
Promising Mid-Term Outcomes after Humeral Head Preserving Surgery of Posterior Fracture Dislocations of the Proximal Humerus

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection Criteria
- Impression fractures of the humeral head (29%)
- (Multifragmentary) surgical neck fractures (18.5%)
- Fractures of the lesser tuberosity (14.3%)
- Fractures of the greater tuberosity (7.8%)
- Other fractures (6%)
- Previous injuries or surgery to the affected shoulder
- Immunosuppressive therapy
- Drug or alcohol abuse
- Patients treated more than three weeks after trauma
- Patients that were treated with arthroplasty (n = 11)
- Patients that had died by the time the follow-up was conducted (n = 6)
2.2. Retrospective Analysis
2.3. Follow-Up Examination
2.4. Surgical Technique
2.5. Statistical Analysis
3. Results
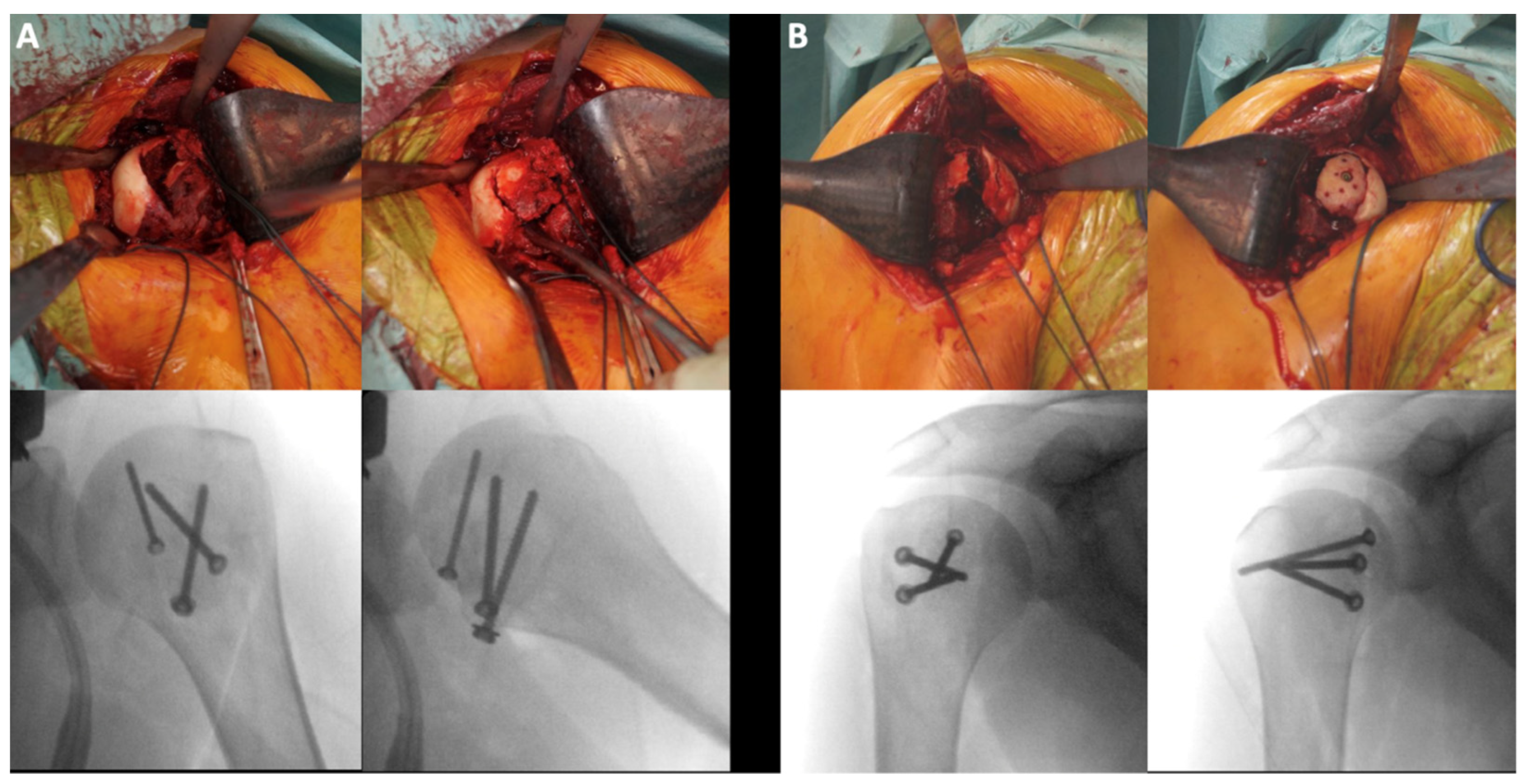
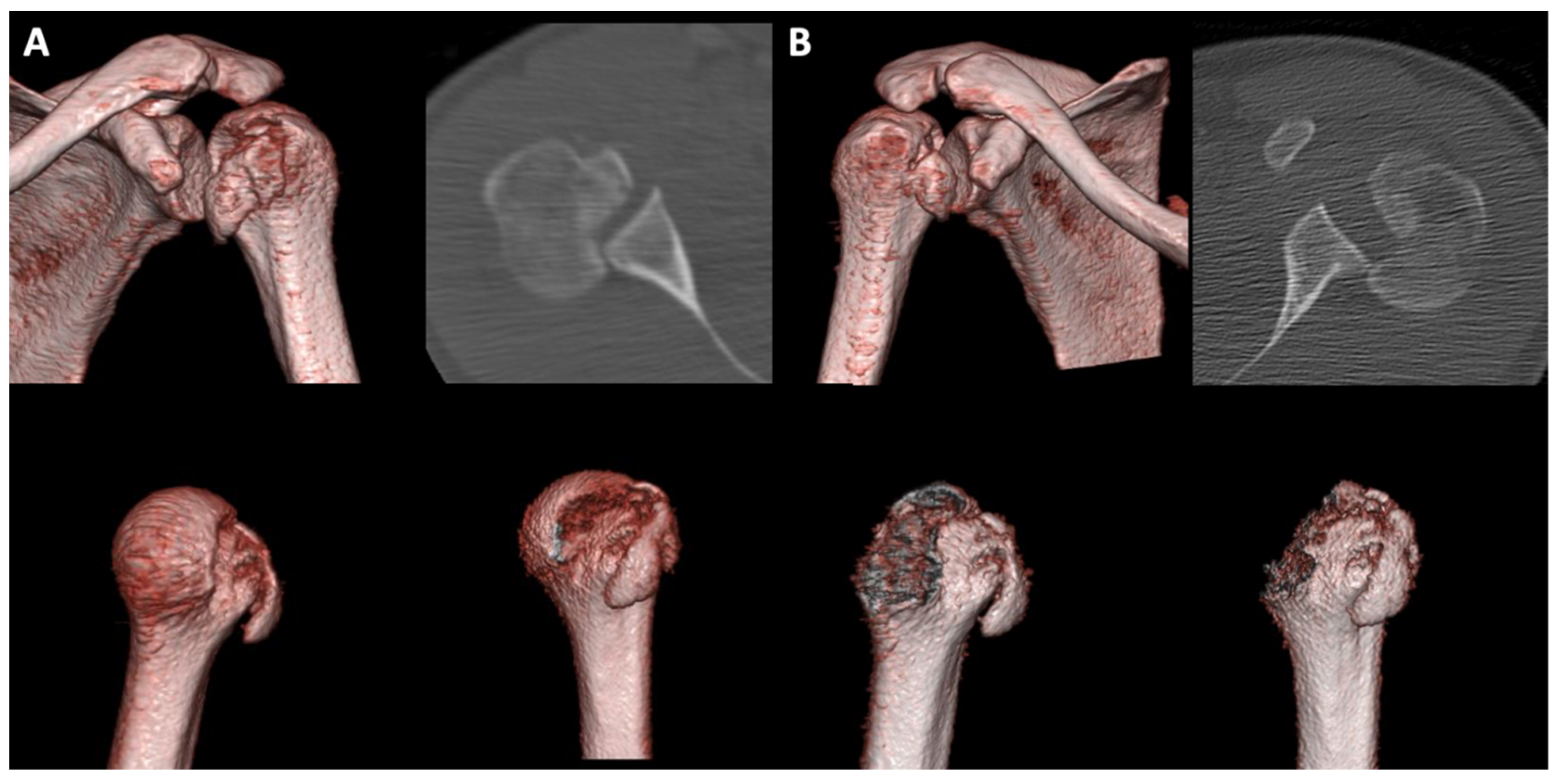
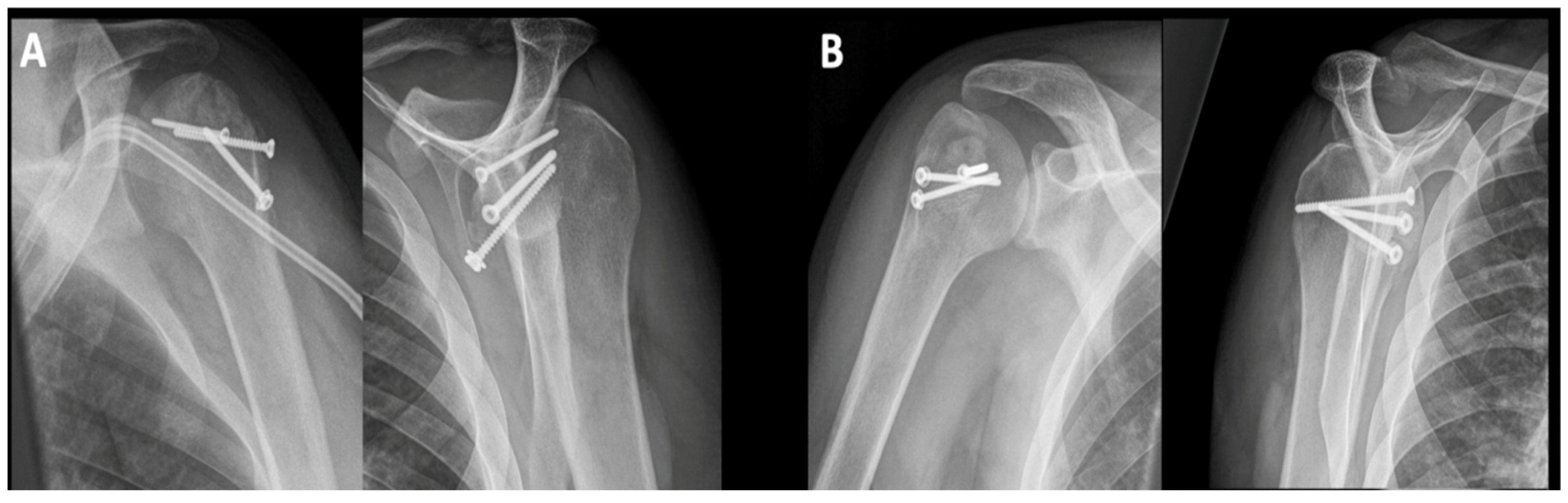
3.1. Impression Type Fractures (ITFs)
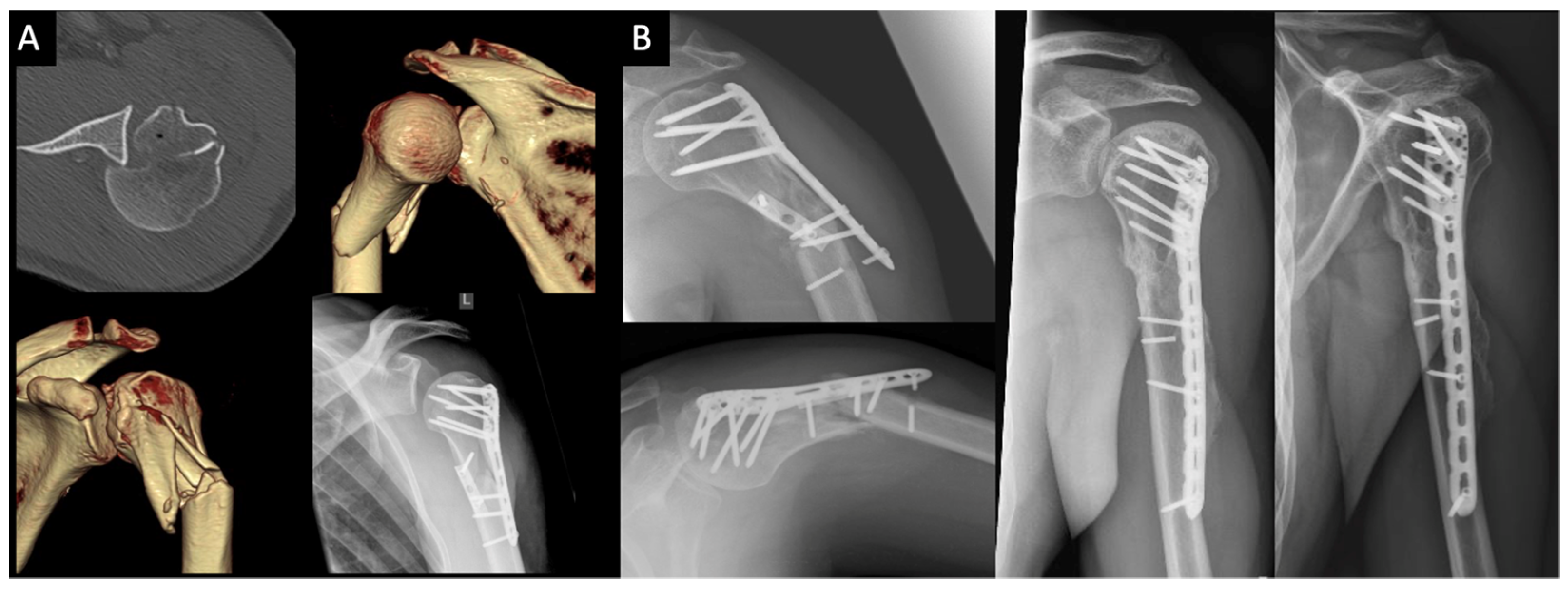
3.2. Surgical Neck Fractures of the Humerus (SNFs)
3.3. Revision Surgery & Complications
3.4. Range of Motion and Functional Scores
4. Discussion
4.1. Surgical Treatment Options
4.2. Clinical Outcome
4.3. Engagement of Bone Defects
4.4. Save the Humeral Head or Replace It?
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Passaretti, D.; Candela, V.; Sessa, P.; Gumina, S. Epidemiology of proximal humeral fractures: A detailed survey of 711 patients in a metropolitan area. J. Shoulder Elb. Surg. 2017, 26, 2117–2124. [Google Scholar] [CrossRef]
- Palvanen, M.; Kannus, P.; Niemi, S.; Parkkari, J. Update in the epidemiology of proximal humeral fractures. Clin. Orthop. Relat. R 2006, 442, 87–92. [Google Scholar] [CrossRef]
