
Associations between High-Density Lipoprotein Functionality and Major Adverse Cardiovascular Events in Patients Who Have Undergone Coronary Computed Tomography Angiography

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Evaluation of Coronary Stenosis Using CCTA
2.2. Evaluation of CAD Risk Factors and Left Ventricular Ejection Fraction (LVEF)
2.3. Measurement of HDL CEC
2.4. Measurement of Secretion of Monocyte Chemotactic Protein 1 (MCP-1)
2.5. Measurement of Caspase 3/7 Activity
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics in All Patients and in the MACE(+) and MACE(−) Groups
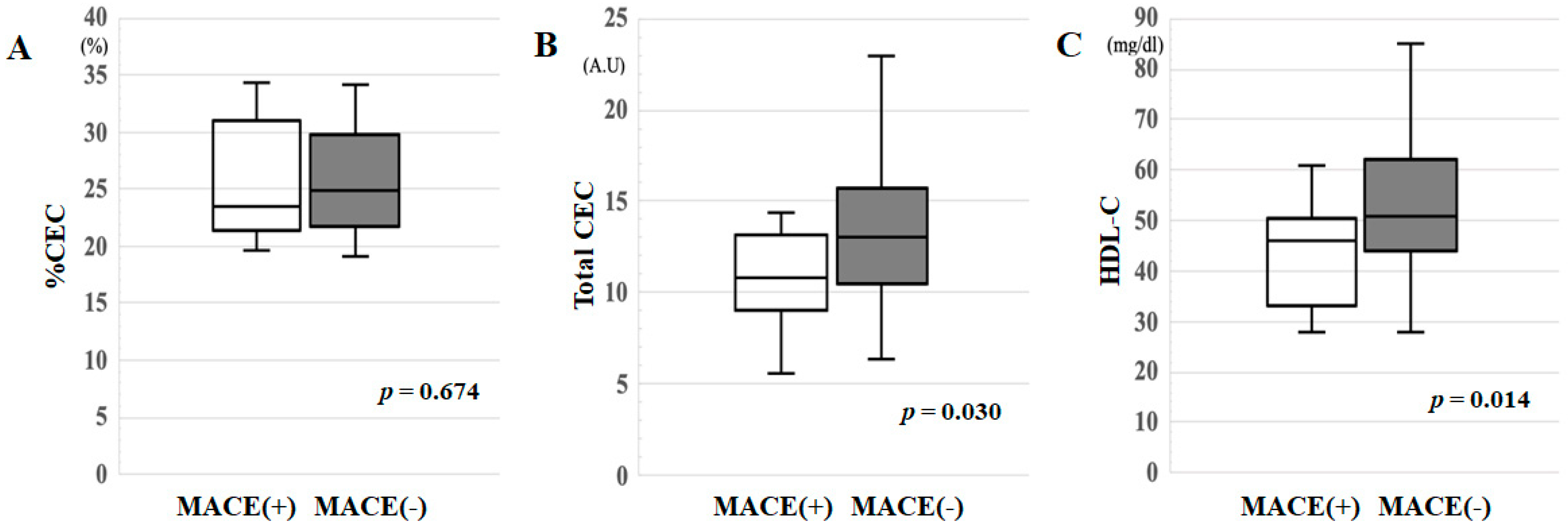
3.2. %CEC, Total CEC and HDL-C in the MACE(+) and MACE(−) Groups
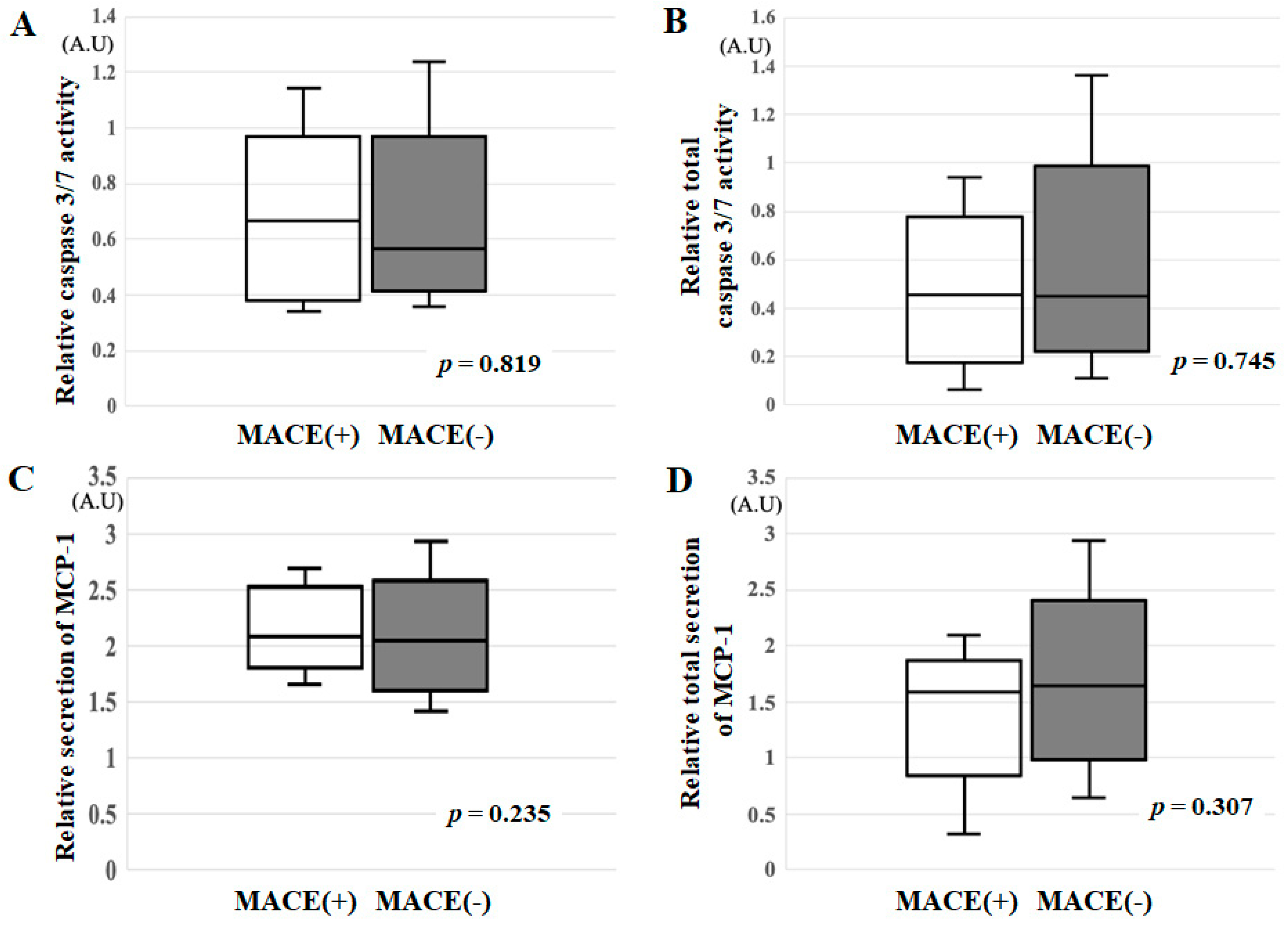
3.3. Relative Caspase 3/7 Activity, Relative Total Caspase 3/7 Activity, Relative Secretion of MCP-1 and Relative Total Secretion of MCP-1 in the MACE(+) and MACE(−) Groups
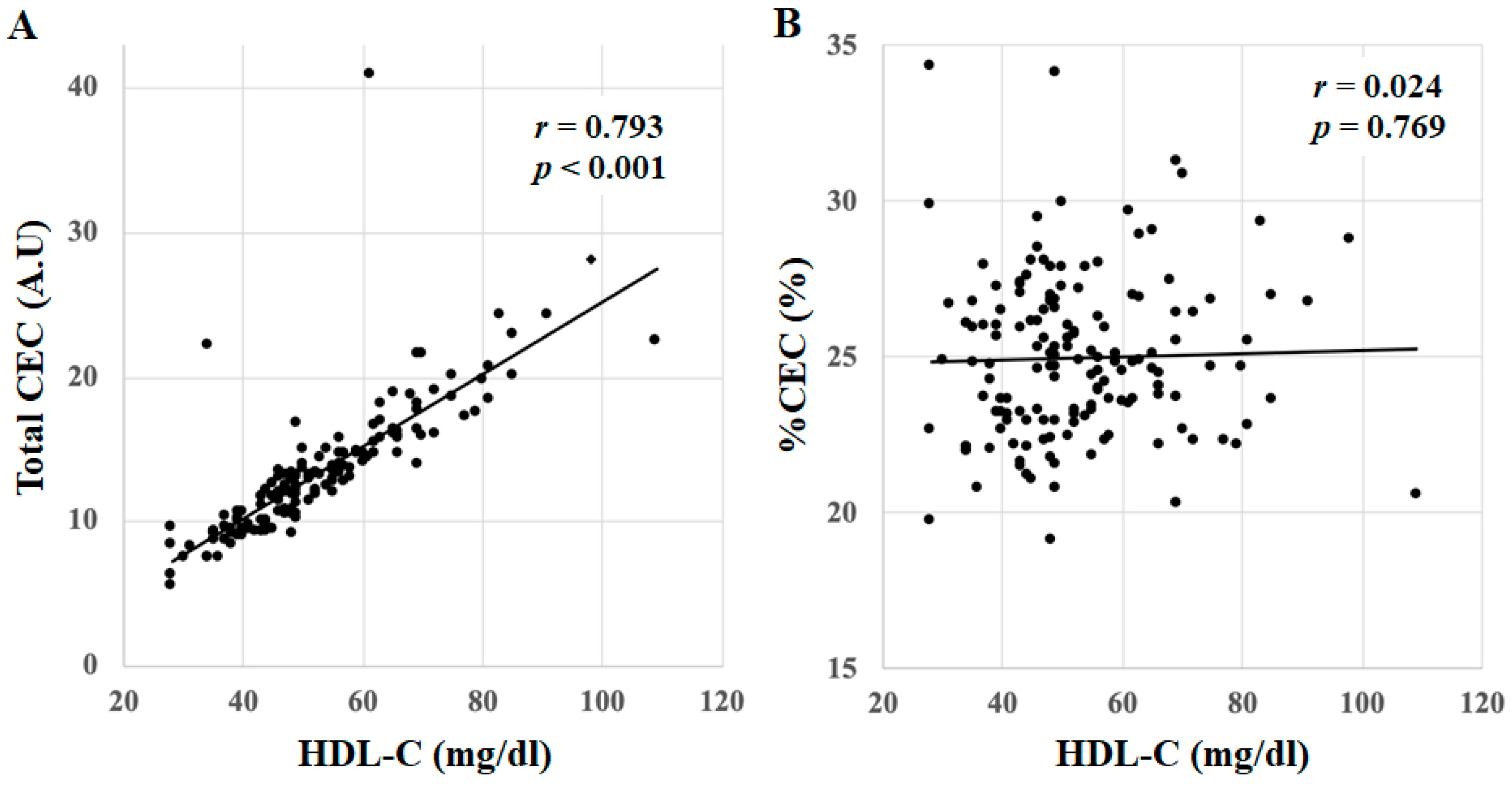
3.4. Correlations between %CEC, Total CEC and HDL-C in All Patients
3.5. Cut-Off Values of Total CEC or HDL-C Levels for the Diagnosis of MACE in All Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barter, P.; Gotto, A.M.; LaRosa, J.C.; Maroni, J.; Szarek, M.; Grundy, S.M.; Kastelein, J.J.P.; Bittner, V.; Fruchart, J.-C. HDL Cholesterol, Very Low Levels of LDL Cholesterol, and Cardiovascular Events. N. Engl. J. Med. 2007, 357, 1301–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Keefe, J.H.; Cordain, L.; Harris, W.H.; Moe, R.M.; Vogel, R. Optimal low-density lipoprotein is 50 to 70 mg/dL: Lower is better and physiologically normal. J. Am. Coll. Cardiol. 2004, 43, 2142–2146. [Google Scholar] [CrossRef] [Green Version]
