
Impact of Morphotype on Image Quality and Diagnostic Performance of Ultra-Low-Dose Chest CT

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
2.2. CT Acquisition
2.3. Dosimetry
2.4. Quantitative Image Quality
2.5. Qualitative Image Quality
2.6. Diagnostic Performance
2.7. Statistical Analysis
3. Results
3.1. Population
3.2. Dosimetry
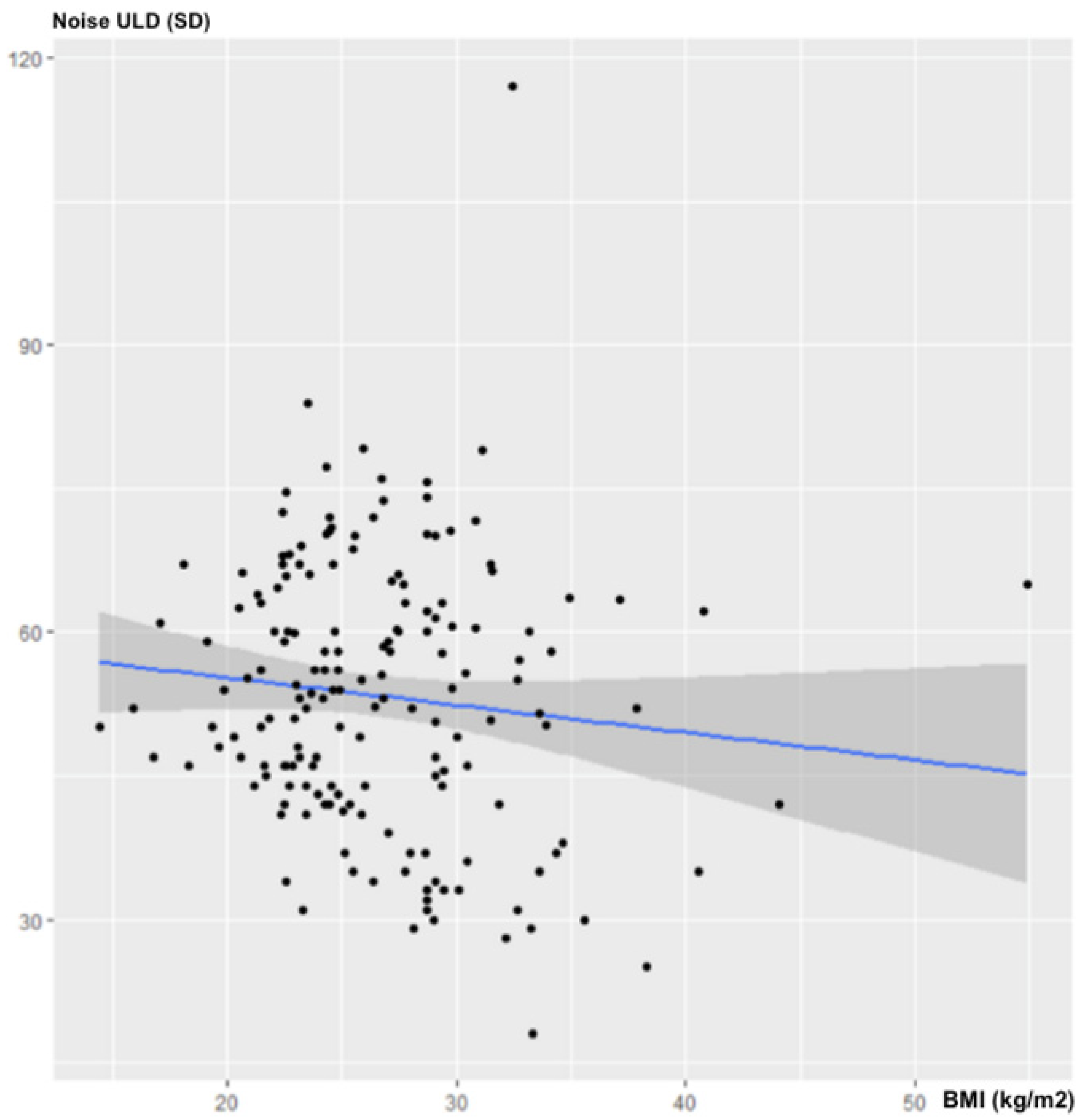
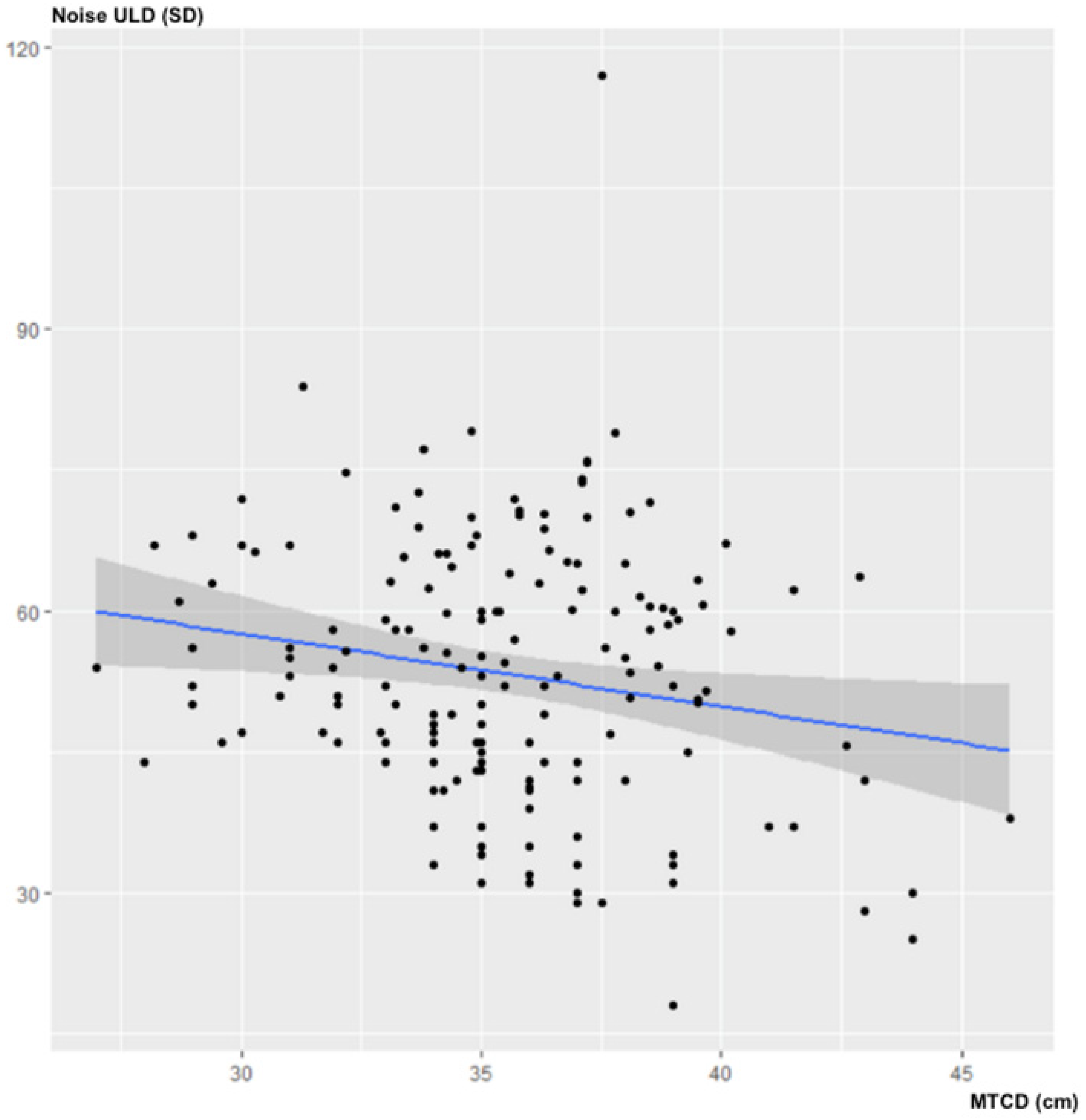
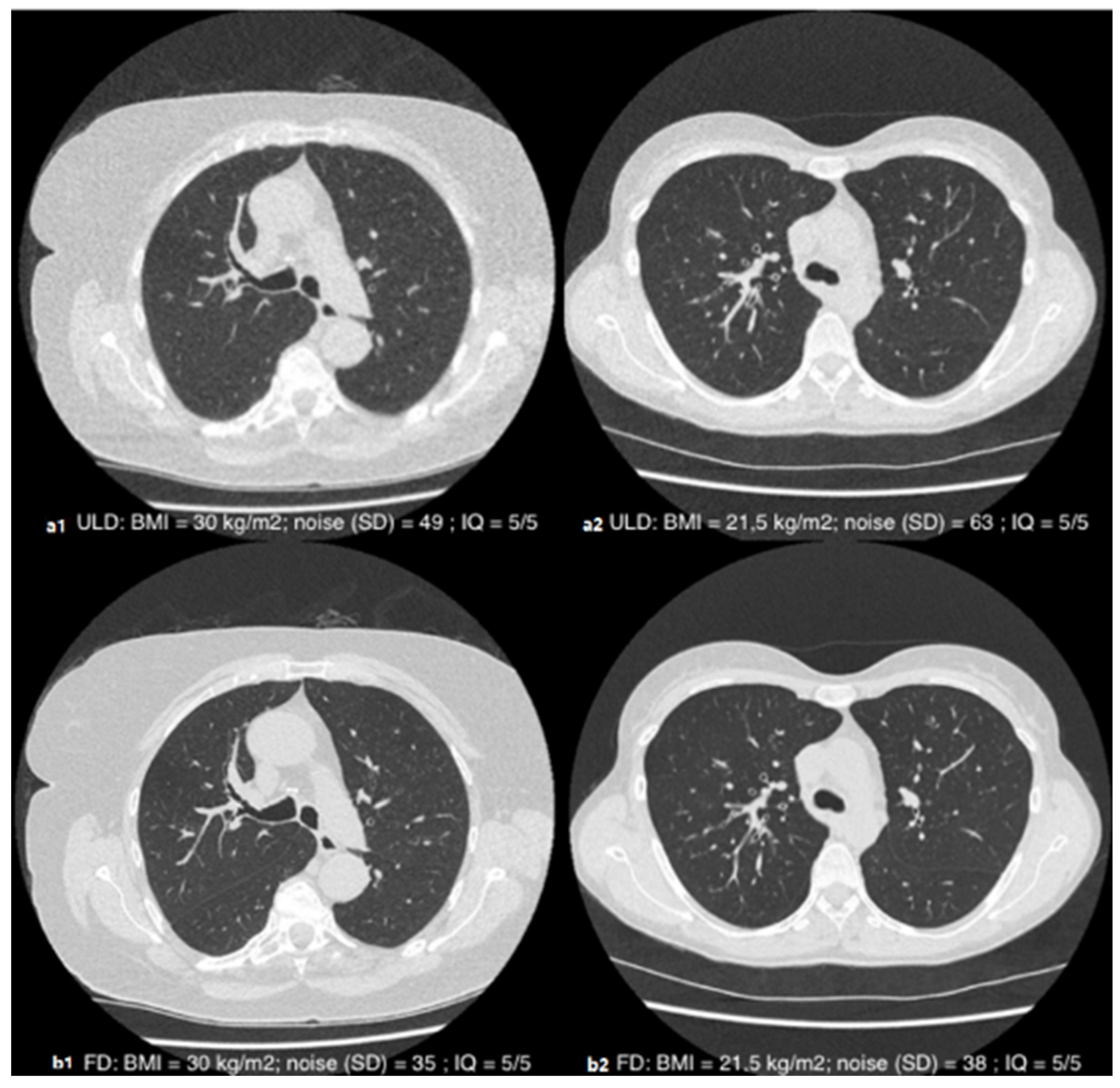
3.3. Quantitative Image Quality
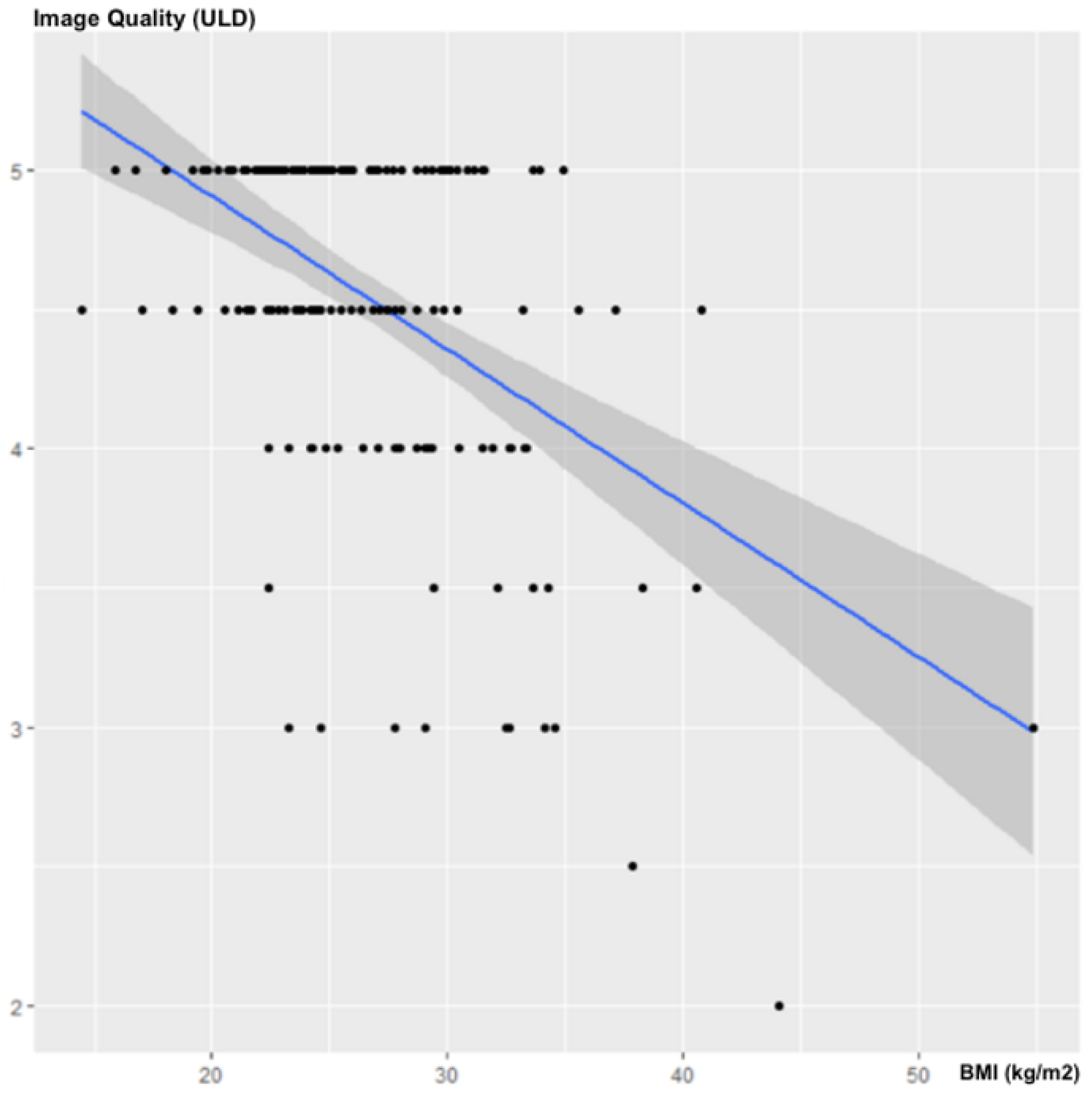
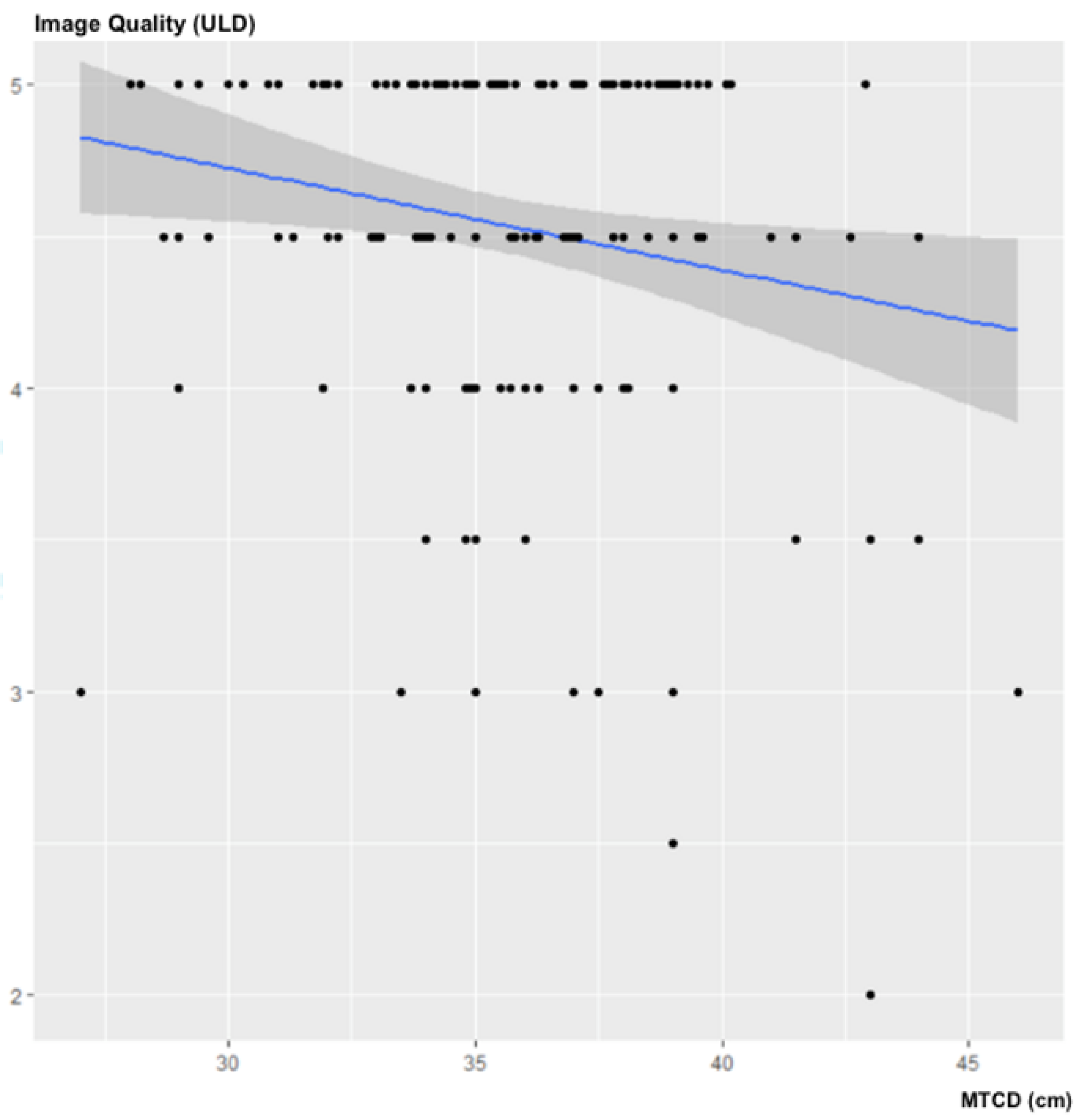
3.4. Subjective Image Quality
3.5. Diagnostic Performance
3.6. Diagnostic Performance per Patient
3.7. Diagnostic Performance per Lesion
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| CT | Computed Tomography |
| DLP | Dose length Product |
| ED | Effective Dose |
| FD | Full Dose |
| MTCD | Maximum Transverse Chest Diameter |
| ROI | Region Of Interest |
| SD | Standard Deviation |
| ULD | Ultra-Low Dose |
References
- Brenner, D.J.; Hall, E.J. Computed Tomography—An Increasing Source of Radiation Exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [Green Version]
- Ohana, M.; Ludes, C.; Schaal, M.; Meyer, E.; Jeung, M.