
Prenatal Screening of Trisomy 21: Could Oxidative Stress Markers Play a Role?

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Overview—Patient Recruitment
2.2. Ethics Statement
2.3. Laboratory Examinations
2.4. Data Management and Statistical Analysis
3. Results
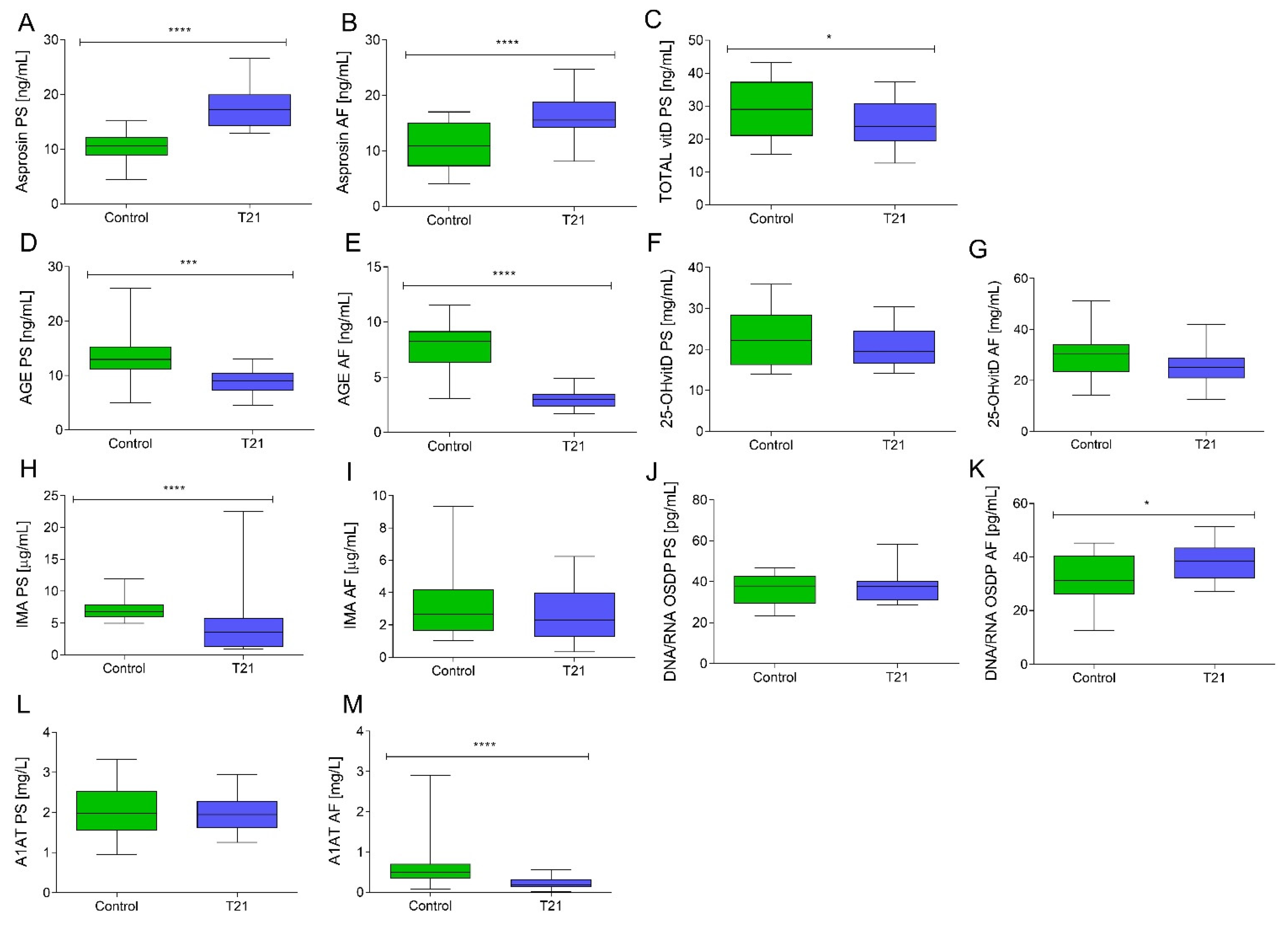
3.1. The Comparison of Oxidative Stress-Related Parameters between the Study and Control Groups
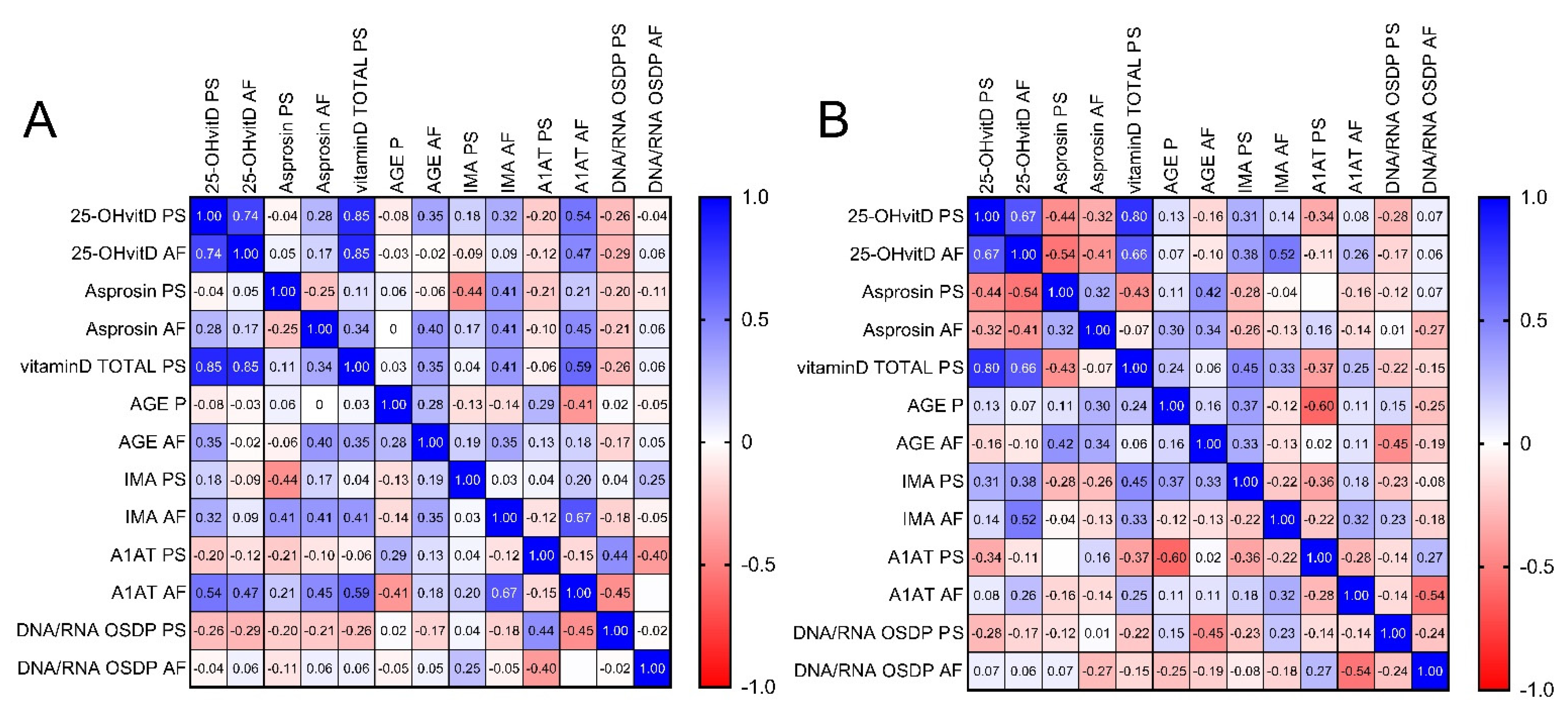
3.2. Correlations between Examined Parameters
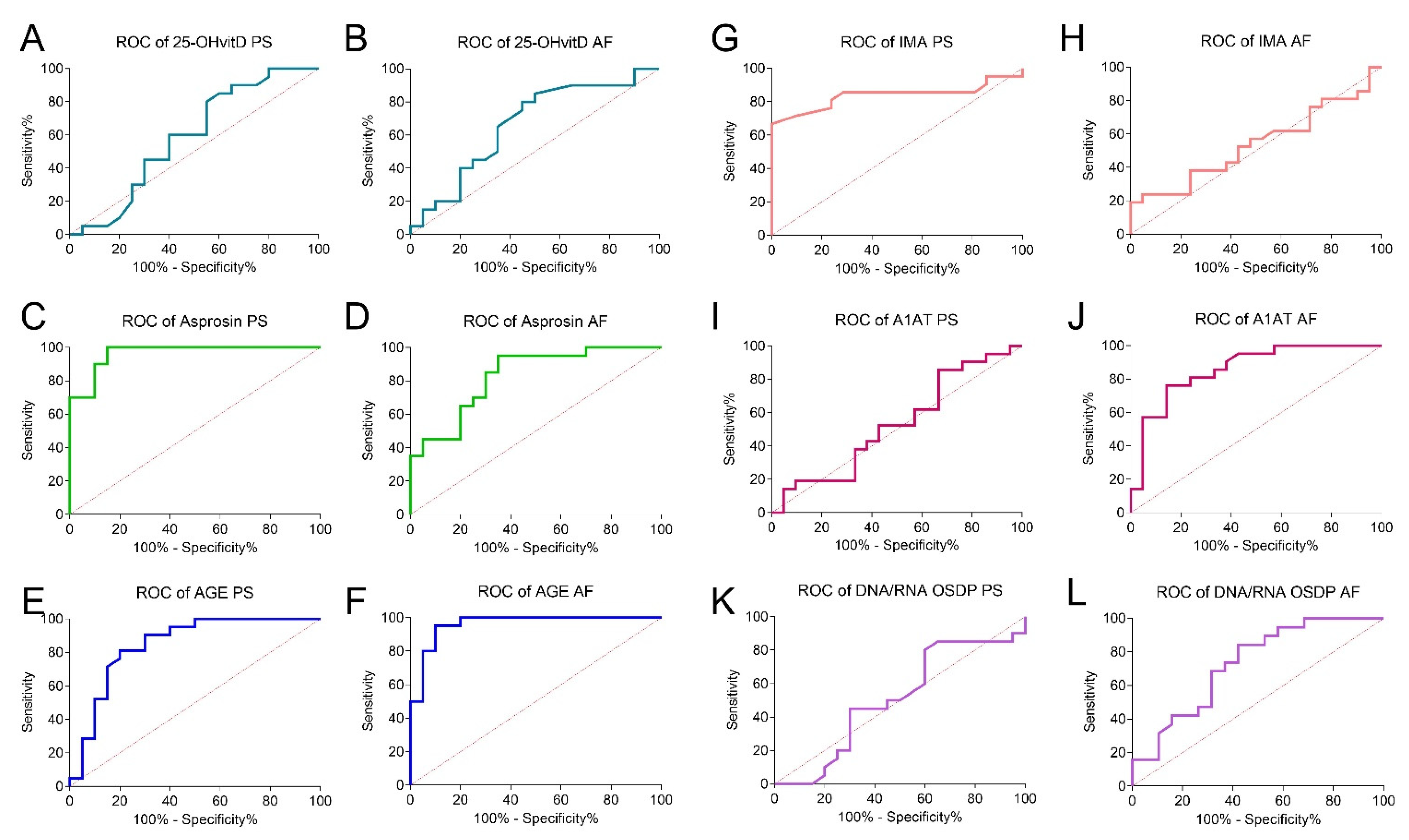
3.3. Screening Utility of the Tested Parameters
4. Discussion
4.1. Main Findings
4.2. Strength and Limitations
4.3. Implications and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Best, K.E.; Glinianaia, S.V.; Lingam, R.; Morris, J.K.; Rankin, J. Projected number of children with isolated spina bifida or down syndrome in England and Wales by 2020. Eur. J. Med. Genet. 2018, 61, 539–545. [Google Scholar] [CrossRef] [Green Version]
- Prevalence Charts and Tables. EU RD Platform. Available online: https://eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data/prevalence_en (accessed on 23 February 2021).
- Nadon, B.; Jackson, S. The polyploid origins of crop genomes and their implications: A case study in legumes. In Advances in Agronomy; Academic Press Inc.: Cambridge, MA, USA, 2020; Volume 159, pp. 275–313. [Google Scholar]
