
Levels of Biological Markers of Nitric Oxide in Serum of Patients with Mandible Fractures


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Blood Sampling
2.2. Determination of Total NO Concentration in Serum
2.3. Determination of Malonodialdehyde (MDA) Concentration in Serum
2.4. Determination of Nitrotyrosine Concentration in Serum
2.5. Determination of Asymmetrical Dimethylarginine (ADMA) Concentration in Serum
2.6. Statistical Evaluation
3. Results
3.1. MDA Concentration in Patient Serum
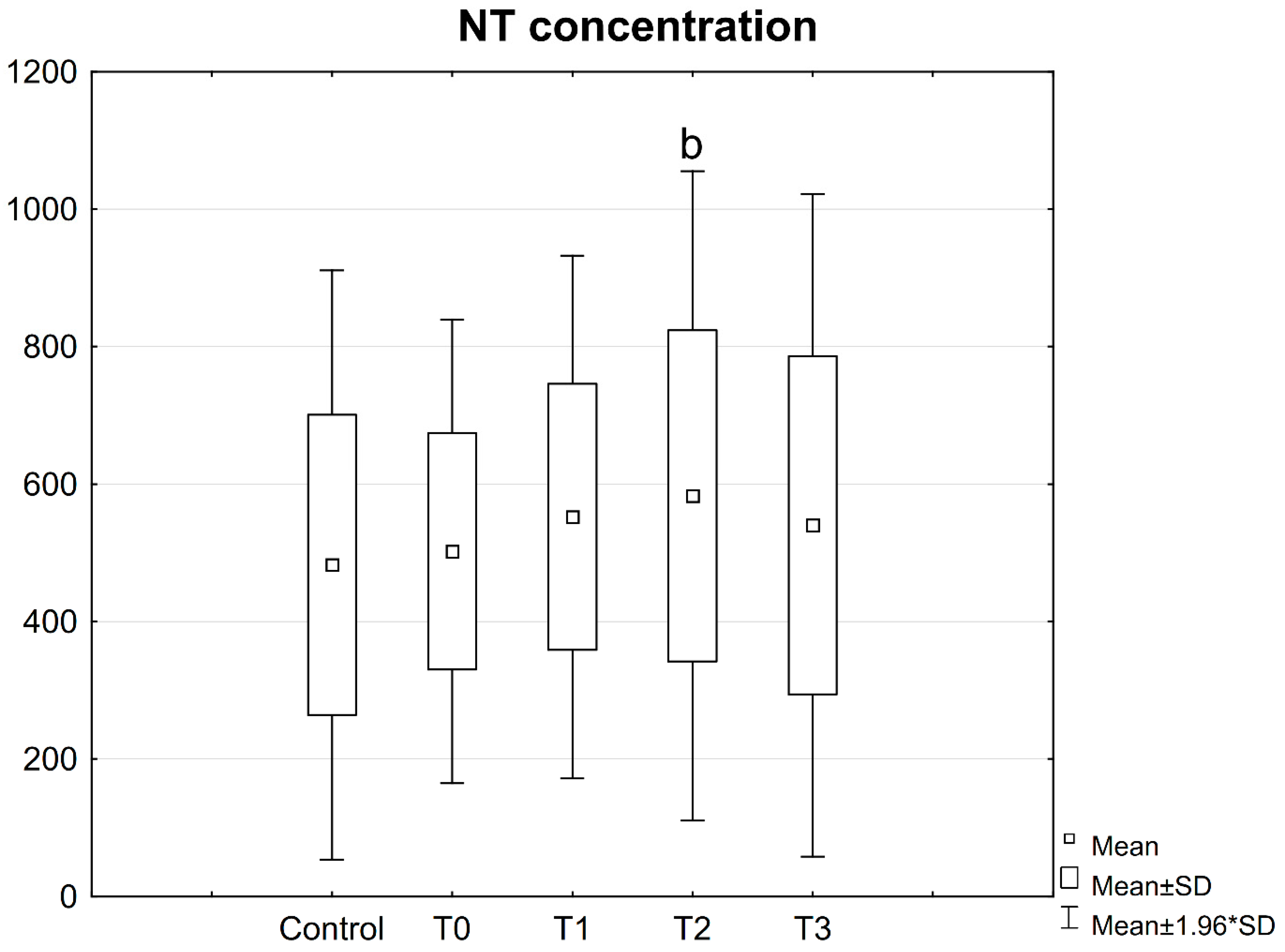
3.2. NT Concentration in Patient Serum
3.3. ADMA Concentration in Patient Serum
3.4. Correlations
3.5. Differences in Terms of the Number of Fractures
3.6. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
Abbreviations
References
- Scott, A.; Khan, K.M.; Cook, J.L.; Duronio, V. What is “inflammation”? Are we ready to move beyond Celsus? Br. J. Sports Med. 2004, 38, 248–249. [Google Scholar]
- Yao, Y.M.; Redl, H.; Bahrami, S.; Schlag, G. The inflammatory basis of trauma/shock-associated multiple organ failure. Inflamm. Res. 1998, 47, 201–210. [Google Scholar] [CrossRef]
- Lenz, A.; Franklin, G.A.; Cheadle, W.G. Systemic inflammation after trauma. Injury 2007, 38, 1336–1345. [Google Scholar] [CrossRef]
- Van’t Hof, R.J.; Ralston, S.H.J. Nitric oxide and bone. Immunology 2001, 103, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Klein-Nulend, J.; van Oers, R.F.M.; Bakker, A.D.; Bacabac, R.G. Nitric oxide signaling in mechanical adaptation of bone. Osteoporosis Int. 2014, 25, 1427–1437. [Google Scholar] [CrossRef]
- Teitelbaum, S.L. Bone resorption by osteoclasts. Science 2000, 289, 1504–1508. [Google Scholar] [CrossRef]
- Caetano-Lopes, J.; Canhão, H.; Fonseca, J.E. Osteoblasts and bone formation. Acta Reumatol. Port. 2007, 32, 103–110. [Google Scholar]
- Probst, A.; Spiegel, H.U. Cellular mechanisms of bone repair. J. Investig. Surg. 1997, 10, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Q.; Dai, K.R.; Qiu, S.J.; Zhu, Z.A. Bone remodeling after internal fixation with diffrenet stiffness plates: Ultrastructural investigation. Chin. Med. J. 1994, 107, 766–770. [Google Scholar] [PubMed]
- Zacharidades, N.; Mezitis, M.; Rallis, G. An audit of mandibular fractures treated by intermaxillary fixation, intraosseous wiring and compression plating. Brit. J. Oral. Maxillofac. Surg. 1996, 34, 293–297. [Google Scholar] [CrossRef]
- Faist, E.; Schinkel, C.; Zimmer, S. Update on the mechanisms of immune suppression of injury and immune modulation. World J. Surg. 1996, 20, 454–459. [Google Scholar] [CrossRef]