- Trikha, V.; Singh, V.; Choudhury, B.; Das, S. Retrospective analysis of proximal humeral fracture-dislocations managed with locked plates. J. Shoulder Elb. Surg. 2017, 26, e293–e299. [Google Scholar] [CrossRef] [PubMed]
- Alkaduhimi, H.; van der Linde, J.A.; Flipsen, M.; van Deurzen, D.F.P.; van den Bekerom, M.P.J. A systematic and technical guide on how to reduce a shoulder dislocation. Turk. J. Emerg. Med. 2016, 16, 155–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, C.M.; Akhtar, A.; Mitchell, M.; Beavis, C. Complex posterior fracture-dislocation of the shoulder. J. Bone Jt. Surg. 2007, 89, 1454–1466. [Google Scholar] [CrossRef]
- Kokkalis, Z.T.; Iliopoulos, I.D.; Antoniou, G.; Antoniadou, T.; Mavrogenis, A.F.; Panagiotopoulos, E. Posterior shoulder fracture–dislocation: An update with treatment algorithm. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 285–294. [Google Scholar] [CrossRef]
- Neer, C.S.; Foster, C.R. Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder. A preliminary report. J. Bone Jt. Surg. 1980, 62, 897–908. [Google Scholar] [CrossRef]
- Rouleau, D.M.; Hebert-Davies, J. Incidence of associated injury in posterior shoulder dislocation. J. Orthop. Trauma 2012, 26, 246–251. [Google Scholar] [CrossRef]
- Sandmann, G.H.; Siebenlist, S.; Imhoff, F.B.; Ahrens, P.; Neumaier, M.; Freude, T.; Biberthaler, P. Balloon-guided inflation osteoplasty in the treatment of Hill-Sachs lesions of the humeral head: Case report of a new technique. Patient Saf. Surg. 2016, 10, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yigit, M.; Yaman, A.; Yigit, E.; Turkdogan, K.A. The overlooked side of convulsion: Bilateral posterior fracture and dislocation of proximal humerus. JPMA J. Pak. Med. Assoc. 2016, 66, 621–622. [Google Scholar]
