0.587 |
| Hypertension | 228 (92%) | 24 (92%) | 204 (92%) | 1 |
| Dyslipidemia | 213 (85%) | 20 (77%) | 193 (86%) | 0.209 |
| HF | 91 (37%) | 12 (46%) | 79 (35%) | 0.282 |
| Current smoking | 25 (10%) | 2 (8%) | 23 (11%) | 0.745 |
| CAD | 136 (55%) | 16 (62%) | 120 (54%) | 0.468 |
| Prior MI | 75 (30%) | 12 (46%) | 63 (28%) | 0.058 |
| History of smoking | 143 (57%) | 20 (77%) | 123 (55%) | 0.032 |
| Prior ischemic stroke | 22 (9%) | 5 (19%) | 17 (8%) | 0.048 |
| Prior TIA | 7 (3%) | 1 (4%) | 6 (3%) | 0.708 |
| Laboratory data (mean ± SD) | ||||
| White blood cell count (x109/L) | 6.9 ± 1.9 | 6.46 ± 0.40 | 6.95 ± 0.13 | 0.222 |
| Platelets (x109/L) | 222.6 ± 61.9 | 204.08 ± 9.62 | 225.42 ± 4.47 | 0.113 |
| Hemoglobin (g/dL) | 13.7 ± 1.46 | 13.72 ± 2.67 | 13.76 ± 0.99 | 0.969 |
| High-sensitivity C-reactive Protein (mg/dL) | 2 [0.3–25.8] | 1.9 [1.05–4.0] | 2.05 [1.05–4.1] | 0.726 |
| Fibrinogen (mg/dL) | 402.6 ± 104 | 407 ± 19.78 | 404 ± 7.72 | 0.994 |
| Creatinine (mg/dL) | 1 ± 0.31 | 1.16 ± 0.06 | 0.97 ± 0.02 | 0.001 |
| HbA1c | 6.5 [6.0–7.4] | 6.4 [5.9–7.1] | 6.9 [6.3–7.8] | 0.060 |
| Tch | 158.6 ± 36.5 | 153.63 ± 6.15 | 159.34 ± 2.69 | 0.628 |
| TG | 132.4 ± 61.5 | 123.46 ± 7.13 | 125.87 ± 3.12 | 0.990 |
| HDL | 50 ± 30.3 | 47.50 ± 9.31 | 51.45 ± 2.44 | 0.634 |
| LDL | 83.8 ± 28.3 | 81.42 ± 5.35 | 85.36 ± 2.23 | 0.670 |
| Failure to achieve lipid control | ||||
| LDL, %; n ** | 108 (49%) | 13 (54%) | 95 (48%) | 0.567 |
| HDL, %; n ** | 100 (44%) | 9 (39%) | 91 (45%) | 0.413 |
| Triglycerides, %; n ** | 68 (30%) | 8 (32%) | 60 (29%) | 0.778 |
| Concomitant medications n (%) | ||||
| ß-blockers | 178 (72%) | 22 (88%) | 156 (70%) | 0.054 |
| ACE inhibitors | 165 (66%) | 14 (56%) | 151 (67%) | 0.252 |
| Statins | 179 (72%) | 19 (76%) | 160 (71%) | 0.630 |
| Calcium channel-blockers | 94 (38%) | 8 (32%) | 86 (38%) | 0.532 |
| Proton pump Inhibitors | 49 (24%) | 8 (31%) | 41 (23%) | 0.407 |
| Randomization group in the AVOCADO study, %; n | ||||
| ASA (75 mg) *** | 167 (66%) | 11 (42%) | 156 (69%) | 0.006 |
| ASA (150 mg) *** | 32 (13%) | 6 (23%) | 26 (12%) | 0.093 |
| Clopidogrel *** | 53 (21%) | 9 (35%) | 44 (20%) | 0.073 |
| ASA total (75 mg + 150 mg) *** | 199 (79%) | 17 (65%) | 182 (81%) | 0.073 |
| miRNAs | ||||
| miR-126 | 0.84 [0.16–8.54] | 7.23 [1.93–47.3] | 0.46 [0.13–6.39] | 0.000032 |
| Let-7e | 0.64 [0.09–4.10] | 3.78 [0.85–25.70] | 0.51 [0.08–3.39] | 0.000216 |
| miR-223 | 8.91 [2.09–69.81] | 19.98 [6.27–94.85] | 8.11 [1.76–67.88] | 0.089 |
| miR-125a-3p | 0.009 [0.001–0.05] | 0.054 [0.006–1.05] | 0.0082 [0.001–0.041] | 0.0006 |
| miRNA | c-Index-AUC (95% CI) | p | Cut-Off | Sensitivity, % | Specificity, % | Positive Predictive Value, % | Negative Predictive Value, % | Positive Likelihood Ratio |
|---|---|---|---|---|---|---|---|---|
| miR-126 | 0.75 (0.66–0.84) | <0.001 | 2.078 | 77% | 63% | 19% | 96% | 2.07 |