- Shijo, H.; Iwabuchi, K.; Hosoda, S.; Watanabe, H.; Nagaoka, I.; Sakakibara, N. Evaluation of neutrophil functions after experimental abdominal surgical trauma. Inflamm. Res. 1998, 47, 67–74. [Google Scholar] [CrossRef]
- Cederberg, D.; Siesjö, P. What has inflammation to do with traumatic brain injury? Childs. Nerv. Syst. 2010, 26, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Saura, M.; Tarin, C.; Zaragoza, C. Recent insights into the implication of nitric oxide in osteoblast differentiation and proliferation during bone development. Sci. World J. 2010, 10, 624–632. [Google Scholar] [CrossRef] [Green Version]
- Ralston, S.H. The Michael Mason Prize Essay. Nitric oxide and bone: What a gas! Br. J. Rheumatol. 1997, 36, 831–838. [Google Scholar] [CrossRef] [Green Version]
- Diwan, A.D.; Wang, M.X.; Jang, D.; Zhu, W.; Murrell, G.A. Nitric oxide modulates fracture healing. J. Bone. Miner. Res. 2000, 15, 342–351. [Google Scholar] [CrossRef]
- Kalyanaraman, H.; Schall, N.; Pilz, R.B. Nitric oxide and cyclic GMP functions in bone. Nitric Oxide 2018, 76, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Rochette, L.; Lorin, J.; Zeller, M.; Guilland, J.C.; Lorgis, L.; Cottin, Y.; Vergely, C. Nitric oxide synthase inhibition and oxidative stress in cardiovascular diseases: Possible therapeutic targets? Pharmacol. Ther. 2013, 140, 239–257. [Google Scholar] [CrossRef] [PubMed]
- Dymara-Konopka, W.; Laskowska, M. The role of nitric oxide, ADMA, and homocysteine in the etiopathogenesis of preeclampsia-review. Int. J. Mol. Sci. 2019, 5, 2757. [Google Scholar] [CrossRef] [Green Version]
- Vatsa, A.; Smit, T.H.; Klein-Nulend, J. Extracellular NO signalling from a mechanically stimulated osteocyte. J. Biomech. 2007, 1, S89–S95. [Google Scholar] [CrossRef]
- Chow, J.W. Role of nitric oxide and prostaglandins in the bone formation response to mechanical loading. Exerc. Sport Sci. Rev. 2000, 28, 185–188. [Google Scholar]
- Turner, C.H.; Owan, I.; Jacob, D.S.; McClintock, R.; Peacock, M. Effects of nitric oxide synthase inhibitors on bone formation in rats. Bone 1997, 21, 487–490. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Rationale for using nitric oxide donor therapy for prevention of bone loss and treatment of osteoporosis in humans. Ann. N. Y. Acad. Sci. 2007, 1117, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Heinonen, I.; Boushel, R.; Hellsten, Y.; Kalliokoski, K. Regulation of bone blood flow in humans: The role of nitric oxide, prostaglandins, and adenosine. Scand. J. Med. Sci. Sports 2018, 28, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Klein-Nulend, J.; van der Plas, A.; Semeins, C.M.; Ajubi, N.E.; Frangos, J.A.; Nijweide, P.J.; et al. Sensitivity of osteocytes to biomechanical stress in vitro. FASEB J. 1995, 9, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Corbett, S.A.; Hukkanen, M.; Batten, J.; McCarthy, I.D.; Polak, J.M.; Hughes, S.P. Nitric oxide in fracture repair. Differential localisation, expression and activity of nitric oxide synthases. J. Bone Joint. Surg. Br. 1999, 81, 531–537. [Google Scholar] [CrossRef]
