
Effects of Clonidine as an Adjuvant to Lidocaine with Epinephrine in Ultrasound Guided Axillary Brachial Plexus Block: A Randomised Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
Sample Size and Statistical Analysis
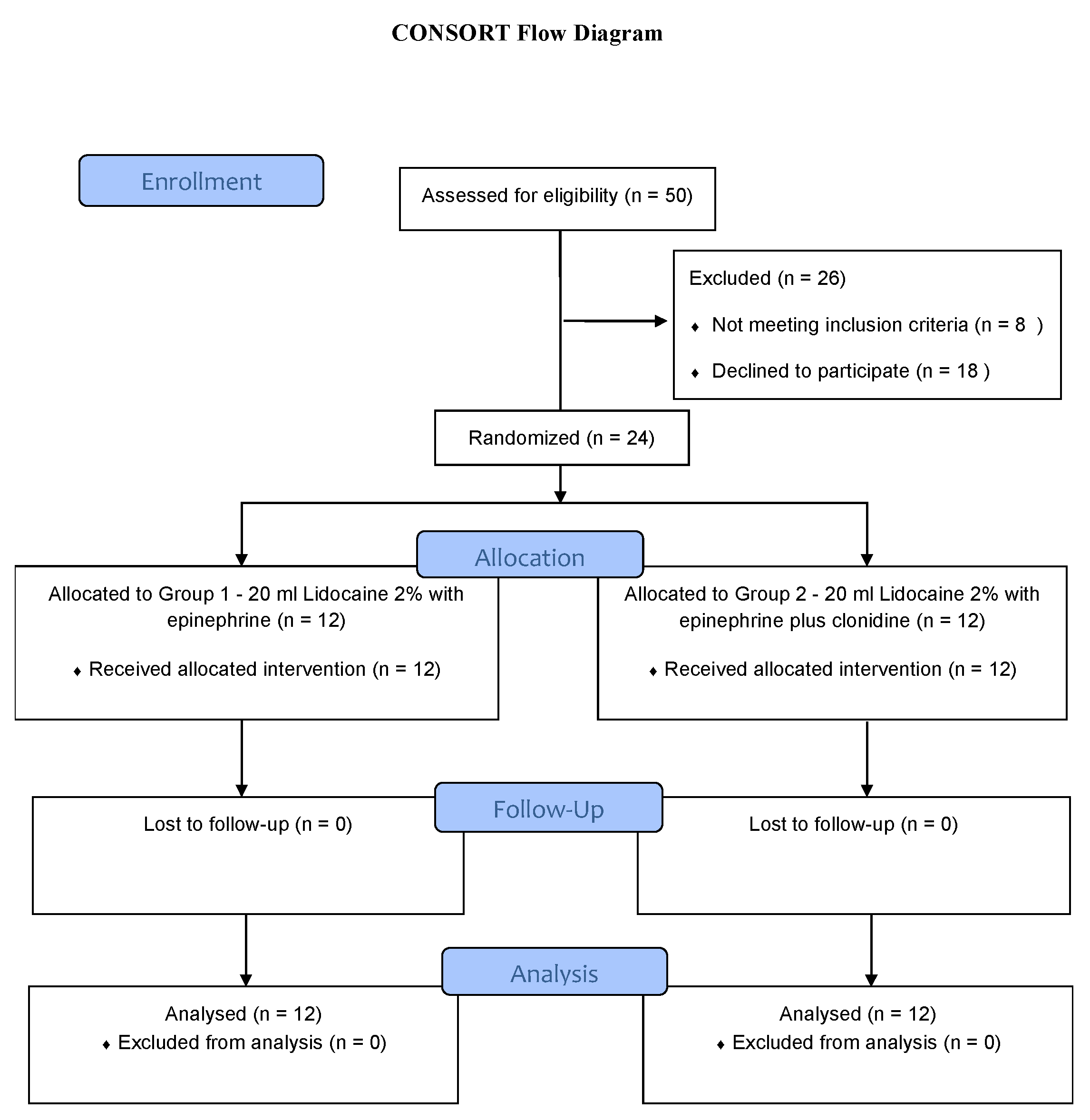
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bazin, J.E.; Massoni, C.; Bruelle, P.; Fenies, V.; Groslier, D.; Schoeffler, P. The addition of opioids to local anaesthetics in brachial plexus block: The comparative effects of morphine, buprenorphine and sufentanil. Anaesthesia 1997, 52, 858–862. [Google Scholar] [CrossRef]
- Candido, K.D.; Winnie, A.P.; Ghaleb, A.H.; Fattouh, M.W.; Franco, C.D. Buprenorphine added to the local anesthetic for axillary brachial plexus block prolongs postoperative analgesia. Reg. Anesth. Pain Med. 2002, 27, 162–167. [Google Scholar] [CrossRef]
- Dogru, K.; Duygulu, F.; Yildiz, K.; Kotanoglu, M.S.; Madenoglu, H.; Boyaci, A. Hemodynamic and blockade effects of high/low epinephrine doses during axillary brachial plexus blockade with lidocaine 1.5%: A randomized, double-blinded study. Reg. Anesth. Pain Med. 2003, 28, 401–405. [Google Scholar] [CrossRef]
- Iskandar, H.; Guillaume, E.; Dixmérias, F.; Binje, B.; Rakotondriamihary, S.; Thiebaut, R.; Maurette, P. The enhancement of sensory blockade by clonidine selectively added to mepivacaine after midhumeral block. Anesth. Analg. 2001, 93, 771–775. [Google Scholar] [CrossRef] [PubMed]
- Patacsil, J.A.; McAuliffe, M.S.; Feyh, L.S.; Sigmon, L.L. Local Anesthetic Adjuvants Providing the Longest Duration of Analgesia for Single- Injection Peripheral Nerve Blocks in Orthopedic Surgery: A Literature Review. AANA J. 2016, 84, 95–103. [Google Scholar] [PubMed]
- Prabhakar, A.; Lambert, T.; Kaye, R.J.; Gaignard, S.M.; Ragusa, J.; Wheat, S.; Moll, V.; Cornett, E.M.; Urman, R.D.; Kaye, A.D. Adjuvants in clinical regional anesthesia practice: A comprehensive review. Best Pract. Res. Clin. Anaesthesiol. 2019, 33, 415–423. [Google Scholar] [CrossRef]
- El-Boghdadly, K.; Brull, R.; Sehmbi, H.; Abdallah, F.W. Perineural Dexmedetomidine Is More Effective Than Clonidine When Added to Local Anesthetic for Supraclavicular Brachial Plexus Block: A Systematic Review and Meta-analysis. Anesth. Analg. 2017, 124, 2008–2020. [Google Scholar] [CrossRef]
