
Hospital Dentistry for Intensive Care Unit Patients: A Comprehensive Review

 ,
,  ,
,
Abstract
:1. Introduction
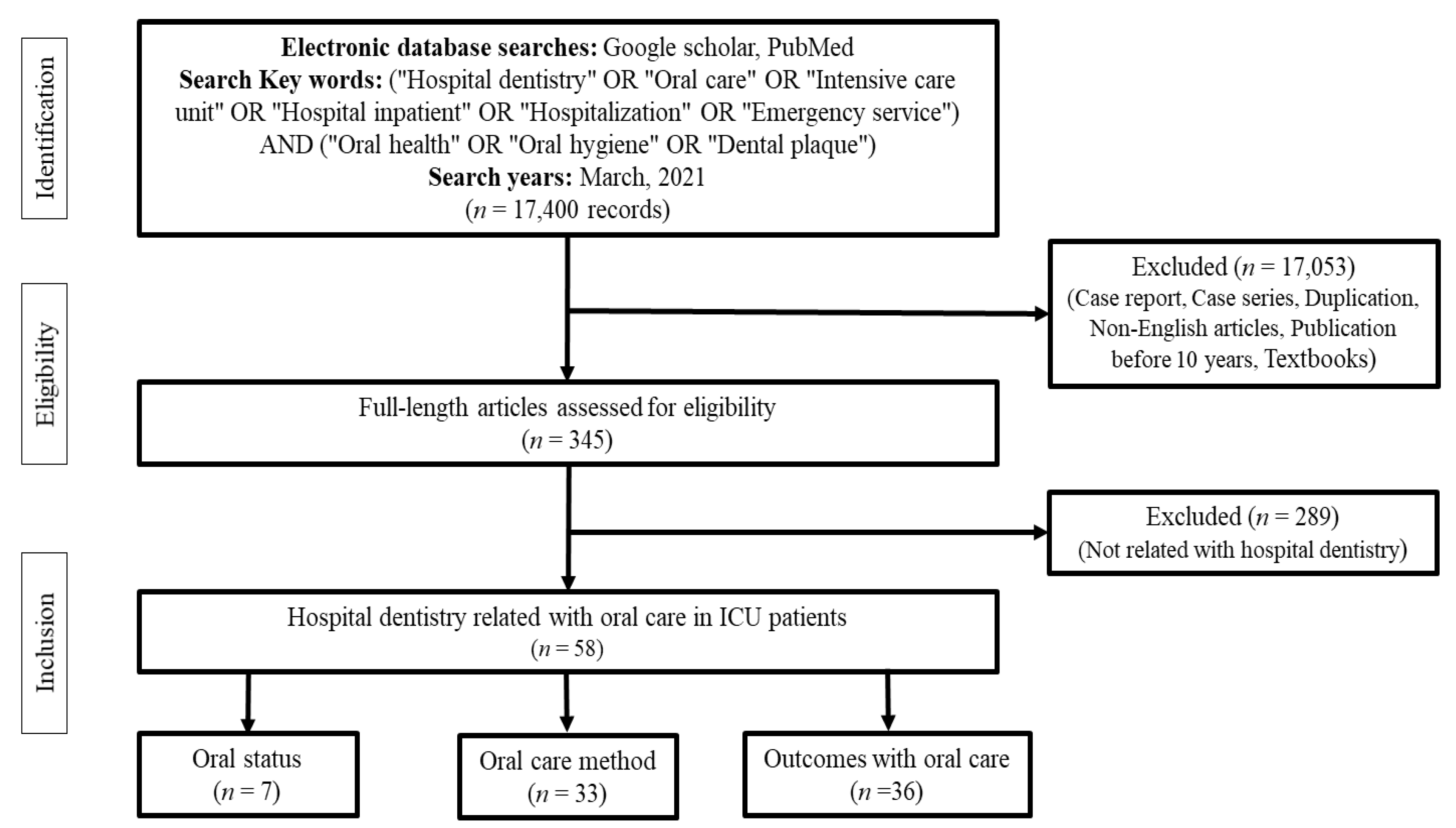
2. Methods
3. Results
3.1. Assessment of Oral Status in Intensive Care Unit Patients
3.2. Oral Hygiene Management Methods for Patients in ICUs
3.2.1. Application of CHX
3.2.2. Tooth Brushing Method
3.2.3. Application of Quantitative Light-Induced Fluorescence Technology
3.3. Outcomes of Oral Management of ICU Patients
3.3.1. Effect of Oral Hygiene Management by Dental Experts
3.3.2. Effects of Oral Hygiene Management Other Than the Prevention of Respiratory Infections
4. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martinez, B.; Fidelis, F.; Mastrocolla, L.; Tempest, L.; Araujo, T.; Castro, F.; Abbud, A.; Kassis, E.; Filho, I. Main aspects of hospital dentistry: Review of its importance. Int. J. Adv. Res. 2016, 4, 2099–2106. [Google Scholar] [CrossRef] [Green Version]
- Javadinia, S.A.; Kuchi, Z.; Saadatju, A.; Tabasi, M.; Adib-Hajbaghery, M. Oral care in trauma patients admitted to the ICU: Viewpoints of ICU nurses. Trauma Mon. 2014, 19, e15110. [Google Scholar] [CrossRef]
- Hillier, B.; Wilson, C.; Chamberlain, D.; King, L. Preventing ventilator-associated pneumonia through oral care, product selection, and application method: A literature review. AACN Adv. Crit. Care 2013, 24, 38–58. [Google Scholar] [CrossRef] [PubMed]
- Jerônimo, L.S.; Abreu, L.G.; Cunha, F.A.; Lima, R.P.E. Association between periodontitis and nosocomial pneumonia: A systematic review and meta-analysis of observational studies. Oral Health Prev. Dent. 2020, 18, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Bellissimo-Rodrigues, W.T.; Menegueti, M.G.; Gaspar, G.G.; de Souza, H.C.C.; Auxiliadora-Martins, M.; Basile-Filho, A.; Martinez, R.; Bellissimo-Rodrigues, F. Is it necessary to have a dentist within an intensive care unit team? Report of a randomised clinical trial. Int. Dent. J. 2018, 68, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Cao, Y.; Lin, J.; Ng, L.; Needleman, I.; Walsh, T.; Li, C. Oral care measures for preventing nursing home-acquired pneumonia. Cochrane Database Syst. Rev. 2018, 9, CD012416. [Google Scholar] [CrossRef] [PubMed]
- Augustyn, B. Ventilator-associated pneumonia: Risk factors and prevention. Crit. Care Nurse 2007, 27, 32–39. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho Baptista, I.M.; Martinho, F.C.; Nascimento, G.G.; da Rocha Santos, C.E.; Prado, R.F.D.; Valera, M.C. Colonization of oropharynx and lower respiratory tract in critical patients: Risk of ventilator-associated pneumonia. Arch. Oral Biol. 2018, 85, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Fusconi, M.; Greco, A.; Galli, M.; Polimeni, A.; Yusef, M.; Cianni, S.D.; De Soccio, G.; FR, F.S.; Lombardi, R.; de Vincentiis, M. Odontogenic phlegmons and abscesses in relation to the financial situation of Italian families. Minerva Stomatol. 2019, 68, 236–241. [Google Scholar] [CrossRef]
