
Vasopressor-Sparing Strategies in Patients with Shock: A Scoping-Review and an Evidence-Based Strategy Proposition

 ,
,
Abstract
:1. Introduction
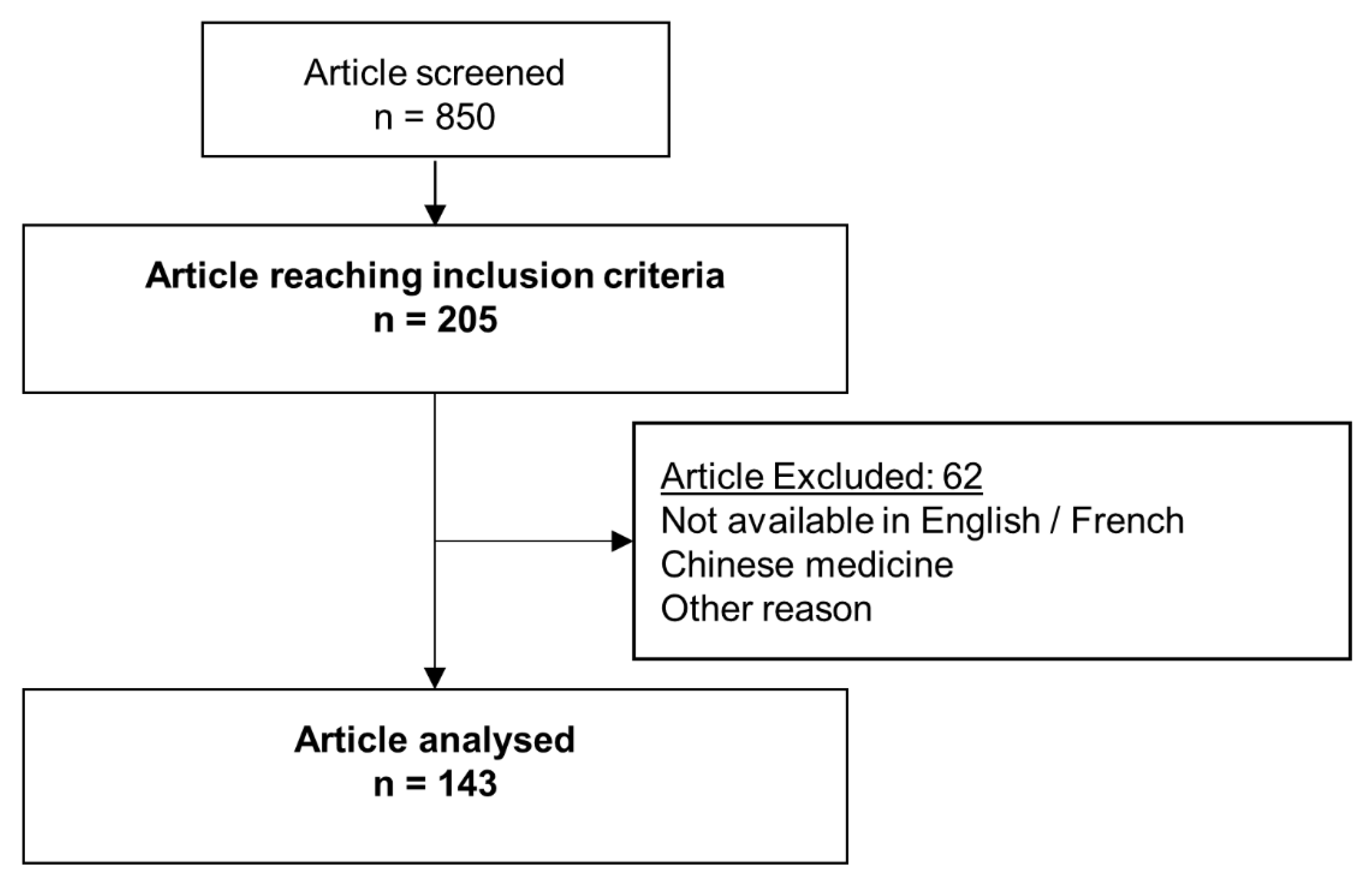
2. Materials and Methods
2.1. Population
2.2. Criteria
2.3. Algorithm and Study Selection
3. Results
3.1. Pharmacological Interventions
3.1.1. Vasopressor
3.1.2. Adjuvant
3.2. Fluid Therapy
3.3. Body Temperature
3.4. Kidney Replacement Therapy
4. Discussion
4.1. Pharmacological Strategies
4.2. Hemodynamic Strategies
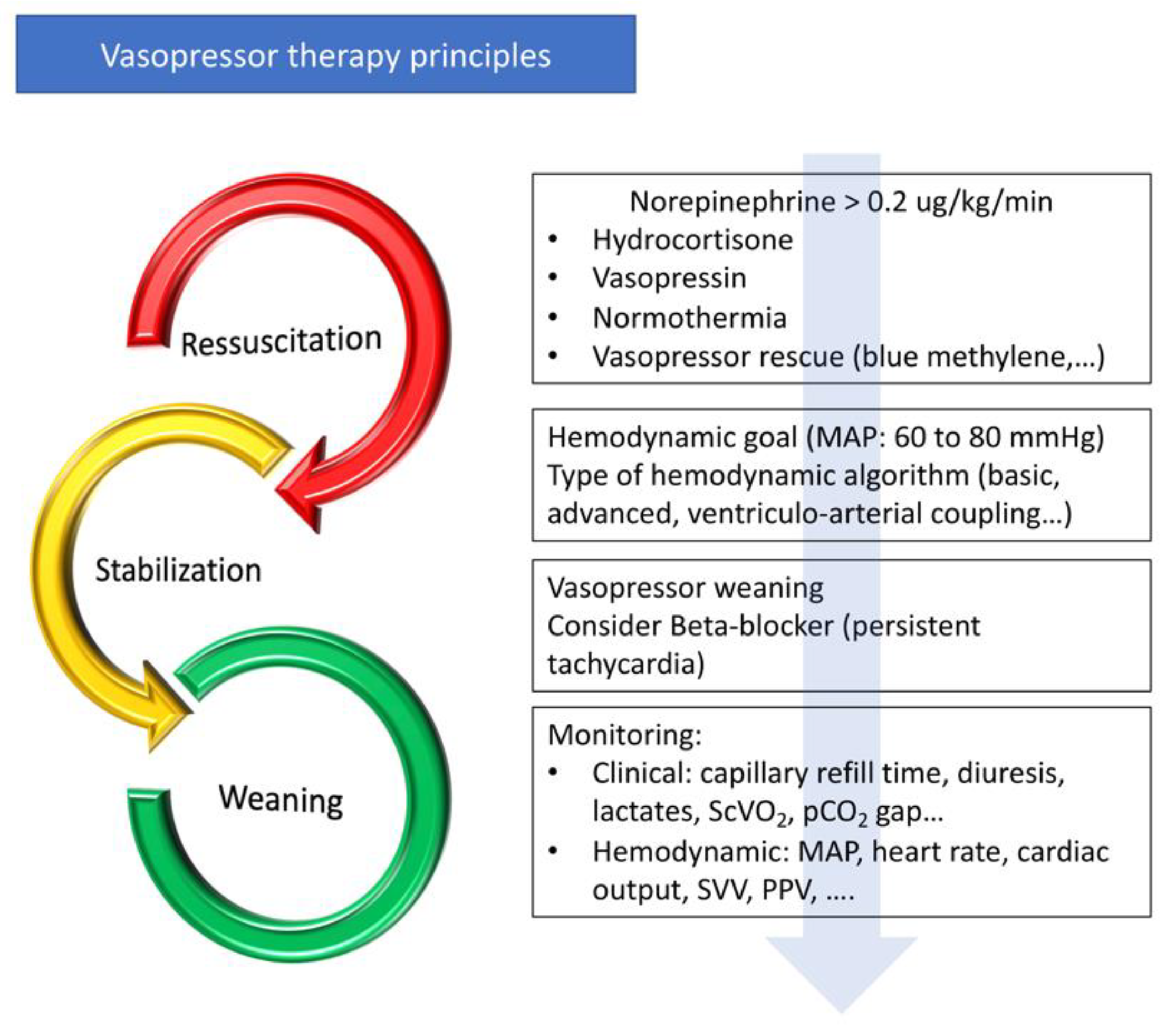
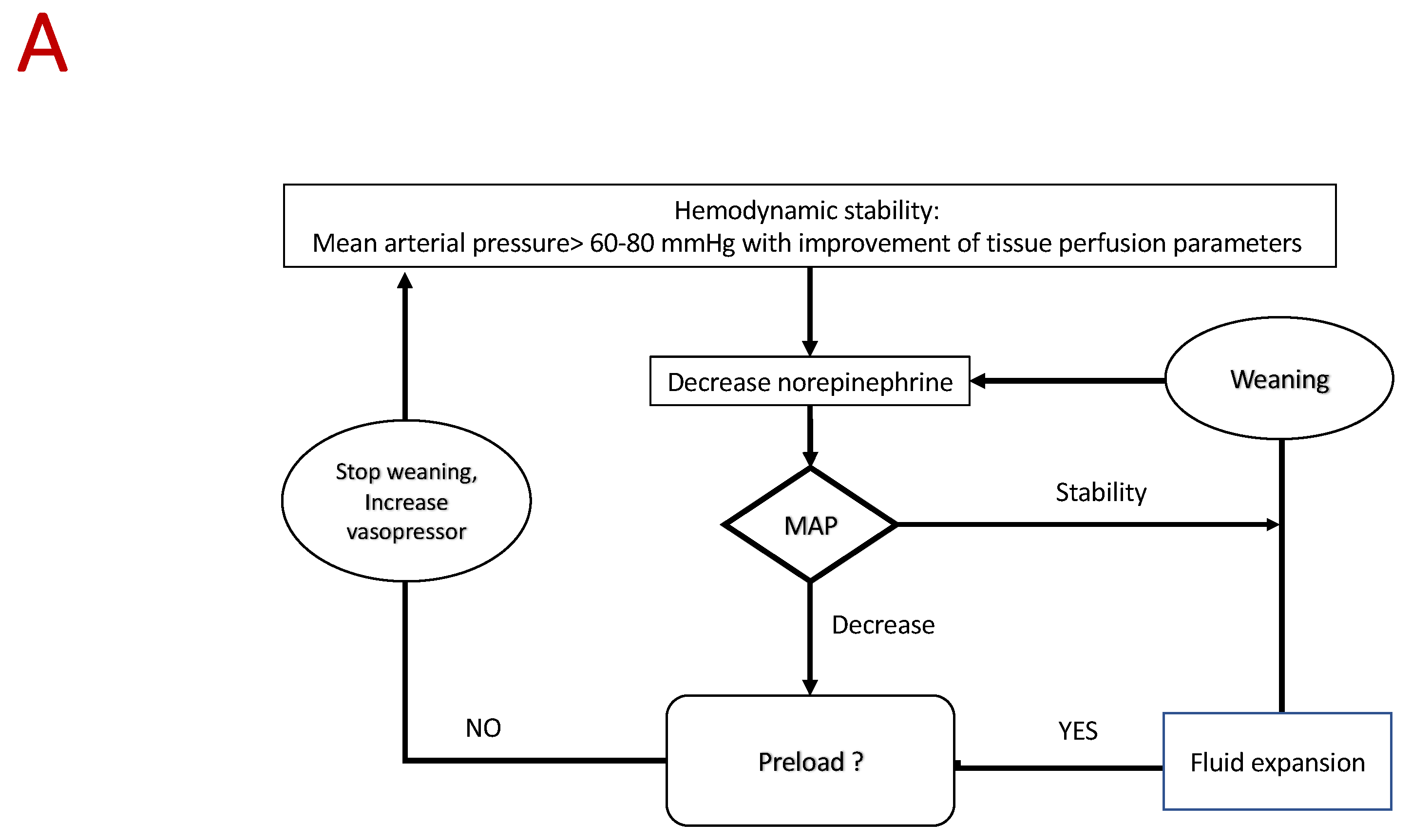
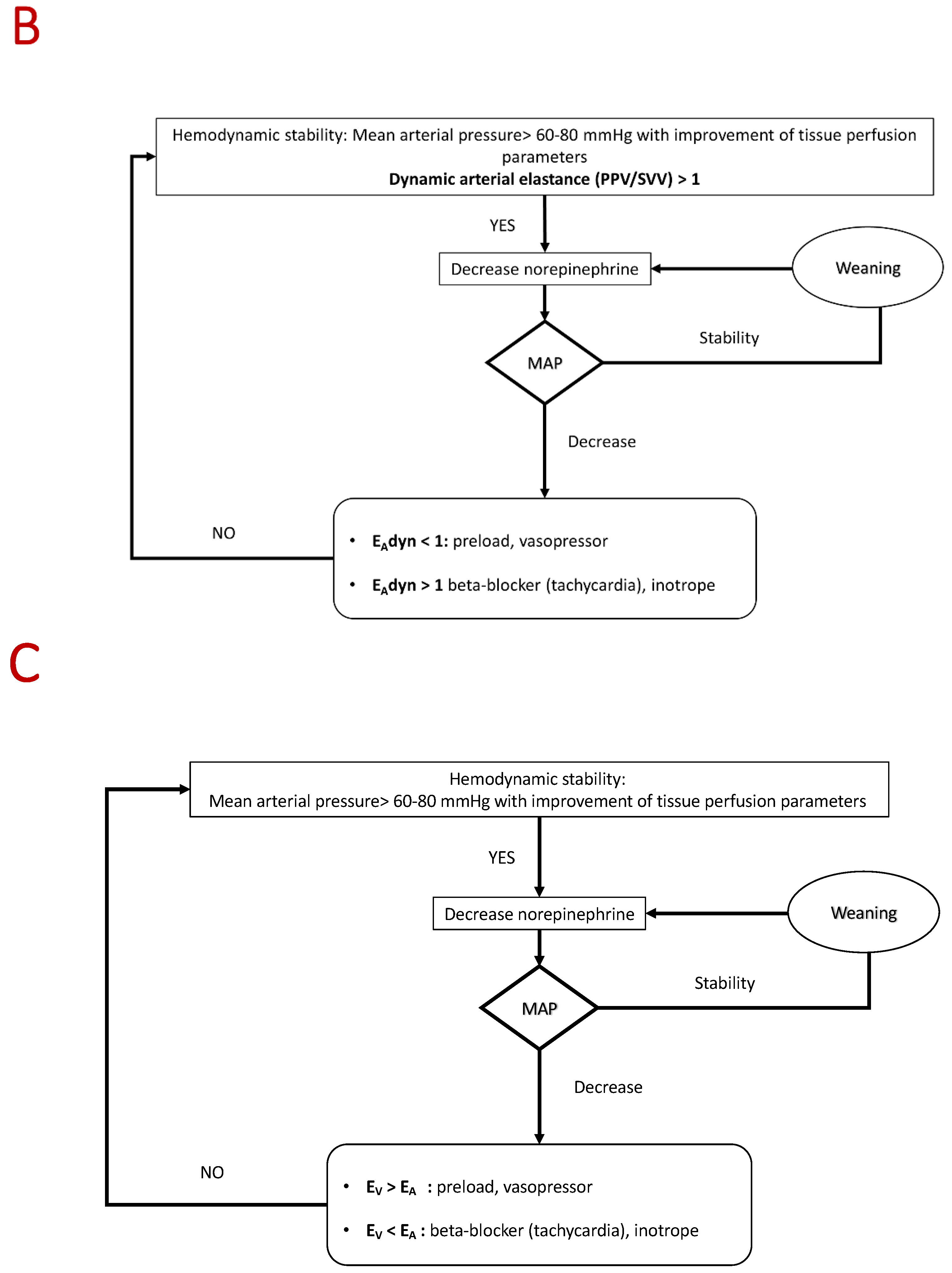
4.3. Proposed Algorithm
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Landry, D.W.; Oliver, J.A. The Pathogenesis of Vasodilatory Shock. N. Engl. J. Med. 2001, 345, 588–595. [Google Scholar] [CrossRef]
- Sakr, Y.; Reinhart, K.; Vincent, J.-L.; Sprung, C.L.; Moreno, R.; Ranieri, V.M.; De Backer, D.; Payen, D. Does dopamine administration in shock influence outcome? Results of the Sepsis Occurrence in Acutely Ill Patients (SOAP) Study*. Crit. Care Med. 2006, 34, 589–597. [Google Scholar] [CrossRef] [Green Version]
- De Backer, D.; Biston, P.; Devriendt, J.; Madl, C.; Chochrad, D.; Aldecoa, C.; Brasseur, A.; Defrance, P.; Gottignies, P.; Vincent, J.-L. Comparison of Dopamine and Norepinephrine in the Treatment of Shock. N. Engl. J. Med. 2010, 362, 779–789. [Google Scholar] [CrossRef] [Green Version]
- Russell, J.A.; Walley, K.R.; Singer, J.; Gordon, A.C.; Hébert, P.C.; Cooper, D.J.; Holmes, C.L.; Mehta, S.; Granton, J.T.; Storms, M.M.; et al. Vasopressin versus Norepinephrine Infusion in Patients with Septic Shock. N. Engl. J. Med. 2008, 358, 877–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Lamontagne, F.; Day, A.G.; Meade, M.O.; Cook, D.J.; Guyatt, G.H.; Hylands, M.; Radermacher, P.; Chrétien, J.M.; Beaudoin, N.; Hébert, P.; et al. Pooled analysis of higher versus lower blood pressure targets for vasopressor therapy septic and vasodilatory shock. Intensive Care Med. 2018, 44, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Guinot, P.-G.; Abou-Arab, O.; Guilbart, M.; Bar, S.; Zogheib, E.; Daher, M.; Besserve, P.; Nader, J.; Caus, T.; Kamel, S.; et al. Monitoring dynamic arterial elastance as a means of decreasing the duration of norepinephrine treatment in vasoplegic syndrome following cardiac surgery: A prospective, randomized trial. Intensive Care Med. 2017, 43, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Hollenberg, S.M. Concise Clinical Review Vasoactive Drugs in Circulatory Shock. Am. J. Respir. Crit. Care Med. 2011, 183, 847–855. [Google Scholar] [CrossRef]
