
Resilience, Emotional Intelligence, and Occupational Performance in Family Members Who Are the Caretakers of Patients with Dementia in Spain: A Cross-Sectional, Analytical, and Descriptive Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Ethical Aspects
2.3. Participants
2.4. Procedure
2.5. Study Variables and Data Collection Instruments
- Sociodemographic variables: sex (man, woman), age, number of children, number of people living at home, marital status (single, married, separated with or without a partner, widowed), educational level (no education, literate, basic, baccalaureate or vocational training, university studies), work outside the home or paid (full/part time, retired-pensioner, unemployed, exclusivity in housework, other).
- Psychosocial variables: relationship with the sick relative (mother, father, others), other people in charge of the caregiver, number of people that the caregiver has under his/her care, age of the patient, hours a day and days a week that they dedicate care, time spent in the situation of caring for the patient, presence of formal support (day center, home help, residence, economic benefit) and/or informal (family, friends, others), knowledge about the family member’s illness and need for more training on it. Living out the experience: whether or not there is a positive perception about living out the experience and feelings that this generates (positive response: feelings of usefulness, love, dedication, gratitude towards the patient, feeling of personal growth, or others. Negative response: overload, physical health problems, mental health problems, others).
- Occupational performance: for the division of occupational performance areas, those based on the Canadian Model of Occupational Performance (C.M.O.P.) [37] were used, classified as Self-Care, Productivity, and Leisure. Each of these areas were evaluated using a Likert-type scale where caregivers responded based on the time spent in each area (1 = not at all, 2 = little, 3 = somewhat, 4 = quite a bit, 5 = a lot). The caregivers were also asked to assess the satisfaction they felt in relation to the time they dedicated by means of a dichotomous answer of yes or no. A sleep assessment was also included, in which the caregivers were asked about the number of hours devoted to sleep per day and for the consideration of having a restful sleep.
2.6. Clinical and Psychological Variables
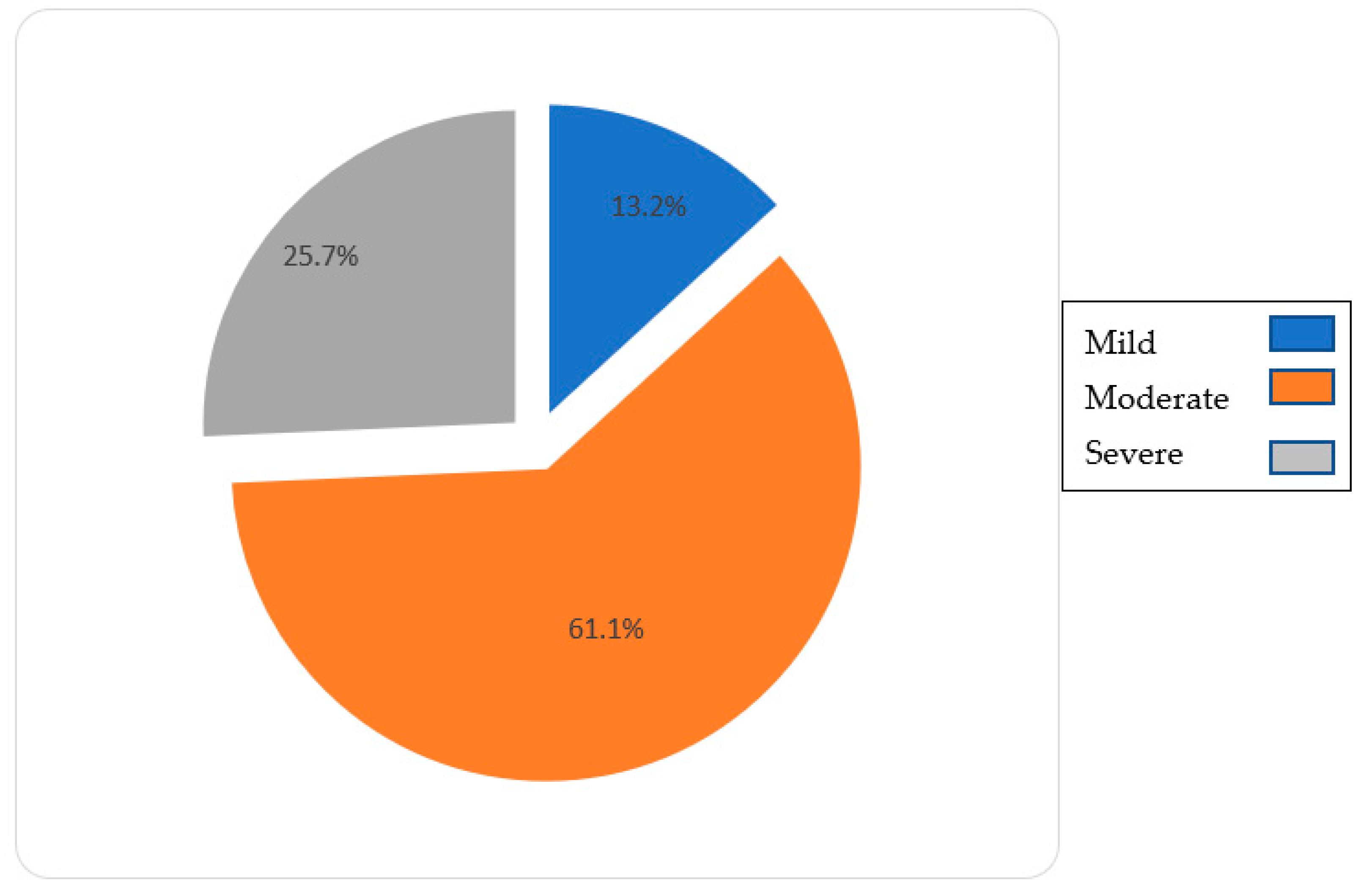
- Diagnosis: Alzheimer’s disease, Vascular Dementia, Lewy body dementia, Frontotemporal dementia, and others, along with the phase of the disease (mild, moderate, and severe). This diagnosis was given by a medical specialist.