- Vorobeichik, L.; Brull, R.; Abdallah, F.W. Evidence basis for using perineural dexmedetomidine to enhance the quality of brachial plexus nerve blocks: A systematic review and meta-analysis of randomized controlled trials. Br. J. Anaesth. 2017, 118, 167–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chawda, P.M.; Sharma, G. A clinical study comparing epinephrine 200 μg or clonidine 90 μg as adjuvants to local anaesthetic agent in brachial plexus block via supraclavicular approach. J. Anaesthesiol. Clin. Pharmacol. 2010, 26, 523–527. [Google Scholar] [PubMed]
- Bernard, J.M.; Macaire, P. Dose-range effects of clonidine added to lidocaine for brachial plexus block. Anesthesiology 1997, 87, 277–284. [Google Scholar] [CrossRef]
- Iohom, G.; Machmachi, A.; Diarra, D.P.; Khatouf, M.; Boileau, S.; Dap, F.; Boini, S.; Mertes, P.-M.; Bouaziz, H. The effects of clonidine added to mepivacaine for paronychia surgery under axillary brachial plexus block. Anesth. Analg. 2005, 100, 1179–1183. [Google Scholar] [CrossRef] [PubMed]
- Antonucci, S. Adiuvants in the axillary brachial plexus blockade. Comparison between clonidine, sufentanil and tramadol. Minerva Anestesiol. 2001, 67, 23–27. [Google Scholar] [PubMed]
- Erlacher, W.; Schuschnig, C.; Koinig, H.; Marhofer, P.; Melischek, M.; Mayer, N.; Kapral, S. Clonidine as adjuvant for mepivacaine, ropivacaine and bupivacaine in axillary, perivascular brachial plexus block. Can. J. Anaesth. J. Can. D’anesthesie 2001, 48, 522–525. [Google Scholar] [CrossRef] [PubMed]
- Singelyn, F.J.; Gouverneur, J.M.; Robert, A. A minimum dose of clonidine added to mepivacaine prolongs the duration of anesthesia and analgesia after axillary brachial plexus block. Anesth. Analg. 1996, 83, 1046–1050. [Google Scholar] [CrossRef] [PubMed]
- Eledjam, J.J.; Deschodt, J.; Viel, E.J.; Lubrano, J.F.; Charavel, P.; d’Athis, F.; Du Cailar, J. Brachial plexus block with bupivacaine: Effects of added alpha-adrenergic agonists: Comparison between clonidine and epinephrine. Can. J. Anaesth. J. Can. D’anesthesie 1991, 38, 870–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaumann, D.; Forster, A.; Griessen, M.; Habre, W.; Poinsot, O.; Della Santa, D. Comparison between clonidine and epinephrine admixture to lidocaine in brachial plexus block. Anesth. Analg. 1992, 75, 69–74. [Google Scholar] [CrossRef]
- Erlacher, W.; Schuschnig, C.; Orlicek, F.; Marhofer, P.; Koinig, H.; Kapral, S. The effects of clonidine on ropivacaine 0.75% in axillary perivascular brachial plexus block. Acta Anaesthesiol. Scand. 2000, 44, 53–57. [Google Scholar] [CrossRef]