- Bangash, M.N.; Kong, M.L.; Pearse, R.M. Use of inotropes and vasopressor agents in critically ill patients. Br. J. Pharmacol. 2012, 165, 2015–2033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, J.A. Vasopressor therapy in critically ill patients with shock. Intensive Care Med. 2019, 45, 1503–1517. [Google Scholar] [CrossRef]
- Russell, J.A.; Gordon, A.C.; Williams, M.D.; Boyd, J.H.; Walley, K.R.; Kissoon, N. Vasopressor Therapy in the Intensive Care Unit. Semin. Respir. Crit. Care Med. 2021, 42, 59–77. [Google Scholar] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merouani, M.; Guignard, B.; Vincent, F.; Borron, S.W.; Karoubi, P.; Fosse, J.-P.; Cohen, Y.; Clec’h, C.; Vicaut, E.; Marbeuf-Gueye, C.; et al. Norepinephrine weaning in septic shock patients by closed loop control based on fuzzy logic. Crit. Care 2008, 12, R155. [Google Scholar] [CrossRef] [Green Version]
- Jeon, K.; Song, J.-U.; Chung, C.R.; Yang, J.H.; Suh, G.Y. Incidence of hypotension according to the discontinuation order of vasopressors in the management of septic shock: A prospective randomized trial (DOVSS). Crit. Care 2018, 22, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahloul, M.; Chaari, A.; Mbarek, M.N.B.; Kallel, H.; Bouaziz, M. Use of Heptaminol Hydrochloride for Catecholamine Weaning in Septic Shock. Am. J. Ther. 2012, 19, e8–e17. [Google Scholar] [CrossRef] [PubMed]
- Asfar, P.; Meziani, F.; Hamel, J.-F.; Grelon, F.; Megarbane, B.; Anguel, N.; Mira, J.-P.; Dequin, P.-F.; Gergaud, S.; Weiss, N.; et al. High versus Low Blood-Pressure Target in Patients with Septic Shock. N. Engl. J. Med. 2014, 17, 1583–1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamontagne, F.; Meade, M.O.; Hébert, P.C.; Asfar, P.; Lauzier, F.; Seely, A.J.E.; Day, A.G.; Mehta, S.; Muscedere, J.; Bagshaw, S.M.; et al. Higher versus lower blood pressure targets for vasopressor therapy in shock: A multicentre pilot randomized controlled trial. Intensive Care Med. 2016, 42, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Morelli, A.; Ertmer, C.; Rehberg, S.; Lange, M.; Orecchioni, A.; Cecchini, V.; Bachetoni, A.; D’Alessandro, M.; Van Aken, H.; Pietropaoli, P.; et al. Continuous terlipressin versus vasopressin infusion in septic shock (TERLIVAP): A randomized, controlled pilot study. Crit. Care 2009, 13, R130. [Google Scholar] [CrossRef] [Green Version]
- Choudhury, A.; Kedarisetty, C.K.; Vashishtha, C.; Saini, D.; Kumar, S.; Maiwall, R.; Sharma, M.K.; Bhadoria, A.S.; Kumar, G.; Joshi, Y.K.; et al. A randomized trial comparing terlipressin and noradrenaline in patients with cirrhosis and septic shock. Liver Int. 2017, 37, 552–561. [Google Scholar] [CrossRef]