- Resilience: the Connor–Davidson Resilience Scale 25 eur (CD-RISC 25eur) was used; official European version translated into Spanish, derived from the original Connor–Davidson Resilience Scale [38]. It was directly purchased from the authors upon request for permission for its use, together with the unpublished manual of the scale [39], revised on 11 January 2015. It is the resilience scale most commonly used [40] in different studies in the same study population, which confirms its validity and reliability [40,41]. It is a tool made up of 25 items that, based on Richardson’s theoretical model [42], comprises five components considered necessary in the assessment of resilience: personal competence, confidence in one’s own intuition and tolerance to adversity, positive acceptance of change, control, and spirituality. The data provided should respond to a situation perceived during the last month, not to a situation experienced at a specific moment. The results fluctuate between 0 and 100; the higher the score, the higher the level or capacity of resilience. Considering the values provided by previous studies [33,40], the cut-off point was established at 74 (coinciding with the fourth quartile) to distinguish the two groups of caregivers: caregivers with high resilience and caregivers with moderate or low resilience.
- Emotional intelligence: the TMMS-24 Emotional Intelligence scale was used, a version adapted to Spanish in 2004 by Fernández et al. [43], from the Trait Meta-Knowledge Scale on Emotional States, Trait Meta-Mood Scale [35], elaborated by the research group of Salovey and Mayer in 1995. It consists of a self-report that evaluates the perception of intrapersonal emotional intelligence. It consists of 24 items distributed in three subscales, Emotional Attention, Emotional Clarity, and Emotional Repair, with eight items each. The cut-off point was established at 79, coinciding with the median, dividing the sample into individuals with high emotional intelligence and individuals with low emotional intelligence.
2.7. Statistical Analysis
3. Results
3.1. Occupational Performance
3.2. Resilience and Emotional Intelligence
3.3. Resilience and Occupational Performance
3.4. Emotional Intelligence and Occupational Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galende, A.V.; Ortiz, M.E.; Velasco, S.L.; Luque, M.L.; Miguel, C.L.D.S.D.; Jurczynska, C.P. Informe de la Fundación del Cerebro. Impacto social de la enfermedad de Alzheimer y otras demencias. Neurología 2017, 36, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Pinto, J.A. La Enfermedad de Alzheimer y Otras Demencias: Detección y Cuidados en Las Personas Mayores; Dirección General de Salud Pública y Alimentación: Madrid, Spain, 2007. [Google Scholar]
- Peña-Longobardo, L.M.; Oliva-Moreno, J. Caregiver Burden in Alzheimer’s Disease Patients in Spain. J. Alzheimer’s Dis. 2014, 43, 1293–1302. [Google Scholar] [CrossRef]
- Grupo de trabajo de la Guía de Práctica Clínica sobre la atención integral a las personas con enfermedad de Alzheimer y otras demencias. Guía de Práctica Clínica Sobre la Atención Integral a Las Personas con Enfermedad de Alzheimer y Otras Demencias: Plan. de Calidad Para el Sistema Nacional de Salud del Ministerio de Sanidad, Política Social e Igualdad; Agência d’lnformació, Avaluació i Qualitat en Salut de Cataluña: Barcelona, Spain, 2010. [Google Scholar]
- National Collaborating Centre for Mental Health. Dementia: The NICE-SCIE Guideline on Supporting People with Dementia and Their Carers in Health and Social Care; The British Psychological Society & The Royal College of Psychiatrists: London, UK, 2007. [Google Scholar]
- Novais, T.; Dauphinot, V.; Krolak-Salmon, P.; Mouchoux, C. How to explore the needs of informal caregivers of individuals with cognitive impairment in Alzheimer’s disease or related diseases? A systematic review of quantitative and qualitative studies. BMC Geriatr. 2017, 17, 86. [Google Scholar] [CrossRef] [Green Version]
- Crespo, M.; López, J. El Apoyo a los Cuidadores de Familiares Mayores Dependientes en el Hogar: Desarrollo del Programa “Cómo mantener su Bienestar”; Instituto de Mayores y Servicios Sociales (IMSERSO): Madrid, Spain, 2007. [Google Scholar]
