
Investigation of the Efficiency of Mask Wearing, Contact Tracing, and Case Isolation during the COVID-19 Outbreak


Abstract
:1. Introduction
2. Methods
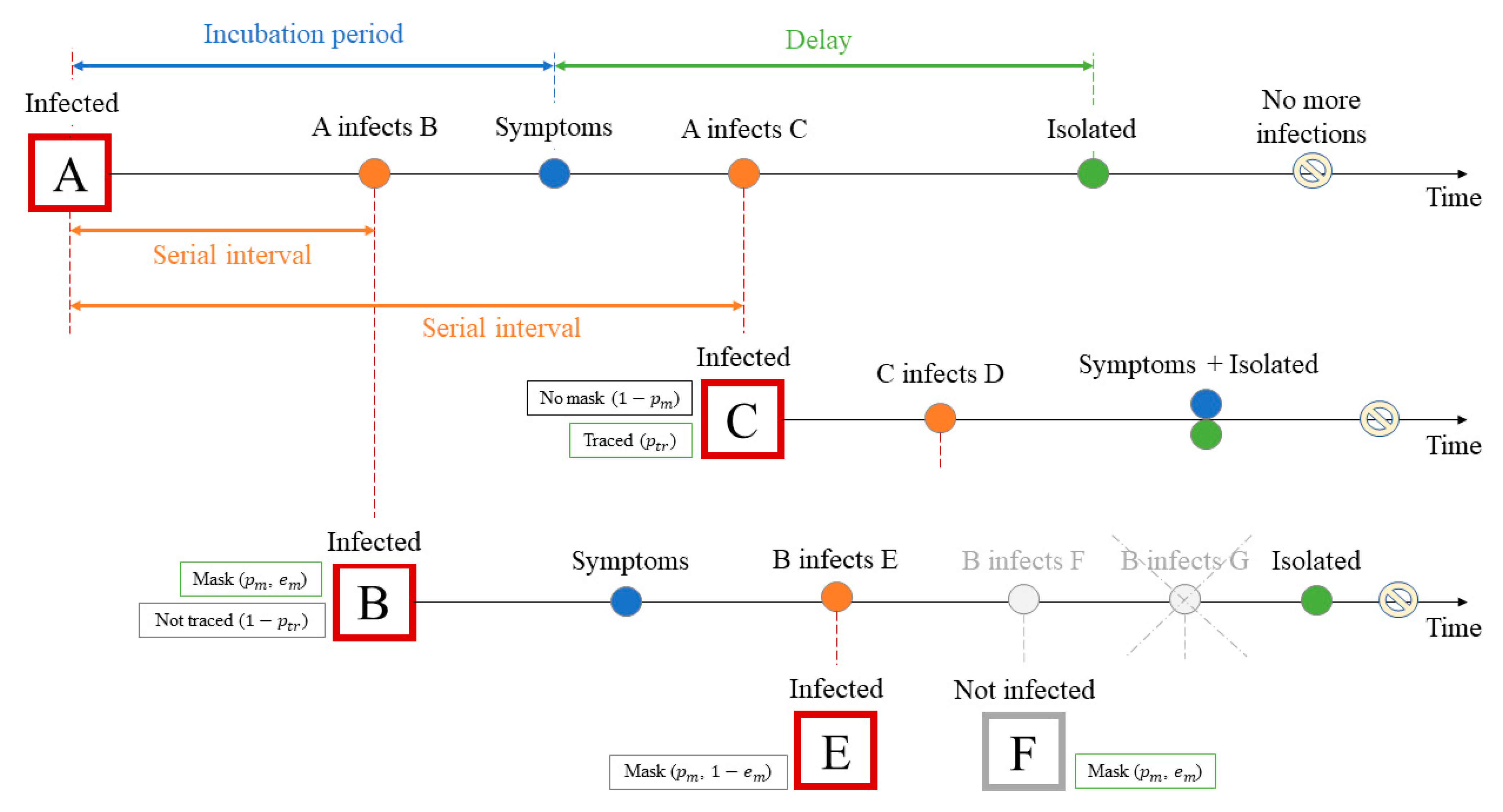
2.1. Stochastic Transmission Model
2.2. Threshold Value for and Outbreak Control
2.3. Time Data for the Transmission Model