- Morelli, A.; Donati, A.; Ertmer, C.; Rehberg, S.; Kampmeier, T.; Orecchioni, A.; Di Russo, A.; D’Egidio, A.; Landoni, G.; Lombrano, M.R.; et al. Effects of vasopressinergic receptor agonists on sublingual microcirculation in norepinephrine-dependent septic shock. Crit. Care 2011, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Svoboda, P.; Scheer, P.; Kantorová, I.; Doubek, J.; Dudra, J.; Radvan, M.; Radvanova, J. Terlipressin in the treatment of late phase catecholamine-resistant septic shock. Hepatogastroenterology 2012, 59, 1043–1047. [Google Scholar]
- Liu, Z.M.; Chen, J.; Kou, Q.; Lin, Q.; Huang, X.; Tang, Z.; Kang, Y.; Li, K.; Zhou, L.; Song, Q.; et al. Terlipressin versus norepinephrine as infusion in patients with septic shock: A multicentre, randomised, double-blinded trial. Intensive Care Med. 2018, 44, 1816–1825. [Google Scholar] [CrossRef] [PubMed]
- Morelli, A.; Ertmer, C.; Lange, M.; Dü Nser, M.; Rehberg, S.; Van Aken, H.; Pietropaoli, P.; Westphal, M. Effects of short-term simultaneous infusion of dobutamine and terlipressin in patients with septic shock: The DOBUPRESS study †. Br. J. Anaesth. 2008, 100, 494–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dünser, M.W.; Mayr, A.J.; Ulmer, H.; Knotzer, H.; Sumann, G.; Pajk, W.; Friesenecker, B.; Hasibeder, W.R. Arginine vasopressin in advanced vasodilatory shock: A prospective, randomized, controlled study. Circulation 2003, 107, 2313–2319. [Google Scholar] [CrossRef] [Green Version]
- Luckner, G.; Dünser, M.W.; Stadlbauer, K.H.; Mayr, V.D.; Jochberger, S.; Wenzel, V.; Ulmer, H.; Pajk, W.; Hasibeder, W.R.; Friesenecker, B.; et al. Cutaneous vascular reactivity and flow motion response to vasopressin in advanced vasodilatory shock and severe postoperative multiple organ dysfunction syndrome. Crit. Care 2006, 10, R40. [Google Scholar] [CrossRef] [Green Version]
- Lauzier, F.; Lévy, B.; Lamarre, P.; Lesur, O. Vasopressin or norepinephrine in early hyperdynamic septic shock: A randomized clinical trial. Intensive Care Med. 2006, 32, 1782–1789. [Google Scholar] [CrossRef] [PubMed]
- Mojtahedzadeh, M.; Barzegar, E.; Ahmadi, A.; Mousavi, S.; Nouri, M.; Mojtahedzadeh, M. The Therapeutic Role of Vasopressin on Improving lactate Clearance During and After Vasogenic Shock: Microcirculation, Is It The Black Box? Acta Med. Iran. 2016, 54, 15–23. Available online: https://acta.tums.ac.ir/index.php/acta/article/view/5384 (accessed on 17 July 2020).
- Argenziano, M.; Choudhri, A.; Oz, M.C.; Rose, E.A.; Smith, C.R.; Landry, D.W. A prospective randomized trial of arginine vasopressin in the treatment of vasodilatory shock after left ventricular assist device placement. Circulation 1997, 96, II-286. Available online: https://europepmc.org/article/med/9386112 (accessed on 17 July 2020).