- Ogita, M.; Miyauchi, K.; Miyazaki, T.; Naito, R.; Konishi, H.; Tsuboi, S.; Dohi, T.; Kasai, T.; Yokoyama, T.; Okazaki, S.; et al. Low high-density lipoprotein cholesterol is a residual risk factor associated with long-term clinical outcomes in diabetic patients with stable coronary artery disease who achieve optimal control of low-density lipoprotein cholesterol. Heart Vessel. 2013, 29, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Gordon, T.; Castelli, W.P.; Hjortland, M.C.; Kannel, W.B.; Dawber, T.R. High density lipoprotein as a protective factor against coronary heart disease. Am. J. Med. 1977, 62, 707–714. [Google Scholar] [CrossRef]
- The AIM-HIGH Investigators Niacin in Patients with Low HDL Cholesterol Levels Receiving Intensive Statin Therapy. N. Engl. J. Med. 2011, 365, 2255–2267. [CrossRef] [PubMed] [Green Version]
- Kinoshita, M.; Yokote, K.; Arai, H.; Iida, M.; Ishigaki, Y.; Ishibashi, S.; Umemoto, S.; Egusa, G.; Ohmura, H.; Okamura, T.; et al. Japan Atherosclerosis Society (JAS) Guidelines for Prevention of Atherosclerotic Cardiovascular Diseases 2017. J. Atheroscler. Thromb. 2018, 25, 846–984. [Google Scholar] [CrossRef] [Green Version]
- Hirata, A.; Sugiyama, D.; Watanabe, M.; Tamakoshi, A.; Iso, H.; Kotani, K.; Kiyama, M.; Yamada, M.; Ishikawa, S.; Murakami, Y.; et al. Association of extremely high levels of high-density lipoprotein cholesterol with cardiovascular mortality in a pooled analysis of 9 cohort studies including 43,407 individuals: The EPOCH–JAPAN study. J. Clin. Lipidol. 2018, 12, 674–684.e5. [Google Scholar] [CrossRef]
- Dimmeler, S.; Haendeler, J.; Zeiher, A.M. Regulation of endothelial cell apoptosis in atherothrombosis. Curr. Opin. Lipidol. 2002, 13, 531–536. [Google Scholar] [CrossRef]
- Farbstein, D.; Levy, A.P. HDL dysfunction in diabetes: Causes and possible treatments. Expert Rev. Cardiovasc. Ther. 2012, 10, 353–361. [Google Scholar] [CrossRef] [Green Version]