- Heilmann, L.F.; Katthagen, J.C.; Raschke, M.J.; Lill, H.; Schliemann, B.; Bajjati, H.E.; Jensen, G.; Dey-Hazra, R.O. Posterior fracture dislocation of the proximal humerus. Obere Extrem. 2019, 14, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Boyle, M.J.; Youn, S.-M.; Frampton, C.M.A.; Ball, C.M. Functional outcomes of reverse shoulder arthroplasty compared with hemiar-throplasty for acute proximal humeral fractures. J. Shoulder Elb. Surg. 2013, 22, 32–37. [Google Scholar] [CrossRef]
- Resch, H.; Tauber, M.; Neviaser, R.J.; Neviaser, A.S.; Majed, A.; Halsey, T.; Hirzinger, C.; Al-Yassari, G.; Zyto, K.; Moroder, P. Classification of proximal humeral fractures based on a pathomorphologic analysis. J Shoulder Elb Surg. 2016, 25, 455–462. [Google Scholar] [CrossRef]
- Neer, C.S. Displaced fractures of the proximal humerus. Clin. Orthop. Relat. R 1971, 81, 183–184. [Google Scholar] [CrossRef]
- Guix, J.M.M.; Pedrós, J.S.; Serrano, A.C. Updated classification system for proximal humeral fractures. Clin. Med. Res. 2009, 7, 32–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moroder, P.; Runer, A.; Kraemer, M.; Fierlbeck, J.; Niederberger, A.; Cotofana, S.; Vasvari, I.; Hettegger, B.; Tauber, M.; Hurschler, C.; et al. Influence of defect size and localization on the engagement of reverse hill-sachs lesions. Am. J. Sports Med. 2015, 43, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Katolik, L.I.; Romeo, A.A.; Cole, B.J.; Verma, N.N.; Hayden, J.K.; Bach, B.R. Normalization of the constant score. J. Shoulder Elb. Surg. 2005, 14, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Rodia, F.; Ventura, A.; Touloupakis, G.; Theodorakis, E.; Ceretti, M. Missed posterior shoulder dislocation and McLaughlin lesion after an electrocution accident. Chin. J. Traumatol./Zhonghua Chuang Shang Za Zhi 2012, 15, 376–378. [Google Scholar] [PubMed]