-Y.; Labani, A.; Roy, C. Quel avenir pour la radiographie thoracique face au scanner ultra-low dose? Rev. Pneumol. Clin. 2017, 73, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Kanal, K.M.; Butler, P.F.; Sengupta, D.; Bhargavan-Chatfield, M.; Coombs, L.P.; Morin, R.L. U.S. Diagnostic Reference Levels and Achievable Doses for 10 Adult CT Examinations. Radiology 2017, 284, 120–133. [Google Scholar] [CrossRef] [Green Version]
- Sarma, A.; Heilbrun, M.E.; Conner, K.E.; Stevens, S.M.; Woller, S.C.; Elliott, C.G. Radiation and Chest CT Scan Examinations. Chest 2012, 142, 750–760. [Google Scholar] [CrossRef] [PubMed]
- Nicolan, B.; Greffier, J.; Dabli, D.; de Forges, H.; Arcis, E.; Al Zouabi, N.; Larbi, A.; Beregi, J.-P.; Frandon, J. Diagnostic performance of ultra-low dose versus standard dose CT for non-traumatic abdominal emergencies. Diagn. Interv. Imaging 2021, 102, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Beister, M.; Kolditz, D.; Kalender, W.A. Iterative reconstruction methods in X-ray CT. Phys. Med. 2012, 28, 94–108. [Google Scholar] [CrossRef]
- Singh, R.; Digumarthy, S.R.; Muse, V.V.; Kambadakone, A.R.; Blake, M.A.; Tabari, A.; Hoi, Y.; Akino, N.; Angel, E.; Madan, R.; et al. Image Quality and Lesion Detection on Deep Learning Reconstruction and Iterative Reconstruction of Submillisievert Chest and Abdominal CT. AJR Am. J. Roentgenol. 2020, 214, 566–573. [Google Scholar] [CrossRef]
- Ludes, C.; Schaal, M.; Labani, A.; Jeung, M.Y.; Roy, C.; Ohana, M. Ultra-low dose chest CT: The end of chest radiograph? Presse Med. 2016, 45, 291–301. [Google Scholar] [CrossRef]