- Asim, A.; Kumar, A.; Muthuswamy, S.; Jain, S.; Agarwal, S. Down syndrome: An insight of the disease. J. Biomed. Sci. 2015, 22, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Carlson, L.M.; Vora, N.L. Prenatal Diagnosis: Screening and Diagnostic Tools. Obstet. Gynecol. Clin. N. Am. 2017, 44, 245–256. [Google Scholar] [CrossRef] [Green Version]
- Erturk, B.; Karaca, E.; Aykut, A.; Durmaz, B.; Guler, A.; Buke, B.; Yeniel, A.O.; Ergenoglu, A.M.; Ozkinay, F.; Ozeren, M.; et al. Prenatal Evaluation of MicroRNA Expressions in Pregnancies with Down Syndrome. BioMed Res. 2016, 2016, 5312674. [Google Scholar] [CrossRef] [Green Version]
- Shan, D.; Wang, H.; Khatri, P.; Niu, Y.; Song, W.; Zhao, S.; Jiang, Y.; Ma, Q.; Liu, X.; Zhang, R.; et al. The Urinary Peptidome as a Noninvasive Biomarker Development Strategy for Prenatal Screening of Down’s Syndrome. OMICS A J. Integr. Biol. 2019, 23, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Santorum, M.; Wright, D.; Syngelaki, A.; Karagioti, N.; Nicolaides, K.H. Accuracy of first-trimester combined test in screening for trisomies 21, 18 and 13. Ultrasound Obstet. Gynecol. 2017, 49, 714–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil, M.M.; Accurti, V.; Santacruz, B.; Plana, M.N.; Nicolaides, K.H. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: Updated meta-analysis. Ultrasound Obstet. Gynecol. 2017, 50, 302–314. [Google Scholar] [CrossRef]