- Keskin, D.; Kiziltunc, A. Time-dependent changes in serum nitric oxide levels after long bone fracture. Tohoku J. Exp. Medy. 2007, 213, 283–289. [Google Scholar] [CrossRef] [Green Version]
- Prasad, G.; Dhillon, M.S.; Khullar, M.; Nagi, O.N. Evaluation of oxidative stress after fractures. A preliminary study. Acta Orthop. Belg. 2003, 69, 546–551. [Google Scholar]
- Anderson, S.M.; Naidoo, R.N.; Pillay, Y.; Tiloke, C.; Muttoo, S.; Asharam, K.; Chuturgoon, A.A. HIV induced nitric oxide and lipid peroxidation, influences neonatal birthweight in a South African population. Environ. Int. 2018, 21, 1–12. [Google Scholar] [CrossRef]
- Tsikas, D. Assessment of lipid peroxidation by measuring malondialdehyde (MDA) and relatives in biological samples: Analytical and biological challenges. Anal Biochem. 2017, 5, 13–30. [Google Scholar] [CrossRef]
- Del Rio, D.; Stewart, A.J.; Pellegrini, N. A review of recent studies on malondialdehyde as toxic molecule and biological marker of oxidative stress. Nutr. Metab. Cardiovasc. Dis. 2005, 15, 316–328. [Google Scholar] [CrossRef] [PubMed]
- Göktürk, E.; Turgut, A.; Bayçu, C.; Günal, I.; Seber, S.; Gülbas, Z. Oxygen-free radicals impair fracture healing in rats. Acta Orthop. Scand. 1995, 66, 473–475. [Google Scholar] [CrossRef]
- Ahsan, H. 3-Nitrotyrosine: A biomarker of nitrogen free radical species modified proteins in systemic autoimmunogenic conditions. Hum. Immunol. 2013, 74, 1392–1399. [Google Scholar] [CrossRef] [PubMed]
- Yeo, W.S.; Lee, S.J.; Lee, J.R.; Kim, K.P. Nitrosative protein tyrosine modifications: Biochemistry and functional significance. J. Biochem. Mol. Biol. 2008, 41, 194–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saimanen, I.; Rahkola, D.; Kuosmanen, V.; Kärkkäinen, J.; Selander, T.; Holopainen, A.; Aspinen, S.; Eskelinen, M. Nitrotyrosine (NT), a nitrosative stress biomarker, plasma concentrations in gallstone disease and cancer patients. Anticancer Res. 2019, 39, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Yang, H.; Mu, J.; Lu, T.; Peng, J.; Deng, X.; et al. Nitric oxide regulates protein methylation during stress responses in plants. Mol. Cell 2017, 67, 702–710. [Google Scholar] [CrossRef]
- Fulton, M.D.; Brown, T.; Zheng, Y.G. The biological axis of protein arginine methylation and asymmetric dimethylarginine. Int. J. Mol. Sci. 2019, 20, 3322. [Google Scholar] [CrossRef] [Green Version]