- O’Donnell, B.D.; Iohom, G. An estimation of the minimum effective anesthetic volume of 2% lidocaine in ultrasound-guided axillary brachial plexus block. Anesthesiology 2009, 111, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Kaabachi, O.; Ouezini, R.; Koubaa, W.; Ghrab, B.; Zargouni, A.; Ben Abdelaziz, A. Tramadol as an adjuvant to lidocaine for axillary brachial plexus block. Anesth. Analg. 2009, 108, 367–370. [Google Scholar] [CrossRef]
- Murphy, D.B.; McCartney, C.J.; Chan, V.W. Novel analgesic adjuncts for brachial plexus block: A systematic review. Anesth. Analg. 2000, 90, 1122–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCartney, C.J.; Duggan, E.; Apatu, E. Should we add clonidine to local anesthetic for peripheral nerve blockade? A qualitative systematic review of the literature. Reg. Anesth. Pain Med. 2007, 32, 330–338. [Google Scholar] [CrossRef]
- Hrishi, A.P.; Rao, G.; Lionel, K.R. Efficacy of Clonidine as an Additive on the Duration of Action of Brachial Plexus Block Performed Under Ultrasound and Nerve Locator Guidance: A Prospective Randomized Study. Anesth. Essays Res. 2019, 13, 105–110. [Google Scholar]
- Singelyn, F.J.; Dangoisse, M.; Bartholomée, S.; Gouverneur, J.M. Adding clonidine to mepivacaine prolongs the duration of anesthesia and analgesia after axillary brachial plexus block. Reg. Anesth. 1992, 17, 148–150. [Google Scholar]
- Hutschala, D.; Mascher, H.; Schmetterer, L.; Klimscha, W.; Fleck, T.; Eichler, H.G.; Tschernko, E.M. Clonidine added to bupivacaine enhances and prolongs analgesia after brachial plexus block via a local mechanism in healthy volunteers. Eur. J. Anaesthesiol. 2004, 21, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Maze, M.; Tranquilli, W. Alpha-2 adrenoceptor agonists: Defining the role in clinical anesthesia. Anesthesiology 1991, 74, 581–605. [Google Scholar] [CrossRef]
- Matthews, W.D.; Jim, K.F.; Hieble, J.P.; DeMarinis, R.M. Postsynaptic alpha adrenoceptors on vascular smooth muscle. Fed. Proc. 1984, 43, 2923–2928. [Google Scholar]
- Langer, S.Z.; Duval, N.; Massingham, R. Pharmacologic and therapeutic significance of alpha-adrenoceptor subtypes. J. Cardiovasc. Pharmacol. 1985, 7 (Suppl. 8), S1–S8. [Google Scholar]
- Molnar, R.R.; Davies, M.J.; Scott, D.A.; Silbert, B.S.; Mooney, P.H. Comparison of clonidine and epinephrine in lidocaine for cervical plexus block. Reg. Anesth. 1997, 22, 137–142. [Google Scholar] [PubMed]
