
OnabotulinumtoxinA in Migraine: A Review of the Literature and Factors Associated with Efficacy


Abstract
:1. Introduction
2. A Brief History of Botulinum Toxin
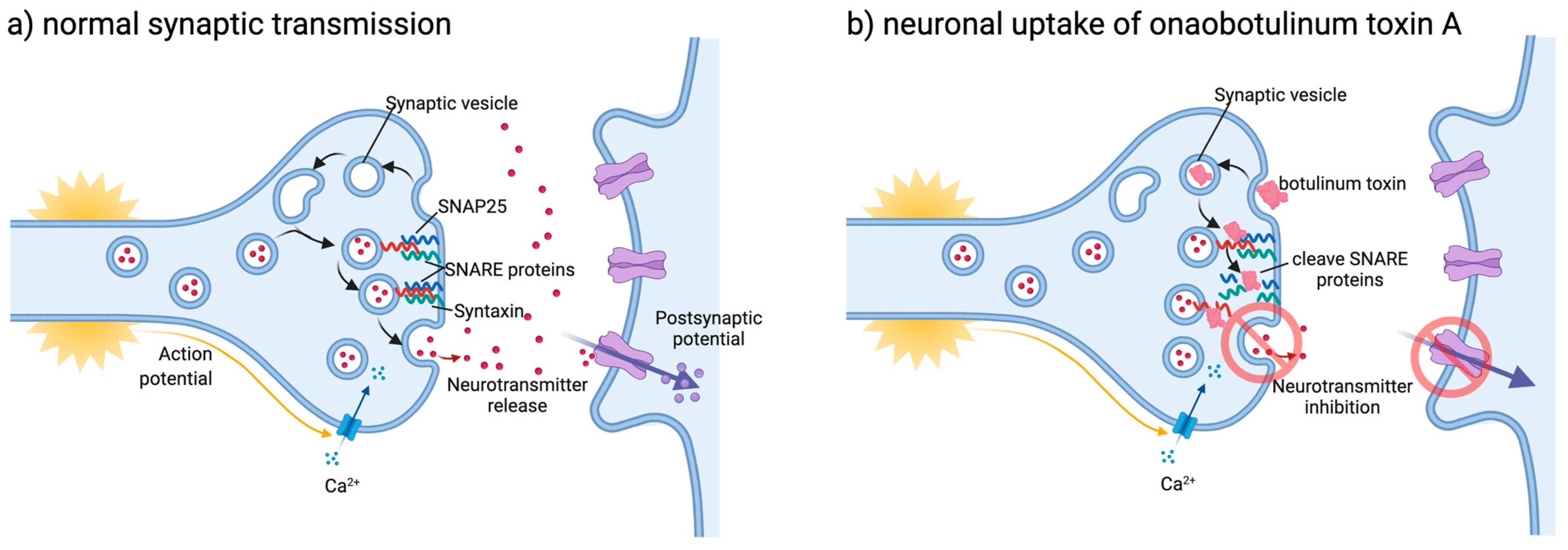
3. Mechanism of Action
4. Efficacy of OnabotulinumtoxinA
4.1. Quality of Life Measures
4.2. Efficacy Compared to Other Treatments
4.3. Efficacy in Hemiplegic Migraine
4.4. Efficacy in Medication Overuse Headache
5. Factors Associated with Efficacy of Botulinum Toxin
5.1. Clinical Factors
5.2. Biomarkers
5.3. Imaging Features
5.4. Genetic Markers
6. Clinical Considerations
6.1. Assessment of Efficacy When Commencing Botulinum Toxin
6.2. Wearing Off Effect of Botulinum Toxin
6.3. Stopping Botulinum Toxin
7. Emerging Concepts
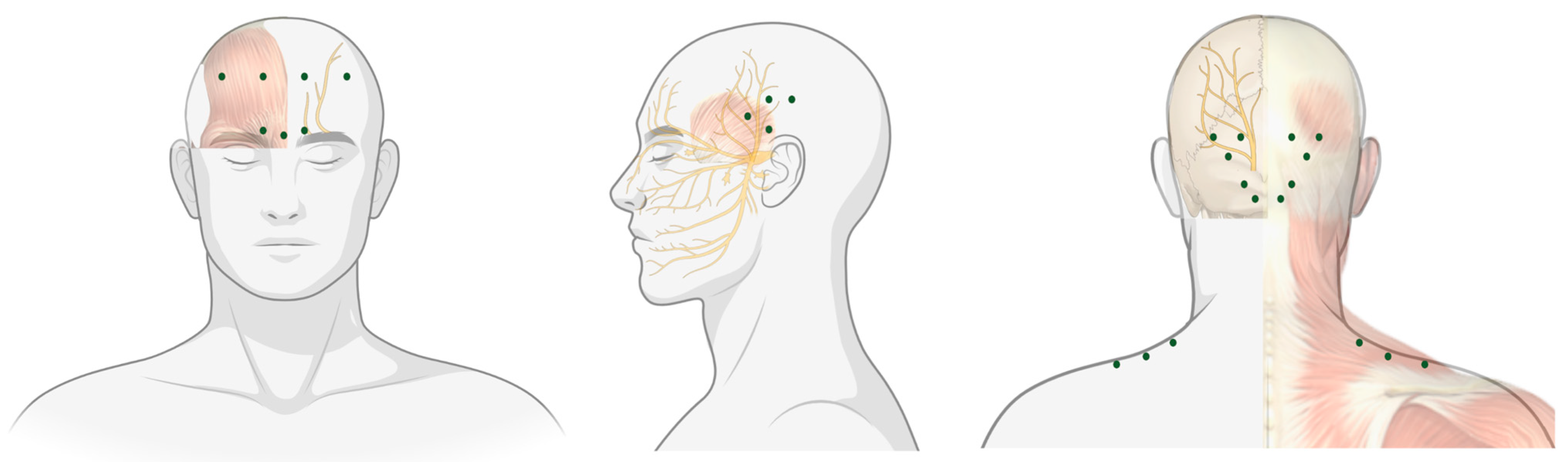
7.1. Location of Injections
7.2. Current Studies
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2018, 17, 954–976. [Google Scholar] [CrossRef] [Green Version]
- The International Classification of Headache Disorders 3rd edition. Available online: https://ichd-3.org/ (accessed on 12 August 2019).
- Buse, D.C.; Greisman, J.D.; Baigi, K.; Lipton, R.B. Migraine progression: A Systematic Review. Headache 2019, 59, 306–338. [Google Scholar] [CrossRef]
- Horowitz, B.Z. Botulinum toxin. Crit. Care Clin. 2005, 21, 825–839, viii. [Google Scholar] [CrossRef]
