
Renal Outcome of IgM Nephropathy: A Comparative Prospective Cohort Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definition
2.2. Study Design and Data Collection
2.3. Statistical Analysis
3. Results
3.1. Clinical and Pathological Features of Patients
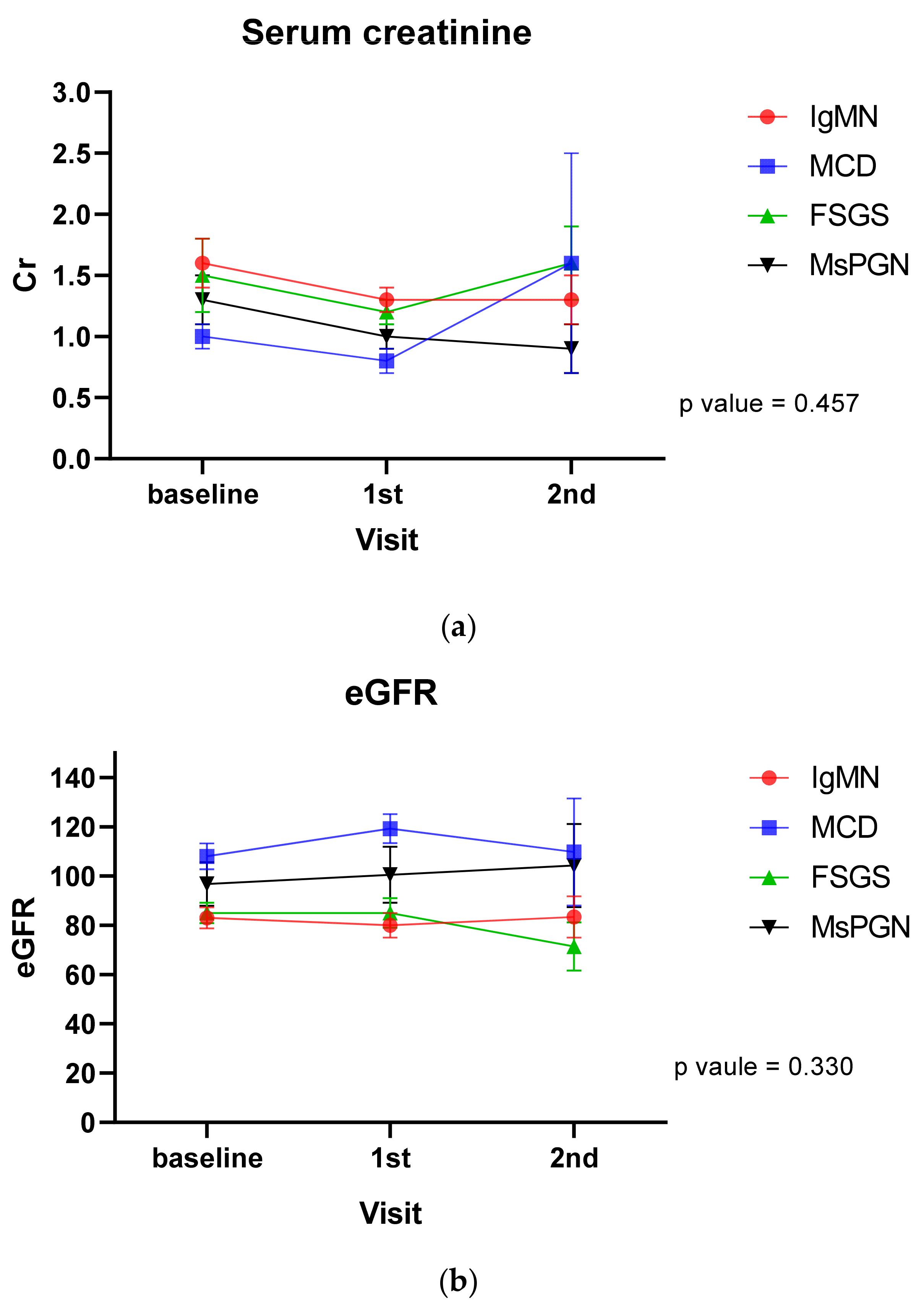
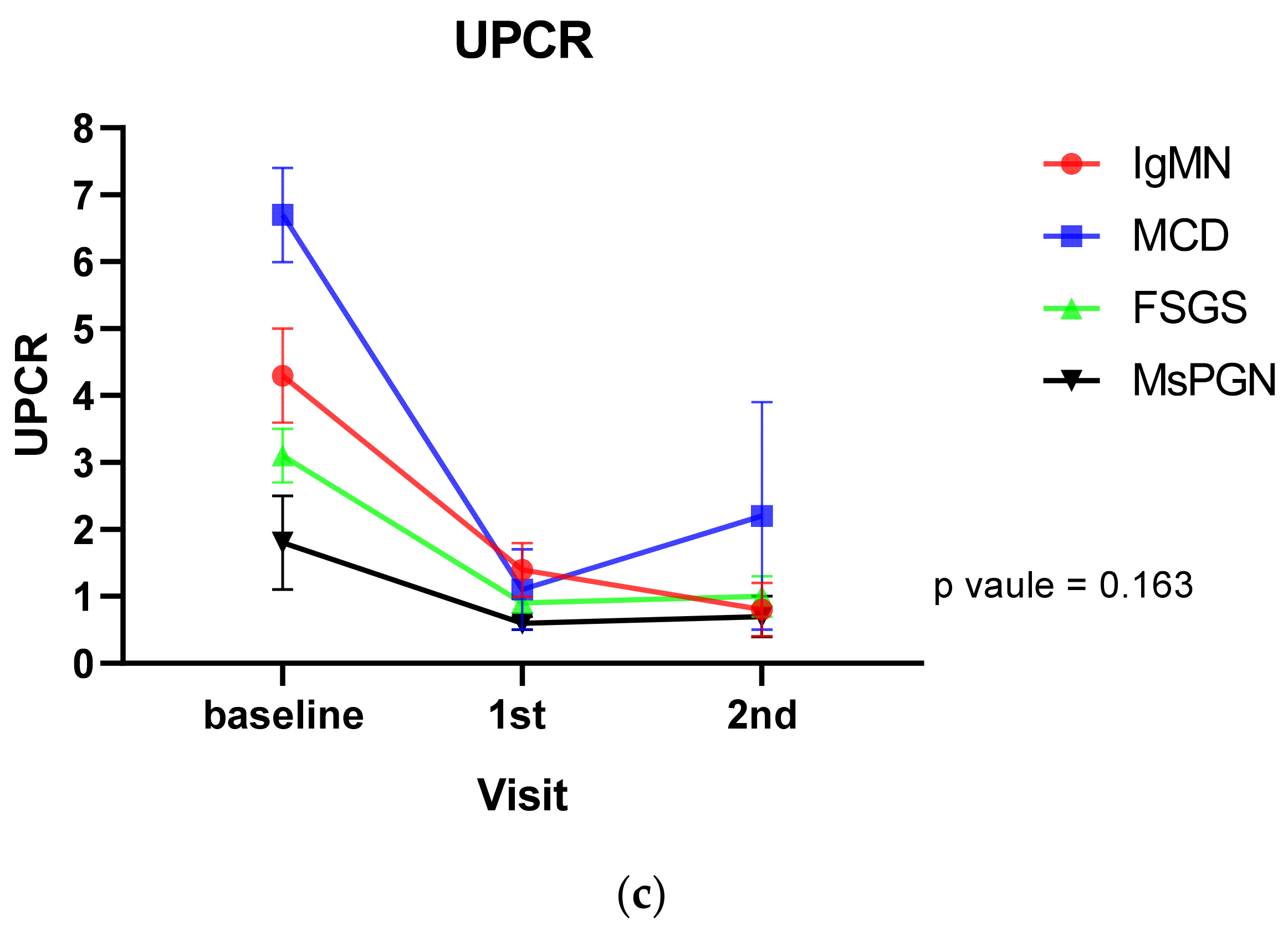
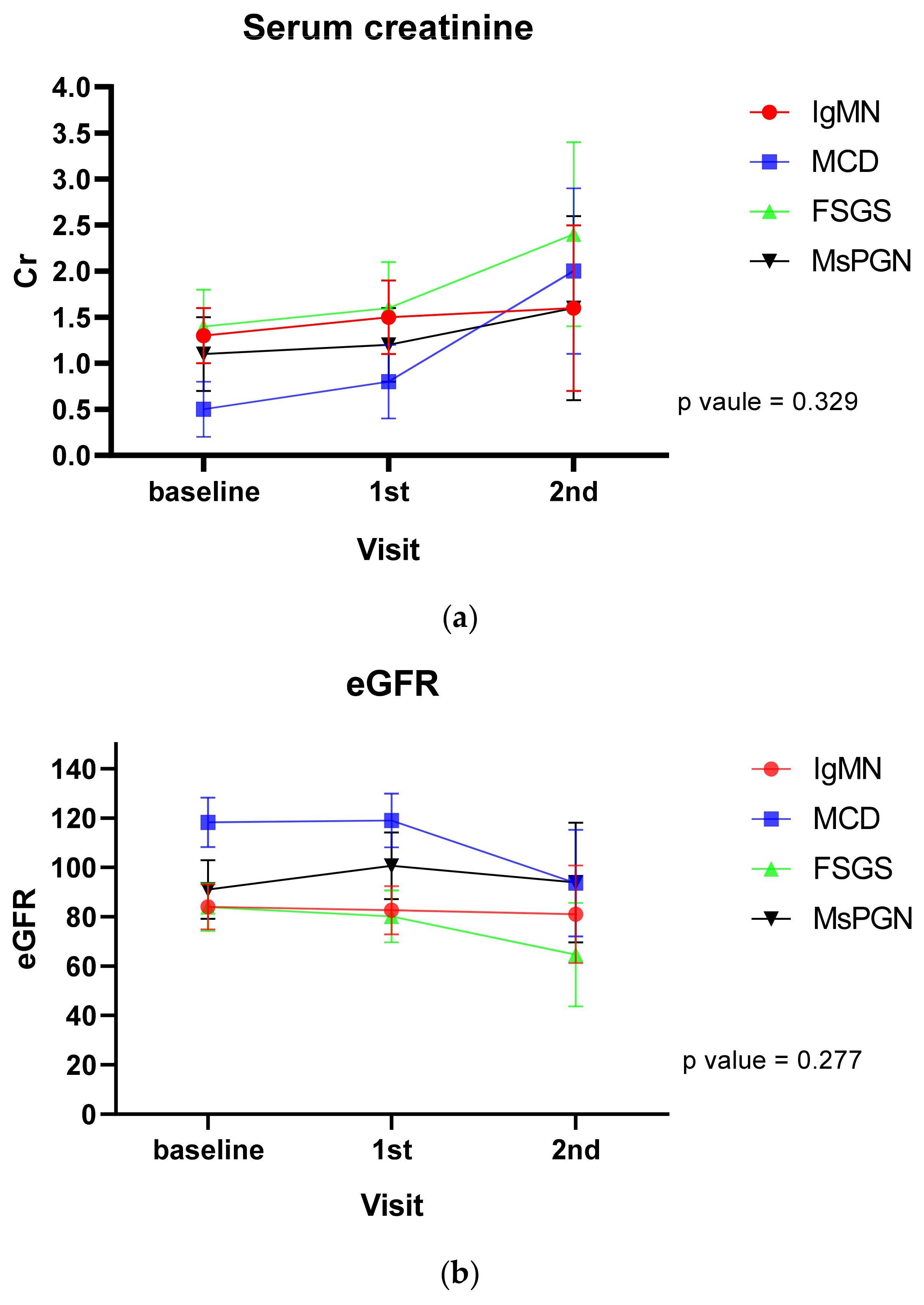
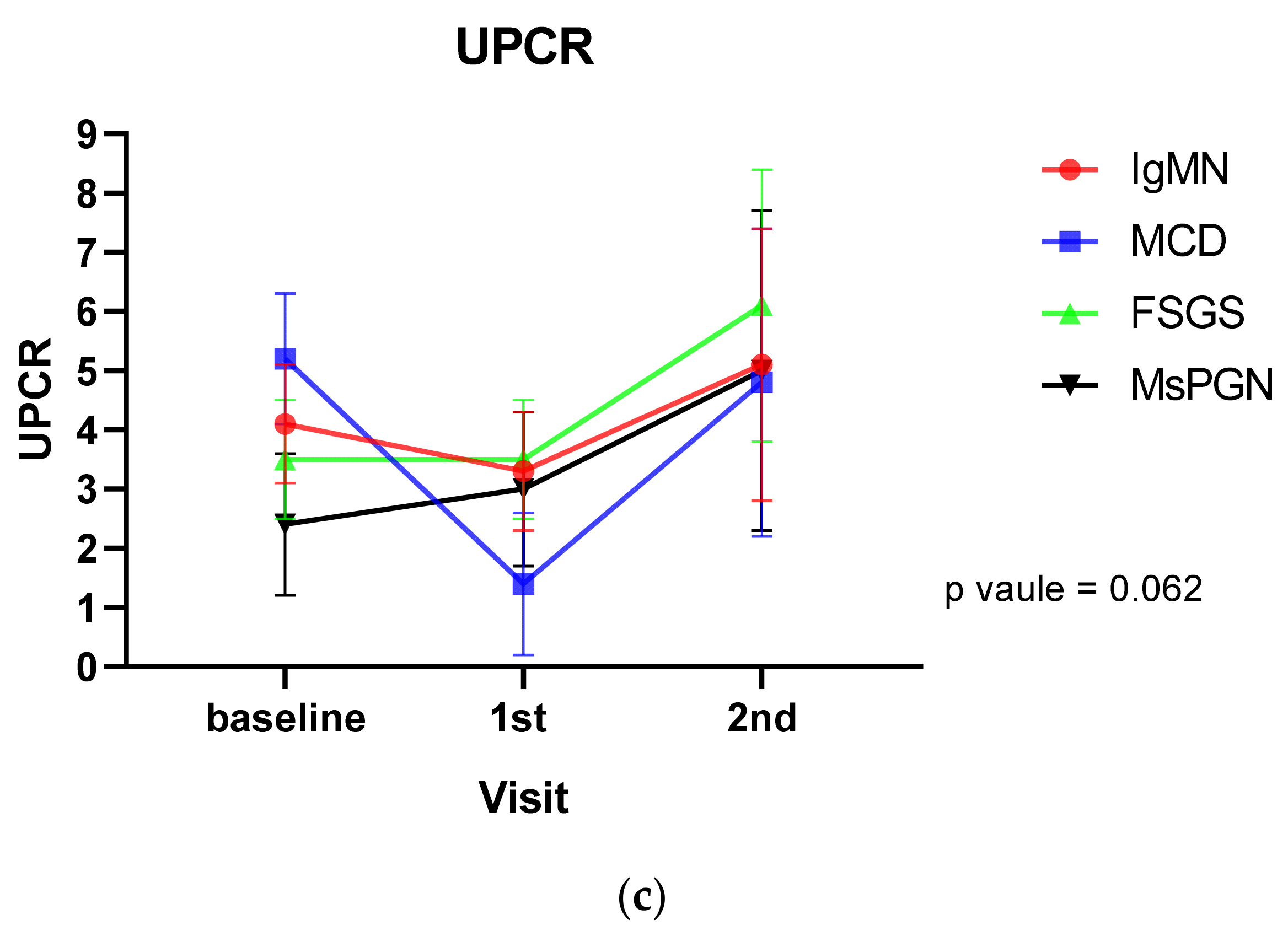
3.2. Renal Outcome
3.3. IgMN Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cohen, A.H.; Border, W.A.; Glassock, R.J. Nehprotic syndrome with glomerular mesangial IgM deposits. Lab. Investig. 1978, 38, 610–619. [Google Scholar]
- Bhasin, H.K.; Abuelo, J.G.; Nayak, R.; Esparza, A.R. Mesangial proliferative glomerulonephritis. Lab. Investig. 1978, 39, 21–29. [Google Scholar]
- Connor, T.M.; Aiello, V.; Griffith, M.; Cairns, T.; Roufosse, C.; Cook, H.T.; Pusey, C.D. The natural history of immunoglobulin M nephropathy in adults. Nephrol. Dial. Transplant. 2016, 32, 823–829. [Google Scholar] [CrossRef] [Green Version]
- Myllymäki, J.; Saha, H.; Mustonen, J.; Helin, H.; Pasternack, A. IgM nephropathy: Clinical picture and long-term prognosis. Am. J. Kidney Dis. 2003, 41, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Mubarak, M.; Kazi, J.I. IgM nephropathy revisited. Nephrourol. Mon. 2012, 4, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Mokhtar, G.A.; Jalalah, S.; Sultana, S. Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center. J. Nephropharmacol. 2014, 3, 33–37. [Google Scholar] [PubMed]
- Brugnano, R.; Del Sordo, R.; Covarelli, C.; Gnappi, E.; Pasquali, S. IgM nephropathy: Is it closer to minimal change disease or to focal segmental glomerulosclerosis? J. Nephrol. 2016, 29, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Shakeel, S.; Mubarak, M.; Kazi, J.I.; Lanewala, A. The prevalence and clinicopathological profile of IgM nephropathy in children with steroid-resistant nephrotic syndrome at a single centre in Pakistan. J. Clin. Pathol. 2012, 65, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Al-Eisa, A.; Carter, J.E.; Lirenman, D.S.; Magil, A.B. Childhood IgM Nephropathy: Comparison with Minimal Change Disease. Nephron 1996, 72, 37–43. [Google Scholar] [CrossRef]
- Feehally, J.; Cameron, J.S. IgA Nephropathy: Progress Before and Since Berger. Am. J. Kidney Dis. 2011, 58, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, A.; Fervenza, F.C.; Smith, R.J.H.; De Vriese, A.S.; Sethi, S. C3 Glomerulopathy: Ten Years’ Experience at Mayo Clinic. Mayo Clin. Proc. 2018, 93, 991–1008. [Google Scholar] [CrossRef] [PubMed]
- Wenderfer, S.E.; Swinford, R.D.; Braun, M.C. C1q nephropathy in the pediatric population: Pathology and pathogenesis. Pediatr. Nephrol. 2010, 25, 1385–1396. [Google Scholar] [CrossRef]
- Vanikar, A. IgM nephropathy; can we still ignore it. J. Nephropathol. 2013, 2, 98–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.S.; Kang, E.W.; Kie, J.H. A case report of immunoglobulin M nephropathy manifesting as crescentic glomerulonephritis and nephrotic syndrome in an adult. BMC Nephrol. 2019, 20, 335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Stevens, L.A. Estimating GFR Using the CKD Epidemiology Collaboration (CKD-EPI) Creatinine Equation: More Accurate GFR Estimates, Lower CKD Prevalence Estimates, and Better Risk Predictions. Am. J. Kidney Dis. 2010, 55, 622–627. [Google Scholar] [CrossRef] [Green Version]