- Satheeshkumar, P.S.; Papatheodorou, S.; Sonis, S. Enhanced oral hygiene interventions as a risk mitigation strategy for the prevention of non-ventilator-associated pneumonia: A systematic review and meta-analysis. Br. Dent. J. 2020, 228, 615–622. [Google Scholar] [CrossRef]
- Gershonovitch, R.; Yarom, N.; Findler, M. Preventing Ventilator-Associated Pneumonia in Intensive Care Unit by improved Oral Care: A Review of Randomized Control Trials. SN Compr. Clin. Med. 2020, 2, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Blum, D.F.C.; Munaretto, J.; Baeder, F.M.; Gomez, J.; Castro, C.P.P.; Bona, Á.D. Influence of dentistry professionals and oral health assistance protocols on intensive care unit nursing staff. A survey study. Rev. Bras. Ter. Intensiva 2017, 29, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Sreenivasan, V.P.D.; Ganganna, A.; Rajashekaraiah, P.B. Awareness among intensive care nurses regarding oral care in critically ill patients. J. Indian Soc. Periodontol. 2018, 22, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Sgarioni, R.M.d.P.; Miranda, A.; Carvalho, C.B.d.; Sousa, M.G. Knowledge of Intensive Care Professionals About Oral Health Measures Applied in a Private Hospital ICU. EC Dent. Sci. 2017, 8, 165–171. [Google Scholar]
- Miranda, A.F.; de Paula, R.M.; de Castro Piau, C.G.; Costa, P.P.; Bezerra, A.C. Oral care practices for patients in Intensive Care Units: A pilot survey. Indian J. Crit. Care Med. Peer Rev. Off. Publ. Indian Soc. Crit. Care Med. 2016, 20, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Araújo, R.J.; Oliveira, L.C.; Hanna, L.M.; Corrêa, A.M.; Carvalho, L.H.; Alvares, N.C. Perceptions and actions of oral care performed by nursing teams in intensive care units. Rev. Bras. Ter. Intensiva 2009, 21, 38–44. [Google Scholar] [PubMed]
- Amaral, C.O.F.d.; Pereira, L.C.; Guy, N.A.; Amaral Filho, M.S.P.d.; Logar, G.d.A.; Straioto, F.G. Oral health evaluation of cardiac patients admitted to cardiovascular pre-surgery intervention. RGO Rev. Gaúcha Odontol. 2016, 64, 419–424. [Google Scholar] [CrossRef] [Green Version]
- Amaral, C.O.F.d.; Belon, L.M.R.; Silva, E.A.d.; Nadai, A.d.; Amaral Filho, M.S.P.d.; Straioto, F.G. The importance of hospital dentistry: Oral health status in hospitalized patients. RGO Rev. Gaúcha Odontol. 2018, 66, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Eilers, J.; Berger, A.M.; Petersen, M.C. Development, testing, and application of the oral assessment guide. Oncol. Nurs. Forum 1988, 15, 325–330. [Google Scholar] [PubMed]
- Terezakis, E.; Needleman, I.; Kumar, N.; Moles, D.; Agudo, E. The impact of hospitalization on oral health: A systematic review. J. Clin. Periodontol. 2011, 38, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Özçaka, Ö.; Başoğlu, O.K.; Buduneli, N.; Taşbakan, M.S.; Bacakoğlu, F.; Kinane, D.F. Chlorhexidine decreases the risk of ventilator-associated pneumonia in intensive care unit patients: A randomized clinical trial. J. Periodontal Res. 2012, 47, 584–592. [Google Scholar] [CrossRef]