- Whitcup, S.M. The History of Botulinum Toxins in Medicine: A Thousand Year Journey. Handb. Exp. Pharmacol. 2021, 263, 3–10. [Google Scholar]
- Erbguth, F.J.; Naumann, M. Historical aspects of botulinum toxin: Justinus Kerner (1786-1862) and the “sausage poison”. Neurology 1999, 53, 1850–1853. [Google Scholar] [CrossRef]
- Van Ermengem, E. Classics in infectious diseases. A new anaerobic bacillus and its relation to botulism. E. van Ermengem. Originally published as "Ueber einen neuen anaëroben Bacillus und seine Beziehungen zum Botulismus" in Zeitschrift für Hygiene und Infektionskrankheiten 26: 1-56, 1897. Rev. Infect. Dis. 1979, 1, 701–719. [Google Scholar]
- Scott, A.B. Botulinum toxin injection into extraocular muscles as an alternative to strabismus surgery. Ophthalmology. 1980, 87, 1044–1049. [Google Scholar] [CrossRef]
- Binder, W.J.; Blitzer, A.; Brin, M.F. Treatment of hyperfunctional lines of the face with botulinum toxin A. Dermatol. Surg. 1998, 24, 1198–1205. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F. OnabotulinumtoxinA for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 2010, 50, 921–936. [Google Scholar]
- Whitcup, S.M.; Turkel, C.C.; DeGryse, R.E.; Brin, M.F. Development of onabotulinumtoxinA for chronic migraine. Ann. N. Y. Acad. Sci. 2014, 1329, 67–80. [Google Scholar] [CrossRef]
- Available online: https://app.biorender.com/biorender-templates (accessed on 31 May 2021).