- Yim, T.; Kim, S.-U.; Park, S.; Lim, J.-H.; Jung, H.-Y.; Cho, J.-H.; Kim, C.-D.; Kim, Y.-L.; Han, M.-H.; Choi, J.-Y.; et al. Patterns in renal diseases diagnosed by kidney biopsy: A single-center experience. Kidney Res. Clin. Prac. 2020, 39, 60–69. [Google Scholar] [CrossRef] [Green Version]
- Zabaneh, I.D.; Bandak, D.N.; Thammineni, V.S. IgM glomerulonephritis. Biomed. Res. Clin. Prac. 2018, 3, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Border, W.A. Distinguishing minimal-change disease from mesangial disorders. Kidney Int. 1988, 34, 419–434. [Google Scholar] [CrossRef] [Green Version]
- Habib, R.; Girardin, E.; Gagnadoux, M.-F.; Hinglais, N.; Levy, M.; Broyer, M. Immunopathological findings in idiopathic nephrosis: Clinical significance of glomerular “immune deposits”. Pediatr. Nephrol. 1988, 2, 402–408. [Google Scholar] [CrossRef]
- Tejani, A. Morphological Transition in Minimal Change Nephrotic Syndrome. Nephron 1985, 39, 157–159. [Google Scholar] [CrossRef]
- Chan, Y.H.; Wong, K.M.; Choi, K.S.; Chak, W.L.; Cheung, C.Y. Clinical manifestation and progression of IgMmesangial nephropathy: A single center perspective. Hong Kong J. Nephrol. 2000, 2, 23–26. [Google Scholar] [CrossRef] [Green Version]
- Strassheim, D.; Renner, B.; Panzer, S.; Fuquay, R.; Kulik, L.; Ljubanović, D.; Holers, V.M.; Thurman, J.M. IgM Contributes to Glomerular Injury in FSGS. J. Am. Soc. Nephrol. 2013, 24, 393–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platt, J.L.; Cascalho, M. IgM in the kidney: A multiple personality disorder. Kidney Int. 2015, 88, 439–441. [Google Scholar] [CrossRef] [Green Version]
- Boes, M.; Prodeus, A.P.; Schmidt, T.; Carroll, M.C.; Chen, J. A Critical Role of Natural Immunoglobulin M in Immediate Defense against Systemic Bacterial Infection. J. Exp. Med. 1998, 188, 2381–2386. [Google Scholar] [CrossRef] [PubMed]
- Grönwall, C.; Silverman, G. Natural IgM: Beneficial Autoantibodies for the Control of Inflammatory and Autoimmune Disease. J. Clin. Immunol. 2014, 34, 12–21. [Google Scholar] [CrossRef] [Green Version]
- Wootla, B.; Watzlawik, J.O.; Denic, A.; Rodriguez, M. The road to remyelination in demyelinating diseases: Current status and prospects for clinical treatment. Expert Rev. Clin. Immunol. 2013, 9, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Panzer, S.E.; Laskowski, J.; Renner, B.; Kulik, L.; Ljubanovic, D.; Huber, K.M.; Zhong, W.; Pickering, M.C.; Holers, V.M.; Thurman, J.M. IgM exacerbates glomerular disease progression in complement-induced glomerulopathy. Kidney Int. 2015, 88, 528–537. [Google Scholar] [CrossRef] [Green Version]
- Ji-Yun, Y.; Melvin, T.; Sibley, R.; Michael, A.F. No evidence for a specific role of IgM in mesangial proliferation of idiopathic nephrotic syndrome. Kidney Int. 1984, 25, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Vilches, A.R.; Turner, D.R.; Cameron, J.S.; Ogg, C.S.; Chantler, C.; Williams, D.G. Significance of mesangial IgM deposition in “minimal change” nephrotic syndrome. Lab. Investig. 1982, 46, 5–10. [Google Scholar]