- Carbone, L.; Cariati, F.; Sarno, L.; Conforti, A.; Bagnulo, F.; Strina, I.; Pastore, L.; Maruotti, G.M.; Alviggi, C. Non-Invasive Prenatal Testing: Current Perspectives and Future Challenges. Genes 2020, 12, 15. [Google Scholar] [CrossRef]
- Akolekar, R.; Beta, J.; Picciarelli, G.; Ogilvie, C.; D’Antonio, F. Procedure-related risk of miscarriage following amniocentesis and chorionic villus sampling: A systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2015, 45, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Zbucka-Kretowska, M.; Charkiewicz, K.; Czerniecki, J.; Goscik, J.; Wolczynski, S.; Laudanski, P. Amniotic Fluid Angiogenic and Inflammatory Factor Profiling in Foetal Down Syndrome. Fetal Diagn. Ther. 2017, 44, 44–50. [Google Scholar] [CrossRef]
- Muchová, J.; Žitňanová, I.; Ďuračková, Z. Oxidative Stress and Down Syndrome. Do Antioxidants Play a Role in Therapy? Physiol. Res. 2014, 63, 535–542. [Google Scholar] [CrossRef]
- Barone, E.; Head, E.; Butterfield, D.A.; Perluigi, M. HNE-modified proteins in Down syndrome: Involvement in development of Alzheimer disease neuropathology. Free Radic. Biol. Med. 2017, 111, 262–269. [Google Scholar] [CrossRef] [Green Version]
- Perluigi, M.; Butterfield, D.A. The identification of protein biomarkers for oxidative stress in Down syndrome. Expert Rev. Proteom. 2011, 8, 427–429. [Google Scholar] [CrossRef] [Green Version]