- Frampton, J.E.; Silberstein, S. OnabotulinumtoxinA: A Review in the Prevention of Chronic Migraine. Drugs 2018, 78, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum Neurotoxins: Biology, Pharmacology, and Toxicology. Pharmacol. Rev. 2017, 69, 200–235. [Google Scholar] [CrossRef]
- Herd, C.P.; Tomlinson, C.L.; Rick, C.; Scotton, W.J.; Edwards, J.; Ives, N.; Clarke, C.E.; Sinclair, A. Botulinum toxins for the prevention of migraine in adults. Cochrane Database Syst. Rev. 2018, 6, Cd011616. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Gaul, C.; García-Moncó, J.C.; Sommer, K.; Martelletti, P. An open-label prospective study of the real-life use of onabotulinumtoxinA for the treatment of chronic migraine: The REPOSE study. J. Headache Pain. 2019, 20, 26. [Google Scholar] [CrossRef] [Green Version]
- Bruloy, E.; Sinna, R.; Grolleau, M.D.J.; Bout-Roumazeilles, A.; Berard, E.; Chaput, B. Botulinum Toxin versus Placebo: A Meta-Analysis of Prophylactic Treatment for Migraine. Plast. Reconstr. Surg. 2019, 143, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Shen, B.; Wang, L. Impact of the botulinum-A toxin on prevention of adult migraine disorders. J. Integr Neurosci. 2020, 19, 201–208. [Google Scholar]
- Blumenfeld, A.M.; Tepper, S.J.; Robbins, L.D.; Manack Adams, A.; Buse, D.C.; Orejudos, A.; DSilberstein, S. Effects of onabotulinumtoxinA treatment for chronic migraine on common comorbidities including depression and anxiety. J. Neurol. Neurosurg. Psychiatry 2019, 90, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demiryurek, B.E.; Ertem, D.H.; Tekin, A.; Ceylan, M.; Aras, Y.G.; Gungen, B.D. Effects of onabotulinumtoxinA treatment on efficacy, depression, anxiety, and disability in Turkish patients with chronic migraine. Neurol. Sci. 2016, 37, 1779–1784. [Google Scholar] [CrossRef]
- Maasumi, K.; Thompson, N.R.; Kriegler, J.S.; Tepper, S.J. Effect of OnabotulinumtoxinA Injection on Depression in Chronic Migraine. Headache 2015, 55, 1218–1224. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Dodick, D.W.; Diener, H.; Degryse, R.E.; Turkel, C.C.; Lipton, R.B.; Silberstein, S.D. OnabotulinumtoxinA for chronic migraine: Efficacy, safety, and tolerability in patients who received all five treatment cycles in the PREEMPT clinical program. Acta. Neurol. Scand. 2014, 129, 61–70. [Google Scholar] [CrossRef]
- Aydinlar, E.I.; Dikmen, P.Y.; Kosak, S.; Kocaman, A.S. OnabotulinumtoxinA effectiveness on chronic migraine, negative emotional states and sleep quality: A single-center prospective cohort study. J. Headache Pain 2017, 18, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kollewe, K.; Escher, C.M.; Wulff, D.U.; Fathi, D.; Paracka, L.; Mohammadi, B.; Karst, M.; Dressler, D. Long-term treatment of chronic migraine with OnabotulinumtoxinA: Efficacy, quality of life and tolerability in a real-life setting. J. Neural Transm (Vienna) 2016, 123, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Mathew, N.T.; Jaffri, S.F. A double-blind comparison of onabotulinumtoxina (BOTOX) and topiramate (TOPAMAX) for the prophylactic treatment of chronic migraine: A pilot study. Headache 2009, 49, 1466–1478. [Google Scholar] [CrossRef] [PubMed]
- Cady, R.K.; Schreiber, C.P.; Porter, J.A.; Blumenfeld, A.M.; Farmer, K.U. A multi-center double-blind pilot comparison of onabotulinumtoxinA and topiramate for the prophylactic treatment of chronic migraine. Headache 2011, 51, 21–32. [Google Scholar] [CrossRef]
- Blumenfeld, A.M.; Schim, J.D.; Chippendale, T.J. Botulinum toxin type A and divalproex sodium for prophylactic treatment of episodic or chronic migraine. Headache 2008, 48, 210–220. [Google Scholar] [CrossRef]
- Tepper, S.J.; Fang, J.; Zhou, L.; Shen, Y.; Vo, P.; Abdrabboh, A.; Glassberg, M.B.; Ferraris, M. Effectiveness of erenumab and onabotulinumtoxinA on acute medication usage and health care resource utilization as migraine prevention in the United States. J. Manag. Care Spec. Pharm. 2021. [Google Scholar] [CrossRef]