- Steel, B.J. Oral hygiene and mouth care for older people in acute hospitals: Part 1. Nurs. Older People 2017, 29, 26–31. [Google Scholar] [CrossRef]
- Jang, C.S.; Shin, Y.S. Effects of combination oral care on oral health, dry mouth and salivary pH of intubated patients: A randomized controlled trial. Int. J. Nurs. Pract. 2016, 22, 503–511. [Google Scholar] [CrossRef]
- Özden, D.; Türk, G.; Düger, C.; Güler, E.K.; Tok, F.; Gülsoy, Z. Effects of oral care solutions on mucous membrane integrity and bacterial colonization. Nurs. Crit. Care 2014, 19, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Beck, S. Impact of a systematic oral care protocol on stomatitis after chemotherapy. Cancer Nurs. 1979, 2, 185–199. [Google Scholar] [CrossRef]
- Barnason, S.; Graham, J.; Wild, M.C.; Jensen, L.B.; Rasmussen, D.; Schulz, P.; Woods, S.; Carder, B. Comparison of two endotracheal tube securement techniques on unplanned extubation, oral mucosa, and facial skin integrity. Heart Lung 1998, 27, 409–417. [Google Scholar] [CrossRef]
- Fourrier, F.; Duvivier, B.; Boutigny, H.; Roussel-Delvallez, M.; Chopin, C. Colonization of dental plaque: A source of nosocomial infections in intensive care unit patients. Crit. Care Med. 1998, 26, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, V.; Hallberg, I.R.; Jahnke, H.; Kleiman, C.; Hagell, P. Oral health, ventilator-associated pneumonia, and intracranial pressure in intubated patients in a neuroscience intensive care unit. Am. J. Crit. Care 2009, 18, 368–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, D.; Senior, N.; James, I.; Roberts, G. Oral health status of children in a Paediatric Intensive Care Unit. Intensive Care Med. 2000, 26, 319–324. [Google Scholar] [CrossRef] [PubMed]
- McNally, L.; Gosney, M.A.; Doherty, U.; Field, E.A. The orodental status of a group of elderly in-patients: A preliminary assessment. Gerodontology 1999, 16, 81–84. [Google Scholar] [CrossRef]
- Mersel, A.; Babayof, I.; Rosin, A. Oral health needs of elderly short-term patients in a geriatric department of a general hospital. Spec. Care Dent. 2000, 20, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Ling, G.Y.; Love, R.M.; MacFadyen, E.E.; Thomson, W.M. Oral health of older people admitted to hospital for needs assessment. N. Z. Dent. J. 2014, 110, 131–137. [Google Scholar] [PubMed]
- Gibney, J.M.; Wright, C.; Sharma, A.; D’Souza, M.; Naganathan, V. The oral health status of older patients in acute care on admission and Day 7 in two Australian hospitals. Age Ageing 2017, 46, 852–856. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S68–S77. [Google Scholar] [CrossRef]
- Tablan, O.C.; Anderson, L.J.; Besser, R.; Bridges, C.; Hajjeh, R. Guidelines for preventing health-care-associated pneumonia, 2003: Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR. Recomm. Rep. 2004, 53, 1–36. [Google Scholar]