- Ohana, M.; Ludes, C.; Schaal, M.; Meyer, E.; Jeung, M.Y.; Labani, A.; Roy, C. What future for chest X-ray against ultra-low-dose computed tomography? Rev. Pneumol. Clin. 2016, 73, 3–12. [Google Scholar] [CrossRef]
- Tækker, M.; Kristjánsdóttir, B.; Graumann, O.; Laursen, C.B.; Pietersen, P.I. Diagnostic accuracy of low-dose and ultra-low-dose CT in detection of chest pathology: A systematic review. Clin. Imaging 2021, 74, 139–148. [Google Scholar] [CrossRef]
- Lee, S.W.; Kim, Y.; Shim, S.S.; Lee, J.K.; Lee, S.J.; Ryu, Y.J.; Chang, J.H. Image quality assessment of ultra low-dose chest CT using sinogram-affirmed iterative reconstruction. Eur. Radiol. 2014, 24, 817–826. [Google Scholar] [CrossRef]
- Messerli, M.; Kluckert, T.; Knitel, M.; Wälti, S.; Desbiolles, L.; Rengier, F.; Warschkow, R.; Bauer, R.W.; Alkadhi, H.; Leschka, S.; et al. Ultralow dose CT for pulmonary nodule detection with chest x-ray equivalent dose—A prospective intra-individual comparative study. Eur. Radiol. 2017, 27, 3290–3299. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Park, S.Y.; Lee, H.Y.; Lee, K.S.; Shin, K.E.; Moon, J.W. Ultra-Low-Dose Chest CT in Patients with Neutropenic Fever and Hematologic Malignancy: Image Quality and Its Diagnostic Performance. Cancer Res. Treat. 