- Patel, B.M.; Chittock, D.R.; Russell, J.A.; Walley, K.R. Beneficial effects of short-term vasopressin infusion during severe septic shock. Anesthesiology 2002, 96, 576–582. [Google Scholar] [CrossRef]
- Hajjar, L.A.; Vincent, J.L.; Barbosa Gomes Galas, F.R.; Rhodes, A.; Landoni, G.; Osawa, E.A.; Melo, R.R.; Sundin, M.R.; Grande, S.M.; Gaiotto, F.A.; et al. Vasopressin versus Norepinephrine in Patients with Vasoplegic Shock after Cardiac Surgery. Anesthesiology 2017, 126, 85–93. [Google Scholar] [CrossRef]
- Gordon, A.C.; Mason, A.J.; Thirunavukkarasu, N.; Perkins, G.D.; Cecconi, M.; Cepkova, M.; Pogson, D.G.; Aya, H.D.; Anjum, A.; Frazier, G.J.; et al. Effect of Early Vasopressin vs Norepinephrine on Kidney Failure in Patients With Septic Shock. JAMA 2016, 316, 509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanna, A.; English, S.W.; Wang, X.S.; Ham, K.; Tumlin, J.; Szerlip, H.; Busse, L.W.; Altaweel, L.; Albertson, T.E.; Mackey, C.; et al. Angiotensin II for the Treatment of Vasodilatory Shock. N. Engl. J. Med. 2017, 377, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Chawla, L.S.; Busse, L.; Brasha-Mitchell, E.; Davison, D.; Honiq, J.; Alotaibi, Z.; Seneff, M.G. Intravenous angiotensin II for the treatment of high-output shock (ATHOS trial): A pilot study. Crit. Care 2014, 18, 534. [Google Scholar] [CrossRef] [Green Version]
- Lv, Q.Q.; Gu, X.H.; Chen, Q.H.; Yu, J.Q.; Zheng, R.Q. Early initiation of low-dose hydrocortisone treatment for septic shock in adults: A randomized clinical trial. Am. J. Emerg. Med. 2017, 35, 1810–1814. [Google Scholar] [CrossRef]
- Hyvernat, H.; Barel, R.; Gentilhomme, A.; Césari-Giordani, J.F.; Freche, A.; Kaidomar, M.; Goubaux, B.; Pradier, C.; Dellamonica, J.; Bernardin, G. Effects of increasing hydrocortisone to 300mgper day in the treatment of septic shock: A pilot study. Shock 2016, 46, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Bollaert, P.E.; Charpentier, C.; Levy, B.; Debouverie, M.; Audibert, G.; Larcan, A. Reversal of late septic shock with supraphysiologic doses of hydrocortisone. Crit. Care Med. 1998, 26, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Cicarelli, D.D.; Vieira, J.E.; Benseñor, F.E.M. Early dexamethasone treatment for septic shock patients: A prospective randomized clinical trial. Sao Paulo Med. J. 2007, 125, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Sprung, C.L.; Annane, D.; Keh, D.; Moreno, R.; Singer, M.; Freivogel, K.; Weiss, Y.G.; Benbenishty, J.; Kalenka, A.; Forst, H.; et al. Hydrocortisone Therapy for Patients with Septic Shock. N. Engl. J. Med. 2008, 358, 111–124. [Google Scholar] [CrossRef] [Green Version]
- Annane, D.; Renault, A.; Brun-Buisson, C.; Megarbane, B.; Quenot, J.-P.; Siami, S.; Cariou, A.; Forceville, X.; Schwebel, C.; Martin, C.; et al. Hydrocortisone plus Fludrocortisone for Adults with Septic Shock. N. Engl. J. Med. 2018, 378, 809–818. [Google Scholar] [CrossRef]
- Venkatesh, B.; Finfer, S.; Cohen, J.; Rajbhandari, D.; Arabi, Y.; Bellomo, R.; Billot, L.; Correa, M.; Glass, P.; Harward, M.; et al. Adjunctive Glucocorticoid Therapy in Patients with Septic Shock. N. Engl. J. Med. 2018, 378, 797–808. [Google Scholar] [CrossRef]
- Annane, D.; Sébille, V.; Charpentier, C.; Bollaert, P.-E.; François, B.; Korach, J.-M.; Capellier, G.; Cohen, Y.; Azoulay, E.; Troché, G.; et al. Effect of Treatment With Low Doses of Hydrocortisone and Fludrocortisone on Mortality in Patients With Septic Shock. JAMA 2002, 288, 862. [Google Scholar] [CrossRef] [Green Version]
- Gordon, A.C.; Mason, A.J.; Perkins, G.D.; Stotz, M.; Terblanche, M.; Ashby, D.; Brett, S.J. The Interaction of Vasopressin and Corticosteroids in Septic Shock. Crit. Care Med. 2014, 42, 1325–1333. [Google Scholar] [CrossRef]
- Iglesias, J.; Vassallo, A.V.; Patel, V.V.; Sullivan, J.B.; Cavanaugh, J.; Elbaga, Y. Outcomes of Metabolic Resuscitation Using Ascorbic Acid, Thiamine, and Glucocorticoids in the Early Treatment of Sepsis: The ORANGES Trial. Chest 2020, 158, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Moskowitz, A.; Huang, D.T.; Hou, P.C.; Gong, J.; Doshi, P.B.; Grossestreuer, A.V.; Andersen, L.W.; Ngo, L.; Sherwin, R.L.; Berg, K.M.; et al. Effect of Ascorbic Acid, Corticosteroids, and Thiamine on Organ Injury in Septic Shock: The ACTS Randomized Clinical Trial. JAMA 2020, 324, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Donnino, M.W.; Andersen, L.W.; Berg, K.M.; Chase, M.; Sherwin, R.; Smithline, H.; Carney, E.; Ngo, L.; Patel, P.V.; Liu, X.; et al. Corticosteroid therapy in refractory shock following cardiac arrest: A randomized, double-blind, placebo-controlled, trial. Crit. Care 2016, 20, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oppert, M.; Reinicke, A.; Gräf, K.J.; Barckow, D.; Frei, U.; Eckardt, K.U. Plasma cortisol levels before and during “low-dose” hydrocortisone therapy and their relationship to hemodynamic improvement in patients with septic shock. Intensive Care Med. 2000, 26, 1747–1755. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Aljumah, A.; Dabbagh, O.; Tamim, H.M.; Rishu, A.H.; Al-Abdulkareem, A.; Al Knawy, B.; Hajeer, A.H.; Tamimi, W.; Cherfan, A. Low-dose hydrocortisone in patients with cirrhosis and septic shock: A randomized controlled trial. CMAJ 2010, 182, 1971–1977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaufmann, I.; Briegel, J.; Schliephake, F.; Hoelzl, A.; Chouker, A.; Hummel, T.; Schelling, G.; Thiel, M. Stress doses of hydrocortisone in septic shock: Beneficial effects on opsonization-dependent neutrophil functions. Intensive Care Med. 2008, 34, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Ngaosuwan, K.; Ounchokdee, K.; Chalermchai, T. Clinical Outcomes of Minimized Hydrocortisone Dosage of 100 Mg/Day on Lower Occurrence of Hyperglycemia in Septic Shock Patients. Shock 2018, 50, 280–285. [Google Scholar] [CrossRef]
- Oppert, M.; Schindler, R.; Husung, C.; Offermann, K.; Gräf, K.-J.; Boenisch, O.; Barckow, D.; Frei, U.; Eckardt, K.-U. Low-dose hydrocortisone improves shock reversal and reduces cytokine levels in early hyperdynamic septic shock*. Crit. Care Med. 2005, 33, 2457–2464. [Google Scholar] [CrossRef]
- Mussack, T.; Briegel, J.; Schelling, G.; Jochum, M. Hemofiltrastion does not influence early S-100B serum levels in septic shock patients receiving stress doses of hydrocortisone or placebo. Eur. J. Med. Res. 2005, 10, 11–17. [Google Scholar]
- Briegel, J.; Forst, H.; Haller, M.; Schelling, G.; Kilger, E.; Kuprat, G.; Hemmer, B.; Hummel, T.; Lenhart, A.; Heyduck, M.; et al. Stress doses of hydrocortisone reverse hyperdynamic septic shock: A prospective, randomized, double-blind, single-center study. Crit. Care Med. 1999, 27, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Rivers, E.; Nguyen, B.; Havstad, S.; Ressler, J.; Muzzin, A.; Knoblich, B.; Peterson, E.; Tomlanovich, M. Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. N. Engl. J. Med. 2001, 345, 1368–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.-M.; Huang, C.-D.; Lin, H.-C.; Liu, C.-Y.; Wang, C.-H.; Kuo, H.-P. A modified goal-directed protocol improves clinical outcomes in intensive care unit patients with septic shock. Shock 2006, 26, 551–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, N.F.; Zheng, R.Q.; Lin, H.; Shao, J.; Yu, J.Q.; Yang, D.G. Improved sepsis bundles in the treatment of septic shock: A prospective clinical study. Am. J. Emerg. Med. 2015, 33, 1045–1049. [Google Scholar] [CrossRef]