- Pobo, A.; Lisboa, T.; Rodriguez, A.; Sole, R.; Magret, M.; Trefler, S.; Gómez, F.; Rello, J.; Investigators, R.S. A randomized trial of dental brushing for preventing ventilator-associated pneumonia. Chest 2009, 136, 433–439. [Google Scholar] [CrossRef]
- Carvajal, C.; Pobo, A.; Díaz, E.; Lisboa, T.; Llauradó, M.; Rello, J. Oral hygiene with chlorhexidine on the prevention of ventilator-associated pneumonia in intubated patients: A systematic review of randomized clinical trials. Med. Clin. 2010, 135, 491–497. [Google Scholar] [CrossRef]
- Ikawa, T.; Mizutani, K.; Sudo, T.; Kano, C.; Ikeda, Y.; Akizuki, T.; Kobayashi, H.; Izumi, Y.; Iwata, T. Clinical comparison of an electric-powered ionic toothbrush and a manual toothbrush in plaque reduction: A randomized clinical trial. Int. J. Dent. Hyg. 2021, 19, 93–98. [Google Scholar] [CrossRef]
- Moretti, A.J.; Zhang, S.; Phillips, S.T.; Williams, K.; Moss, K.L.; Offenbacher, S. Evaluation of a Curved Design Rubber Bristle Interdental Cleaner on Patients with Gingivitis. J. Dent. Hyg. 2020, 94, 6–13. [Google Scholar]
- Jansson, M.M.; Syrjälä, H.P.; Ohtonen, P.P.; Meriläinen, M.H.; Kyngäs, H.A.; Ala-Kokko, T.I. Effects of simulation education on oral care practices-a randomized controlled trial. Nurs. Crit. Care 2017, 22, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Haghighi, A.; Shafipour, V.; Bagheri-Nesami, M.; Gholipour Baradari, A.; Yazdani Charati, J. The impact of oral care on oral health status and prevention of ventilator-associated pneumonia in critically ill patients. Aust. Crit. Care 2017, 30, 69–73. [Google Scholar] [CrossRef]
- Kusahara, D.M.; Friedlander, L.T.; Peterlini, M.A.; Pedreira, M.L. Oral care and oropharyngeal and tracheal colonization by Gram-negative pathogens in children. Nurs. Crit. Care 2012, 17, 115–122. [Google Scholar] [CrossRef]
- Akifusa, S.; Isobe, A.; Kibata, K.; Oyama, A.; Oyama, H.; Ariyoshi, W.; Nishihara, T. Comparison of dental plaque reduction after use of electric toothbrushes with and without QLF-D-applied plaque visualization: A 1-week randomized controlled trial. BMC Oral Health 2020, 20, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, M.; Papas, A.; Gerlach, R.W. Safety and effectiveness of a two-step dentifrice/gel sequence with medication-associated hyposalivation: A randomized controlled trial in a vulnerable population. Am. J. Dent. 2018, 31, 24A–28A. [Google Scholar]
- Yao, L.Y.; Chang, C.K.; Maa, S.H.; Wang, C.; Chen, C.C. Brushing teeth with purified water to reduce ventilator-associated pneumonia. J. Nurs. Res. 2011, 19, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, T.; Yoshizawa, K.; Takahashi, K.; Ishida, C.; Komai, K.; Kobayashi, K.; Sugiura, S. Effectiveness of electric toothbrushing in patients with neuromuscular disability: A randomized observer-blind crossover trial. Spec. Care Dent. 2016, 36, 13–17. [Google Scholar] [CrossRef]