- Ahmed, F.A.; El-Meanawy, A. IgM nephropathy—Successful treatment with rituximab. Saudi J. Kidney Dis. Transplant. 2019, 30, 235. [Google Scholar] [CrossRef]
- Betjes, M.G.; Roodnat, J.I. Resolution of IgM Nephropathy after Rituximab Treatment. Am. J. Kidney Dis. 2009, 53, 1059–1062. [Google Scholar] [CrossRef] [PubMed]
- Salmon, A.H.J.; Kamel, D.; Mathieson, P.W. Recurrence of IgM nephropathy in a renal allograft. Nephrol. Dial. Transplant. 2004, 19, 2650–2652. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (n = 258) | IgMN (n = 94) | MCD (n = 57) | FSGS (n = 81) | MsPGN (n = 26) | p Value | p Value for IgMN vs. MCD | p Value for IgMN vs. FSGS | p Value for IgMN vs. MsPGN | p Value for MCD vs. FSGS | p Value for MCD vs. MsPGN | p Value for FSGS vs. MsPGN | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age, yr | 46.5 ± 16.8 | 46.5 ± 16.1 | 46.2 ± 18.6 | 49.5 ± 16.1 | 38.3 ± 15.9 | 0.033 | 0.996 | 0.675 | 0.125 | 0.642 | 0.234 | 0.016 |
| Female | 123 (47.7) | 45 (47.9) | 20 (35.1) | 44 (54.3) | 14 (53.8) | 0.142 | 0.744 | >0.999 | >0.999 | 0.154 | 0.642 | >0.999 |
| Drinking | 213 (82.6) | 79 (84.0) | 44 (77.2) | 70 (86.4) | 20 (76.9) | 0.441 | >0.999 | >0.999 | >0.999 | 0.955 | >0.999 | >0.999 |
| Smoking | 0.095 | 0.776 | >0.999 | >0.999 | 0.044 | >0.999 | >0.999 | |||||
| Non-smoker | 211 (81.8) | 77 (81.9) | 40 (70.2) | 71 (87.7) | 23 (88.5) | |||||||
| Past smoker | 13 (5.0) | 4 (4.3) | 7 (12.3) | 1 (1.2) | 1 (3.8) | |||||||
| Current smoker | 34 (13.2) | 13 (13.8) | 10 (17.5) | 9 (11.1) | 2 (7.7) | |||||||
| Hypertension | 90 (34.9) | 31 (33.0) | 15 (26.3) | 35 (43.2) | 9 (34.6) | 0.215 | >0.999 | 0.983 | >0.999 | 0.253 | >0.999 | >0.999 |
| Diabetes | 24 (9.3) | 7 (7.4) | 5 (8.8) | 10 (12.3) | 2 (7.7) | 0.712 | 0.712 | >0.999 | >0.999 | >0.999 | >0.999 | >0.999 |
| SBP, mmHg | 127.1 ± 16.7 | 127.6 ± 18.6 | 125.0 ± 14.6 | 129.0 ± 15.8 | 123.2 ± 15.9 | 0.419 | 0.933 | 0.87 | 0.761 | 0.568 | 0.978 | 0.494 |
| DBP, mmHg | 76.5 ± 11.0 | 76.1 ± 12.2 | 75.6 ± 11.1 | 78.1 ± 10.4 | 75.3 ± 8.2 | 0.586 | 0.981 | 0.548 | >0.999 | 0.909 | 0.962 | 0.786 |
| Nephrotic range proteinuria | 95 (36.8) | 34 (36.2) | 37 (64.9) | 21 (25.9) | 3 (11.5) | <0.001 | 0.001 | 0.146 | 0.016 | <0.001 | <0.001 | 0.126 |
| Hematuria | 167 (64.7) | 58 (61.7) | 36 (63.2) | 54 (66.7) | 19 (73.1) | 0.714 | 0.858 | 0.495 | 0.284 | 0.67 | 0.375 | 0.541 |
| WBC, ×10/mm3 | 7.5 ± 2.4 | 7.8 ± 2.6 | 7.7 ± 2.9 | 7.3 ± 1.9 | 6.9 ± 2.3 | 0.576 | 0.947 | 0.931 | 0.486 | >0.999 | 0.857 | 0.748 |
| Hb, g/dL | 13.2 ± 2.1 | 12.8 ± 2.1 | 14.2 ± 1.6 | 13.0 ± 2.0 | 12.8 ± 2.6 | <0.001 | <0.001 | 0.998 | 0.916 | 0.003 | 0.162 | 0.963 |
| HbA1c, % | 5.6 ± 0.6 | 5.6 ± 0.5 | 5.6 ± 0.6 | 5.6 ± 0.7 | 5.4 ± 0.3 | 0.489 | 0.972 | 0.98 | 0.299 | >0.999 | 0.765 | 0.703 |
| BUN, mg/dL | 21.3 ± 14.2 | 22.1 ± 14.2 | 20.0 ± 13.3 | 22.0 ± 15.5 | 19.7 ± 11.9 | 0.45 | 0.819 | 0.97 | 0.706 | 0.578 | 0.995 | 0.603 |
| Creatinine, mg/L | 1.4 ±1.7 | 1.6 ± 1.5 | 1.0 ± 0.5 | 1.5 ± 2.5 | 1.3 ± 1.1 | 0.032 | 0.019 | 0.859 | 0.787 | 0.125 | 0.760 | 0.958 |
| eGFR, mL/min/1.73 m2 | 90.6 ± 41.6 | 83.1 ± 41.7 | 108.0 ± 40.1 | 85.0 ± 37.9 | 96.8 ± 45.6 | 0.001 | 0.002 | 0.996 | 0.443 | 0.004 | 0.765 | 0.440 |