- Sacco, S.; Russo, A.; Geppetti, P.; Grazzi, L.; Negro, A.; Tassorelli, C.; Tedeschi, G.; Martelletti, P. What is changing in chronic migraine treatment? An algorithm for onabotulinumtoxinA treatment by the Italian chronic migraine group. Expert Rev. of Neurother. 2020, 20, 1275–1286. [Google Scholar] [CrossRef]
- Pellesi, L.; Do, T.P.; Ashina, H.; Ashina, M.; Burstein, R. Dual Therapy with Anti-CGRP Monoclonal Antibodies and Botulinum Toxin for Migraine Prevention: Is There a Rationale? Headache 2020, 60, 1056–1065. [Google Scholar] [CrossRef]
- She, T.; Chen, Y.; Tang, T.; Chen, M.; Zheng, H. Calcitonin gene-related peptide antagonists versus botulinum toxin A for the preventive treatment of chronic migraine protocol of a systematic review and network meta-analysis: A protocol for systematic review. Medicine (Baltimore) 2020, 99, e18929. [Google Scholar] [CrossRef]
- Eren, O.E.; Gaul, C.; Peikert, A.; Gendolla, A.; Ruscheweyh, R.; Straube, A. Triptan efficacy does not predict onabotulinumtoxinA efficacy but improves with onabotulinumtoxinA response in chronic migraine patients. Sci. Rep. 2020, 10, 11382. [Google Scholar] [CrossRef] [PubMed]
- Domínguez Vivero, C.; Leira, Y.; Saavedra Piñeiro, M.; Rodríguez-Osorio, X.; Ramos-Cabrer, P.; Villalba Martín, C.; Sobrino, T.; Campos, F.; Castillo, J.; Leira, R. Iron Deposits in Periaqueductal Gray Matter Are Associated with Poor Response to OnabotulinumtoxinA in Chronic Migraine. Toxins 2020, 12, 479. [Google Scholar] [CrossRef]
- Moreno-Mayordomo, R.; Ruiz, M.; Pascual, J.; Gallego de la Sacristana, M.; Vidriales, I.; Sobrado, M.; Cernuda-Morollon, E.; Gago-Veiga, A.B.; Garcia-Azorin, D.; Telleria, J.J.; et al. CALCA and TRPV1 genes polymorphisms are related to a good outcome in female chronic migraine patients treated with OnabotulinumtoxinA. J. Headache Pain 2019, 20, 39. [Google Scholar] [CrossRef] [PubMed]
- Schiano di Cola, F.; Caratozzolo, S.; Liberini, P.; Rao, R.; Padovani, A. Response Predictors in Chronic Migraine: Medication Overuse and Depressive Symptoms Negatively Impact Onabotulinumtoxin-A Treatment. Front. Neurol. 2019, 10, 678. [Google Scholar] [CrossRef] [PubMed]
- De Tommaso, M.; Brighina, F.; Delussi, M. Effects of Botulinum Toxin A on Allodynia in Chronic Migraine: An Observational Open-Label Two-Year Study. Eur. Neurol. 2019, 81, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Young, W.B.; Ivan Lopez, J.; Rothrock, J.F.; Orejudos, A.; Manack Adams, A.; Lipton, R.B.; Blumenfeld, A.M. Effects of onabotulinumtoxinA treatment in patients with and without allodynia: Results of the COMPEL study. J. Headache Pain 2019, 20, 10. [Google Scholar] [CrossRef]
- Domínguez, C.; Vieites-Prado, A.; Pérez-Mato, M.; Sobrino, T.; Rodríguez-Osorio, X.; López, A.; Campos, F.; Martínez, F.; Castillo, J.; Leira, R. CGRP and PTX3 as Predictors of Efficacy of Onabotulinumtoxin Type A in Chronic Migraine: An Observational Study. Headache 2018, 58, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Domínguez, C.; Pozo-Rosich, P.; Torres-Ferrús, M.; Hernández-Beltrán, N.; Jurado-Cobo, C.; González-Oria, C.; Santos, S.; Monzón, M.J.; Latorre, G.; Álvaro, L.C.; et al. OnabotulinumtoxinA in chronic migraine: Predictors of response. A prospective multicentre descriptive study. Eur. J. Neurol. 2018, 25, 411–416. [Google Scholar] [CrossRef]
- Lovati, C.; Giani, L.; Mariotti, D.A.C.; Tabaee Damavandi, P.; Mariani, C.; Pantoni, L. May migraine attack response to triptans be a predictor of the efficacy of Onabotulinum toxin-A prophylaxis? Neurol. Sci. 2018, 39, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, C.S.; Becerra, L.; Smith, J.H.; DeLange, J.M.; Smith, R.M.; Black, D.F.; Welker, K.M.; Burstein, R.; Cutrer, F.M.; Borsook, D. Brain Changes in Responders vs. Non-Responders in Chronic Migraine: Markers of Disease Reversal. Front. Hum. Neurosci. 2016, 10, 497. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.J.; Lee, C.; Choi, H.; Chung, C.S. Factors associated with favorable outcome in botulinum toxin A treatment for chronic migraine: A clinic-based prospective study. J. Neurol. Sci. 2016, 363, 51–54. [Google Scholar] [CrossRef]