- Žitňanová, I.; Korytár, P.; Sobotová, H.; Horáková, L.; Sustrova, M.; Pueschel, S.; Ďuračková, Z. Markers of oxidative stress in children with Down syndrome. Clin. Chem. Lab. Med. 2006, 44, 306–310. [Google Scholar] [CrossRef]
- Barone, E.; Arena, A.; Head, E.; Butterfield, D.A.; Perluigi, M. Disturbance of redox homeostasis in Down Syndrome: Role of iron dysmetabolism. Free Radic. Biol. Med. 2018, 114, 84–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrocco, I.; Altieri, F.; Peluso, I. Measurement and Clinical Significance of Biomarkers of Oxidative Stress in Humans. Oxid. Med. Cell. Longev. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Buczyńska, A.; Sidorkiewicz, I.; Ławicki, S.; Krętowski, A.; Zbucka-Krętowska, M. The Significance of Apolipoprotein E Measurement in the Screening of Fetal Down Syndrome. J. Clin. Med. 2020, 9, 3995. [Google Scholar] [CrossRef]
- Gupta, K.K.; Attri, J.P.; Singh, A.; Kaur, H.; Kaur, G. Basic concepts for sample size calculation: Critical step for any clinical trials! Saudi J. Anaesth. 2016, 10, 328–331. [Google Scholar] [CrossRef]
- Eusebi, P. Diagnostic Accuracy Measures. Cerebrovasc. Dis. 2013, 36, 267–272. [Google Scholar] [CrossRef]
- MedCalc’s Odds Ratio Calculator. Available online: https://www.medcalc.org/calc/odds_ratio.php (accessed on 2 May 2021).