- Khera, A.V.; Cuchel, M.; De La Llera-Moya, M.; Rodrigues, A.; Burke, M.F.; Jafri, K.; French, B.C.; Phillips, J.A.; Mucksavage, M.L.; Wilensky, R.L.; et al. Cholesterol Efflux Capacity, High-Density Lipoprotein Function, and Atherosclerosis. N. Engl. J. Med. 2011, 364, 127–135. [Google Scholar] [CrossRef] [Green Version]
- Rohatgi, A.; Khera, A.; Berry, J.D.; Givens, E.G.; Ayers, C.R.; Wedin, K.E.; Neeland, I.J.; Yuhanna, I.S.; Rader, D.R.; De Lemos, J.A.; et al. HDL Cholesterol Efflux Capacity and Incident Cardiovascular Events. N. Engl. J. Med. 2014, 371, 2383–2393. [Google Scholar] [CrossRef] [Green Version]
- Imaizumi, S.; Miura, S.; Takata, K.; Takamiya, Y.; Kuwano, T.; Sugihara, M.; Ike, A.; Iwata, A.; Nishikawa, H.; Saku, K. Association between cholesterol efflux capacity and coronary restenosis after successful stent implantation. Heart Vessel. 2015, 31, 1257–1265. [Google Scholar] [CrossRef]
- Tashiro, K.; Inoue, H.; Shiga, Y.; Tsukihashi, Y.; Imaizumi, T.; Norimatsu, K.; Idemoto, Y.; Kuwano, T.; Sugihara, M.; Nishikawa, H.; et al. Associations Between High Levels of High-Density Lipoprotein Cholesterol and the Presence and Severity of Coronary Artery Disease in Patients Who Have Undergone Coronary Computed Tomography Angiography. J. Clin. Med. Res. 2020, 12, 734–739. [Google Scholar] [CrossRef]
- Norimatsu, K.; Kuwano, T.; Miura, S.; Shimizu, T.; Shiga, Y.; Suematsu, Y.; Miyase, Y.; Adachi, S.; Nakamura, A.; Imaizumi, S.; et al. Significance of the percentage of cholesterol efflux capacity and total cholesterol efflux capacity in patients with or without coronary artery disease. Heart Vessel. 2016, 32, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Miura, S.; Suematsu, Y.; Matsuo, Y.; Imaizumi, S.; Yahiro, E.; Uehara, Y.; Saku, K. Induction of endothelial tube for-mation and anti-inflammation by newly developed apolipoprotein A-I mimetic peptide. IJC Metab. Endocr. 