| UPCR | 2.0 (0.7–6.2) | 1.7 (0.3–6.0) | 6.2 (2.0–9.0) | 1.8 (0.9–3.9) | 0.6 (0.3–1.8) | <0.001 | 0.001 | 0.946 | 0.203 | <0.001 | <0.001 | 0.013 |
| ESR, mm/hr | 28.4 ± 26.6 | 26.5 ± 25.6 | 37.9 ± 29.8 | 26.6 ± 24.7 | 21.8 ± 26.0 | 0.019 | 0.088 | 0.967 | 0.528 | 0.131 | 0.047 | 0.337 |
| hs-CRP, mg/L | 0.8 ± 3.4 | 0.4 ± 1.0 | 0.8 ± 2.3 | 0.5 ± 1.6 | 3.6 ± 9.3 | 0.908 | 0.998 | 0.934 | 0.997 | 0.918 | 0.994 | 0.994 |
| Total protein, g/dL | 6.1 ± 1.4 | 6.2 ± 1.3 | 4.9 ± 1.4 | 6.5 ± 1.1 | 6.9 ± 0.9 | <0001 | <0.001 | 0.482 | 0.189 | <0.001 | <0.001 | 0.762 |
| Albumin, g/dL | 3.4 ± 1.1 | 3.5 ± 1.1 | 2.4 ± 1.1 | 3.7 ± 0.9 | 4.0 ± 0.8 | <0001 | <0.001 | 0.74 | 0.188 | <0.001 | <0.001 | 0.462 |
| Total cholesterol, mg/dL | 248.4 ± 118.3 | 234.4 ± 101.8 | 344.7 ± 133.3 | 214.8 ± 97.9 | 184.3 ± 64.5 | <0001 | <0.001 | 0.476 | 0.04 | <0.001 | <0.001 | 0.379 |
| Ferritin, ng/mL | 192.0 ± 244.1 | 189.2 ± 230.7 | 262.2 ± 299.2 | 157.8 ± 208.5 | 163.9 ± 264.6 | 0.031 | 0.173 | 0.792 | 0.899 | 0.025 | 0.132 | >0.999 |
| C3 depletion | 29 (11.7) | 15 (16.5) | 3 (5.5) | 6 (7.7) | 5 (21.7) | 0.057 | 0.050 | 0.084 | 0.548 | 0.735 | 0.045 | 0.119 |
| C4 depletion | 1 (0.4) | 0 (0.0) | 0 (0.0) | 1 (1.3) | 0 (0.0) | 0.632 | N/A | 0.462 | N/A | <0.999 | N/A | >0.999 |
| IgG, mg/dL | 940.5 ± 453.7 | 942.1 ± 392.0 | 616.9 ± 383.7 | 1059.0 ± 371.4 | 1307.4 ± 626.9 | <0001 | <0.001 | 0.185 | 0.017 | <0.001 | <0.001 | 0.195 |
| IgA, mg/dL | 241.5 ± 115.8 | 222.2 ± 103.8 | 264.2 ± 138.6 | 249.4 ± 117.5 | 238.1 ± 86.4 | 0.366 | 0.346 | 0.605 | 0.887 | 0.923 | 0.989 | >0.999 |
| IgM, mg/dL | 162.0 ± 434.0 | 231.7 ± 702.6 | 132.9 ± 106.1 | 115.1 ± 61.1 | 112.5 ± 57.3 | 0.88 | 0.991 | 0.966 | 0.985 | 0.874 | 0.942 | >0.999 |
| IgE, mg/dL | 653.9 ± 3078.4 | 416.3 ± 910.4 | 1548.6 ± 6377.9 | 489.3 ± 1451.9 | 156.8 ± 250.3 | 0.01 | 0.242 | 0.339 | 0.461 | 0.018 | 0.074 | 0.994 |
| Treatment | ||||||||||||
| RAAS blocker (%) | 152 (63.1) | 60 (64.5) | 22 (44.0) | 56 (73.7) | 14 (63.6) | 0.009 | 0.108 | >0.999 | >0.999 | 0.005 | 0.749 | >0.999 |
| Furosemide (%) | 84 (35.0) | 28 (30.1) | 37 (74.0) | 15 (19.7) | 4 (19.0) | <0001 | <0001 | 0.742 | >0.999 | <0001 | <0001 | >0.999 |
| Glucocorticoids (%) | 106 (44.0) | 36 (38.7) | 39 (78.0) | 23 (30.3) | 8 (36.4) | <0001 | <0001 | >0.999 | >0.999 | <0001 | 0.004 | >0.999 |
| Rituximab (%) | 1 (0.4) | 1 (1.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | >0.999 | >0.999 | >0.999 | >0.999 | N/A | N/A | N/A |
| Other immunosuppressants (%) | 10 (4.2) | 5 (5.4) | 3 (6.0) | 2 (2.6) | 0 (0.0) | 0.653 | >0.999 | >0.999 | >0.999 | >0.999 | >0.999 | >0.999 |
| Overall (n = 258) | IgMN (n = 94) | MCD (n = 57) | FSGS (n = 81) | MsPGN (n = 26) | p Value | p Value for IgMN vs. MCD | p Value for IgMN vs. FSGS | p Value for IgMN vs. MsPGN | p Value for MCD vs. FSGS | p Value for MCD vs. MsPGN | p Value for FSGS vs. MsPGN | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Glomerulosclerosis, % | 22.4 ± 26.0 | 23.8 ± 26.6 | 2.5 ± 6.2 | 33.9 ± 25.4 | 21.7 ± 28.3 | <0001 | <0.001 | 0.011 | 0.901 | <0.001 | 0.01 | 0.113 |
| Mesangial matrix expansion | <0001 | >0.999 | 0.35 | <0001 | 0.427 | <0001 | 0.001 | |||||