- Ross, M.G.; Idah, R. Correlation of maternal plasma volume and composition with amniotic fluid index in normal human pregnancy. J. Matern. Neonatal Med. 2004, 15, 104–108. [Google Scholar] [CrossRef]
- Suliburska, J.; Kocylowski, R.D.; Komorowicz, I.; Grzesiak, M.; Bogdański, P.; Barałkiewicz, D. Concentrations of Mineral in Amniotic Fluid and Their Relations to Selected Maternal and Fetal Parameters. Biol. Trace Elem. Res. 2016, 172, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Wald, N.J.; Kennard, A. Prenatal biochemical screening for Down’s syndrome and neural tube defects. Curr. Opin. Obstet. Gynecol. 1992, 4, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, T.; Duckyoung, Y.; Ito, A.; Kurosawa, K.; Maehata, Y.; Kubodera, T.; Ikeda, M.; Lee, M.-C.-I. Increased oxidative stress biomarkers in the saliva of Down syndrome patients. Arch. Oral Biol. 2013, 58, 1246–1250. [Google Scholar] [CrossRef] [PubMed]
- Rueda, N.; Flórez, J.; Martínez-Cué, C. Apoptosis in Down’s syndrome: Lessons from studies of human and mouse models. Apoptosis 2012, 18, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Ahlfors, H.; Anyanwu, N.; Pakanavicius, E.; Dinischiotu, N.; Lana-Elola, E.; Watson-Scales, S.; Tosh, J.; Wiseman, F.; Briscoe, J.; Page, K.; et al. Gene expression dysregulation domains are not a specific feature of Down syndrome. Nat. Commun. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Zheng, Y.; Yao, X. Functions of spindle checkpoint and its relationship to chromosome instability. Chin. Sci. Bull. 2002, 47, 617–623. [Google Scholar] [CrossRef]
- Le Page, F.; Cabral-Neto, J.; Cooper, P.K.; Sarasin, A. Transcription-coupled repair of 8-oxoguanine in human cells. In Methods in Enzymology; Academic Press Inc.: Cambridge, MA, USA, 2002; Volume 353, pp. 536–547. [Google Scholar]
- Zafrilla, P.; Cerda, B.; Soler, A.; Xandri, J.M.; Martinez-Cachá, A.; Mulero, J. Oxidative stress in Down Syndrome. J. Genet. Gene Ther. 2014, 5. [Google Scholar] [CrossRef] [Green Version]
- Perrone, S.; Perrone, S.; Longini, M.; Bellieni, C.; Centini, G.; Kenanidis, A.; De Marco, L.; Petraglia, F.; Buonocore, G. Early oxidative stress in amniotic fluid of pregnancies with Down syndrome. Clin. Biochem. 2007, 40, 177–180. [Google Scholar] [CrossRef]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef]
- Othman Bokhari, M.; Mujallid, M.F.; Alsulami, S.A.; Adel, A.; Milyani, M.A.A.; Malatani, N.N.; Al-Sharief, R.A.; Alsolami, M.A.; Al-Agha, A.E. Autoimmunity and Vitamin D deficiency in children affected with Trisomy 21. Curr. Pediatr. Res. 2018, 22, 182–184. [Google Scholar]
- De-Regil, L.M.; Palacios, C.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef] [Green Version]
- Nair-Shalliker, V.; Armstrong, B.K.; Fenech, M. Does vitamin D protect against DNA damage? Mutat. Res. Fundam. Mol. Mech. Mutagen. 2012, 733, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Koduah, P.; Paul, F.; Dörr, J.-M. Vitamin D in the prevention, prediction and treatment of neurodegenerative and neuroinflammatory diseases. EPMA J. 2017, 8, 313–325. [Google Scholar] [CrossRef] [Green Version]
- Zubillaga, P.; Garrido, A.; Mugica, I.; Ansa, J.; Zabalza, R.; Emparanza, J.I. Effect of vitamin D and calcium supplementation on bone turnover in institutionalized adults with Down’s Syndrome. Eur. J. Clin. Nutr. 2005, 60. [Google Scholar] [CrossRef]
- Pérez-López, F.R.; Pasupuleti, V.; Mezones-Holguin, E.; Benites-Zapata, V.A.; Thota, P.; Deshpande, A.; Hernandez, A.V. Effect of vitamin D supplementation during pregnancy on maternal and neonatal outcomes: A systematic review and meta-analysis of randomized controlled trials. Fertil. Steril. 2015, 103, 1278–1288. [Google Scholar] [CrossRef] [PubMed]