2014, 5, 70–72. [Google Scholar] [CrossRef] [Green Version]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2012, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, D.C.; Hoang, A.; Barrett, P.H.R.; Wong, A.T.Y.; Nestel, P.J.; Sviridov, D.; Watts, G.F. Apolipoprotein B-100 and ApoA-II Kinetics as Determinants of Cellular Cholesterol Efflux. J. Clin. Endocrinol. Metab. 2012, 97, E1658–E1666. [Google Scholar] [CrossRef] [Green Version]
- Melchior, J.T.; Street, S.E.; Andraski, A.B.; Furtado, J.D.; Sacks, F.M.; Shute, R.L.; Greve, E.I.; Swertfeger, D.; Li, H.; Shah, A.S.; et al. Apolipoprotein A-II alters the proteome of human lipoproteins and enhances cholesterol efflux from ABCA1. J. Lipid Res. 2017, 58, 1374–1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelli, W.P.; Garrison, R.J.; Wilson, P.W.F.; Abbott, R.D.; Kalousdian, S.; Kannel, W.B. Incidence of Coronary Heart Disease and Lipoprotein Cholesterol Levels. JAMA 1986, 256, 2835–2838. [Google Scholar] [CrossRef]
- Kaur, M.; Ahuja, K.R.; Khubber, S.; Zhou, L.; Verma, B.R.; Meenakshisundaram, C.; Gad, M.M.; Saad, A.; Dhaliwal, K.; Isogai, T.; et al. Effect of High-Density Lipoprotein Cholesterol Levels on Overall Survival and Major Adverse Cardiovascular and Cerebrovascular Events. Am. J. Cardiol. 2021, 146, 8–14. [Google Scholar] [CrossRef]
- Li, Y.-H.; Taiwanese Secondary Prevention for Patients with AtheRosCLErotic Disease (T-SPARCLE) Registry Investigators; Tseng, W.-K.; Yin, W.-H.; Lin, F.-J.; Wu, Y.-W.; Hsieh, I.-C.; Lin, T.-H.; Sheu, W.H.-H.; Yeh, H.-I.; et al. Prognostic effect of high-density lipoprotein cholesterol level in patients with atherosclerotic cardiovascular disease under statin treatment. Sci. Rep. 2020, 10, 21835. [Google Scholar] [CrossRef] [PubMed]
- Di Angelantonio, E.; Sarwar, N.; Perry, P.; Kaptoge, S.; Ray, K.K.; Thompson, A.; Wood, A.M.; Lewington, S.; Sattar, N.; Packard, C.J.; et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA J. Am. Med. Assoc. 2009, 302, 1993–2000. [Google Scholar] [CrossRef] [Green Version]