- Warnhoff, M.; Jensen, G.; Dey Hazra, R.O.; Theruvath, P.; Lill, H.; Ellwein, A. Double plating—Surgical technique and good clinical results in complex and highly unstable proximal humeral fractures. Injury 2021, 52, 2285–2291. [Google Scholar] [CrossRef]
- Katthagen, J.C.; Lutz, O.; Voigt, C.; Lill, H.; Ellwein, A. Cement augmentation of humeral head screws reduces early implant-related complications after locked plating of proximal humeral fractures. Obere Extrem. 2018, 13, 123–129. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira, C.T.B.; da Graça, E.; Fanelli, V.A. Posterior four-part fracture-dislocations of the proximal humerus: Clinical and func-tional evaluation of osteosynthesis treatment. Rev. Bras. Ortop. Engl. Ed. 2018, 53, 350–356. [Google Scholar] [CrossRef]
- Johnson, N.; Pandey, R. Proximal humerus fracture–dislocation managed by mini-open reduction and percutaneous screw fixa-tion. Shoulder Elb. 2018, 11, 353–358. [Google Scholar] [CrossRef]
- Luigi, B.V.; Stefano, L.; Mauro, M. Locked posterior fracture-dislocation of the shoulder. Acta BioMed. Atenei Parm. 2020, 90, 139–146. [Google Scholar]
- Gerber, C.; Catanzaro, S.; Jundt-Ecker, M.; Farshad, M. Long-term outcome of segmental reconstruction of the humeral head for the treatment of locked posterior dislocation of the shoulder. J. Shoulder Elb. Surg. 2014, 23, 1682–1690. [Google Scholar] [CrossRef] [PubMed]
- Kukkonen, J.; Kauko, T.; Vahlberg, T.; Joukainen, A.; Äärimaa, V. Investigating minimal clinically important difference for Constant score in patients undergoing rotator cuff surgery. J. Shoulder Elb. Surg. 2013, 22, 1650–1655. [Google Scholar] [CrossRef] [PubMed]
- Robinson, C.M.; Stirling, P.H.C.; Goudie, E.B.; MacDonald, D.J.; Strelzow, J.A. Complications and long-term outcomes of open re-duction and plate fixation of proximal humeral fractures. J. Bone Jt. Surg. 2019, 101, 2129–2139. [Google Scholar] [CrossRef]