- Hayashida, S.; Funahara, M.; Sekino, M.; Yamaguchi, N.; Kosai, K.; Yanamoto, S.; Yanagihara, K.; Umeda, M. The effect of tooth brushing, irrigation, and topical tetracycline administration on the reduction of oral bacteria in mechanically ventilated patients: A preliminary study. BMC Oral Health 2016, 16, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higashiguchi, T.; Ohara, H.; Kamakura, Y.; Kikutani, T.; Kuzuya, M.; Enoki, H.; Sanada, H.; Matsuzaki, M.; Maruyama, M. Efficacy of a New Post-Mouthwash Intervention (Wiping Plus Oral Nutritional Supplements) for Preventing Aspiration Pneumonia in Elderly People: A Multicenter, Randomized, Comparative Trial. Ann. Nutr. Metab. 2017, 71, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Takeyasu, Y.; Yamane, G.Y.; Tonogi, M.; Watanabe, Y.; Nishikubo, S.; Serita, R.; Imura, K. Ventilator-associated pneumonia risk decreased by use of oral moisture gel in oral health care. Bull. Tokyo Dent. Coll. 2014, 55, 95–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Par, M.; Badovinac, A.; Plancak, D. Oral hygiene is an important factor for prevention of ventilator-associated pneumonia. Acta Clin. Croat. 2014, 53, 72–78. [Google Scholar]
- Rabello, F.; Araújo, V.E.; Magalhães, S. Effectiveness of oral chlorhexidine for the prevention of nosocomial pneumonia and ventilator-associated pneumonia in intensive care units: Overview of systematic reviews. Int. J. Dent. Hyg. 2018, 16, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Goss, L.K.; Coty, M.B.; Myers, J.A. A review of documented oral care practices in an intensive care unit. Clin. Nurs. Res. 2011, 20, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.T.; Tang, S.S.; Fu, L.J. The effectiveness of different concentrations of chlorhexidine for prevention of ventilator-associated pneumonia: A meta-analysis. J. Clin. Nurs. 2014, 23, 1461–1475. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.; Owens, M. Does oral care with chlorhexidine reduce ventilator-associated pneumonia in mechanically ventilated adults? Br. J. Nurs. 2019, 28, 682–689. [Google Scholar] [CrossRef]
- Sajjan, P.; Laxminarayan, N.; Kar, P.P.; Sajjanar, M. Chlorhexidine as an antimicrobial agent in dentistry–a review. Oral Health Dent. Manag. 2016, 15, 93–100. [Google Scholar]
- Lorente, L.; Lecuona, M.; Jiménez, A.; Palmero, S.; Pastor, E.; Lafuente, N.; Ramos, M.J.; Mora, M.L.; Sierra, A. Ventilator-associated pneumonia with or without toothbrushing: A randomized controlled trial. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 2621–2629. [Google Scholar] [CrossRef]
- Brookes, Z.L.S.; Bescos, R.; Belfield, L.A.; Ali, K.; Roberts, A. Current uses of chlorhexidine for management of oral disease: A narrative review. J. Dent. 2020, 103, 103497. [Google Scholar] [CrossRef]
- Healthcare Bigdata Hub. Available online: http://opendata.hira.or.kr/op/opc/olapHifrqSickInfo.do (accessed on 13 April 2021).