2.4. Mask Wearing
- (1)
- (2)
- (3)
2.5. SARS-CoV-2 Infection Parameters
3. Results
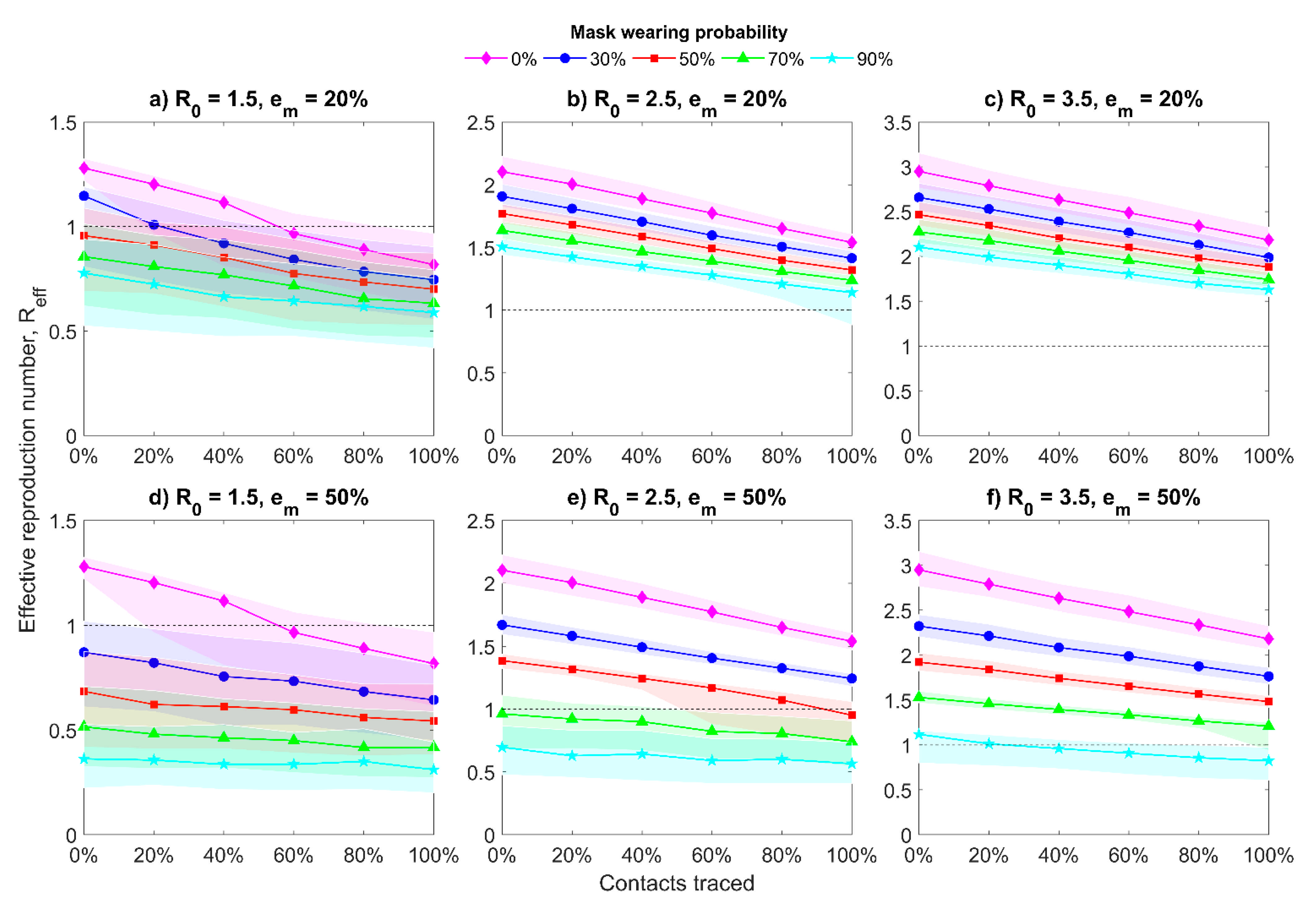
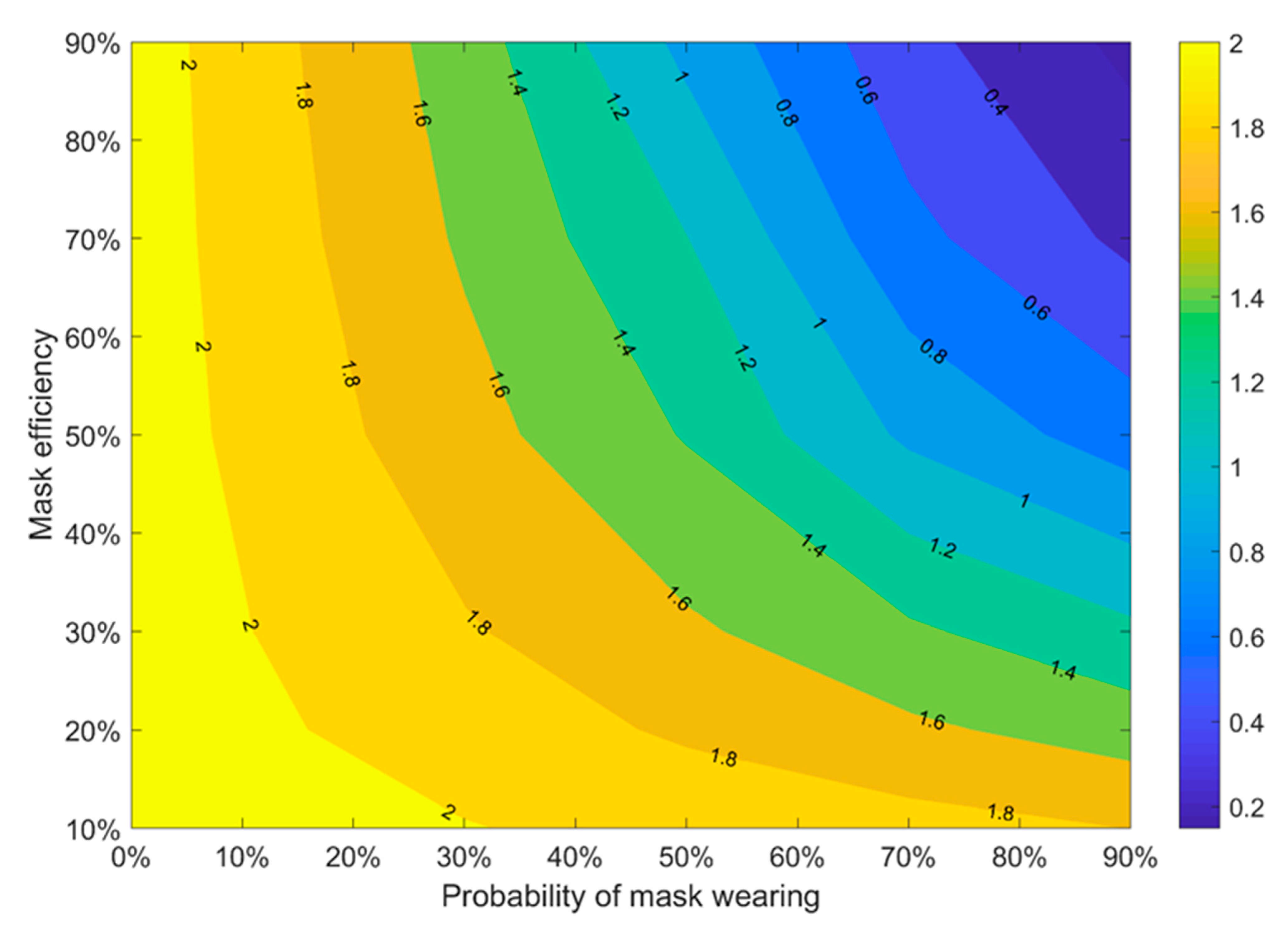
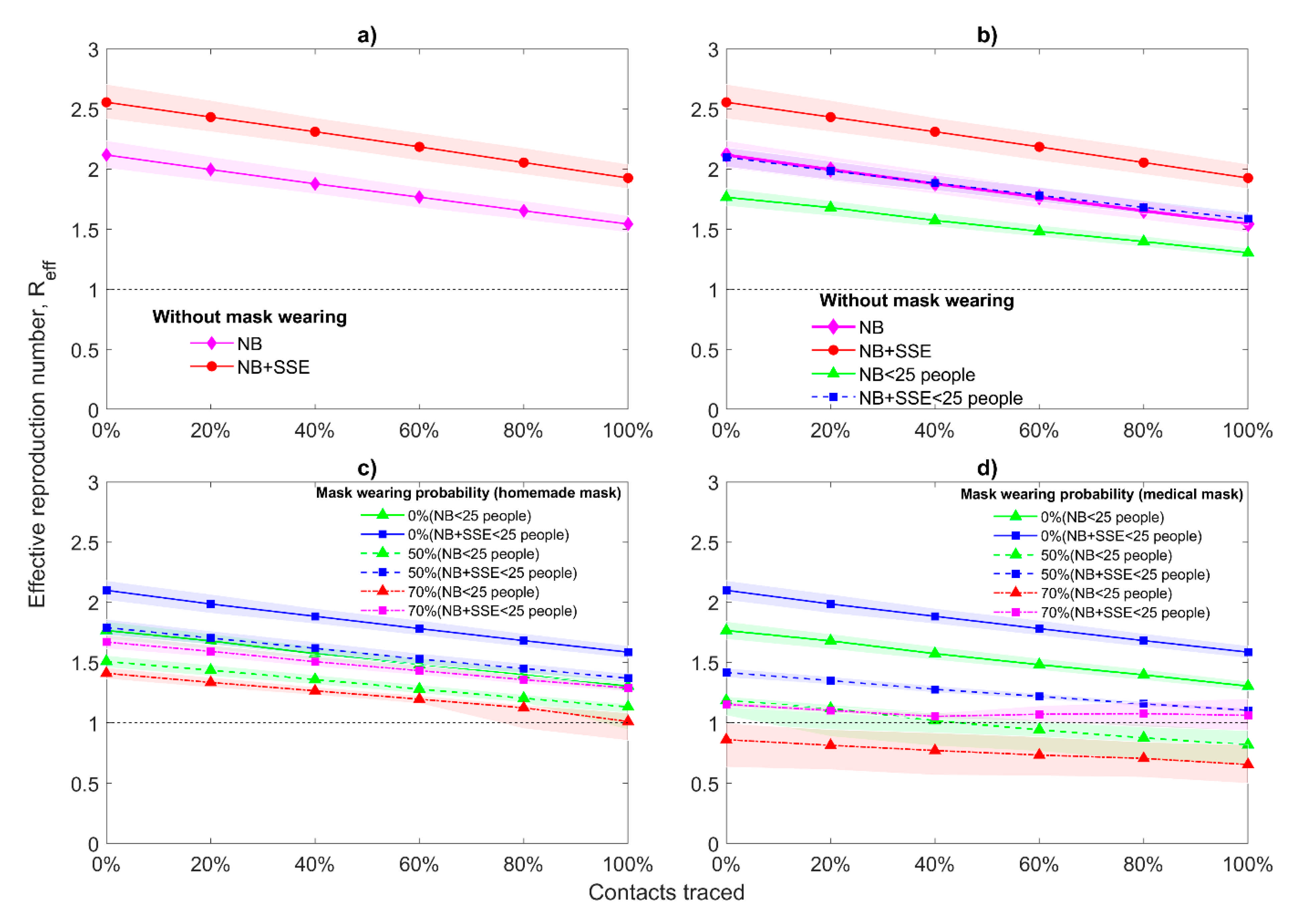
3.1. Effective Reproduction Number
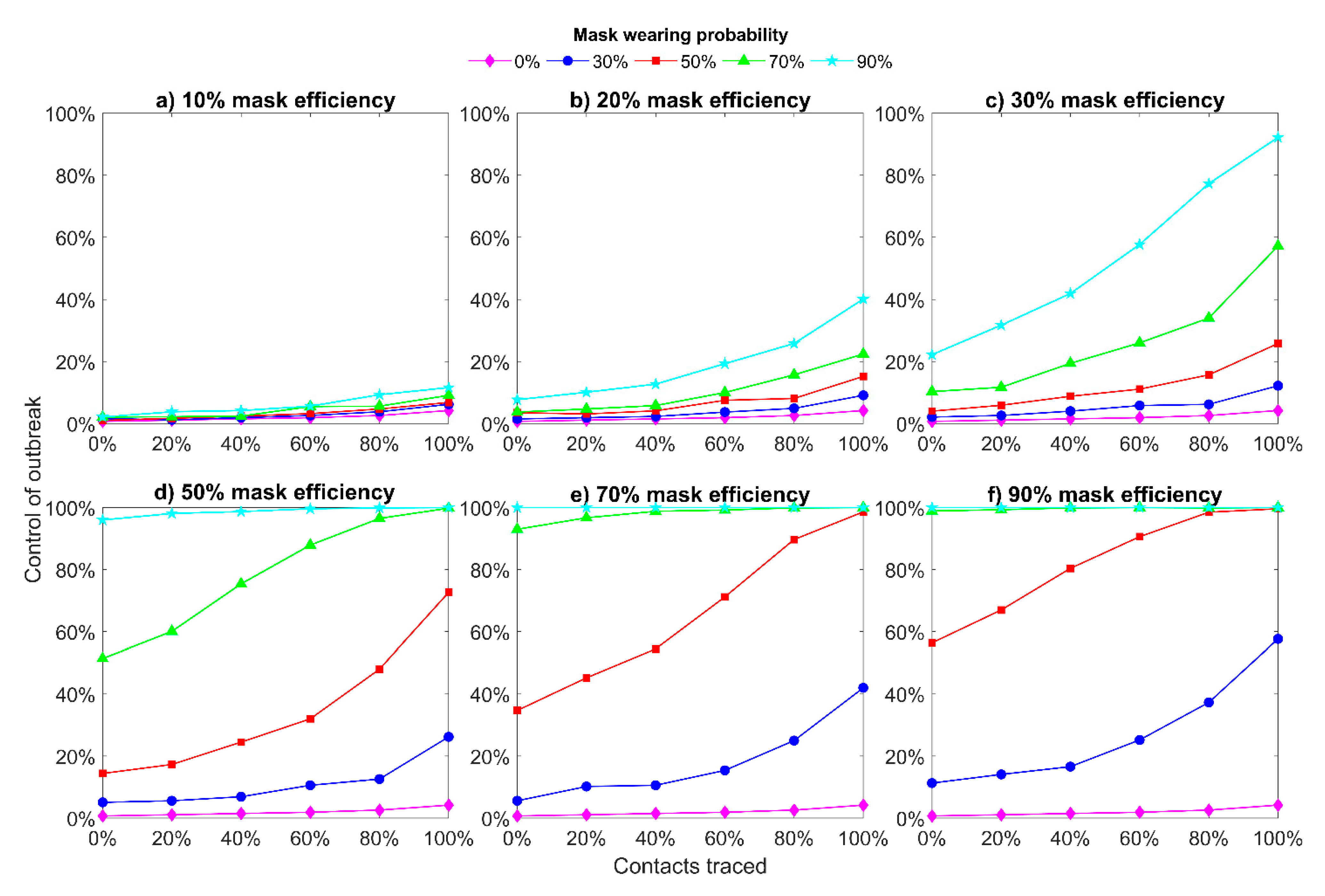
3.2. Outbreak Control