- Chen, C.; Kollef, M.H. Targeted fluid minimization following initial resuscitation in septic shock a pilot study. Chest 2015, 148, 1462–1469. [Google Scholar] [CrossRef]
- Gomersall, C.D.; Joynt, G.M.; Freebairn, R.C.; Hung, V.; Buckley, T.A.; Oh, T.E. Resuscitation of critically ill patients based on the results of gastric tonometry: A prospective, randomized, controlled trial. Crit. Care Med. 2000, 28, 607–614. [Google Scholar] [CrossRef]
- Jones, A.E.; Shapiro, N.I.; Trzeciak, S.; Arnold, R.C.; Claremont, H.A.; Kline, J.A. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: A randomized clinical trial. JAMA J. Am. Med. Assoc. 2010, 303, 739–746. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Zheng, R.; Lin, H.; Chen, Q.; Shao, J.; Wang, D. Global end-diastolic volume index vs CVP goal-directed fluid resuscitation for COPD patients with septic shock: A randomized controlled trial. Am. J. Emerg. Med. 2017, 35, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Mouncey, P.R.; Osborn, T.M.; Power, G.S.; Harrison, D.A.; Sadique, M.Z.; Grieve, R.D.; Jahan, R.; Harvey, S.E.; Bell, D.; Bion, J.F.; et al. Trial of Early, Goal-Directed Resuscitation for Septic Shock. N. Engl. J. Med. 2015, 372, 1301–1311. [Google Scholar] [CrossRef] [Green Version]
- Corl, K.A.; Prodromou, M.; Merchant, R.C.; Gareen, I.; Marks, S.; Banerjee, D.; Amass, T.; Abbasi, A.; Delcompare, C.; Palmisciano, A.; et al. The Restrictive IV Fluid Trial in Severe Sepsis and Septic Shock (RIFTS). Crit. Care Med. 2019, 47, 951–959. [Google Scholar] [CrossRef]
- Yealy, D.M.; Kellum, J.A.; Huang, D.T.; Barnato, A.E.; Weissfeld, L.A.; Pike, F.; Terndrup, T.; Wang, H.E.; Hou, P.C.; LoVecchio, F.; et al. A Randomized Trial of Protocol-Based Care for Early Septic Shock. N. Engl. J. Med. 2014, 370, 1683–1693. [Google Scholar]
- Peake, S.L.; Delaney, A.; Bailey, M.; Bellomo, R.; Cameron, P.A.; Cooper, D.J.; Higgins, A.M.; Holdgate, A.; Howe, B.D.; Webb, S.A.R.; et al. Goal-Directed Resuscitation for Patients with Early Septic Shock. N. Engl. J. Med. 2014, 371, 1496–1506. [Google Scholar]
- Richard, J.C.; Bayle, F.; Bourdin, G.; Leray, V.; Debord, S.; Delannoy, B.; Stoian, A.C.; Wallet, F.; Yonis, H.; Guerin, C. Preload dependence indices to titrate volume expansion during septic shock: A randomized controlled trial. Crit. Care 2015, 19, 5. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Ni, H.; Qian, Z. Effectiveness of treatment based on PiCCO parameters in critically ill patients with septic shock and/or acute respiratory distress syndrome: A randomized controlled trial. Intensive Care Med. 2015, 41, 444–451. [Google Scholar] [CrossRef]
- Tokarik, M.; Sjöberg, F.; Balik, M.; Pafcuga, I.; Broz, L. Fluid therapy lidco controlled trial - Optimization of volume resuscitation of extensively burned patients through noninvasive continuous real-time hemodynamic monitoring LiDCO. J. Burn. Care Res. 2013, 34, 537–542. [Google Scholar] [CrossRef]
- Annane, D.; Siami, S.; Jaber, S.; Martin, C.; Elatrous, S.; Descorps Declère, A.; Charles Preiser, J.; Outin, H.; Troché, G.; Charpentier, C.; et al. Effects of Fluid Resuscitation With Colloids vs Crystalloids on Mortality in Critically Ill Patients Presenting With Hypovolemic Shock The CRISTAL Randomized Trial. JAMA 2013, 310, 1809–1817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caironi, P.; Tognoni, G.; Masson, S.; Fumagalli, R.; Pesenti, A.; Romero, M.; Fanizza, C.; Caspani, L.; Faenza, S.; Grasselli, G.; et al. Albumin Replacement in Patients with Severe Sepsis or Septic Shock. N. Engl. J. Med. 2014, 370, 1412–1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morelli, A.; Ertmer, C.; Westphal, M.; Rehberg, S.; Kampmeier, T.; Ligges, S.; Orecchioni, A.; D’Egidio, A.; D’Ippoliti, F.; Raffone, C.; et al. Effect of heart rate control with esmolol on hemodynamic and clinical outcomes in patients with septic shock: A randomized clinical trial. JAMA J. Am. Med. Assoc. 2013, 310, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Kirov, M.Y.; Evgenov, O.V.; Evgenov, N.V.; Egorina, E.M.; Sovershaev, M.A.; Sveinbjørnsson, B.; Nedashkovsky, E.V.; Bjertnaes, L.J. Infusion of methylene blue in human septic shock: A pilot, randomized, controlled study. Crit. Care Med. 2001, 29, 1860–1867. [Google Scholar] [CrossRef] [PubMed]
- Levin, R.L.; Degrange, M.A.; Bruno, G.F.; Del Mazo, C.D.; Taborda, D.J.; Griotti, J.J.; Boullon, F.J. Methylene blue reduces mortality and morbidity in vasoplegic patients after cardiac surgery. Ann. Thorac. Surg. 2004, 77, 496–499. [Google Scholar] [CrossRef]
- Annane, D.; Cariou, A.; Maxime, V.; Azoulay, E.; D’Honneur, G.; Timsit, J.F.; Cohen, Y.; Wolf, M.; Fartoukh, M.; Adrie, C.; et al. Corticosteroid Treatment and Intensive Insulin Therapy for Septic Shock in Adults. JAMA 2010, 303, 341. [Google Scholar]
- Galley, H.F.; Howdle, P.D.; Walker, B.E.; Webster, N.R. The effects of intravenous antioxidants in patients with septic shock. Free. Radic. Biol. Med. 1997, 23, 768–774. [Google Scholar] [CrossRef]
- Spapen, H.; Zhang, H.; Demanet, C.; Vleminckx, W.; Vincent, J.L.; Huyghens, L. Does N-acetyl-L-cysteine influence cytokine response during early human septic shock? Chest 1998, 113, 1616–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Csontos, C.; Rezman, B.; Foldi, V.; Bogar, L.; Drenkovics, L.; Röth, E.; Weber, G.; Lantos, J. Effect of N-acetylcysteine treatment on oxidative stress and inflammation after severe burn. Burns 2012, 38, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Luethi, N.; Young, P.J.; Frei, D.R.; Eastwood, G.M.; French, C.J.; Deane, A.M.; Shehabi, Y.; Hajjar, L.A.; Oliveira, G.; et al. Effect of Vitamin, C.; Hydrocortisone, and Thiamine vs. Hydrocortisone Alone on Time Alive and Free of Vasopressor Support Among Patients With Septic Shock: The VITAMINS Randomized Clinical Trial. JAMA 2020, 323, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.; Liao, Y.; Guan, J.; Guo, Y.; Zhao, M.; Hu, J.; Zhou, J.; Wang, H.; Cen, Z.; Tang, Y.; et al. Combined Treatment With Hydrocortisone, Vitamin, C.; and Thiamine for Sepsis and Septic Shock: A Randomized Controlled Trial. Chest 2020, 158, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.Y.; Ryoo, S.M.; Park, J.E.; Jo, Y.H.; Jang, D.H.; Suh, G.J.; Kim, T.; Kim, Y.J.; Kim, S.; Cho, H.; et al. Combination therapy of vitamin C and thiamine for septic shock: A multi-centre, double-blinded randomized, controlled study. Intensive Care Med. 2020, 46, 2015–2025. [Google Scholar] [CrossRef]
- Santer, P.; Anstey, M.H.; Patrocínio, M.D.; Wibrow, B.; Teja, B.; Shay, D.; Shaefi, S.; Parsons, C.S.; Houle, T.T.; Eikermann, M.; et al. Effect of midodrine versus placebo on time to vasopressor discontinuation in patients with persistent hypotension in the intensive care unit (MIDAS): An international randomised clinical trial. Intensive Care Med. 2020, 46, 1884–1893. [Google Scholar] [CrossRef] [PubMed]
- Schortgen, F.; Clabault, K.; Katsahian, S.; Devaquet, J.; Mercat, A.; Deye, N.; Dellamonica, J.; Bouadma, L.; Cook, F.; Beji, O.; et al. Fever Control Using External Cooling in Septic Shock A Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2012, 185, 1088–1095. [Google Scholar] [CrossRef]
- Itenov, T.S.; Johansen, M.E.; Bestle, M.; Thormar, K.; Hein, L.; Gyldensted, L.; Lindhardt, A.; Christensen, H.; Estrup, S.; Pedersen, H.P.; et al. Induced hypothermia in patients with septic shock and respiratory failure (CASS): A randomised, controlled, open-label trial. Lancet Respir. Med. 2018, 6, 183–192. [Google Scholar] [CrossRef] [Green Version]