- Eberhard, J.; Jepsen, S.; Jervøe-Storm, P.M.; Needleman, I.; Worthington, H.V. Full-mouth disinfection for the treatment of adult chronic periodontitis. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef] [Green Version]
- Berry, A.M.; Davidson, P.M.; Masters, J.; Rolls, K.; Ollerton, R. Effects of three approaches to standardized oral hygiene to reduce bacterial colonization and ventilator associated pneumonia in mechanically ventilated patients: A randomised control trial. Int. J. Nurs. Stud. 2011, 48, 681–688. [Google Scholar] [CrossRef]
- Berry, A.M. A comparison of Listerine® and sodium bicarbonate oral cleansing solutions on dental plaque colonisation and incidence of ventilator associated pneumonia in mechanically ventilated patients: A randomised control trial. Intensive Crit. Care Nurs. 2013, 29, 275–281. [Google Scholar] [CrossRef]
- De Lacerda Vidal, C.F.; Vidal, A.K.; Monteiro, J.G., Jr.; Cavalcanti, A.; Henriques, A.P.C.; Oliveira, M.; Godoy, M.; Coutinho, M.; Sobral, P.D.; Vilela, C.; et al. Impact of oral hygiene involving toothbrushing versus chlorhexidine in the prevention of ventilator-associated pneumonia: A randomized study. BMC Infect. Dis. 2017, 17, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhagat, V.; Hoang, H.; Crocombe, L.A.; Goldberg, L.R. Incorporating oral health care education in undergraduate nursing curricula-a systematic review. BMC Nurs. 2020, 19, 66. [Google Scholar] [CrossRef] [PubMed]
- Gambetta-Tessini, K.; Mariño, R.; Ghanim, A.; Adams, G.G.; Manton, D.J. Validation of quantitative light-induced fluorescence-digital in the quantification of demarcated hypomineralized lesions of enamel. J. Investig. Clin. Dent. 2017, 8, e12259. [Google Scholar] [CrossRef]
- Kim, Y.; Jung, H.I.; Kim, Y.K.; Ku, J.K. Histologic analysis of osteonecrosis of the jaw according to the different aspects on quantitative light-induced fluorescence images. Photodiagnosis Photodyn. Ther. 2021, 34, 102212. [Google Scholar] [CrossRef]
- Kim, I.H.; Kim, Y.; Choi, J.; Ku, J.K. The novel application of quantitative light-induced fluorescence to oral mucosal necrosis: A case report with histologic findings. Photodiagnosis Photodyn. Ther. 2020, 31, 101806. [Google Scholar] [CrossRef]
- Roberts, N.; Moule, P. Chlorhexidine and tooth-brushing as prevention strategies in reducing ventilator-associated pneumonia rates. Nurs. Crit. Care 2011, 16, 295–302. [Google Scholar] [CrossRef]
- Khadka, S.; Khan, S.; King, A.; Goldberg, L.R.; Crocombe, L.; Bettiol, S. Poor oral hygiene, oral microorganisms and aspiration pneumonia risk in older people in residential aged care: A systematic review. Age Ageing 2021, 50, 81–87. [Google Scholar] [CrossRef]
- Bellissimo-Rodrigues, W.T.; Menegueti, M.G.; Gaspar, G.G.; Nicolini, E.A.; Auxiliadora-Martins, M.; Basile-Filho, A.; Martinez, R.; Bellissimo-Rodrigues, F. Effectiveness of a dental care intervention in the prevention of lower respiratory tract nosocomial infections among intensive care patients: A randomized clinical trial. Infect. Control. Hosp. Epidemiol. 2014, 35, 1342–1348. [Google Scholar] [CrossRef]
- Hua, F.; Xie, H.; Worthington, H.V.; Furness, S.; Zhang, Q.; Li, C. Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia. Cochrane Database Syst. Rev. 2016, 10, CD008367. [Google Scholar] [CrossRef] [PubMed]