- Gaumann, D.M.; Brunet, P.C.; Jirounek, P. Clonidine enhances the effects of lidocaine on C-fiber action potential. Anesth. Analg. 1992, 74, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Butterworth, J.F.; Strichartz, G.R. The alpha 2-adrenergic agonists clonidine and guanfacine produce tonic and phasic block of conduction in rat sciatic nerve fibers. Anesth. Analg. 1993, 76, 295–301. [Google Scholar]
- Kroin, J.S.; Buvanendran, A.; Beck, D.R.; Topic, J.E.; Watts, D.E.; Tuman, K.J. Clonidine prolongation of lidocaine analgesia after sciatic nerve block in rats Is mediated via the hyperpolarization-activated cation current, not by alpha-adrenoreceptors. Anesthesiology 2004, 101, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Sia, S.; Lepri, A. Clonidine administered as an axillary block does not affect postoperative pain when given as the sole analgesic. Anesth. Analg. 1999, 88, 1109–1112. [Google Scholar] [PubMed]
- Kopacz, D.J.; Bernards, C.M. Effect of clonidine on lidocaine clearance in vivo: A microdialysis study in humans. Anesthesiology 2001, 95, 1371–1376. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Motor Test | Sensory Test | |
|---|---|---|
| Median | Flexion of radial 3 fingers | Thenar eminence |
| Radial | Extension of wrist | Dorsum of hand |
| Ulnar | Abduction of fingers | Hypothenar eminence |
| Musculocutaneous | Elbow flexion | Over base first metacarpal |
| Modified Bromage Scale Score and definition 4 Full power in relevant muscle. 3 Reduced power but ability to move muscle against resistance 2 Ability to move relevant muscle group against gravity but not against resistance 1 Flicker of movement in relevant muscle group 0 No movement in relevant muscle group | ||
| Group 1 n = 12 | Group 2 n = 12 | p Value | |
|---|---|---|---|
| Age, y | 41.4 ± 10.6 | 42.3 ± 8.6 | 0.82 |
| Sex, M/F, | 7/5 | 8/4 | 0.67 |
| BMI, Kg/m2 | 25.8 ± 1.8 | 25.7 ± 2.0 | 0.98 |
| ASA grade (I/II/III), n | 9/3/0 | 7/5/0 | 0.39 |
| Duration of surgery, min | 63.9 ± 15.9 | 61.8 ± 15.4 | 0.74 |
| Site of surgery (Forearm, wrist, hand), n | 0/10/2 | 1/6/5 |
| Group 1 n = 12 | Group 2 n = 12 | p Value | |
|---|---|---|---|
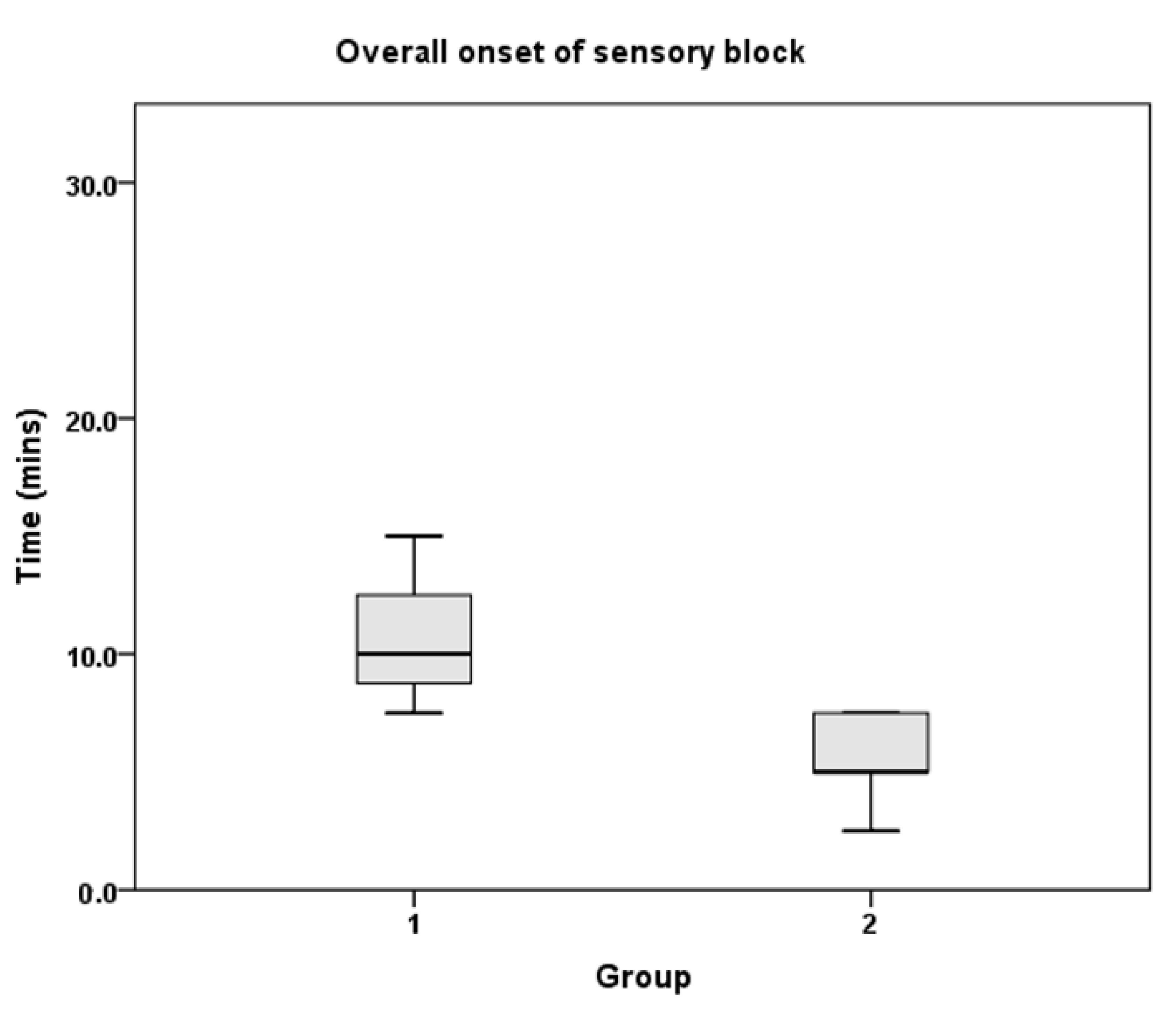
| Overall sensory block | 10 (8.8–12.5) | 5 (5–7.5) | <0.001 |
| Overall motor block | 7.5 (6.3–7.5) | 5 (2.5–7.5) | 0.001 |