- Fuernau, G.; Beck, J.; Desch, S.; Eitel, I.; Jung, C.; Erbs, S.; Mangner, N.; Lurz, P.; Fengler, K.; Jobs, A.; et al. Mild Hypothermia in Cardiogenic Shock Complicating Myocardial Infarction: Randomized SHOCK-COOL Trial. Circulation 2019, 139, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Boussekey, N.; Chiche, A.; Faure, K.; Devos, P.; Guery, B.; D’Escrivan, T.; Georges, H.; Leroy, O. A pilot randomized study comparing high and low volume hemofiltration on vasopressor use in septic shock. Intensive Care Med. 2008, 34, 1646–1653. [Google Scholar] [CrossRef]
- Chu, L.-P.; Zhou, J.-J.; Yu, Y.-F.; Huang, Y.; Dong, W.-X. Clinical Effects of Pulse High-Volume Hemofiltration on Severe Acute Pancreatitis Complicated With Multiple Organ Dysfunction Syndrome. Ther. Apher. Dial. 2013, 17, 78–83. [Google Scholar] [CrossRef]
- Combes, A.; Bréchot, N.; Amour, J.; Cozic, N.; Lebreton, G.; Guidon, C.; Zogheib, E.; Thiranos, J.C.; Rigal, J.C.; Bastien, O.; et al. Early high-volume hemofiltration versus standard care for post-cardiac surgery shock the HEROICS study. Am. J. Respir. Crit. Care Med. 2015, 192, 1179–1190. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.K.; Coates, E.C.; Smith, D.J.; Karlnoski, R.A.; Hickerson, W.L.; Arnold-Ross, A.L.; Mosier, M.J.; Halerz, M.; Sprague, A.M.; Mullins, R.F.; et al. High-volume hemofiltration in adult burn patients with septic shock and acute kidney injury: A multicenter randomized controlled trial. Crit. Care 2017, 21, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Joannes-Boyau, O.; Honoré, P.M.; Perez, P.; Bagshaw, S.M.; Grand, H.; Canivet, J.L.; Dewitte, A.; Flamens, C.; Pujol, W.; Grandoulier, A.S.; et al. High-volume versus standard-volume haemofiltration for septic shock patients with acute kidney injury (IVOIRE study): A multicentre randomized controlled trial. Intensive Care Med. 2013, 39, 1535–1546. [Google Scholar] [CrossRef]
- Quenot, J.P.; Binquet, C.; Vinsonneau, C.; Barbar, S.D.; Vinault, S.; Deckert, V.; Lemaire, S.; Hassain, A.A.; Bruyère, R.; Souweine, B.; et al. Very high volume hemofiltration with the Cascade system in septic shock patients. Intensive Care Med. 2015, 41, 2111–2120. [Google Scholar] [CrossRef] [PubMed]
- Hawchar, F.; László, I.; Öveges, N.; Trásy, D.; Ondrik, Z.; Molnar, Z. Extracorporeal cytokine adsorption in septic shock: A proof of concept randomized, controlled pilot study. J. Crit. Care 2019, 49, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Wang, S.R.; Su, W.; Liu, J.Y. Removal of humoral mediators and the effect on the survival of septic patients by hemoperfusion with neutral microporous resin column. Ther. Apher. Dial. 2010, 14, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Bagshaw, S.M.; Antonelli, M.; Foster, D.M.; Klein, D.J.; Marshall, J.C.; Palevsky, P.M.; Weisberg, L.S.; Schorr, C.A.; Trzeciak, S.; et al. Effect of Targeted Polymyxin B Hemoperfusion on 28-Day Mortality in Patients With Septic Shock and Elevated Endotoxin Level: The EUPHRATES Randomized Clinical Trial. JAMA 2018, 320, 1455–1463. [Google Scholar] [CrossRef] [Green Version]
- Payen, D.M.; Guilhot, J.; Launey, Y.; Lukaszewicz, A.C.; Kaaki, M.; Veber, B.; Pottecher, J.; Joannes-Boyau, O.; Martin-Lefevre, L.; Jabaudon, M.; et al. Early use of polymyxin B hemoperfusion in patients with septic shock due to peritonitis: A multicenter randomized control trial. Intensive Care Med. 2015, 41, 975–984. [Google Scholar] [CrossRef] [Green Version]
- Vincent, J.L.; Laterre, P.F.; Cohen, J.; Burchardi, H.; Bruining, H.; Lerma, F.A.; Wittebole, X.; De Backer, D.; Brett, S.; Marzo, D.; et al. A pilot-controlled study of a polymyxim B-immobilized hemoperfusion cartridge in patients with severe sepsis secondary to intra-abdominal infection. Shock 2005, 23, 400–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morelli, A.; Ertmer, C.; Rehberg, S.; Lange, M.; Orecchioni, A.; Laderchi, A.; Bachetoni, A.; D’Alessandro, M.; Van Aken, H.; Pietropaoli, P.; et al. Phenylephrine versus norepinephrine for initial hemodynamic support of patients with septic shock: A randomized, controlled trial. Crit. Care 2008, 12, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myburgh, A.; Higgins, A.; Jovanovska, A.; Lipman, J.; Ramakrishnan, N.; Santamaria, J. A comparison of epinephrine and norepinephrine in critically ill patients. Intensive Care Med. 2008, 34, 2226–2234. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Clere-Jehl, R.; Legras, A.; Morichau-Beauchant, T.; Leone, M.; Frederique, G.; Quenot, J.P.; Kimmoun, A.; Cariou, A.; Lassus, J.; et al. Epinephrine Versus Norepinephrine for Cardiogenic Shock After Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2018, 72, 173–182. [Google Scholar] [CrossRef]
- Annane, D.; Vignon, P.; Renault, A.; Bollaert, P.E.; Charpentier, C.; Martin, C.; Troché, G.; Ricard, J.D.; Nitenberg, G.; Papazian, L.; et al. Norepinephrine plus dobutamine versus epinephrine alone for management of septic shock: A randomised trial. Lancet 2007, 370, 676–684. [Google Scholar] [CrossRef]
- Levy, B.; Perez, P.; Perny, J.; Thivilier, C.; Gerard, A. Comparison of norepinephrine-dobutamine to epinephrine for hemodynamics, lactate metabolism, and organ function variables in cardiogenic shock. A prospective, randomized pilot study*. Crit. Care Med. 2011, 39, 450–455. [Google Scholar] [CrossRef]
- Russell, J.A.; Vincent, J.L.; Kjølbye, A.L.; Olsson, H.; Blemings, A.; Spapen, H.; Carl, P.; Laterre, P.F.; Grundemar, L. Selepressin, a novel selective vasopressin V1A agonist, is an effective substitute for norepinephrine in a phase IIa randomized, placebo-controlled trial in septic shock patients. Crit. Care 2017, 21, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torgersen, C.; Dünser, M.W.; Wenzel, V.; Jochberger, S.; Mayr, V.; Schmittinger, C.A.; Lorenz, I.; Schmid, S.; Westphal, M.; Grander, W.; et al. Comparing two different arginine vasopressin doses in advanced vasodilatory shock: A randomized, controlled, open-label trial. Intensive Care Med. 2010, 36, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Hua, F.; Wang, X.; Zhu, L. Terlipressin decreases vascular endothelial growth factor expression and improves oxygenation in patients with acute respiratory distress syndrome and shock. J. Emerg. Med. 2013, 44, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Nuding, S.; Schröder, J.; Presek, P.; Wienke, A.; Müller-Werdan, U.; Ebelt, H.; Werdan, K. Reducing Elevated Heart Rates in Patients with Multiple Organ Dysfunction Syndrome with the i f (Funny Channel Current) Inhibitor Ivabradine. Shock 2018, 49, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Angus, D.C.; Artigas, A.; Kalil, A.; Basson, B.R.; Jamal, H.H.; Johnson, G.; Bernard, G.R. Effects of drotrecogin alfa (activated) on organ dysfunction in the PROWESS trial*. Crit. Care Med. 2003, 31, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Privalle, C.T.; Singer, M.; Lorente, J.A.; Boehm, E.; Meier-Hellmann, A.; Darius, H.; Ferrer, R.; Sirvent, J.-M.; Marx, G.; et al. Multicenter, Randomized, Placebo-Controlled Phase III Study of Pyridoxalated Hemoglobin Polyoxyethylene in Distributive Shock (PHOENIX)*. Crit. Care Med. 2015, 43, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Kinasewitz, G.T.; Privalle, C.T.; Imm, A.; Steingrub, J.S.; Malcynski, J.T.; Balk, R.A.; DeAngelo, J. Multicenter, randomized, placebo-controlled study of the nitric oxide scavenger pyridoxalated hemoglobin polyoxyethylene in distributive shock*. Crit. Care Med. 2008, 36, 1999–2007. [Google Scholar] [CrossRef]