3.3. Superspreading Events
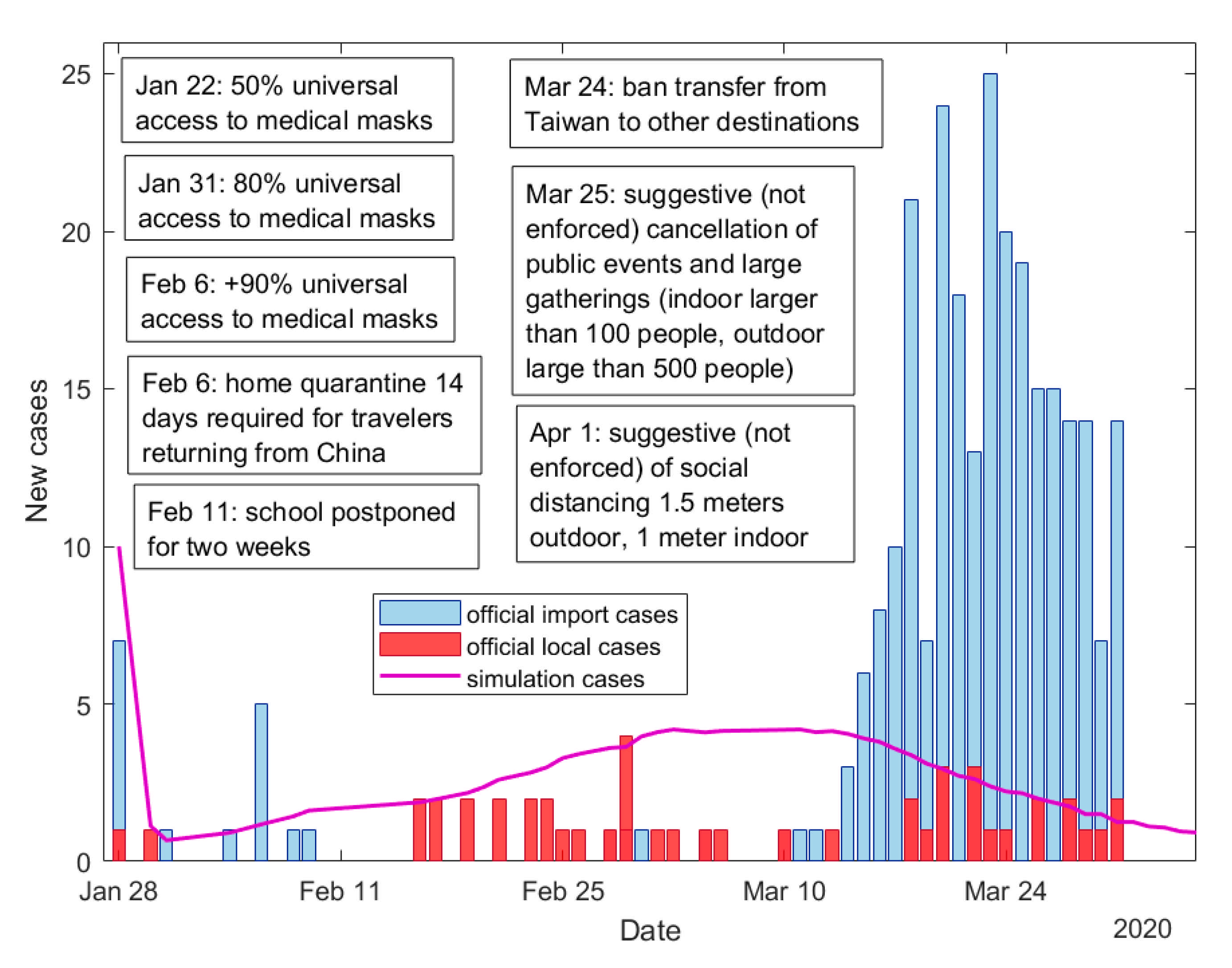
3.4. Comparison with Official Taiwanese Data
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 13 January 2021).
- Fraser, C.; Riley, S.; Anderson, R.M.; Ferguson, N.M. Factors that make an infectious disease outbreak controllable. Proc. Natl. Acad. Sci. USA 2004, 101, 6146–6151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Rational Use of Personal Protective Equipment for Coronavirus Disease (COVID-19) and Considerations during Severe Shortages. Available online: https://www.who.int/publications/i/item/rational-use-of-personal-protective-equipment-for-coronavirus-disease-(covid-19)-and-considerations-during-severe-shortages (accessed on 13 January 2021).
- Advice on the Use of Masks in the Context of COVID-19. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-IPC_Masks-Children-2020.1 (accessed on 13 January 2021).