- Haase, C.L.; Tybjaerg-Hansen, A.; Grande, P.; Frikke-Schmidt, R. Genetically Elevated Apolipoprotein A-I, High-Density Lipoprotein Cholesterol Levels, and Risk of Ischemic Heart Disease. J. Clin. Endocrinol. Metab. 2010, 95, E500–E510. [Google Scholar] [CrossRef] [Green Version]
- Hirata, A.; Okamura, T.; Sugiyama, D.; Kuwabara, K.; Kadota, A.; Fujiyoshi, A.; Miura, K.; Okuda, N.; Ohkubo, T.; Okayama, A.; et al. The Relationship between Very High Levels of Serum High-Density Lipoprotein Cholesterol and Cause-Specific Mortality in a 20-Year Follow-Up Study of Japanese General Population. J. Atheroscler. Thromb. 2016, 23, 800–809. [Google Scholar] [CrossRef]
- Madsen, C.M.; Varbo, A.; Nordestgaard, B.G. Extreme high high-density lipoprotein cholesterol is paradoxically associated with high mortality in men and women: Two prospective cohort studies. Eur. Heart J. 2017, 38, 2478–2486. [Google Scholar] [CrossRef] [Green Version]
- Retterstol, L.; Eikvar, L.; Bohn, M.; Bakken, A.; Erikssen, J.; Berg, K. C-reactive protein predicts death in patients with previous premature myocardial infarction—A 10 year follow-up study. Atherosclerosis 2002, 160, 433–440. [Google Scholar] [CrossRef]
- Chew, D.P.; Bhatt, D.L.; Robbins, M.A.; Penn, M.S.; Schneider, J.P.; Lauer, M.; Topol, E.J.; Ellis, S.G. Incremental Prognostic Value of Elevated Baseline C-Reactive Protein Among Established Markers of Risk in Percutaneous Coronary Intervention. Circulation 2001, 104, 992–997. [Google Scholar] [CrossRef] [Green Version]
- Nissen, S.E.; Tuzcu, E.M.; Schoenhagen, P.; Crowe, T.; Sasiela, W.J.; Tsai, J.; Orazem, J.; Magorien, R.D.; O’Shaughnessy, C.; Ganz, P. Statin Therapy, LDL Cholesterol, C-Reactive Protein, and Coronary Artery Disease. N. Engl. J. Med. 2005, 352, 29–38. [Google Scholar] [CrossRef]