- Kielstein, J.T.; Cooke, J.P. Should we measure asymmetric dimethylarginine in patients with coronary artery disease? Clin. Chem. 2007, 53, 161–163. [Google Scholar] [CrossRef] [Green Version]
- Fleszar, M.G.; Wisniewski, J.; Zboch, M.; Diakowska, D.; Gamian, A.; Krzystek-Korpacka, M. Targeted metabolomic analysis of nitric oxide/L-arginine pathway metabolites in dementia: Association with pathology, severity, and structural brain changes. Sci. Rep. 2019, 9, 13764. [Google Scholar] [CrossRef] [PubMed]
- De Gennaro Colonna, V.; Bianchi, M.; Pascale, V.; Ferrario, P.; Morelli, F.; Pascale, W.; Tomasoni, L.; Turiel, M. Asymmetric dimethylarginine (ADMA): An endogenous inhibitor of nitric oxide synthase and a novel cardiovascular risk molecule. Med. Sci. Monit. 2009, 15, RA91–RA101. [Google Scholar]
- Chen, S.; Li, N.; Deb-Chatterji, M.; Dong, Q.; Kielstein, J.T.; Weissenborn, K.; Worthmann, H. Asymmetric dimethyarginine as marker and mediator in ischemic stroke. Int. J. Mol. Sci. 2012, 13, 15983–16004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Leitner, E.C.; Klinke, A.; Atzler, D.; Slocum, J.L.; Lund, N.; Kielstein, J.T.; et al. Pathogenic cycle between the endogenous nitric oxide synthase inhibitor asymmetrical dimethylarginine and the leukocyte-derived hemoprotein myeloperoxidase. Circulation 2011, 124, 2735–2745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, Z.S.; Quarles, L.D.; Chen, Q.Q.; Yu, Y.H.; Qu, X.P.; Jiang, C.H.; et al. Effect of asymmetric dimethylarginine on osteoblastic differentiation. Kidney Int. 2001, 60, 1699–1704. [Google Scholar] [CrossRef] [Green Version]
- Kanazawa, I.; Yano, S.; Yamaguchi, T.; Notsu, Y.; Nabika, T.; Sugimoto, T. Relationships between dimethylarginine and the presence of vertebral fractures in type 2 diabetes mellitus. Clin. Endocrinol. 2010, 73, 463–468. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 15) | Patients (n = 20) | ||
|---|---|---|---|
| Parameter (Unit) | Value | Value | Reference Value |
| WBC (×103/μL) | 7.28 ± 2.5 | 11.16 ± 3.8 | 4.00–10.00 |
| RBC (×106/μL) | 4.94 ± 0.21 | 4.83 ± 0.3 | 4.50–6.50 |
| HGB (g/dL) | 13.7 ± 0.5 | 14.93 ± 0.9 | 13.00–18.00 |
| HCT (%) | 45.26 ± 3.42 | 42.40 ± 2.3 | 40.00–54.00 |
| MCV (fL) | 87.04 ± 2.9 | 88.03 ± 3.5 | 82.00–94.00 |
| MCH (pg) | 29.28 ± 1.9 | 31.00 ± 1.4 | 27.00–34.00 |
| MCHC (g/dL) | 33.74 ± 0.6 | 35.21 ± 0.8 | 31.00–37.00 |
| RDW-SD (fL) | 42.39 ± 3.1 | 40.65 ± 4.2 | 37.00–47.00 |
| RDW-CV (%) | 13.81 ± 1.8 | 12.43 ± 1.1 | 11.5–15.00 |
| PLT (×103/μL) | 239.82 ± 30.5 | 255.25 ± 44.3 | 130.00–350.00 |
| PCT (%) | 0.19 ± 0.06 | 0.26 ± 0.04 | 0.1–0.4 |