- Schliemann, B.; Muder, D.; Geßmann, J.; Schildhauer, T.A.; Seybold, D. Locked posterior shoulder dislocation: Treatment options and clinical outcomes. Arch. Orthop. Trauma Surg. 2011, 131, 1127–1134. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rating | Forward Flexion | Abduction |
|---|---|---|
| Excellent | 151–180° | 151–180° |
| Very good | 121–150° | 121–150° |
| Good | 91–120° | 91–120° |
| Fair | 61–90° | 61–90° |
| Bad | 31–60° | 31–60° |
| Very Bad | 0–30° | 0–30° |
| Pat. ID | Age | Gender | Fracture | Treatment | TFU (y) Follow-Up (y) |
|---|---|---|---|---|---|
| 1 | 43 | M | ITF | Allo- and autograft | 7.6 |
| 2 | 31 | W | ITF | Allograft | 7.6 |
| 3 | 48 | M | ITF | SPO, 1x screw | 5.4 |
| 4 | 28 | M | ITF | Allograft, 6x screw | 2.4 |
| 5 | 33 | M | ITF | Allo- and autograft, 3x screw | 2.8 |
| 6 | 33 | M | ITF | Allo- and autograft, 3x screw | 2.8 |
| 7 | 27 | W | ITF | Allograft | 3.3 |
| 8 | 47 | M | ITF | Allograft | 3.4 |
| 9 | 47 | M | ITF | Mod. McLaughlin procedure, 3x screw | 4.6 |
| 10 | 29 | M | ITF | Autograft, 2x screw | 4.6 |
| 11 | 45 | M | ITF | Allo- and autograft, 3x screw | 4.3 |
| 12 | 35 | M | ITF | Autograft, 2x screw | 8.4 |
| 13 | 39 | M | SNF | DPO | 5.9 |
| 14 | 48 | W | SNF | DPO | 2.7 |
| 15 | 68 | M | SNF | Allo- and autograft, 2x screw, SPO | 2.2 |
| 16 | 47 | M | SNF | 2x screw, SPO | 2.3 |
| 17 | 45 | M | SNF | Autograft, 2x screw | 4.2 |
| 18 | 60 | W | SNF | SPO, 2x screw | 2.5 |
| 19 | 58 | M | SNF | Autograft, SPO, 1x screw | 2.1 |
| ITF (n = 12), Mean | SNF (n = 7), Mean | p-Value | |
|---|---|---|---|
| Forward Flexion | 172° (160–184°) | 118° (65–172°) | 0.421 |
| Abduction | 172° (160–184°) | 115° (60–171°) | 0.421 |