- Cernuda-Morollón, E.; Ramón, C.; Martínez-Camblor, P.; Serrano-Pertierra, E.; Larrosa, D.; Pascual, J. OnabotulinumtoxinA decreases interictal CGRP plasma levels in patients with chronic migraine. Pain 2015, 156, 820–824. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.H.; Chen, S.P.; Fuh, J.L.; Wang, Y.F.; Wang, S.J. Efficacy, safety, and predictors of response to botulinum toxin type A in refractory chronic migraine: A retrospective study. J. Chin. Med. Assoc. 2014, 77, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagola, I.; Esteve-Belloch, P.; Palma, J.A.; Luquin, M.R.; Riverol, M.; Martinez-Vila, E.; Irimia, P. [Predictive factors of the response to treatment with onabotulinumtoxinA in refractory migraine]. Rev. Neurol. 2014, 58, 241–246. [Google Scholar] [PubMed]
- Bumb, A.; Seifert, B.; Wetzel, S.; Agosti, R. Patients profiling for Botox® (onabotulinum toxin A) treatment for migraine: A look at white matter lesions in the MRI as a potential marker. Springerplus 2013, 2, 377. [Google Scholar] [CrossRef] [Green Version]
- Grogan, P.M.; Alvarez, M.V.; Jones, L. Headache direction and aura predict migraine responsiveness to rimabotulinumtoxin B. Headache 2013, 53, 126–136. [Google Scholar] [CrossRef]
- Kim, C.C.; Bogart, M.M.; Wee, S.A.; Burstein, R.; Arndt, K.A.; Dover, J.S. Predicting migraine responsiveness to botulinum toxin type A injections. Arch. Dermatol. 2010, 146, 159–163. [Google Scholar] [CrossRef]
- Burstein, R.; Dodick, D.; Silberstein, S. Migraine prophylaxis with botulinum toxin A is associated with perception of headache. Toxicon 2009, 54, 624–627. [Google Scholar] [CrossRef] [Green Version]
- Mathew, N.T.; Kailasam, J.; Meadors, L. Predictors of response to botulinum toxin type A (BoNTA) in chronic daily headache. Headache 2008, 48, 194–200. [Google Scholar] [CrossRef]
- Jakubowski, M.; McAllister, P.J.; Bajwa, Z.H.; Ward, T.N.; Smith, P.; Burstein, R. Exploding vs. imploding headache in migraine prophylaxis with Botulinum Toxin A. Pain 2006, 125, 286–295. [Google Scholar] [CrossRef]
- Eross, E.J.; Gladstone, J.P.; Lewis, S.; Rogers, R.; Dodick, D.W. Duration of migraine is a predictor for response to botulinum toxin type A. Headache 2005, 45, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.Y.; Garza, I.; Dodick, D.W.; Robertson, C.E. The Effect of OnabotulinumtoxinA on Aura Frequency and Severity in Patients with Hemiplegic Migraine: Case Series of 11 Patients. Headache 2018, 58, 973–985. [Google Scholar] [CrossRef]
- De Goffau, M.J.; Klaver, A.R.E.; Willemsen, M.G.; Bindels, P.J.E.; Verhagen, A.P. The Effectiveness of Treatments for Patients with Medication Overuse Headache: A Systematic Review and Meta-Analysis. J. Pain 2017, 18, 615–627. [Google Scholar] [CrossRef] [Green Version]
- Chiang, C.C.; Schwedt, T.J.; Wang, S.J.; Dodick, D.W. Treatment of medication-overuse headache: A systematic review. Cephalalgia 2016, 36, 371–386. [Google Scholar] [CrossRef]
- Pijpers, J.A.; Kies, D.A.; Louter, M.A.; van Zwet, E.W.; Ferrari, M.D.; Terwindt, G.M. Acute withdrawal and botulinum toxin A in chronic migraine with medication overuse: A double-blind randomized controlled trial. Brain 2019, 142, 1203–1214. [Google Scholar] [CrossRef] [Green Version]
- Butera, C.; Colombo, B.; Bianchi, F.; Cursi, M.; Messina, R.; Amadio, S.; Guerriero, R.; Comi, G.; Del Carro, U. Refractory chronic migraine: Is drug withdrawal necessary before starting a therapy with onabotulinum toxin type A? Neurol. Sci. 2016, 37, 1701–1706. [Google Scholar] [CrossRef]