| MPV (fL) | 9.44 ± 1.2 | 10.11 ± 0.9 | 7.00–12.00 |
| PDW (fL) | 8.24 ± 1.7 | 12.30 ± 2.9 | 6.00–16.00 |
| P-LCR (%) | 17.35 ± 7.3 | 25.23 ± 8.0 | 6.00–40.00 |
| PT (sec.) | 12.81 ± 0.9 | 12.39 ± 0.6 | 11.50–15.00 |
| INR (sec.) | 0.83 ± 0.05 | 0.95 ± 0.04 | 0.8–1.2 |
| APTT (sec.) | 27.34 ± 2.53 | 28.79 ± 3.2 | 24.00–35.00 |
| APTT Ratio | 0.99 ± 0.18 | 0.96 ± 0.1 | 0.8–1.2 |
| Sodium (mmol/L) | 139.72 ± 3.1 | 137.82 ± 2.4 | 136.0–145.0 |
| Potassium (mmol/L) | 3.9 ± 0.33 | 4.60 ± 0.4 | 3.5–5.1 |
| NO Mean (±SD) | MDA Mean (±SD) | NT Mean (±SD) | ADMA Mean (±SD) | ||
|---|---|---|---|---|---|
| Control | 55.19 (±12.24) | 356.21 (±122.11) | 482.42 (±218.6) | 166.93 (±59.15) | |
| T0 | Single fracture | 90.14 * (±21.52) | 222.58 * (±85.41) | 407.28 (±101) | 286.43 * (±142.6) |
| Double fracture | 78.71 * (±22.39) | 208.82 * (±44.41) | 540.27 (±182.22) | 259.67 * (±74.22) | |
| T1 | Single fracture | 96.58 * (±30.61) | 233.35 * (±77.8) | 486.91 (±156.85) | 255.19 * (±73.15) |
| Double fracture | 79.97 * (±20.07) | 162.9 * (±45.48) | 582.65 (±207.31) | 262.11 * (±106.49) | |
| T2 | Single fracture | 102.17 * (±19.21) | 295.51 (±32.76) | 421.85 (±247.32) | 124.36 (±58.95) |
| Double fracture | 76.65 (±27.96) | 207.7 * (±76.72) | 629.2 (±236.82) | 164.24 (±81.96) | |
| T3 | Single fracture | 88.59 * (±6.15) | 191.73 * (±34.45) | 416.33 (±170,43) | 129.04 (±36.87) |
| Double fracture | 86.41 * (±5.52) | 184.11 * (±25.05) | 787.51 (±189.25) | 83.16 (±21.36) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wozniak, L.; Ratajczak-Wrona, W.; Borys, J.; Antonowicz, B.; Nowak, K.; Bortnik, P.; Jablonska, E. Levels of Biological Markers of Nitric Oxide in Serum of Patients with Mandible Fractures. J. Clin. Med. 2021, 10, 2832. https://doi.org/10.3390/jcm10132832
Wozniak L, Ratajczak-Wrona W, Borys J, Antonowicz B, Nowak K, Bortnik P, Jablonska E. Levels of Biological Markers of Nitric Oxide in Serum of Patients with Mandible Fractures. Journal of Clinical Medicine. 2021; 10(13):2832. https://doi.org/10.3390/jcm10132832
Chicago/Turabian StyleWozniak, Lukasz, Wioletta Ratajczak-Wrona, Jan Borys, Bozena Antonowicz, Karolina Nowak, Piotr Bortnik, and Ewa Jablonska. 2021. "Levels of Biological Markers of Nitric Oxide in Serum of Patients with Mandible Fractures" Journal of Clinical Medicine 10, no. 13: 2832. https://doi.org/10.3390/jcm10132832
APA StyleWozniak, L., Ratajczak-Wrona, W., Borys, J., Antonowicz, B., Nowak, K., Bortnik, P., & Jablonska, E. (2021). Levels of Biological Markers of Nitric Oxide in Serum of Patients with Mandible Fractures. Journal of Clinical Medicine, 10(13), 2832. https://doi.org/10.3390/jcm10132832