2014, 46, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Liu, B.; Meng, H.; Lv, W.; Jia, H. Efficacy and Radiation Exposure of Ultra-Low-Dose Chest CT at 100 kVp with Tin Filtration in CT-Guided Percutaneous Core Needle Biopsy for Small Pulmonary Lesions Using a Third-Generation Dual-Source CT Scanner. J. Vasc. Interv. Radiol. 2019, 30, 95–102. [Google Scholar] [CrossRef]
- Hu-Wang, E.; Schuzer, J.L.; Rollison, S.; Leifer, E.S.; Steveson, C.; Gopalakrishnan, V.; Yao, J.; Machado, T.; Jones, A.M.; Julien-Williams, P.; et al. Chest CT Scan at Radiation Dose of a Posteroanterior and Lateral Chest Radiograph Series: A Proof of Principle in Lymphangioleiomyomatosis. Chest 2019, 155, 528–533. [Google Scholar] [CrossRef]
- Macri, F.; Greffier, J.; Pereira, F.; Rosa, A.C.; Khasanova, E.; Claret, P.-G.; Larbi, A.; Gualdi, G.; Beregi, J.P. Value of ultra-low-dose chest CT with iterative reconstruction for selected emergency room patients with acute dyspnea. Eur. J. Radiol. 2016, 85, 1637–1644. [Google Scholar] [CrossRef] [PubMed]
- Beregi, J.; Greffier, J. Low and ultra-low dose radiation in CT: Opportunities and limitations. Diagn. Interv. Imaging 2019, 100, 63–64. [Google Scholar] [CrossRef] [PubMed]
- Schaal, M.; Séverac, F.; Labani, A.; Jeung, M.-Y.; Roy, C.; Ohana, M. Diagnostic Performance of Ultra-Low-Dose Computed Tomography for Detecting Asbestos-Related Pleuropulmonary Diseases: Prospective Study in a Screening Setting. PLoS ONE 2016, 11, e0168979. [Google Scholar] [CrossRef]