- Andreou, A.P.; Trimboli, M.; Al-Kaisy, A.; Murphy, M.; Palmisani, S.; Fenech, C.; Smith, T.; Lambru, G. Prospective real-world analysis of OnabotulinumtoxinA in chronic migraine post-National Institute for Health and Care Excellence UK technology appraisal. Eur. J. Neurol. 2018, 25, 1069-e83. [Google Scholar] [CrossRef] [PubMed]
- Bendtsen, L.; Sacco, S.; Ashina, M.; Mitsikostas, D.; Ahmed, F.; Pozo-Rosich, P.; Martelletti, P. Guideline on the use of onabotulinumtoxinA in chronic migraine: A consensus statement from the European Headache Federation. J. Headache Pain 2018, 19, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbanti, P.; Egeo, G. Predictors of response to onabotulinumtoxin A in chronic migraine. Eur. J. Neurol. 2018, 25, e40. [Google Scholar] [CrossRef]
- Barbanti, P.; Aurilia, C.; Dall'Armi, V.; Egeo, G.; Fofi, L.; Bonassi, S. The phenotype of migraine with unilateral cranial autonomic symptoms documents increased peripheral and central trigeminal sensitization. A case series of 757 patients. Cephalalgia 2016, 36, 1334–1340. [Google Scholar] [CrossRef] [PubMed]
- Valfrè, W.; Rainero, I.; Bergui, M.; Pinessi, L. Voxel-based morphometry reveals gray matter abnormalities in migraine. Headache 2008, 48, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Maleki, N.; Becerra, L.; Brawn, J.; Bigal, M.; Burstein, R.; Borsook, D. Concurrent functional and structural cortical alterations in migraine. Cephalalgia 2012, 32, 607–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domínguez, C.; López, A.; Ramos-Cabrer, P.; Vieites-Prado, A.; Pérez-Mato, M.; Villalba, C.; Sobrino, T.; Rodriguez-Osorio, X.; Campos, F.; Castillo, J.; et al. Iron deposition in periaqueductal gray matter as a potential biomarker for chronic migraine. Neurology 2019, 92, e1076–e1085. [Google Scholar] [CrossRef] [PubMed]
- Tassorelli, C.; Aguggia, M.; De Tommaso, M.; Geppetti, P.; Grazzi, L.; Pini, L.A.; Sarchielli, P.; Tedeschi, G.; Martelletti, P.; Cortelli, P. Onabotulinumtoxin A for the management of chronic migraine in current clinical practice: Results of a survey of sixty-three Italian headache centers. J. Headache Pain 2017, 18, 66. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Diener, H.C.; DeGryse, R.E.; Lipton, R.B.; Turkel, C.C. Per cent of patients with chronic migraine who responded per onabotulinumtoxinA treatment cycle: PREEMPT. J. Neurol. Neurosurg. Psychiatry 2015, 86, 996–1001. [Google Scholar] [CrossRef]
- Sarchielli, P.; Romoli, M.; Corbelli, I.; Bernetti, L.; Verzina, A.; Brahimi, E.; Eusebi, P.; Caproni, S.; Calabresi, P. Stopping Onabotulinum Treatment after the First Two Cycles Might Not Be Justified: Results of a Real-life Monocentric Prospective Study in Chronic Migraine. Front. Neurol. 2017, 8, 655. [Google Scholar] [CrossRef]
- Vernieri, F.; Paolucci, M.; Altamura, C.; Pasqualetti, P.; Mastrangelo, V.; Pierangeli, G.; Cevoli, S.; D'Amico, D.; Grazzi, L. Onabotulinumtoxin-A in Chronic Migraine: Should Timing and Definition of Non-Responder Status Be Revised? Suggestions from a Real-Life Italian Multicenter Experience. Headache 2019, 59, 1300–1309. [Google Scholar] [CrossRef]
- Ornello, R.; Guerzoni, S.; Baraldi, C.; Evangelista, L.; Frattale, I.; Marini, C.; Tiseo, C.; Pistoia, F.; Sacco, S. Sustained response to onabotulinumtoxin A in patients with chronic migraine: Real-life data. J. Headache Pain 2020, 21, 40. [Google Scholar] [CrossRef] [Green Version]
- Zidan, A.; Roe, C.; Burke, D.; Mejico, L. OnabotulinumtoxinA wear-off in chronic migraine, observational cohort study. J. Clin. Neurosci. 2019, 69, 237–240. [Google Scholar] [CrossRef]
- Masters-Israilov, A.; Robbins, M.S. OnabotulinumtoxinA Wear-off Phenomenon in the Treatment of Chronic Migraine. Headache 2019, 59, 1753–1761. [Google Scholar] [CrossRef]