- Chacko, R.; Rajan, A.; Lionel, P.; Thilagavathi, M.; Yadav, B.; Premkumar, J. Oral decontamination techniques and ventilator-associated pneumonia. Br. J. Nurs. 2017, 26, 594–599. [Google Scholar] [CrossRef]
- Vilela, M.C.; Ferreira, G.Z.; Santos, P.S.; Rezende, N.P. Oral care and nosocomial pneumonia: A systematic review. Einstein 2015, 13, 290–296. [Google Scholar] [CrossRef] [Green Version]
- Malhan, N.; Usman, M.; Trehan, N.; Sinha, A.; Settecase, V.A.; Fried, A.D.; Kupfer, Y.Y.; Kamholz, S.L. Oral Care and Ventilator-Associated Pneumonia. Am. J. Ther. 2019, 26, e604–e607. [Google Scholar] [CrossRef]
- Zuckerman, L.M. Oral Chlorhexidine Use to Prevent Ventilator-Associated Pneumonia in Adults: Review of the Current Literature. Dimens. Crit. Care Nurs. 2016, 35, 25–36. [Google Scholar] [CrossRef]
- Kaneoka, A.; Pisegna, J.M.; Miloro, K.V.; Lo, M.; Saito, H.; Riquelme, L.F.; LaValley, M.P.; Langmore, S.E. Prevention of Healthcare-Associated Pneumonia with Oral Care in Individuals Without Mechanical Ventilation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Infect. Control. Hosp. Epidemiol. 2015, 36, 899–906. [Google Scholar] [CrossRef]
- El-Rabbany, M.; Zaghlol, N.; Bhandari, M.; Azarpazhooh, A. Prophylactic oral health procedures to prevent hospital-acquired and ventilator-associated pneumonia: A systematic review. Int. J. Nurs. Stud. 2015, 52, 452–464. [Google Scholar] [CrossRef]
- Dale, C.; Angus, J.E.; Sinuff, T.; Mykhalovskiy, E. Mouth care for orally intubated patients: A critical ethnographic review of the nursing literature. Intensive Crit. Care Nurs. 2013, 29, 266–274. [Google Scholar] [CrossRef]
- Gu, W.J.; Gong, Y.Z.; Pan, L.; Ni, Y.X.; Liu, J.C. Impact of oral care with versus without toothbrushing on the prevention of ventilator-associated pneumonia: A systematic review and meta-analysis of randomized controlled trials. Critical Care 2012, 16, R190. [Google Scholar] [CrossRef] [Green Version]
- Tada, A.; Miura, H. Prevention of aspiration pneumonia (AP) with oral care. Arch. Gerontol. Geriatr. 2012, 55, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Sjögren, P.; Wårdh, I.; Zimmerman, M.; Almståhl, A.; Wikström, M. Oral Care and Mortality in Older Adults with Pneumonia in Hospitals or Nursing Homes: Systematic Review and Meta-Analysis. J. Am. Geriatr. Soc. 2016, 64, 2109–2115. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, B.F.; Gonzalez, L.P.; Calvo, M.C.; Sanchez, F.C.; Alonso, C.R.P.; de Alba Romero, C. Oral care in a neonatal intensive care unit. J. Matern. Fetal Neonatal Med. 2017, 30, 953–957. [Google Scholar] [CrossRef] [PubMed]
- Izumi, M.; Takeuchi, K.; Ganaha, S.; Akifusa, S.; Yamashita, Y. Effects of oral care with tongue cleaning on coughing ability in geriatric care facilities: A randomised controlled trial. J. Oral Rehabil. 2016, 43, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Szabo, C.M. The effect of oral care on intracranial pressure: A review of the literature. J. Neurosci. Nurs. 2011, 43, E1–E9. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, L.; Weir, W.I.; Gregori, D.; Taylor, N.; Zandstra, D.F.; van Saene, J.J.M.; van Saene, H.K.F. Impact of Oral Chlorhexidine on Bloodstream Infection in Critically Ill Patients: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Cardiothorac. Vasc. Anesth. 2017, 31, 2236–2244. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Articles/Types | Subject Information | Index | Average Results | |