| 0, negative | 91 (40.6) | 38 (40.4) | 22 (50.0) | 31 (45.6) | 0 (0.0) | |||||||
| 1, trace | 72 (32.1) | 35 (37.2) | 17 (38.6) | 16 (23.5) | 4 (22.2) | |||||||
| 2, mild | 53 (23.7) | 18 (19.1) | 5 (11.4) | 19 (27.9) | 11 (61.1) | |||||||
| 3, moderate | 5 (2.2) | 0 (0.0) | 0 (0.0) | 2 (2.9) | 3 (16.7) | |||||||
| 4, marked | 3 (1.3) | 3 (3.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||||||
| Mesangial cell proliferation | <0001 | >0.999 | 0.341 | <0001 | 0.086 | <0001 | 0.001 | |||||
| 0, negative | 91 (40.6) | 38 (40.4) | 20 (45.5) | 33 (48.5) | 0 (0.0) | |||||||
| 1, trace | 75 (33.5) | 36 (38.3) | 20 (45.5) | 15 (22.1) | 4 (22.2) | |||||||
| 2, mild | 53 (23.7) | 20 (21.3) | 4 (9.1) | 18 (26.5) | 11 (61.1) | |||||||
| 3, moderate | 5 (2.2) | 0 (0.0) | 0 (0.0) | 2 (2.9) | 3 (16.7) | |||||||
| Crescent, % | 1.8 ± 11.0 | 2.4 ± 13.1 | 0.0 ± 0.0 | 2.0 ± 12.6 | 1.7 ± 5.9 | 0.085 | 0.396 | 0.998 | 0.396 | 0.341 | 0.03 | 0.522 |
| Interstitial fibrosis | 0.001 | 0.002 | >0.999 | >0.999 | <0001 | 0.016 | >0.999 | |||||
| 0, negative | 78 (34.8) | 30 (31.9) | 28 (63.6) | 16 (23.5) | 4 (22.2) | |||||||
| 1, trace | 63 (28.1) | 23 (24.5) | 11 (25.0) | 22 (32.4) | 7 (38.9) | |||||||
| 2, mild | 56 (25.0) | 29 (30.9) | 5 (11.4) | 18 (26.5) | 4 (22.2) | |||||||
| 3, moderate | 26 (11.6) | 11 (11.7) | 0 (0.0) | 12 (17.6) | 3 (16.7) | |||||||
| 4, marked | 1 (0.4) | 1 (1.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||||||
| Tubular atrophy | 0.003 | 0.026 | >0.999 | >0.999 | 0.002 | 0.011 | >0.999 | |||||
| 0, negative | 86 (38.4) | 34 (36.2) | 29 (65.9) | 19 (27.9) | 4 (22.2) | |||||||
| 1, trace | 56 (25.0) | 21 (22.3) | 9 (20.5) | 19 (27.9) | 7 (38.9) | |||||||
| 2, mild | 56 (25.0) | 27 (28.7) | 6 (13.6) | 19 (27.9) | 4 (22.2) | |||||||
| 3, moderate | 23 (10.3) | 9 (9.6) | 0 (0.0) | 11 (16.2) | 3 (16.7) | |||||||
| 4, marked | 3 (1.3) | 3 (3.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||||||
| Acute tubular necrosis | 0.529 | >0.999 | >0.999 | >0.999 | >0.999 | >0.999 | >0.999 | |||||
| 0, negative | 198 (88.4) | 84 (89.4) | 39 (88.6) | 60 (88.2) | 15 (83.3) | |||||||
| 1, trace | 5 (2.2) | 0 (0.0) | 2 (4.5) | 2 (2.9) | 1 (5.6) | |||||||
| 2, mild | 11 (4.9) | 5 (5.3) | 1 (2.3) | 4 (5.9) | 1 (5.6) | |||||||
| 3, moderate | 10 (4.5) | 5 (5.3) | 2 (4.5) | 2 (2.9) | 1 (5.6) | |||||||
| Arterial intimal hyalinosis | 0.077 | >0.999 | 0.326 | 0.125 | >0.999 | >0.999 | >0.999 | |||||
| 0, negative | 194 (87.8) | 85 (91.4) | 38 (90.5) | 57 (83.8) | 14 (77.8) | |||||||
| 1, trace | 15 (6.8) | 7 (7.5) | 3 (7.1) | 4 (5.9) | 1 (5.6) | |||||||
| 2, mild | 8 (3.6) | 1 (1.1) | 1 (2.4) | 5 (7.4) | 1 (5.6) | |||||||
| 3, moderate | 4 (1.8) | 0 (0.0) | 0 (0.0) | 2 (2.9) | 2 (11.1) | |||||||
| Fibrous wall thickening | 0.869 | >0.999 | >0.999 | >0.999 | >0.999 | >0.999 | >0.999 | |||||
| 0, negative | 148 (67.0) | 62 (66.7) | 31 (73.8) | 44 (64.7) | 11 (61.1) | |||||||
| 1, trace | 19 (8.6) | 7 (7.5) | 4 (9.5) | 7 (10.3) | 1 (5.6) | |||||||
| 2, mild | 29 (13.1) | 15 (16.1) | 4 (9.5) | 7 (10.3) | 3 (16.7) | |||||||
| 3, moderate | 22 (10.0) | 8 (8.6) | 3 (7.1) | 9 (13.2) | 2 (11.1) | |||||||
| 4, marked | 3 (1.4) | 1 (1.1) | 0 (0.0) | 1 (1.5) | 1 (5.6) | |||||||