- Quintas, S.; García-Azorín, D.; Heredia, P.; Talavera, B.; Gago-Veiga, A.B.; Guerrero, A.L. Wearing Off Response to OnabotulinumtoxinA in Chronic Migraine: Analysis in a Series of 193 Patients. Pain Med. 2019, 20, 1815–1821. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.A.; Mohammed, A.E.; Poongkunran, M.; Chimakurthy, A.; Pepper, M. Wearing Off Effect of OnabotulinumtoxinA Near the End of Treatment Cycle for Chronic Migraine: A 4-Year Clinical Experience. Headache 2020, 60, 430–440. [Google Scholar] [CrossRef] [PubMed]
- Evidente, V.G.H.; Pappert, E.J. Botulinum toxin therapy for cervical dystonia: The science of dosing. Tremor Other Hyperkinet Mov (N. Y.) 2014, 4, 273. [Google Scholar] [CrossRef]
- Cruz, F.; Herschorn, S.; Aliotta, P.; Brin, M.; Thompson, C.; Lam, W.; Daniell, G.; Heesakkers, J.; Haag-Molkenteller, C. Efficacy and Safety of OnabotulinumtoxinA in Patients with Urinary Incontinence Due to Neurogenic Detrusor Overactivity: A Randomised, Double-Blind, Placebo-Controlled Trial. Eur. Urol. 2011, 60, 742–750. [Google Scholar] [CrossRef]
- Ching, J.; Tinsley, A.; Rothrock, J. Prognosis Following Discontinuation of OnabotulinumA Therapy in "Super-responding" Chronic Migraine Patients. Headache 2019, 59, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, A.M.; Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Brin, M.F.; Binder, W.J. Insights into the Functional Anatomy Behind the PREEMPT Injection Paradigm: Guidance on Achieving Optimal Outcomes. Headache 2017, 57, 766–777. [Google Scholar] [CrossRef] [Green Version]
- Bratbak, D.F.; Nordgård, S.; Stovner, L.J.; Linde, M.; Dodick, D.W.; Aschehoug, I.; Folvik, M.; Tronvik, E. Pilot study of sphenopalatine injection of onabotulinumtoxinA for the treatment of intractable chronic migraine. Cephalalgia 2017, 37, 356–364. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.G.; Bae, J.H.; Kim, H.; Wang, S.J.; Kim, S.T. A Proposal for Botulinum Toxin Type A Injection into the Temporal Region in Chronic Migraine Headache. Toxins 2020, 12, 214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kara, M.; Gürçay, E.; Aydın, G.; Kaymak, B.; Sekizkardeş, M.; Akıncı, A.; Uludüz, D.; Özçakar, L. Botulinum toxin injections to cranial sutures for chronic migraine Rewinding the technique using ultrasound imaging. Toxicon 2019, 172, 19–22. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Population | Diagnosis | MOH | Therapy | Follow-Up (Months) | Definition of Response | Percentage Responders | Significant Predictors | Non-Significant Predictors |
|---|---|---|---|---|---|---|---|---|---|
| Eren, 2020 [32] | Germany, n = 49 | 100% CM | U | 155 units OnaB-A PREEMPT | 3 | ≥30% fewer MHD | 38.8% | None | Triptan efficacy |
| Domínguez Vivero, 2020 [33] | Spain, n = 62 | 100% CM | U | 155 units OnaB-A PREEMPT | 3 | ≥50% fewer headaches | 75.8% | Age, CGRP (>50 ng/mL), PTX3 (>1000 pg/mL), iron deposition in GP and PAG | Gender, BMI, smoking, phenotype (intensity, aura, duration), allodynia, presence or location of WML |
| Moreno-Mayordomo, 2019 [34] | Spain, n = 156 | 100% CM | U | 155 units OnaB-A PREEMPT | 6 | ≥50% fewer MMD | 76.9% | Polymorphisms CALCA rs3781719 TRPV1 rs222749, | 23 other SNPs |
| Schiano di Cola, 2019 [35] | Italy, n = 84 | 100% CM | 65.5% | 155–195 units OnaB-A PREEMPT | 12 | ≥50% fewer headaches | 73.9% | Depressive symptoms, MOH | N/A |
| de Tommaso, 2019 [36] | Italy, n = 120 | 100% CM | U | 155–195 units OnaB-A PREEMPT | 24 | ≥50% fewer headaches | 61.6% | Less severe allodynia | N/A |
| Young, 2019 [37] | USA, Aus, Korea, n = 715 | 100% CM | U | 155 units OnaB-A PREEMPT | 27 | Mean reduction MHD | N/A | absence allodynia (only at 27 months) | N/A |
| Domínguez, 2018 [38] | Spain, n = 62 | 100% CM | U | 155 units OnaB-A PREEMPT | 6 | ≥50% fewer headaches | 75.8% | CGRP, PTX3 | TNF-⍺, IL-10, IL-6, hs-CRP, cFn, S100, NSE |
| Domínguez, 2018 [39] | Spain, n = 725 | 100% CM | 58.2% | 155 units OnaB-A PREEMPT | 12 | ≥50% fewer headaches | 79.3% | CM duration, Unilateral pain, combined symptomatic treatment, fewer days of disability, milder headache | Gender, MA, depression, fibromyalgia, |