|---|---|---|---|---|
| [20]/Review | [27] | Plaque index | At ICU stay day 0: 23% After 10 days: 93% | |
| [28,29] | Gingivitis | Significantly increased | ||
| [21]/Original | Before intervention (n = 66) | No. of teeth lost | 14.3 ± 8.3 | |
| Probing depth | 3.8 ± 1.0 mm | |||
| Plaque index | 85.6 ± 20.5% | |||
| Bleeding on probing | 48.6 ± 29.7% | |||
| [22]/Review | [30] | Patients from England (n= 150) | Need for dental operative intervention | 75% |
| Denture-related candidiasis | 38% | |||
| Dental examination within 1 year | 15% | |||
| [31] | Patients from Israel (n = 225) | Needs of direct dental treatment | 65% | |
| Pseudomembranous candidiasis | 56% | |||
| [32] | Patients from New Zealand (n = 200) | Need for periodontal intervention | 90% | |
| Need for fillings or extractions | 71% | |||
| Carious teeth | 1.9 | |||
| [33] | Patients from Australia (n = 575) | Unhealthy oral condition | 76% | |
| Poor oral hygiene | 38% | |||
| [5]/Original | Hospitalization within 7 days (n = 254) | Gingivitis | 54.8% | |
| Complete edentulism | 38.2% | |||
| Periodontitis | 29.5% | |||
| Dental caries | 29.1% | |||
| Tooth fracture (residual roots) | 17.0% | |||
| Mucositis | 6.3% | |||
| Oral candidiasis | 1.6% | |||
| Odontogenic abscess | 0.8% | |||
| Not Recommended | |
|---|---|
| Hydrogen peroxide | Irritable, unpleasant taste, and genotoxic |
| Sodium bicarbonate | Irritation and chemical burns caused by high pH |
| Topical antibiotics | Changes in the microflora in the oral cavity, unable act against all bacteria that can cause VAP, and risk of developing resistance |
| Citric acid and glycerin | Can temporarily relieve dry mouth but cause hard tissue demineralization because of low pH |
| Povidone-iodine | Not effective in reducing plaque and toxic |
| Recommended | |
| Chlorhexidine | Effective in VAP prevention and plaque control at 0.12–0.2% concentration |
| Artificial saliva | Beneficial for moisturizing mucosa and maintaining physiological oral flora |
| Vaseline | Beneficial for moisturizing mucosa and maintaining physiological oral flora |
| Mechanical plaque control | The most basic and efficient method, a toothbrush is better than a cotton swab, and tooth brushing with toothpaste is more effective |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jun, M.-K.; Ku, J.-K.; Kim, I.-h.; Park, S.-Y.; Hong, J.; Kim, J.-Y.; Lee, J.-K. Hospital Dentistry for Intensive Care Unit Patients: A Comprehensive Review. J. Clin. Med. 2021, 10, 3681. https://doi.org/10.3390/jcm10163681
Jun M-K, Ku J-K, Kim I-h, Park S-Y, Hong J, Kim J-Y, Lee J-K. Hospital Dentistry for Intensive Care Unit Patients: A Comprehensive Review. Journal of Clinical Medicine. 2021; 10(16):3681. https://doi.org/10.3390/jcm10163681
Chicago/Turabian StyleJun, Mi-Kyoung, Jeong-Kui Ku, Il-hyung Kim, Sang-Yoon Park, Jinson Hong, Jae-Young Kim, and Jeong-Keun Lee. 2021. "Hospital Dentistry for Intensive Care Unit Patients: A Comprehensive Review" Journal of Clinical Medicine 10, no. 16: 3681. https://doi.org/10.3390/jcm10163681
APA StyleJun, M. -K., Ku, J. -K., Kim, I. -h., Park, S. -Y., Hong, J., Kim, J. -Y., & Lee, J. -K. (2021). Hospital Dentistry for Intensive Care Unit Patients: A Comprehensive Review. Journal of Clinical Medicine, 10(16), 3681. https://doi.org/10.3390/jcm10163681