| Foot process effacement | <0.001 | <0.001 | <0.001 | 0.589 | 0.163 | <0.001 | 0.003 | |||||
| 0, no | 38 (16.5) | 20 (21.7) | 5 (9.6) | 10 (14.5) | 3 (17.6) | |||||||
| 1, focal | 42 (18.3) | 28 (30.4) | 1 (1.9) | 1 (7.2) | 8 (47.1) | |||||||
| 2, diffuse | 150 (65.2) | 44 (47.8) | 46 (88.5) | 2 (78.3) | 6 (35.3) |
| IgMN | MCD | FSGS | MsPGN | p Value (Time Effect) | p Value (Group Effect) | p Value (Time*Group Effect) | p Value for IgMN vs. MCD | p Value for IgMN vs. FSGS | p Value for IgMN vs. MsPGN | p Value for MCD vs. FSGS | p Value for MCD vs. MsPGN | p Value for FSGS vs. MsPGN | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Serum creatinine | 0.232 | 0.141 | 0.329 | ||||||||||
| Baseline | 1.3 ± 0.3 | 0.5 ± 0.3 | 1.4 ± 0.4 | 1.1 ± 0.4 | <0.001 | 0.867 | 0.376 | 0.005 | 0.011 | 0.444 | |||
| 1st visit | 1.5 ± 0.4 | 0.8 ± 0.4 | 1.6 ± 0.5 | 1.2 ± 0.4 | 0.02 | 0.783 | 0.488 | 0.054 | 0.287 | 0.433 | |||
| 2nd visit | 1.6 ± 0.9 | 2.0 ± 0.9 | 2.4 ± 1.0 | 1.6 ± 1.0 | 0.446 | 0.132 | 0.964 | 0.492 | 0.492 | 0.178 | |||
| eGFR | 0.113 | 0.001 | 0.277 | ||||||||||
| Baseline | 84.1 ± 9.2 | 118.3 ± 10.0 | 83.9 ± 9.7 | 91.1 ± 11.9 | <0.001 | 0.98 | 0.44 | <0.001 | 0.011 | 0.439 | |||
| 1st visit | 82.7 ± 9.8 | 119.0 ± 10.9 | 80.2 ± 10.5 | 100.7 ± 13.5 | <0.001 | 0.745 | 0.125 | <0.001 | 0.161 | 0.087 | |||
| 2nd visit | 81.0 ± 19.8 | 93.7 ± 21.6 | 64.7 ± 21.0 | 93.9 ± 24.3 | 0.331 | 0.119 | 0.377 | 0.037 | 0.99 | 0.053 | |||
| UPCR | 0.006 | 0.522 | 0.062 | ||||||||||
| Baseline | 4.1 ± 1.0 | 5.2 ± 1.1 | 3.5 ± 1.0 | 2.4 ± 1.2 | 0.173 | 0.381 | 0.082 | 0.035 | 0.008 | 0.225 | |||
| 1st visit | 3.3 ± 1.0 | 1.4 ± 1.2 | 3.5 ± 1.0 | 3.0 ± 1.3 | 0.107 | 0.831 | 0.835 | 0.058 | 0.264 | 0.704 | |||
| 2nd visit | 5.1 ± 2.3 | 4.8 ± 2.6 | 6.1 ± 2.3 | 5.0 ± 2.7 | 0.8896 | 0.4184 | 0.9501 | 0.461 | 0.948 | 0.5023 | |||
| Overall (n = 94) | MCD-Like (n = 25) | FSGS-Like (n = 21) | MsPGN (n = 48) | p Value | p Value for MCD-Like vs. FSGS-Like | p Value for MCD-Like vs. MsPGN-Like | p Value for FSGS-Like vs. MsPGN-Like | |
|---|---|---|---|---|---|---|---|---|
| Clinical findings | ||||||||
| Age | 46.5 ± 16.1 | 45.7 ± 16.5 | 50.9 ± 19.3 | 44.9 ± 14.3 | 0.311 | 0.498 | 0.986 | 0.285 |
| Female | 45 (47.9) | 12 (48.0) | 9 (42.9) | 24 (50.0) | 0.861 | >0.999 | >0.999 | >0.999 |
| Drinking | 15 (16.0) | 5 (20.0) | 4 (19.0) | 6 (12.5) | 0.614 | >0.999 | >0.999 | >0.999 |
| Smoking | 0.056 | >0.999 | >0.999 | 0.030 | ||||
| Non-smoker | 77 (81.9) | 20 (80.0) | 14 (66.7) | 43 (89.6) | ||||
| Past smoker | 4 (4.3) | 1 (4.0) | 3 (14.3) | 0 (0.0) | ||||
| Current smoker | 13 (13.8) | 4 (16.0) | 4 (19.0) | 5 (10.4) | ||||
| Hypertension | 31 (33.0) | 6 (24.0) | 11 (52.4) | 14 (29.2) | 0.091 | 0.141 | >0.999 | 0.195 |
| Diabetes | 7 (7.4) | 1 (4.0) | 3 (14.3) | 3 (6.3) | 0.501 | 0.954 | >0.999 | >0.999 |
| SBP, mmHg | 127.6 ± 18.6 | 124.2 ± 15.5 | 135.9 ± 25.1 | 125.8 ± 15.8 | 0.122 | 0.164 | 0.877 | 0.169 |
| DBP, mmHg | 76.1 ± 12.2 | 76.8 ± 8.9 | 76.8 ± 19.7 | 75.3 ± 9.3 | 0.795 | 0.890 | 0.796 | 0.954 |
| Nephrotic range proteinuria | 34 (36.2) | 25 (100) | 9 (42.9) | 0 (0) | <0.001 | <0.001 | <0.001 | <0.001 |
| Hematuria | 58 (61.7) | 17 (68) | 12 (57.1) | 29 (60.4) | 0.729 | 0.452 | 0.527 | 0.800 |