- Gallacher, J.E. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: An individual participant meta-analysis. Lancet 2010, 375, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Ren, J.; Morgan, S.; Liu, Z.; Dou, C.; Liu, B. Monocyte Chemoattractant Protein-1 (MCP-1) Regulates Macrophage Cytotoxicity in Abdominal Aortic Aneurysm. PLoS ONE 2014, 9, e92053. [Google Scholar] [CrossRef]
- Kristono, G.A.; Holley, A.S.; Hally, K.E.; Brunton-O’Sullivan, M.M.; Shi, B.; Harding, S.A.; Larsen, P.D. An IL-6-IL-8 score derived from principal component analysis is predictive of adverse outcome in acute myocardial infarction. Cytokine X 2020, 2, 100037. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Chen, H.; Gao, J.; Liu, Y.; Li, J.; Wang, J. Molecular machinery and interplay of apoptosis and autophagy in coronary heart disease. J. Mol. Cell. Cardiol. 2019, 136, 27–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 151) | MACE(+) Group (n = 13) | MACE(−) Group (n = 138) | |
|---|---|---|---|
| Age (years) | 65 (58–71) | 67 (58–70) | 64 (58–71) |
| Male (%) | 62 | 62 | 57 |
| BMI (kg/m2) | 23 ± 3 | 23 ± 4 | 23 ± 3 |
| Smoking (%) | 39 | 62 * | 34 |
| HTN (%) | 78 | 77 | 71 |
| SBP (mmHg) | 134 (123–146) | 136 (123–146) | 133 (123–146) |
| DBP (mmHg) | 76 ± 12 | 79 ± 19 | 76 ± 11 |
| DL (%) | 71 | 77 | 64 |
| LDL-C (mg/dL) | 108 ± 28 | 94 ± 28 | 109 ± 28 |
| HDL-C (mg/dL) | 50 (43–61) | 46 (33–50) * | 51 (44–62) |
| TG (mg/dL) | 114 (79–159) | 113 (76–187) | 114 (79–156) |
| DM (%) | 23 | 23 | 21 |
| HbA1c (%) | 5.6 (5.3–6.2) | 5.8 (5.4–6.6) | 5.6 (5.3–6.2) |
| FBG (mg/dL) | 101 (93–114) | 101 (93–124) | 101 (93–114) |
| CKD (%) | 5 | 8 | 6 |
| eGFR (mL/min/1.73 m2) | 66 ± 14 | 67 ± 10 | 68 ± 14 |
| LVEF (%) | 68 ± 9 | 67 ± 12 | 68 ± 5 |
| CAD (%) | 48 | 61 | 47 |
| The number of VD | 0.92 ± 1.10 | 1.38 ± 1.32 | 0.88 ± 1.07 |
| Gensini score | 12 ± 15 | 16 ± 15 | 11 ± 14 |
| Medications | |||
| ARB/ACE-I (%) | 44 | 46 | 41 |
| CCB (%) | 35 | 31 | 33 |