- López, A.; Lorente, J.A.; Steingrub, J.; Bakker, J.; McLuckie, A.; Willatts, S.; Brockway, M.; Anzueto, A.; Holzapfel, L.; Breen, D.; et al. Multiple-center, randomized, placebo-controlled, double-blind study of the nitric oxide synthase inhibitor 546C88: Effect on survival in patients with septic shock*. Crit. Care Med. 2004, 32, 21–30. [Google Scholar] [CrossRef]
- Bakker, J.; Grover, R.; McLuckie, A.; Holzapfel, L.; Andersson, J.; Lodato, R.; Watson, D.; Grossman, S.; Donaldson, J.; Takala, J. Administration of the nitric oxide synthase inhibitor NG-methyl-l-arginine hydrochloride (546C88) by intravenous infusion for up to 72 hours can promote the resolution of shock in patients with severe sepsis: Results of a randomized, double-blind, placebo-controlled multicenter study (study no. 144-002)*. Crit. Care Med. 2004, 32, 1–12. [Google Scholar] [PubMed]
- Watson, D.; Grover, R.; Anzueto, A.; Lorente, J.; Smithies, M.; Bellomo, R.; Guntupalli, K.; Grossman, S.; Donaldson, J.; Le Gall, J.-R. Cardiovascular effects of the nitric oxide synthase inhibitor NG-methyl-l-arginine hydrochloride (546C88) in patients with septic shock: Results of a randomized, double-blind, placebo-controlled multicenter study (study no. 144-002)*. Crit. Care Med. 2004, 32, 13–20. [Google Scholar] [CrossRef]
- Bernard, G.R.; Francois, B.; Mira, J.-P.; Vincent, J.-L.; Dellinger, R.P.; Russell, J.A.; LaRosa, S.P.; Laterre, P.-F.; Levy, M.M.; Dankner, W.; et al. Evaluating the Efficacy and Safety of Two Doses of the Polyclonal Anti-Tumor Necrosis Factor-α Fragment Antibody AZD9773 in Adult Patients With Severe Sepsis and/or Septic Shock. Crit. Care Med. 2014, 42, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Carlet, J. INTERSEPT: An international, multicenter, placebo-controlled trial of monoclonal antibody to human tumor necrosis factor-α in patients with sepsis. Crit. Care Med. 1996, 24, 1431–1440. [Google Scholar] [CrossRef]
- Abraham, E.; Anzueto, A.; Gutierrez, G.; Tessler, S.; San Pedro, G.; Wunderink, R.; Dal Nogare, A.; Nasraway, S.; Berman, S.; Cooney, R.; et al. Double-blind randomised controlled trial of monoclonal antibody to human tumour necrosis factor in treatment of septic shock. Lancet 1998, 351, 929–933. [Google Scholar] [CrossRef]
- Annane, D.; Timsit, J.-F.; Megarbane, B.; Martin, C.; Misset, B.; Mourvillier, B.; Siami, S.; Chagnon, J.-L.; Constantin, J.-M.; Petitpas, F.; et al. Recombinant Human Activated Protein C for Adults with Septic Shock. A Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2013, 187, 1091–1097. [Google Scholar] [CrossRef]
- Dhainaut, J.F.; Antonelli, M.; Wright, P.; Desachy, A.; Reignier, J.; Lavoue, S.; Charpentier, J.; Belger, M.; Cobas-Meyer, M.; Maier, C.; et al. Extended drotrecogin alfa (activated) treatment in patients with prolonged septic shock. Intensive Care Med. 2009, 35, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Whitson, M.R.; Mo, E.; Nabi, T.; Healy, L.; Koenig, S.; Narasimhan, M.; Mayo, P.H. Feasibility, Utility, and Safety of Midodrine during Recovery Phase from Septic Shock. Chest 2016, 149, 1380–1383. [Google Scholar] [CrossRef]
- Rizvi, M.S.; Nei, A.M.; Gajic, O.; Mara, K.C.; Barreto, E.F. Continuation of Newly Initiated Midodrine Therapy After Intensive Care and Hospital Discharge. Crit. Care Med. 2019, 47, e648–e653. [Google Scholar] [CrossRef] [PubMed]
- Hammond, D.A.; Smith, M.N.; Peksa, G.D.; Trivedi, A.P.; Balk, R.A.; Menich, B.E. Midodrine as an Adjuvant to Intravenous Vasopressor Agents in Adults With Resolving Shock: Systematic Review and Meta-Analysis. J. Intensive Care Med. 2019, 35, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Payen, D.; Mateo, J.; Cavaillon, J.M.; Fraisse, F.; Floriot, C.; Vicaut, E. Impact of continuous venovenous hemofiltration on organ failure during the early phase of severe sepsis: A randomized controlled trial*. Crit. Care Med. 2009, 37, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Sun, S.; Zhu, B.; Mei, Z.; Wang, L.; Zhu, S.; Zhao, W. Effects of Coupled Plasma Filtration Adsorption on Septic Patients with Multiple Organ Dysfunction Syndrome. Ren. Fail. 2012, 34, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Landry, D.W.; Levin, H.R.; Gallant, E.M.; Ashton, R.C.; Seo, S.; D’Alessandro, D.; Oz, M.C.; Oliver, J.A. Vasopressin deficiency contributes to the vasodilation of septic shock. Circulation 1997, 95, 1122–1125. [Google Scholar] [CrossRef] [PubMed]
- Hammond, D.A.; Sacha, G.L.; Bissell, B.D.; Musallam, N.; Altshuler, D.; Flannery, A.H.; Lam, S.W.; Bauer, S.R. Effects of Norepinephrine and Vasopressin Discontinuation Order in the Recovery Phase of Septic Shock: A Systematic Review and Individual Patient Data Meta-Analysis. Pharmacotherapy 2019, 39, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Zhang, S.; Xu, J.; Xie, J.; Huang, L.; Huang, Y.; Yang, Y.; Qiu, H. Norepinephrine vs Vasopressin: Which Vasopressor Should Be Discontinued First in Septic Shock? A Meta-Analysis. Shock 2020, 53, 50–57. [Google Scholar] [CrossRef]
- Bellissant, E. Effect of hydrocortisone on phenylephrine– mean arterial pressure dose-response relationship in septic shock. Clin. Pharmacol. Ther. 2000, 68, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Cooper, M.S.; Stewart, P.M. Corticosteroid Insufficiency in Acutely Ill Patients. N. Engl. J. Med. 2003, 348, 727–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annane, D. Corticosteroids for septic shock. In Critical Care Medicine; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Morelli, A.; Singer, M.; Ranieri, V.M.; D’Egidio, A.; Mascia, L.; Orecchioni, A.; Piscioneri, F.; Guarracino, F.; Greco, E.; Peruzzi, M.; et al. Heart rate reduction with esmolol is associated with improved arterial elastance in patients with septic shock: A prospective observational study. Intensive Care Med. 2016, 42, 1528–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertini, P.; Guarracino, F. Septic Shock and the Heart. Curr. Anesthesiol. Rep. 2019, 9, 165–173. [Google Scholar] [CrossRef]
- Angus, D.C.; Barnato, A.E.; Bell, D.; Bellomo, R.; Chong, C.R.; Coats, T.J.; Davies, A.; Delaney, A.; Harrison, D.A.; Holdgate, A.; et al. A systematic review and meta-analysis of early goal-directed therapy for septic shock: The ARISE, ProCESS and ProMISe Investigators. Intensive Care Med. 2015, 41, 1549–1560. [Google Scholar] [CrossRef] [PubMed]
- Hamzaoui, O.; Georger, J.F.; Monnet, X.; Ksouri, H.; Maizel, J.; Richard, C.; Teboul, J.L. Early administration of norepinephrine increases cardiac preload and cardiac output in septic patients with life-threatening hypotension. Crit. Care 2010, 14, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Monnet, X.; Jabot, J.; Maizel, J.; Richard, C.; Teboul, J.-L. Norepinephrine increases cardiac preload and reduces preload dependency assessed by passive leg raising in septic shock patients*. Crit. Care Med. 2011, 39, 689–694. [Google Scholar] [CrossRef]
- Malbrain, M.L.N.G.; Van Regenmortel, N.; Saugel, B.; De Tavernier, B.; Van Gaal, P.J.; Joannes-Boyau, O.; Teboul, J.L.; Rice, T.W.; Mythen, M.; Monnet, X. Principles of fluid management and stewardship in septic shock: It is time to consider the four D’s and the four phases of fluid therapy. Ann. Intensive Care. 2018, 8, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Bar, S.; Nguyen, M.; Abou-Arab, O.; Dupont, H.; Bouhemad, B.; Guinot, P.-G. Dynamic Arterial Elastance Is Associated With the Vascular Waterfall in Patients Treated With Norepinephrine: An Observational Study. Front. Physiol. 2021, 12, 514. [Google Scholar] [CrossRef]