| External Rotation | 69° (60–77°) | 38° (19–57°) | 0.084 |
| Head/shaft-angle | 124.3° (121–127°) | 120.9° (112–130°) | >0.999 |
| CS | 92 (84–99) | 75 (55–93) | 0.099 |
| SST | 100% (100–100%) | 80% (53–100%) | 0.003 * |
| SSV | 91% (85–98%) | 83% (68–98%) | 0.421 |
| Rowe | 97 (92–100) | 88 (78–97) | 0.013 * |
| WOSI | 11 (2–19) | 34 (18–51) | 0.023 * |
| ASES | 96 (92–100) | 85 (68–100) | 0.041 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heilmann, L.F.; Katthagen, J.C.; Raschke, M.J.; Schliemann, B.; Lill, H.; El Bajjati, H.; Jensen, G.; Dey Hazra, R.-O. Promising Mid-Term Outcomes after Humeral Head Preserving Surgery of Posterior Fracture Dislocations of the Proximal Humerus. J. Clin. Med. 2021, 10, 3841. https://doi.org/10.3390/jcm10173841
Heilmann LF, Katthagen JC, Raschke MJ, Schliemann B, Lill H, El Bajjati H, Jensen G, Dey Hazra R-O. Promising Mid-Term Outcomes after Humeral Head Preserving Surgery of Posterior Fracture Dislocations of the Proximal Humerus. Journal of Clinical Medicine. 2021; 10(17):3841. https://doi.org/10.3390/jcm10173841
Chicago/Turabian StyleHeilmann, Lukas F., J. Christoph Katthagen, Michael J. Raschke, Benedikt Schliemann, Helmut Lill, Hassan El Bajjati, Gunnar Jensen, and Rony-Orijit Dey Hazra. 2021. "Promising Mid-Term Outcomes after Humeral Head Preserving Surgery of Posterior Fracture Dislocations of the Proximal Humerus" Journal of Clinical Medicine 10, no. 17: 3841. https://doi.org/10.3390/jcm10173841
APA StyleHeilmann, L. F., Katthagen, J. C., Raschke, M. J., Schliemann, B., Lill, H., El Bajjati, H., Jensen, G., & Dey Hazra, R. -O. (2021). Promising Mid-Term Outcomes after Humeral Head Preserving Surgery of Posterior Fracture Dislocations of the Proximal Humerus. Journal of Clinical Medicine, 10(17), 3841. https://doi.org/10.3390/jcm10173841