- Ludes, C.; Labani, A.; Severac, F.; Jeung, M.; Leyendecker, P.; Roy, C.; Ohana, M. Ultra-low-dose unenhanced chest CT: Prospective comparison of high kV/low mA versus low kV/high mA protocols. Diagn. Interv. Imaging 2019, 100, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Meyer, E.; Labani, A.; Schaeffer, M.; Jeung, M.-Y.; Ludes, C.; Meyer, A.; Roy, C.; Leyendecker, P.; Ohana, M. Wide-volume versus helical acquisition in unenhanced chest CT: Prospective intra-patient comparison of diagnostic accuracy and radiation dose in an ultra-low-dose setting. Eur. Radiol. 2019, 29, 6858–6866. [Google Scholar] [CrossRef]
- Martini, K.; Moon, J.; Revel, M.; Dangeard, S.; Ruan, C.; Chassagnon, G. Optimization of acquisition parameters for reduced-dose thoracic CT: A phantom study. Diagn. Interv. Imaging 2020, 101, 269–279. [Google Scholar] [CrossRef]
- Huda, W.; Ogden, K.M.; Khorasani, M.R. Converting Dose-Length Product to Effective Dose at CT. Radiology 2008, 248, 995–1003. [Google Scholar] [CrossRef] [PubMed]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of Terms for Thoracic Imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prakash, P.; Kalra, M.K.; Ackman, J.B.; Digumarthy, S.R.; Hsieh, J.; Do, S.; Shepard, J.