- Oran, D.P.; Topol, E.J. Prevalence of asymptomatic SARS-CoV-2 infection: A narrative review. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Yi, G.Y.; Zhu, Y. Estimation of the basic reproduction number, average incubation time, asymptomatic infection rate, and case fatality rate for COVID-19: Meta-analysis and sensitivity analysis. J. Med. Virol. 2020, 92, 2543–2550. [Google Scholar] [CrossRef]
- He, D.; Zhao, S.; Lin, Q.; Zhuang, Z.; Cao, P.; Wang, M.H.; Yang, L. The relative transmissibility of asymptomatic COVID-19 infections among close contacts. Int. J. Infect. Dis. 2020, 94, 145–147. [Google Scholar] [CrossRef]
- Byambasuren, O.; Cardona, M.; Bell, K.; Clark, J.; McLaws, M.-L.; Glasziou, P. Estimating the extent of true asymptomatic COVID-19 and its potential for community transmission: Systematic review and meta-analysis. JAMMI 2020, 5, 223–234. [Google Scholar] [CrossRef]
- Long, Q.; Tang, X.-J.; Shi, Q.-L.; Li, Q.; Deng, H.-J.; Yuan, J.; Hu, J.-L.; Xu, W.; Zhang, Y.; Lv, F.-J.; et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef]
- COVID-19 Vaccine Doses Administered per 100 People. Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer?tab=map&zoomToSelection=true&time=latest&pickerSort=desc&pickerMetric=population&Metric=Vaccinations&Interval=Cumulative&Relative+to+Population=true&Align+outbreaks=false&country=USA~ISR~GBR~ARE~OWID_WRL~EuropeanUnion~BRA~CHN~IDN~BGD~RUS~MEX~CHL (accessed on 23 March 2021).
- Moore, S.; Hill, E.M.; Tildesley, M.J.; Dyson, L.; Keeling, M.J. Vaccination and non-pharmaceutical interventions for COVID-19: A mathematical modelling study. Lancet Infect. Dis. 2021, 21, 793–802. [Google Scholar] [CrossRef]
- Gao, W.; Sanna, M.; Huang, G.; Hefler, M.; Tsai, M.-K.; Wen, C.-P. Examining population health during the COVID-19 Pandemic: All-cause, pneumonia and influenza, and road traffic deaths in Taiwan. Ann. Intern. Med. 2021, 174, 880–882. [Google Scholar] [CrossRef]
- Leung, N.H.L.; Chu, D.K.W.; Shiu, E.Y.C.; Chan, K.-H.; McDevitt, J.J.; Hau, B.J.P.; Yen, H.-L.; Li, Y.; Ip, D.K.M.; Malik Peiris, J.S.; et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat. Med. 2020, 26, 676–680. [Google Scholar] [CrossRef] [Green Version]
- Anfinrud, P.; Bax, C.E.; Stadnytskyi, V.; Bax, A. Could SARS-CoV-2 be transmitted via speech droplets? medRxiv 2020. [Google Scholar] [CrossRef]
- Ong, S.W.X.; Tan, Y.K.; Chia, P.Y.; Lee, T.H.; Ng, O.T.; Wong, M.S.J.; Marimuthu, K. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA 2020, 323, 1610–1612. [Google Scholar] [CrossRef] [Green Version]
- Bourouiba, L. Turbulent gas clouds and respiratory pathogen emissions: Potential implications for reducing transmission of COVID-19. JAMA 2020, 323, 1837–1838. [Google Scholar] [CrossRef]
- Visualization of Air Spread when Coughing. Available online: https://youtu.be/MX8InIv0sXs (accessed on 13 June 2020).
- Guidance for Wearing Masks. Help Slow the Spread of COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cloth-face-cover-guidance.html (accessed on 17 May 2021).
- Scientific Brief: Community Use of Cloth Masks to Control the Spread of SARS-CoV-2. Available online: https://www.cdc.gov/coronavirus/2019-ncov/more/masking-science-sars-cov2.html?fbclid=IwAR28PppCa6×2uxwO8Z2baHM0KHS4JXx0inzzMQs3zRHV1qql_0a8mxZfpCw (accessed on 17 May 2021).
- Using Face Masks in the Community: First Update—Effectiveness in Reducing Transmission of COVID-19. Available online: https://www.ecdc.europa.eu/en/publications-data/using-face-masks-community-reducing-covid-19-transmission (accessed on 17 May 2021).