| Let-7e | 0.76 (0.63–0.82) | <0.001 | 0.8201 | 81% | 66% | 18% | 96% | 1.84 |
| miR-223 | 0.60 (0.50–0.70) | 0.094 | 6.617 | 77% | 49% | 15% | 95% | 1.49 |
| miR-125a-3p | 0.71 (0.60–0.82) | 0.001 | 0.0017 | 65% | 61% | 17% | 94% | 1.78 |
| Variable | HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| High miR-126 | ||||
| Univariate | 4.377 | 1.749 | 10.956 | 0.002 |
| Multivariate * | 7.310 | 2.634 | 20.284 | <0.001 |
| High Let-7e | ||||
| Univariate | 4.208 | 1.580 | 11.206 | 0.004 |
| Multivariate * | 5.845 | 2.076 | 16.460 | 0.001 |
| High miR-223 | ||||
| Univariate | 2.389 | 0.952 | 5.977 | 0.063 |
| Multivariate * | 3.073 | 1.170 | 8.071 | 0.023 |
| High miR-125a-3p | ||||
| Univariate | 2.692 | 1.198 | 6.052 | 0.017 |
| Multivariate * | 2.929 | 1.256 | 6.828 | 0.013 |
| Variable | HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| High miR-126 | 5.821 | 1.259 | 24.927 | 0.024 |
| High Let-7e | 3.449 | 0.578 | 21.176 | 0.173 |
| High miR-223 | 0.367 | 0.080 | 1.679 | 0.196 |
| High miR-125a-3p | 1.115 | 0.408 | 3.050 | 0.832 |
| Age | 1.068 | 1.016 | 1.122 | 0.009 |
| Gender (male) | 4.059 | 1.235 | 13.344 | 0.027 |
| History of smoking | 1.656 | 0.519 | 5.289 | 0.395 |
| Prior IS | 4.041 | 1.242 | 12.646 | 0.016 |
| eGFR<30 | 5.879 | 0.841 | 41.100 | 0.074 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pordzik, J.; Eyileten-Postuła, C.; Jakubik, D.; Czajka, P.; Nowak, A.; De Rosa, S.; Gąsecka, A.; Cieślicka-Kapłon, A.; Sulikowski, P.; Filipiak, K.J.; et al. MiR-126 Is an Independent Predictor of Long-Term All-Cause Mortality in Patients with Type 2 Diabetes Mellitus. J. Clin. Med. 2021, 10, 2371. https://doi.org/10.3390/jcm10112371
Pordzik J, Eyileten-Postuła C, Jakubik D, Czajka P, Nowak A, De Rosa S, Gąsecka A, Cieślicka-Kapłon A, Sulikowski P, Filipiak KJ, et al. MiR-126 Is an Independent Predictor of Long-Term All-Cause Mortality in Patients with Type 2 Diabetes Mellitus. Journal of Clinical Medicine. 2021; 10(11):2371. https://doi.org/10.3390/jcm10112371
Chicago/Turabian StylePordzik, Justyna, Ceren Eyileten-Postuła, Daniel Jakubik, Pamela Czajka, Anna Nowak, Salvatore De Rosa, Aleksandra Gąsecka, Agnieszka Cieślicka-Kapłon, Piotr Sulikowski, Krzysztof J. Filipiak, and et al. 2021. "MiR-126 Is an Independent Predictor of Long-Term All-Cause Mortality in Patients with Type 2 Diabetes Mellitus" Journal of Clinical Medicine 10, no. 11: 2371. https://doi.org/10.3390/jcm10112371
APA StylePordzik, J., Eyileten-Postuła, C., Jakubik, D., Czajka, P., Nowak, A., De Rosa, S., Gąsecka, A., Cieślicka-Kapłon, A., Sulikowski, P., Filipiak, K. J., Mirowska-Guzel, D., Siller-Matula, J. M., & Postuła, M. (2021). MiR-126 Is an Independent Predictor of Long-Term All-Cause Mortality in Patients with Type 2 Diabetes Mellitus. Journal of Clinical Medicine, 10(11), 2371. https://doi.org/10.3390/jcm10112371