-A.O.; Gilman, M.D. Diffuse Lung Disease: CT of the Chest with Adaptive Statistical Iterative Reconstruction Technique. Radiology 2010, 256, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatsugami, F.; Matsuki, M.; Nakai, G.; Inada, Y.; Kanazawa, S.; Takeda, Y.; Morita, H.; Takada, H.; Yoshikawa, S.; Fukumura, K.; et al. The effect of adaptive iterative dose reduction on image quality in 320-detector row CT coronary angiography. Br. J. Radiol. 2012, 85, e378–e382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akagi, M.; Nakamura, Y.; Higaki, T.; Narita, K.; Honda, Y.; Awai, K. Deep learning reconstruction of equilibrium phase CT images in obese patients. Eur. J. Radiol. 2020, 133, 109349. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ULD-CT | FD-CT (Reference) | |
|---|---|---|
| Voltage (kV) | 135 | 120 |
| Tube current (mA) | 10 | 80–700 |
| Tube current-time product (mAs) | 3 | 20–200 |
| Pitch | 0.813 | 0.813 |
| Rotation time (s) | 0.275 | 0.275 |
| Collimation | 0.5 × 80 | 0.5 × 80 |
| Reconstructed slice thickness (mm) | 1 | 1 |
| Reconstruction algorithm | AIDR-3D | AIDR-3D |
| Subjective Image Quality | Ratings | |
|---|---|---|
| 1 | Unacceptable image quality | non-diagnostic examination |
| 2 | Poor image quality | |
| 3 | Moderate image quality | diagnostic examination |
| 4 | Good image quality | |
| 5 | Excellent image quality | |
| Notes | R1 | R2 | Average |
|---|---|---|---|
| 1 | 0 (0%) | 0 (0%) | 0 |
| 2 | 2 (1.2%) | 1 (0.6%) | 1.5 |
| 3 | 10 (5.9%) | 19 (11.2%) | 14.5 |
| 4 | 38 (22.3%) | 51 (30%) | 44.5 |