- Rengasamy, S.; Eimer, B.; Shaffer, R.E. Simple respiratory protection—Evaluation of the filtration performance of cloth masks and common fabric materials against 20–1000 nm size particles. Ann. Occup. Hyg. 2010, 54, 789–798. [Google Scholar]
- Davies, A.; Thompson, K.-A.; Giri, K.; Kafatos, G.; Walker, J.; Bennett, A. Testing the efficacy of homemade masks: Would they protect in an influenza pandemic? Disaster Med. Public Health Prep. 2013, 7, 413–418. [Google Scholar] [CrossRef]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, e488–e496. [Google Scholar] [CrossRef] [Green Version]
- Wong, F.; Collins, J.J. Evidence that coronavirus superspreading is fat-tailed. Proc. Natl. Acad. Sci. USA 2020, 117, 29416–29418. [Google Scholar] [CrossRef]
- Cheng, Y.; Ma, N.; Witt, C.; Rapp, S.; Wild, P.S.; Andreae, M.O.; Pöschl, U.; Su, H. Face masks effectively limit the probability of SARS-CoV-2 transmission. Science 2021. [Google Scholar] [CrossRef]
- Endo, A. Centre for the Mathematical Modelling of Infectious Diseases COVID-19 Working Group; Abbott, S.; Kucharski, A.J.; Funk, S. Estimating the overdispersion in COVID-19 transmission using outbreak sizes outside China [version 3; peer review: 2 approved]. Wellcome Open Res. 2020, 5, 67. [Google Scholar] [CrossRef]
- Lloyd-Smith, J.O.; Schreiber, S.J.; Kopp, P.E.; Getz, W.M. Superspreading and the effect of individual variation on disease emergence. Nature 2005, 438, 355–359. [Google Scholar] [CrossRef]
- Johnson, N.L.; Kemp, A.W.; Kotz, S. Univariate Discrete Distributions, 3rd ed.; Wiley: Hoboken, NJ, USA, 2005. [Google Scholar]
- Adam, D.C.; Wu, P.; Wong, J.Y.; Lau, E.H.Y.; Tsang, T.K.; Cauchemez, S.; Leung, G.M.; Cowling, B.J. Clustering and superspreading potential of SARS-CoV-2 infections in Hong Kong. Nat. Med. 2020, 26, 1714–1719. [Google Scholar] [CrossRef]
- Abbott, S.; Hellewell, J.; Munday, J.; Funk, S. The transmissibility of novel Coronavirus in the early stages of the 2019-20 outbreak in Wuhan: Exploring initial point-source exposure sizes and durations using scenario analysis [version 1; peer review: 2 approved]. Wellcome Open Res. 2020, 5, 17. [Google Scholar] [CrossRef] [Green Version]
- Imai, N.; Dorigatti, I.; Cori, A.; Riley, S.; Ferguson, N.M. Report 2: Estimating the potential total number of novel coronavirus cases in Wuhan City, China. Imp. Coll. Lond. 2020. [Google Scholar] [CrossRef]
- Nishiura, H.; Chowell, G. Mathematical and Statistical Estimation Approaches in Epidemiology; Springer: Dordrecht, The Netherlands, 2009; pp. 103–121. [Google Scholar]
- MacIntyre, C.R.; Cauchemez, S.; Dwyer, D.E.; Seale, H.; Cheung, P.; Browne, G.; Fasher, M.; Wood, J.; Gao, Z.; Booy, R.; et al. Face mask use and control of respiratory virus transmission in households. Emerg. Infect. Dis. 2009, 15, 233–241. [Google Scholar] [CrossRef]
- Verma, S.; Dhanak, M.; Frankenfield, J. Visualizing the effectiveness of face masks in obstructing respiratory jets. Phys. Fluids 2020, 32, 061708. [Google Scholar] [CrossRef]
- Sahafizadeh, E.; Sartoli, S. Estimating the reproduction number of COVID-19 in Iran using epidemic modeling. J. Travel Med. 2020, 27, taaa077. [Google Scholar] [CrossRef]
- Zhuang, Z.; Zhao, S.; Lin, Q.; Cao, P.; Lou, Y.; Yang, L.; Yang, S.; He, D.; Xiao, L. Preliminary estimates of the reproduction number of the coronavirus disease (COVID-19) outbreak in Republic of Korea and Italy by 5 March 2020. Int. J. Infect. Dis. 2020, 95, 308–310. [Google Scholar] [CrossRef]
- Kucharski, A.J.; Eggo, R.M.; Watson, C.H.; Camacho, A.; Funk, S.; Edmunds, W.J. Effectiveness of ring vaccination as control strategy for Ebola virus disease. Emerg. Infect. Dis. 2016, 22, 105–108. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 Pandemic Planning Scenarios. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html (accessed on 17 May 2021).
- Backer, J.A.; Klinkenberg, D.; Wallinga, J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China. Euro Surveill. 2020, 25, 2000062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, C.A.; Ghani, A.C.; Leung, G.M.; Hedley, A.J.; Fraser, C.; Riley, S.; Abu-Raddad, L.J.; Ho, L.-M.; Thach, T.-Q.; Chau, P.; et al. Epidemiological determinants of spread of causal agent of severe acute respiratory syndrome in Hong Kong. Lancet 2003, 361, 1761–1766. [Google Scholar] [CrossRef] [Green Version]
- A Bravery Story—A Taiwan National Machine Tool Team for Surgical Mask Production Born to Fight Against Covid-19 Outbreak. Available online: https://www.trade.gov.tw/English/Pages/Detail.aspx?nodeID=855&pid=692054 (accessed on 13 January 2021).