- Annweiler, C. Vitamin D in dementia prevention. Ann. N. Y. Acad. Sci. 2016, 1367, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Nuszkiewicz, J.; Woźniak, A.; Szewczyk-Golec, K. Ionizing Radiation as a Source of Oxidative Stress—The Protective Role of Melatonin and Vitamin D. Int. J. Mol. Sci. 2020, 21, 5804. [Google Scholar] [CrossRef]
- Palacios, C.; De-Regil, L.M.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation during pregnancy: Updated meta-analysis on maternal outcomes. J. Steroid Biochem. Mol. Biol. 2016, 164, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Stagi, S.; Lapi, E.; Romano, S.; Bargiacchi, S.; Brambilla, A.; Giglio, S.; Seminara, S.; De Martino, M. Determinants of Vitamin D Levels in Children and Adolescents with Down Syndrome. Int. J. Endocrinol. 2015, 2015, 896758. [Google Scholar] [CrossRef] [PubMed]
- Lindley, V.M.; Bhusal, K.; Huning, L.; Levine, S.N.; Jain, S.K. Reduced 25(OH) Vitamin D Association with Lower Alpha-1-Antitrypsin Blood Levels in Type 2 Diabetic Patients. J. Am. Coll. Nutr. 2021, 40, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.-L.; Yin, Y.-X.; Ding, J.; Yuan, H.; Yang, L.; Xu, J.-J.; Hu, L.-Q. Alpha-1-antitrypsin suppresses oxidative stress in preeclampsia by inhibiting the p38MAPK signaling pathway: An in vivo and in vitro study. PLoS ONE 2017, 12, e0173711. [Google Scholar] [CrossRef]
- Cabezas-Llobet, N.; Camprubí, S.; García, B.; Alberch, J.; Xifró, X. Human alpha 1-antitrypsin protects neurons and glial cells against oxygen and glucose deprivation through inhibition of interleukins expression. Biochim. Biophys. Acta Gen. Subj. 2018, 1862, 1852–1861. [Google Scholar] [CrossRef]
- Torres-Durán, M.; Lopez-Campos, J.L.; Barrecheguren, M.; Miravitlles, M.; Martinez-Delgado, B.; Castillo, S.; Escribano, A.; Baloira, A.; Navarro-Garcia, M.M.; Pellicer, D.; et al. Alpha-1 antitrypsin deficiency: Outstanding questions and future directions. Orphanet J. Rare Dis. 2018, 13, 114. [Google Scholar] [CrossRef] [Green Version]
- Narasimhan, K.; Lin, S.L.; Tong, T.; Baig, S.; Ho, S.; Sukumar, P.; Biswas, A.; Hahn, S.; Bajic, V.B.; Choolani, M.A. Maternal serum protein profile and immune response protein subunits as markers for non-invasive prenatal diagnosis of trisomy 21, 18, and 13. Prenat. Diagn. 2013, 33, 223–231. [Google Scholar] [CrossRef]
- Tarani, L.; Carito, V.; Ferraguti, G.; Petrella, C.; Greco, A.; Ralli, M.; Messina, M.P.; Rasio, D.; De Luca, E.; Putotto, C.; et al. Neuroinflammatory Markers in the Serum of Prepubertal Children with Down Syndrome. J. Immunol. Res. 2020, 2020, 6937154. [Google Scholar] [CrossRef]
- Gardiner, K.J. Pharmacological approaches to improving cognitive function in down syndrome: Current status and considerations. Drug Des. Dev. Ther. 2014, 9, 103–125. [Google Scholar] [CrossRef] [Green Version]
- Duerrschmid, C.; He, Y.; Wang, C.; Li, C.; Bournat, J.C.; Romere, C.; Saha, P.K.; Lee, M.E.; Phillips, K.J.; Jain, M.; et al. Asprosin is a centrally acting orexigenic hormone. Nat. Med. 2017, 23, 1444–1453. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Tan, Y.; Zhu, L.; Zhang, B.; Feng, P.; Gao, E.; Xu, C.; Wang, X.; Yi, W.; Sun, Y. Asprosin improves the survival of mesenchymal stromal cells in myocardial infarction by inhibiting apoptosis via the activated ERK1/2-SOD2 pathway. Life Sci. 2019, 231, 116554. [Google Scholar] [CrossRef] [PubMed]
- Basim, M.; Alobaidi, A.; Razooq, R.; Al-Samarrai, H. Correlation between Serum Asprosin Level And Oxidative Stress in Iraqi Patients with Type Ii Diabetes Mellitus. Syst. Rev. Pharm. 2020, 11, 1729–1733. [Google Scholar]
- Luís, C.; Fernandes, R.; Soares, R.; von Hafe, P. A state of the art review on the novel mediator asprosin in the metabolic syndrome. Porto Biomed. J. 2020, 5, e108. [Google Scholar] [CrossRef]