| Lovati, 2018 [40] | Italy, n = 44 | 100% CM | U | 170–195 units OnaB-A PREEMPT | 12 | ≥50% fewer MMD | 31.8% | Triptan response | N/A |
| Hubbard, 2016 [41] | USA, n = 23 | 100% CM | U | 150 units modif. OnaB-A PREEMPT | 6 | ≥50% fewer MHD and now EM | 47.8% | Cortical thickness at right SI and aINS, left ParsOp and STG | N/A |
| Lee, 2016 [42] | Korea, n = 70 | 100% CM | 50% R, 47% NR | 155 units OnaB-A PREEMPT | 1.5 | ≥50% fewer MHD, ≥50%fewer abortive Rx OR ≥50% fewer mod-severe headache | 60% | Disease duration MCA/ICA ratio | Age, gender, BMI, concurrent prophylactic medication, MA vs. MoA, psychiatric comorbidity, smoking |
| Cernuda-Morollón, 2015 [43] | Spain, n = 83 | 100% CM | 31.3% | 155–195 units OnaB-A PREEMPT | 6 | ≥50% fewer headaches AND ≥50% reduced VAS | 77.1% | CGRP (76.85 pg/mL vs. 50.45 pg/mL), VIP | Clinical features (MA), age, duration of CM, comorbidity, obesity, prophylactic medication |
| Lin, 2014 [44] | Taiwan, n = 94 | 100% CM | 19.1% | 75–155 units OnaB-A | 3 | ≥30% fewer headaches | 39.4% | Phenotype (ocular) | Phenotype (imploding vs. exploding), gender, MA, BMI, depression, dosage of OnaB-A |
| Pagola, 2014 [45] | Spain, n = 39 | ‘refractory migraine’ | 50% R, 81% NR | U | U | ≥50% fewer MHD | 46.2% | Nil | Unilateral location, implosive pain, pericranial muscle tension, duration of migraine, MOH |
| Bumb, 2013 [46] | Switzerland, n = 111 | U | U | 100 units OnaB-A | U | ≥3 cycles of OnaB-A | 42.3% | None | WML |
| Grogan, 2013 [47] | USA, n = 128 | U, EM + CM | U | RimB-B | U | ≥75% fewer headaches | 79% | MA, phenotype (imploding, ocular) | Gender, dosage, |
| Kim, 2010 [48] | USA, n = 18 | 88.9% EM 11.1% CM | U | 16–78 units OnaB-A | 3 | ≥50% fewer headaches | 72.2% | Phenotype (imploding pain) | N/A |
| Burstein, 2009 [49] | USA, n = 82 | 32.9% EM 67.1% CM | U | U | U | ≥66.7% fewer MMD | 45.1% | Phenotype of pain (imploding or ocular) | EM vs. CM |
| Mathew, 2008 [50] | USA, n = 71 | 100% CM | U | 100 units OnaB-A | 7 | ≥50% fewer headache AND ≥50% reduced MIDAS | 76.1% | Unilateral headache, curaneous alloydrnia, pericranial muscle tenderness | N/A |
| Jakubowski, 2006 [51] | USA, n = 63 | 57.1% EM 42.9% CM | U | 100 units OnaB-A | 6 | ≥80% fewer MMD | 61.9% | Phenotype of pain (imploding or ocular) | Neck muscles tenderness, EM vs. CM |
| Eross, 2005 [52] | USA, n = 74 | 23% EM 77% CM | 23% | 25–100 units OnaB-A | 3 | ≥50% reduced disability | 62% | Age, shorter duration of illness | EM vs. CM, MOH, dosage, muscle tenderness, |
| Brief Study Synopsis | Year Posted | Current Status | Trial Identifier |
|---|---|---|---|
| PraB-A for treatment of chronic migraine | 2021 | Recruiting | NCT04845178 |
| OnaB-A for the treatment of post-stroke and vascular headache | 2020 | Not yet recruiting | NCT04580238 |
| 155 units vs. 100 units of OnaB-A for treatment of chronic migraine | 2020 | Recruiting | NCT04349176 |
| OnaB-A blockade of the SPG for refractory chronic migraine | 2019 | Recruiting | NCT04069897 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ray, J.C.; Hutton, E.J.; Matharu, M. OnabotulinumtoxinA in Migraine: A Review of the Literature and Factors Associated with Efficacy. J. Clin. Med. 2021, 10, 2898. https://doi.org/10.3390/jcm10132898
Ray JC, Hutton EJ, Matharu M. OnabotulinumtoxinA in Migraine: A Review of the Literature and Factors Associated with Efficacy. Journal of Clinical Medicine. 2021; 10(13):2898. https://doi.org/10.3390/jcm10132898
Chicago/Turabian StyleRay, Jason C., Elspeth J. Hutton, and Manjit Matharu. 2021. "OnabotulinumtoxinA in Migraine: A Review of the Literature and Factors Associated with Efficacy" Journal of Clinical Medicine 10, no. 13: 2898. https://doi.org/10.3390/jcm10132898
APA StyleRay, J. C., Hutton, E. J., & Matharu, M. (2021). OnabotulinumtoxinA in Migraine: A Review of the Literature and Factors Associated with Efficacy. Journal of Clinical Medicine, 10(13), 2898. https://doi.org/10.3390/jcm10132898