| WBC, ×10/mm3 | 7.8 ± 2.6 | 8.2 ± 3.0 | 8.5 ± 2.4 | 7.3 ± 2.4 | 0.087 | 0.610 | 0.427 | 0.091 |
| Hb, g/dL | 12.8 ± 2.1 | 12.7 ± 2.6 | 13.2 ± 2.1 | 12.7 ± 1.9 | 0.824 | 0.976 | 0.935 | 0.817 |
| HbA1c, % | 5.6 ± 0.5 | 5.5 ± 0.6 | 5.9 ± 0.6 | 5.5 ± 0.4 | 0.084 | 0.164 | 0.985 | 0.091 |
| BUN, mg/dL | 22.1 ± 14.2 | 25.4 ± 14.7 | 26.5 ± 17.1 | 18.4 ± 11.6 | 0.015 | 0.998 | 0.083 | 0.028 |
| ESR, mm/hr | 26.5 ± 25.6 | 45.8 ± 25.7 | 26.1 ± 27.2 | 16.5 ± 18.6 | <0.001 | 0.022 | <0.0001 | 0.130 |
| hs-CRP, mg/L | 0.4 ± 1.0 | 0.6 ± 1.3 | 0.4 ± 0.6 | 0.4 ± 1.0 | 0.592 | 0.753 | 0.929 | 0.594 |
| Total protein, g/dL | 6.2 ± 1.3 | 5.1 ± 1.1 | 5.9 ± 1.4 | 6.9 ± 0.8 | <0.001 | 0.118 | <0.0001 | 0.016 |
| Albumin, g/dL | 3.5 ± 1.1 | 2.4 ± 0.8 | 3.2 ± 1.1 | 4.2 ± 0.6 | <0.001 | 0.019 | <0.0001 | 0.001 |
| Total cholesterol, mg/dL | 234.4 ± 101.8 | 325.9 ± 108.2 | 226.5 ± 84.3 | 190.1 ± 70.4 | <0.001 | 0.009 | <0.0001 | 0.158 |
| ferritin, ng/mL | 189.2 ± 230.7 | 236.4 ± 328.1 | 213.7 ± 159.7 | 152.3 ± 181.6 | 0.165 | 0.595 | 0.541 | 0.177 |
| C3 depletion | 15 (16.5) | 3 (12.5) | 2 (9.5) | 10 (21.7) | 0.383 | 0.754 | 0.349 | 0.230 |
| C4 depletion | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | >0.999 | >0.999 | >0.999 | >0.999 |
| IgG, mg/dL | 942.1 ± 392.0 | 776.1 ± 476.0 | 935.7 ± 353.3 | 1031.7 ± 336.3 | 0.011 | 0.170 | 0.009 | 0.560 |
| IgA, mg/dL | 222.2 ± 103.8 | 234.4 ± 124.4 | 241.4 ± 67.3 | 207.0 ± 105.5 | 0.288 | 0.907 | 0.654 | 0.260 |
| IgM (serum), mg/dL | 231.7 ± 702.6 | 331.7 ± 786.1 | 127.3 ± 75.0 | 229.3 ± 813.3 | 0.262 | 0.901 | 0.272 | 0.572 |
| Ig E (serum), mg/dL | 416.3 ± 910.4 | 663.8 ± 1590.1 | 694.7 ± 779.3 | 159.6 ± 240.3 | 0.077 | 0.448 | 0.793 | 0.053 |
| Creatinine, mg/dL, baseline | 1.6 ± 1.5 | 1.7 ± 1.5 | 2.0 ± 1.5 | 1.3 ± 1.6 | 0.001 | 0.296 | 0.208 | <0.001 |
| eGFR, baseline | 83.1 ± 41.7 | 77.8 ± 46.0 | 56.3 ± 32.6 | 97.6 ± 36.8 | <0.001 | 0.276 | 0.183 | <0.001 |
| UPCR, baseline | 1.7 (0.3–6.0) | 6.3 (5.6–10.4) | 2.1 (1.5–7.3) | 0.4 (0.1–1.3) | <0.001 | 0.089 | <0.001 | <0.001 |
| Pathologic findings | ||||||||
| Glomerulosclerosis, % | 23.8 ± 26.6 | 19.5 ± 26.8 | 35.3 ± 27.2 | 21.0 ± 25.3 | 0.023 | 0.039 | 0.883 | 0.040 |
| Mesangial matrix expansion | 0.598 | 0.977 | >0.999 | >0.999 | ||||
| 0, negative | 38 (40.4) | 11 (44.0) | 7 (33.3) | 20 (41.7) | ||||
| 1, trace | 35 (37.2) | 7 (28.0) | 11 (52.4) | 17 (35.4) | ||||
| 2, mild | 18 (19.1) | 5 (20.0) | 3 (14.3) | 10 (20.8) | ||||
| 3, moderate | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||||
| 4, marked | 3 (3.2) | 2 (8.0) | 0 (0.0) | 1 (2.1) | ||||
| Mesangial cell proliferation | 0.987 | >0.999 | >0.999 | >0.999 | ||||
| 0, negative | 38 (40.4) | 10 (40.0) | 8 (38.1) | 20 (41.7) | ||||
| 1, trace | 36 (38.3) | 9 (36.0) | 9 (42.9) | 18 (37.5) | ||||
| 2, mild | 20 (21.3) | 6 (24.0) | 4 (19.0) | 10 (20.8) | ||||
| 3, moderate | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||||
| Crescent, % | 2.4 ± 13.1 | 3.6 ± 17.3 | 0.7 ± 2.3 | 2.6 ± 13.8 | 0.688 | 0.810 | 0.999 | 0.700 |
| Interstitial fibrosis | 0.002 | 0.007 | 0.38 | 0.005 | ||||
| 0, negative | 30 (31.9) | 9 (36.0) | 3 (14.3) | 18 (37.5) | ||||
| 1, trace | 23 (24.5) | 8 (32.0) | 1 (4.8) | 14 (29.2) | ||||