- Rejc, B.; Karas-Kuželički, N.; Osredkar, J.; Geršak, K. Correlation between markers of DNA and lipid oxidative damage in maternal and fetoplacental compartment in the mid-trimester of pregnancy. J. Périnat. Med. 2017, 45, 413–419. [Google Scholar] [CrossRef]
- Lott, I.T. Antioxidants in Down syndrome. Biochim. Biophys. Acta Mol. Basis Dis. 2012, 1822, 657–663. [Google Scholar] [CrossRef] [Green Version]
- Reddy, V.S.; Duggina, P.; Vedhantam, M.; Manne, M.; Varma, N.; Nagaram, S.; Srinivas, N. Maternal serum and fetal cord-blood ischemia-modified albumin concentrations in normal pregnancy and preeclampsia: A systematic review and meta-analysis. J. Matern. Neonatal Med. 2018, 31, 3255–3266. [Google Scholar] [CrossRef] [PubMed]
- Keshavarzi, F.; Rastegar, M.; Vessal, M.; Dehbidi, G.R.; Khorsand, M.; Ganjkarimi, A.H.; Takhshid, M.A. Serum ischemia modified albumin is a possible new marker of oxidative stress in phenylketonuria. Metab. Brain Dis. 2017, 33, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Akasaka, J.; Naruse, K.; Sado, T.; Uchiyama, T.; Makino, M.; Yamauchi, A.; Ota, H.; Sakuramoto-Tsuchida, S.; Itaya-Hironaka, A.; Takasawa, S.; et al. Involvement of Receptor for Advanced Glycation Endproducts in Hypertensive Disorders of Pregnancy. Int. J. Mol. Sci. 2019, 20, 5462. [Google Scholar] [CrossRef] [Green Version]
- Vyakaranam, S.; Bhongir, A.; Patlolla, D.; Chintapally, R. Maternal serum ischemia modified albumin as a marker for hypertensive disorders of pregnancy: A pilot study. Int. J. Reprod. Contracept. Obstet. Gynecol. 2015, 4, 611–616. [Google Scholar] [CrossRef] [Green Version]
- Bahinipati, J.; Mohapatra, P.C. Ischemia Modified Albumin as a Marker of Oxidative Stress in Normal Pregnancy. J. Clin. Diagn. Res. 2016, 10, BC15–BC17. [Google Scholar] [CrossRef]
- Berktold, L.V.; Kaisenberg, C.; Hillemanns, P.; Vaske, B.; Schmidt, P. Analysis of the impact of PAPP-A, free β-hCG and nuchal translucency thickness on the advanced first trimester screening. Arch. Gynecol. Obstet. 2013, 287, 413–420. [Google Scholar] [CrossRef]
- Reynolds, T. Giving antioxidants to infants with Down’s syndrome. BMJ 2008, 336, 568–569. [Google Scholar] [CrossRef] [Green Version]
- Metere, A.; Frezzotti, F.; Graves, C.E.; Vergine, M.; De Luca, A.; Pietraforte, D.; Giacomelli, L. A possible role for selenoprotein glutathione peroxidase (GPx1) and thioredoxin reductases (TrxR1) in thyroid cancer: Our experience in thyroid surgery. Cancer Cell Int. 2018, 18, 7. [Google Scholar] [CrossRef] [PubMed]
- Ellis, J.M.; Tan, H.K.; Gilbert, R.E.; Muller, D.P.R.; Henley, W.; Moy, R.; Pumphrey, R.; Ani, C.; Davies, S.; Edwards, V.; et al. Supplementation with antioxidants and folinic acid for children with Down’s syndrome: Randomised controlled trial. BMJ 2008, 336, 594–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salman, M. Systematic review of the effect of therapeutic dietary supplements and drugs on cognitive function in subjects with Down syndrome. Eur. J. Paediatr. Neurol. 2002, 6, 213–219. [Google Scholar] [CrossRef]
- Czeizel, A.E.; Puhó, E. Maternal use of nutritional supplements during the first month of pregnancy and decreased risk of Down’s syndrome: Case-control study. Nutrition 2005, 21, 698–704. [Google Scholar] [CrossRef]
- Nachvak, S.M.; Neyestani, T.R.; Mahboob, S.A.; Sabour, S.; Keshawarz, S.A.; Speakman, J.R. α-Tocopherol supplementation reduces biomarkers of oxidative stress in children with Down syndrome: A randomized controlled trial. Eur. J. Clin. Nutr. 2014, 68, 1119–1123. [Google Scholar] [CrossRef] [Green Version]