| 5 | 120 (70.6%) | 99 (58.2%) | 109.5 |
| Average ± SD | 4.62 ± 0.65 | 4.46 ± 0.71 | 4.5 ± 0.70 |
| Number of Lesions (n) | ULD-CT vs. FD-CT | Error Rate % | ||||
|---|---|---|---|---|---|---|
| Se (%) | Sp (%) | VPP (%) | VPN (%) | |||
| Abnormalities | 243 | 77 (188/243) | 99 (1276/1287) | 94 (188/199) | 65 (860/1331) | 25.9 |
| Solid nodule | 66 | 86 (57/66) | 94 (98/104) | 90 (57/63) | 92 (98/107) | 9 |
| 95% CI | [0.75; 0.93] | [0.88; 0.98] | [0.80; 0.96] | [0.84; 0.96] | ||
| Ground glass nodule | 8 | 62 (5/8) | 99 (161/162) | 83 (5/6) | 98 (161/164) | 2 |
| 95% CI | [0.24; 0.91] | [0.97; 0.99] | [0.36; 0.99] | [0.95; 0.99] | ||
| Mass > 3 cm | 3 | 100 (3/3) | 100 (167/167) | 100 (3/3) | 100 (167/167) | 0 |
| 95% CI | [0.29; 1] | [0.98; 1] | [0.29; 1] | 0.98; 1] | ||
| Ground glass opacity | 30 | 70 (21/30) | 99 (139/140) | 95 (21/22) | 94 (139/148) | 6 |
| 95% CI | [0.51; 0.85] | [0.96; 0.99] | [0.77; 0.99] | [0.89; 0.97] | ||
| Alveolar consolidation | 24 | 83 (20/24) | 99 (144/146) | 91 (20/22) | 97 (144/148) | 4 |
| 95% CI | [0.63; 0.95] | [0.95; 0.99] | [0.71; 0.99] | 0.93; 0.99] | ||
| Emphysema | 58 | 81 (47/58) | 99 (111/112) | 98 (47/48) | 91 (111/122) | 7 |
| 95% CI | [0.69; 0.90] | [0.95; 0.99] | [0.89; 0.99] | [0.84; 0.95] | ||
| Interstitial septal thickening | 11 | 45 (5/11) | 100 (159/159) | 100 (5/5) | 96 (159/165) | 4 |
| 95% CI | [0.17; 0.77] | [0.98; 1] | [0.48; 1] | [0.92; 0.99] | ||