| β-blocker (%) | 17 | 0 | 17 |
| Diuretic (%) | 13 | 15 | 12 |
| Statin (%) | 34 | 46 | 35 |
| EPA (%) | 2 | 8 | 2 |
| Insulin (%) | 10 | 8 | 6 |
| Sulfonylurea (%) | 13 | 23 | 12 |
| Biguanide (%) | 10 | 23 | 9 |
| DPP4-I (%) | 10 | 15 | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, H.; Shiga, Y.; Norimatsu, K.; Tashiro, K.; Futami, M.; Suematsu, Y.; Sugihara, M.; Nishikawa, H.; Katsuda, Y.; Miura, S.-i. Associations between High-Density Lipoprotein Functionality and Major Adverse Cardiovascular Events in Patients Who Have Undergone Coronary Computed Tomography Angiography. J. Clin. Med. 2021, 10, 2431. https://doi.org/10.3390/jcm10112431
Inoue H, Shiga Y, Norimatsu K, Tashiro K, Futami M, Suematsu Y, Sugihara M, Nishikawa H, Katsuda Y, Miura S-i. Associations between High-Density Lipoprotein Functionality and Major Adverse Cardiovascular Events in Patients Who Have Undergone Coronary Computed Tomography Angiography. Journal of Clinical Medicine. 2021; 10(11):2431. https://doi.org/10.3390/jcm10112431
Chicago/Turabian StyleInoue, Hiroko, Yuhei Shiga, Kenji Norimatsu, Kohei Tashiro, Makito Futami, Yasunori Suematsu, Makoto Sugihara, Hiroaki Nishikawa, Yousuke Katsuda, and Shin-ichiro Miura. 2021. "Associations between High-Density Lipoprotein Functionality and Major Adverse Cardiovascular Events in Patients Who Have Undergone Coronary Computed Tomography Angiography" Journal of Clinical Medicine 10, no. 11: 2431. https://doi.org/10.3390/jcm10112431
APA StyleInoue, H., Shiga, Y., Norimatsu, K., Tashiro, K., Futami, M., Suematsu, Y., Sugihara, M., Nishikawa, H., Katsuda, Y., & Miura, S. -i. (2021). Associations between High-Density Lipoprotein Functionality and Major Adverse Cardiovascular Events in Patients Who Have Undergone Coronary Computed Tomography Angiography. Journal of Clinical Medicine, 10(11), 2431. https://doi.org/10.3390/jcm10112431