- Revilla, N.R.; Martínez-Cué, C. Antioxidants in down syndrome: From preclinical studies to clinical trials. Antioxidants 2020, 9, 626. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Marker | Material | Study Group | Unit | Median Value | Min | Max | p Value (Control vs. T21) | p Value (between Study Material) | |
|---|---|---|---|---|---|---|---|---|---|
| Control PS vs. Control AF | T21 PS vs. T21 AF | ||||||||
| 25-OH vitamin D | PS | Control | mg/mL | 22.22 | 14.00 | 35.92 | NS | p < 0.01 | NS |
| T21 | 19.51 | 14.24 | 30.44 | ||||||
| AF | Control | 30.60 | 14.24 | 51.34 | NS | ||||
| T21 | 25.20 | 12.59 | 42.07 | ||||||
| Asprosin | PS | Control | ng/mL | 10.57 | 4.45 | 15.17 | p < 0.0001 | NS | NS |
| T21 | 17.28 | 12.94 | 26.59 | ||||||
| AF | Control | 10.87 | 4.01 | 17.03 | p < 0.0001 | ||||
| T21 | 15.53 | 8.09 | 24.77 | ||||||
| AGE | PS | Control | ng/mL | 12.96 | 4.96 | 26.03 | p < 0.001 | p < 0.01 | p < 0.0001 |
| T21 | 9.16 | 4.52 | 13.01 | ||||||
| AF | Control | 8.27 | 3.06 | 11.55 | p < 0.0001 | ||||
| T21 | 3.00 | 1.67 | 4.89 | ||||||
| IMA | PS | Control | µg/mL | 6.79 | 5.00 | 12.00 | p < 0.0001 | p < 0.0001 | NS |
| T21 | 3.61 | 0.90 | 22.52 | ||||||
| AF | Control | 2.64 | 1.05 | 9.34 | NS | ||||
| T21 | 2.28 | 0.33 | 6.23 | ||||||
| A1AT | PS | Control | mg/L | 1.98 | 0.95 | 3.38 | NS | p < 0.001 | p < 0.0001 |
| T21 | 1.95 | 1.26 | 1.69 | ||||||
| AF | Control | 0.49 | 0.08 | 2.90 | p < 0.0001 | ||||
| T21 | 0.18 | 0.01 | 0.56 | ||||||
| DNA/RNA OSDP | PS | Control | pg/mL | 37.81 | 23.21 | 46.83 | NS | NS | NS |
| T21 | 37.57 | 28.53 | 58.40 | ||||||
| AF | Control | 31.16 | 12.64 | 45.22 | p < 0.05 | ||||
| T21 | 38.48 | 27.06 | 51.46 | ||||||
| Marker | Unit | AUC | p (AUC = 0.50) | Cut Off Value | Sensitivity | Specificity | OR | p |
|---|---|---|---|---|---|---|---|---|
| 25-OH vitamin D PS | mg/mL | 0.59 | NS | <26.18 | 0.85 | 0.40 | 1.62 | NS |
| 25-OH vitamin D AF | mg/mL | 0.66 | NS | <31.21 | 0.85 | 0.50 | 3.27 | NS |
| Asprosin PS | ng/mL | 0.97 | <0.0001 | >12.70 | 1.00 | 0.85 | 8.20 | p < 0.05 |
| Asprosin AF | ng/mL | 0.83 | <0.001 | >12.91 | 0.95 | 0.65 | 22.78 | p < 0.05 |
| AGE PS | ng/mL | 0.85 | <0.001 | <11.00 | 0.81 | 0.80 | 1.00 | NS |
| AGE AF | ng/mL | 0.96 | <0.0001 | <4.184 | 0.95 | 0.90 | 2.11 | p < 0.05 |
| IMA PS | µg/mL | 0.84 | <0.001 | <4.798 | 0.67 | 1.00 | 1.05 | NS |
| IMA AF | µg/mL | 0.54 | NS | <1.798 | 0.38 | 0.76 | 0.18 | p < 0.05 |
| A1AT PS | mg/L | 0.53 | NS | <2.341 | 0.81 | 0.33 | 5.75 | p < 0.05 |
| A1AT AF | mg/L | 0.87 | <0.0001 | <0.3180 | 0.76 | 0.86 | 0.71 | NS |
| DNA/RNA OSDP PS | pg/mL | 0.51 | NS | <40.30 | 0.80 | 0.40 | 3.27 | NS |
| DNA/RNA OSDP AF | pg/mL | 0.73 | <0.05 | >31.76 | 0.84 | 0.58 | 3.78 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buczyńska, A.; Sidorkiewicz, I.; Ławicki, S.; Krętowski, A.J.; Zbucka-Krętowska, M. Prenatal Screening of Trisomy 21: Could Oxidative Stress Markers Play a Role? J. Clin. Med. 2021, 10, 2382. https://doi.org/10.3390/jcm10112382
Buczyńska A, Sidorkiewicz I, Ławicki S, Krętowski AJ, Zbucka-Krętowska M. Prenatal Screening of Trisomy 21: Could Oxidative Stress Markers Play a Role? Journal of Clinical Medicine. 2021; 10(11):2382. https://doi.org/10.3390/jcm10112382
Chicago/Turabian StyleBuczyńska, Angelika, Iwona Sidorkiewicz, Sławomir Ławicki, Adam Jacek Krętowski, and Monika Zbucka-Krętowska. 2021. "Prenatal Screening of Trisomy 21: Could Oxidative Stress Markers Play a Role?" Journal of Clinical Medicine 10, no. 11: 2382. https://doi.org/10.3390/jcm10112382
APA StyleBuczyńska, A., Sidorkiewicz, I., Ławicki, S., Krętowski, A. J., & Zbucka-Krętowska, M. (2021). Prenatal Screening of Trisomy 21: Could Oxidative Stress Markers Play a Role? Journal of Clinical Medicine, 10(11), 2382. https://doi.org/10.3390/jcm10112382