| Bronchiectasis | 31 | 71 (22/31) | 100 (139/139) | 100 (22/22) | 94 (139/148) | 5 |
| 95% CI | [0.52; 0.86] | [0.97; 1] | [0.85; 1] | [0.89; 0.97] | ||
| Fibrosis | 12 | 67 (8/12) | 100 (158/158) | 100 (8/8) | 98 (158/162) | 2 |
| 95% CI | [0.35; 0.90] | [0.98; 1] | [0.63; 1] | [0.94; 0.99] | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortlieb, A.-C.; Labani, A.; Severac, F.; Jeung, M.-Y.; Roy, C.; Ohana, M. Impact of Morphotype on Image Quality and Diagnostic Performance of Ultra-Low-Dose Chest CT. J. Clin. Med. 2021, 10, 3284. https://doi.org/10.3390/jcm10153284
Ortlieb A-C, Labani A, Severac F, Jeung M-Y, Roy C, Ohana M. Impact of Morphotype on Image Quality and Diagnostic Performance of Ultra-Low-Dose Chest CT. Journal of Clinical Medicine. 2021; 10(15):3284. https://doi.org/10.3390/jcm10153284
Chicago/Turabian StyleOrtlieb, Anne-Claire, Aissam Labani, François Severac, Mi-Young Jeung, Catherine Roy, and Mickaël Ohana. 2021. "Impact of Morphotype on Image Quality and Diagnostic Performance of Ultra-Low-Dose Chest CT" Journal of Clinical Medicine 10, no. 15: 3284. https://doi.org/10.3390/jcm10153284
APA StyleOrtlieb, A. -C., Labani, A., Severac, F., Jeung, M. -Y., Roy, C., & Ohana, M. (2021). Impact of Morphotype on Image Quality and Diagnostic Performance of Ultra-Low-Dose Chest CT. Journal of Clinical Medicine, 10(15), 3284. https://doi.org/10.3390/jcm10153284