- Lamontagne, F.; Richards-Belle, A.; Thomas, K.; Harrison, D.A.; Sadique, M.Z.; Grieve, R.D.; Camsooksai, J.; Darnell, R.; Gordon, A.C.; Henry, D.; et al. Effect of Reduced Exposure to Vasopressors on 90-Day Mortality in Older Critically Ill Patients with Vasodilatory Hypotension: A Randomized Clinical Trial. JAMA J. Am. Med. Assoc. 2020. [Google Scholar] [CrossRef]
- Marshall, J.C. Choosing the Best Blood Pressure Target for Vasopressor Therapy. JAMA J. Am. Med. Assoc. 2020, 323, 931–933. [Google Scholar] [CrossRef]
- Schmittinger, C.A.; Torgersen, C.; Luckner, G.; Schröder, D.C.H.; Lorenz, I.; Dünser, M.W. Adverse cardiac events during catecholamine vasopressor therapy: A prospective observational study. Intensive Care Med. 2012, 38, 950–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckley, M.S.; Barletta, J.F.; Smithburger, P.L.; Radosevich, J.J.; Kane-Gill, S.L. Catecholamine Vasopressor Support Sparing Strategies in Vasodilatory Shock. Pharmacother. J. Hum. Pharmacol. Drug. Ther. 2019, 39, 382–398. [Google Scholar] [CrossRef]
- Nguyen, M.; Abou-Arab, O.; Bar, S.; Dupont, H.; Bouhemad, B.; Guinot, P.-G. Echocardiographic measure of dynamic arterial elastance predict pressure response during norepinephrine weaning: An observational study. Sci. Rep. 2021, 11, 1–7. [Google Scholar] [CrossRef]
- Nguyen, M.; Berhoud, V.; Bartamian, L.; Martin, A.; Ellouze, O.; Bouhemad, B.; Guinot, P.-G. Agreement between different non-invasive methods of ventricular elastance assessment for the monitoring of ventricular–arterial coupling in intensive care. J. Clin. Monit. Comput. 2019, 34, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Guinot, P.-G.; Bernard, E.; Levrard, M.; Dupont, H.; Lorne, E. Dynamic arterial elastance predicts mean arterial pressure decrease associated with decreasing norepinephrine dosage in septic shock. Crit. Care 2015, 19, 14. [Google Scholar] [CrossRef] [Green Version]
- Bar, S.; Leviel, F.; Abou Arab, O.; Badoux, L.; Mahjoub, Y.; Dupont, H.; Lorne, E.; Guinot, P.-G. Dynamic arterial elastance measured by uncalibrated pulse contour analysis predicts arterial-pressure response to a decrease in norepinephrine. Br. J. Anaesth. 2018, 7, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guinot, P.-G.; Longrois, D.; Kamel, S.; Lorne, E.; Dupont, H. Ventriculo-Arterial Coupling Analysis Predicts the Hemodynamic Response to Norepinephrine in Hypotensive Postoperative Patients: A Prospective Observational Study. Crit. Care Med. 2018, 46, e17–e25. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.P.; Ting, C.T.; Yang, T.M.; Liu, C.P.; Maughan, W.L.; Chang, M.S.; Kass, D.A. Effective arterial elastance as index of arterial vascular load in humans. Circulation 1992, 86, 513–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, M.I.M.; Jian, Z.; Settels, J.J.; Hatib, F.; Cecconi, M.; Pinsky, M.R. Reliability of effective arterial elastance using peripheral arterial pressure as surrogate for left ventricular end-systolic pressure. J. Clin. Monit. Comput. 2019, 33, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.C.; Mondy, J.S.; Meredith, J.W.; Miller, P.R.; Owings, J.T.; Holcroft, J.W. Clinical application of ventricular end-systolic elastance and the ventricular pressure-volume diagram. Shock 1997, 7, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-H.; Fetics, B.; Nevo, E.; Rochitte, C.E.; Chiou, K.-R.; Ding, P.-A.; Kawaguchi, M.; Kass, D.A. Noninvasive single-beat determination of left ventricular end-systolic elastance in humans. J. Am. Coll. Cardiol. 2001, 38, 2028–2034. [Google Scholar] [CrossRef] [Green Version]
- Kass, D.A.; Kelly, R.P. Ventriculo-arterial coupling: Concepts, assumptions, and applications. Ann. Biomed. Eng. 1992, 20, 41–62. [Google Scholar] [CrossRef]
- Wijnberge, M.; Geerts, B.F.; Hol, L.; Lemmers, N.; Mulder, M.P.; Berge, P.; Schenk, J.; Terwindt, L.E.; Hollmann, M.W.; Vlaar, A.P.; et al. Effect of a Machine Learning–Derived Early Warning System for Intraoperative Hypotension vs Standard Care on Depth and Duration of Intraoperative Hypotension During Elective Noncardiac Surgery. JAMA 2020, 323, 1052–1060. [Google Scholar] [CrossRef]
- Venkatesh, B.; Khanna, A.K.; Cohen, J. Less is more: Catecholamine-sparing strategies in septic shock. Intensive Care Med. 2019, 45, 1810–1812. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention | References | Outcome Evaluated | Clinical Effect | Proposal |
|---|---|---|---|---|
| Hemodynamic management | ||||
| Active, hemodynamic algorithm | [7,13] | Dose and duration | Positive | Systematic |
| Blood pressure target | [16,17] | Dose and duration | Positive | Individualized on organ perfusion |
| Wean norepinephrine before vasopressin | [14] | Duration | Uncertain | Wean norepinephrine first |
| Pharmocological | ||||
| Dopamine | [3] | Dose and duration | Negative | No |
| Terlipressin | [18,19,20,21,22,23] | Dose and duration | Negative | No |
| Vasopressin | [4,20,24,25,26,27,28,29,30,31] | Dose and duration | Uncertain | Consider if norepinephrine > 0.2 µg/kg/min |
| Angiotensin-2 | [32,33] | Dose and duration | Uncertain | Mores studies need |
| Glucocorticoids | [34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52] | Dose and duration | Positive | Systematic if norepinephrine > 0.2 µg/kg/min |
| Fluid therapy and hemodynamic goal direct therapy | [53,54,55,56,57,58,59,60,61,62,63,64,65,66] | Dose and duration | Uncertain | Assess preload dependency |
| Colloid | [67,68] | Dose and duration | Positive | Not recommended |
| Beta-blockers | [69] | Dose | Uncertain | Selected population with persistent tachycardia |
| Methylene blue | [70,71] | Dose and duration | Uncertain | Rescue |
| Mineralocorticosteroids | [39,72] | Duration | Negative | No |
| N-acetyl cysteine | [73,74,75] | Dose and duration | Uncertain | No |
| Vitamin C | [43,44,73,76,77,78] | Dose and duration | Negative | No |
| Oral vasopressor | [15,79] | Dose and duration | Negative | No |
| Non-pharmacological | ||||
| Body temperature | [80,81,82] | Dose and duration | Positive | Target normothermia |
| High volume hemo-filtration | [83,84,85,86,87,88] | Dose and duration | Negative | No |
| Adsorption | [89,90,91,92,93] | Dose and duration | Uncertain | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guinot, P.-G.; Martin, A.; Berthoud, V.; Voizeux, P.; Bartamian, L.; Santangelo, E.; Bouhemad, B.; Nguyen, M. Vasopressor-Sparing Strategies in Patients with Shock: A Scoping-Review and an Evidence-Based Strategy Proposition. J. Clin. Med. 2021, 10, 3164. https://doi.org/10.3390/jcm10143164
Guinot P-G, Martin A, Berthoud V, Voizeux P, Bartamian L, Santangelo E, Bouhemad B, Nguyen M. Vasopressor-Sparing Strategies in Patients with Shock: A Scoping-Review and an Evidence-Based Strategy Proposition. Journal of Clinical Medicine. 2021; 10(14):3164. https://doi.org/10.3390/jcm10143164
Chicago/Turabian StyleGuinot, Pierre-Grégoire, Audrey Martin, Vivien Berthoud, Pierre Voizeux, Loic Bartamian, Erminio Santangelo, Belaid Bouhemad, and Maxime Nguyen. 2021. "Vasopressor-Sparing Strategies in Patients with Shock: A Scoping-Review and an Evidence-Based Strategy Proposition" Journal of Clinical Medicine 10, no. 14: 3164. https://doi.org/10.3390/jcm10143164
APA StyleGuinot, P. -G., Martin, A., Berthoud, V., Voizeux, P., Bartamian, L., Santangelo, E., Bouhemad, B., & Nguyen, M. (2021). Vasopressor-Sparing Strategies in Patients with Shock: A Scoping-Review and an Evidence-Based Strategy Proposition. Journal of Clinical Medicine, 10(14), 3164. https://doi.org/10.3390/jcm10143164