| Radial nerve | |||
| Sensory block | 10 (7.5–11.3) | 5 (3.8–7.5) | 0.002 |
| Motor block | 5 (5–7.5) | 3.8 (2.5–5] | 0.014 |
| Ulnar nerve | |||
| Sensory block | 7.5 (7.5–10) | 5 (5–6.3) | 0.005 |
| Motor block | 5 (5–7.5) | 3.75 (2.5–5) | 0.007 |
| Median nerve | |||
| Sensory block | 7.5 (5–11.25) | 5 (5–7.5) | 0.001 |
| Motor block | 5 (5–7.5) | 3.8 (2.5–5) | 0.005 |
| Musculocutaneous nerve | |||
| Sensory block | 7.5 (7.5–8.8) | 5 (5–6.8) | 0.003 |
| Motor block | 5 (2.5–6.3) | 2.5 (2.5–5) | 0.18 |
| Group 1 n = 12 | Group 2 n = 12 | p Value | |
|---|---|---|---|
| Overall sensory block | 168 (148–190) | 225 (200–231) | <0.001 |
| Overall motor block | 168 (148–186) | 225 (208–231) | <0.001 |
| Radial nerve | |||
| Sensory block | 175 (148–192) | 225 (200–231) | 0.001 |
| Motor block | 180 (151–187) | 225 (208–231) | <0.001 |
| Ulnar nerve | |||
| Sensory block | 182 (156–192) | 227 (200–241) | 0.002 |
| Motor block | 178 (148–190) | 226 (211–233) | <0.001 |
| Median nerve | |||
| Sensory block | 180 (156–190) | 230 (200–241) | 0.001 |
| Motor block | 176 (156–193) | 225 (215–238) | <0.001 |
| Musculocutaneous nerve | |||
| Sensory block | 180 (156–195) | 233 (215–241) | 0.001 |
| Motor block | 168 (156–195) | 225 (215–231) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ranganath, A.; Hitka, T.; Iohom, G. Effects of Clonidine as an Adjuvant to Lidocaine with Epinephrine in Ultrasound Guided Axillary Brachial Plexus Block: A Randomised Controlled Trial. J. Clin. Med. 2021, 10, 4181. https://doi.org/10.3390/jcm10184181
Ranganath A, Hitka T, Iohom G. Effects of Clonidine as an Adjuvant to Lidocaine with Epinephrine in Ultrasound Guided Axillary Brachial Plexus Block: A Randomised Controlled Trial. Journal of Clinical Medicine. 2021; 10(18):4181. https://doi.org/10.3390/jcm10184181
Chicago/Turabian StyleRanganath, Anil, Tomas Hitka, and Gabriella Iohom. 2021. "Effects of Clonidine as an Adjuvant to Lidocaine with Epinephrine in Ultrasound Guided Axillary Brachial Plexus Block: A Randomised Controlled Trial" Journal of Clinical Medicine 10, no. 18: 4181. https://doi.org/10.3390/jcm10184181
APA StyleRanganath, A., Hitka, T., & Iohom, G. (2021). Effects of Clonidine as an Adjuvant to Lidocaine with Epinephrine in Ultrasound Guided Axillary Brachial Plexus Block: A Randomised Controlled Trial. Journal of Clinical Medicine, 10(18), 4181. https://doi.org/10.3390/jcm10184181