- Jian, S.W.; Cheng, H.Y.; Huang, X.T.; Liu, D.P. Contact tracing with digital assistance in Taiwan’s COVID-19 outbreak response. Int. J. Infect. Dis. 2020, 101, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Imai, N.; Cori, A.; Dorigatti, I.; Baguelin, M.; Donnelly, C.A.; Riley, S.; Ferguson, N.M. Report 3: Transmissibility of 2019-nCoV. Imp. Coll. Lond. 2020. [Google Scholar] [CrossRef]
- Wang, C.J.; Ng, C.Y.; Brook, R.H. Response to COVID-19 in Taiwan: Big data analytics, new technology, and proactive testing. JAMA 2020, 323, 1341–1342. [Google Scholar] [CrossRef]
- Wong, J. Combating COVID-19 in Democratic Taiwan and South Korea. Curr. Hist. 2020, 119, 210–216. [Google Scholar] [CrossRef]
- Taiwan Centers for Disease Control. Press Releases. Available online: https://www.cdc.gov.tw/En/Bulletin/List/7tUXjTBf6paRvrhEl-mrPg (accessed on 13 June 2021).
- Kim, S.; Jeong, Y.D.; Byun, J.H.; Cho, G.; Park, A.; Jung, J.H.; Roh, Y.; Choi, S.; Muhammad, I.M.; Jung, I.H. Evaluation of COVID-19 epidemic outbreak caused by temporal contact-increase in South Korea. Int. J. Infect. Dis. 2020, 96, 454–457. [Google Scholar] [CrossRef]
- Heating, Ventilation and Air-Conditioning Systems in the Context of COVID-19. Available online: https://www.ecdc.europa.eu/en/publications-data/heating-ventilation-air-conditioning-systems-covid-19 (accessed on 13 January 2021).
- Coronavirus Disease (COVID-19) Advice for the Public: When and How to Use Masks. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks (accessed on 13 January 2021).
- How to Protect Yourself & Others. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html (accessed on 17 May 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Value | Reference | ||
|---|---|---|---|
| Fixed | |||
| Initial symptomatic cases | 5; 20; 40; 50; 100 | Tested | |
| Initial asymptomatic cases | 0; 20; 50; 100 | Tested | |
| Reproduction number | 1.5; 2.5; 3.5 | [24,32,38] | |
| Dispersion parameter for negative binomial distribution | 0.1 | [27] | |
| Tail parameter for Fréchet distribution | 1.7 | [25] | |
| Isolation efficiency | 100% | [24] | |
| Proportion of transmission before symptoms onset | 40% | [3] | |
| Proportion of asymptomatic cases (produced from symptomatic) | 15% | [8] | |
| Proportion of asymptomatic cases (produced from asymptomatic) | 50% | [8] | |
| Infectivity of asymptomatic cases | 0.75· | [39] | |
| Percentage of contacts traced | 0%; 20%; 40%; 60%; 80%; 100% | [24] | |
| Mask efficiency | 10%; 20%; 30%; 50%; 70%; 90% | [14,22,34] | |
| Mask wearing probability | 0%; 30%; 50%; 70%; 90% | Tested | |
| Sampled | Mean | Standard deviation | |
| Incubation period | 5.75 | 2.63 | [40] |
| Serial interval | Incubation period | 2 | [24] |
| Delay between symptoms onset and isolation time | 3.83 | 2.38 | [41] |
| The infection shedding period for asymptomatic cases | 19 | 8.15 | [10] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filonets, T.; Solovchuk, M.; Gao, W.; Sheu, T.W.-H. Investigation of the Efficiency of Mask Wearing, Contact Tracing, and Case Isolation during the COVID-19 Outbreak. J. Clin. Med. 2021, 10, 2761. https://doi.org/10.3390/jcm10132761
Filonets T, Solovchuk M, Gao W, Sheu TW-H. Investigation of the Efficiency of Mask Wearing, Contact Tracing, and Case Isolation during the COVID-19 Outbreak. Journal of Clinical Medicine. 2021; 10(13):2761. https://doi.org/10.3390/jcm10132761
Chicago/Turabian StyleFilonets, Tatiana, Maxim Solovchuk, Wayne Gao, and Tony Wen-Hann Sheu. 2021. "Investigation of the Efficiency of Mask Wearing, Contact Tracing, and Case Isolation during the COVID-19 Outbreak" Journal of Clinical Medicine 10, no. 13: 2761. https://doi.org/10.3390/jcm10132761
APA StyleFilonets, T., Solovchuk, M., Gao, W., & Sheu, T. W. -H. (2021). Investigation of the Efficiency of Mask Wearing, Contact Tracing, and Case Isolation during the COVID-19 Outbreak. Journal of Clinical Medicine, 10(13), 2761. https://doi.org/10.3390/jcm10132761