| 2, mild | 29 (30.9) | 3 (12.0) | 12 (57.1) | 14 (29.2) | ||||
| 3, moderate | 11 (11.7) | 4 (16.0) | 5 (23.8) | 2 (4.2) | ||||
| 4, marked | 1 (1.1) | 1 (4.0) | 0 (0.0) | 0 (0.0) | ||||
| Tubular atrophy | 0.001 | 0.005 | 0.253 | 0.008 | ||||
| 0, negative | 34 (36.2) | 11 (44.0) | 4 (19.0) | 19 (39.6) | ||||
| 1, trace | 21 (22.3) | 6 (24.0) | 1 (4.8) | 14 (29.2) | ||||
| 2, mild | 27 (28.7) | 3 (12.0) | 11 (52.4) | 13 (27.1) | ||||
| 3, moderate | 9 (9.6) | 2 (8.0) | 5 (23.8) | 2 (4.2) | ||||
| 4, marked | 3 (3.2) | 3 (12.0) | 0 (0.0) | 0 (0.0) | ||||
| Acute tubular necrosis | 0.815 | >0.999 | >0.999 | >0.999 | ||||
| 0, negative | 84 (89.4) | 22 (88.0) | 18 (85.7) | 44 (91.7) | ||||
| 1, trace | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||||
| 2, mild | 5 (5.3) | 1 (4.0) | 2 (9.5) | 2 (4.2) | ||||
| 3, moderate | 5 (5.3) | 2 (8.0) | 1 (4.8) | 2 (4.2) | ||||
| Arterial intimal hyalinosis | 0.182 | 0.614 | 0.267 | >0.999 | ||||
| 0, negative | 85 (91.4) | 24 (96.0) | 19 (90.5) | 42 (89.4) | ||||
| 1, trace | 7 (7.5) | 0 (0.0) | 2 (9.5) | 5 (10.6) | ||||
| 2, mild | 1 (1.1) | 1 (4.0) | 0 (0.0) | 0 (0.0) | ||||
| 3, moderate | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||||
| Fibrous wall thickening | 0.178 | 0.387 | 0.404 | >0.999 | ||||
| 0, negative | 62 (66.7) | 15 (60.0) | 17 (81.0) | 30 (63.8) | ||||
| 1, trace | 7 (7.5) | 0 (0.0) | 1 (4.8) | 6 (12.8) | ||||
| 2, mild | 15 (16.1) | 7 (28.0) | 1 (4.8) | 7 (14.9) | ||||
| 3, moderate | 8 (8.6) | 2 (8.0) | 2 (9.5) | 4 (8.5) | ||||
| 4, marked | 1 (1.1) | 1 (4.0) | 0 (0.0) | 0 (0.0) | ||||
| Foot process effacement | 0.002 | 0.147 | 0.055 | <0.001 | ||||
| 0, no | 20 (21.7) | 5 (20.8) | 3 (14.3) | 12 (25.5) | ||||
| 1, focal | 28 (30.4) | 5 (20.8) | 1 (4.8) | 22 (46.8) | ||||
| 2, diffuse | 44 (47.8) | 14 (58.3) | 17 (81.0) | 13 (27.7) |
| Adjusted OR (95% Cl) | p Value | |
|---|---|---|
| Hypertension | ||
| No | 1 | |
| Yes | 4.52 (1.07–19.05) | 0.04 |
| Immunosuppressant | ||
| No use | 1 | |
| Use | 7.83 (1.00–61.51) | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chae, Y.; Yoon, H.E.; Chang, Y.K.; Kim, Y.S.; Kim, H.W.; Choi, B.S.; Park, C.W.; Song, H.C.; Kim, Y.O.; Koh, E.S.; et al. Renal Outcome of IgM Nephropathy: A Comparative Prospective Cohort Study. J. Clin. Med. 2021, 10, 4191. https://doi.org/10.3390/jcm10184191
Chae Y, Yoon HE, Chang YK, Kim YS, Kim HW, Choi BS, Park CW, Song HC, Kim YO, Koh ES, et al. Renal Outcome of IgM Nephropathy: A Comparative Prospective Cohort Study. Journal of Clinical Medicine. 2021; 10(18):4191. https://doi.org/10.3390/jcm10184191
Chicago/Turabian StyleChae, Yura, Hye Eun Yoon, Yoon Kyung Chang, Young Soo Kim, Hyung Wook Kim, Bum Soon Choi, Cheol Whee Park, Ho Cheol Song, Young Ok Kim, Eun Sil Koh, and et al. 2021. "Renal Outcome of IgM Nephropathy: A Comparative Prospective Cohort Study" Journal of Clinical Medicine 10, no. 18: 4191. https://doi.org/10.3390/jcm10184191
APA StyleChae, Y., Yoon, H. E., Chang, Y. K., Kim, Y. S., Kim, H. W., Choi, B. S., Park, C. W., Song, H. C., Kim, Y. O., Koh, E. S., & Chung, S. (2021). Renal Outcome of IgM Nephropathy: A Comparative Prospective Cohort Study. Journal of Clinical Medicine, 10(18), 4191. https://doi.org/10.3390/jcm10184191