- Pinquart, M.; Sörensen, S. Differences between caregivers and noncaregivers in psychological health and physical health: A meta-analysis. Psychol. Aging 2003, 18, 250–267. [Google Scholar] [CrossRef] [PubMed]
- Garriga, O.T.; Cors, O.S.; Olmo, J.G.; Pousa, S.L.; Franch, J.V.; Vila, S.M. Distribución factorial de la carga en cuidadores de pacientes con enfermedad de Alzheimer. Red CDPD 2008, 46, 582. [Google Scholar] [CrossRef]
- Arrieta, E.; Fernández, L.; González, V.; Goñi, M.; Guerrero, M.; López, P. Guía de Atención al Paciente con Demencia en Atención Primaria; Gerencia Regional de Salud Junta de Castilla y León: España, Spain, 2007. [Google Scholar]
- Borsje, P.; Wetzels, R.B.; Lucassen, P.L.; Pot, A.M.; Koopmans, R.T. The course of neuropsychiatric symptoms in community-dwelling patients with dementia: A systematic review. Int. Psychogeriatr. 2014, 27, 385–405. [Google Scholar] [CrossRef] [PubMed]
- González, M.; Saucedo, M.C.; Pacheco, I.M.; Carmona, F.; García, A.M.; Calderón, A. El proceso de afrontamiento en cuidadoras familiares de personas con alto grado de dependencia. Psychol. Sci. 2014, 69, 502–513. [Google Scholar]
- Aldana, G.; Guarino, L. Chronic stress, coping and health in caregivers of Alzheimer’s disease patients. Summa Psicológica 2012, 9, 5–14. [Google Scholar]
- García, M.d.M.; Mateo, I.; Gutiérrez, P. Cuidados y Cuidadores en el Sistema Informal de Salud; Escuela Andaluza de Salud Pública e Instituto Andaluz de la Mujer: Granada, Spain, 1999. [Google Scholar]
- García-Calvente, M.D.M.; Mateo-Rodríguez, I.; Maroto-Navarro, G. El impacto de cuidar en la salud y la calidad de vida de las mujeres. Gac. Sanit. 2004, 18, 83–92. [Google Scholar] [CrossRef]
- Martín, M. La Sobrecarga del Cuidador en la Enfermedad de Alzheimer y Otras Demencias [Internet]. Available online: http://www.zonahospitalaria.com/category/zhn27/ (accessed on 7 September 2021).
- Espín, A.M. “Escuela de Cuidadores” como programa psicoeducativo para cuidadores informales de adultos mayores con demencia. Rev. Cub. Salud. Publica 2009, 35, 2. [Google Scholar]
- Rodríguez, A. Sobrecarga Psicofísica en Familiares Cuidadores de Enfermos de Alzheimer. Causas, problemas y soluciones [Internet]. Available online: http://www.gerontalia.com/ (accessed on 7 September 2021).
- Waite, A.; Bebbington, P.; Skelton-Robinson, M.; Orrell, M. Social factors and depression in carers of people with dementia. Int. J. Geriatr. Psychiatry 2004, 19, 582–587. [Google Scholar] [CrossRef]
- Gao, C.; Chapagain, N.Y.; Scullin, M.K. Sleep duration and sleep quality in caregivers of patients with dementia. JAMA Netw. Open 2019, 2, e199891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, R.; Simões-Neto, J.P.; Santos, R.L.; De Sousa, M.F.B.; Baptista, M.A.T.; Lacerda, I.B.; Kimura, N.R.S.; Dourado, M.C.N. Caregivers’ resilience is independent from the clinical symptoms of dementia. Arq. Neuro-Psiquiatr. 2016, 74, 967–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joling, K.J.; Windle, G.; Dröes, R.-M.; Meiland, F.; Van Hout, H.P.; Vroomen, J.M.; Van De Ven, P.M.; Moniz-Cook, E.; Woods, B. Factors of resilience in informal caregivers of people with dementia from integrative international data analysis. Dement. Geriatr. Cogn. Disord. 2016, 42, 198–214. [Google Scholar] [CrossRef]
- Monteiro, A.M.F.; Santos, R.L.; Kimura, N.; Baptista, M.A.T.; Dourado, M.C.N. Coping strategies among caregivers of people with Alzheimer disease: A systematic review. Trends Psychiatry Psychother 2018, 40, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Wilks, S.E.; Croom, B. Perceived stress and resilience in Alzheimer’s disease caregivers: Testing moderation and mediation models of social support. Aging Ment. Health 2008, 12, 357–365. [Google Scholar] [CrossRef] [PubMed]
- García MGimenez, S.I. La inteligencia emocional y sus principales modelos: Propuesta de un modelo integrador. Espiral. Cuad. Del Profr. 2010, 3, 4. [Google Scholar]
- American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and Process, 4th ed.; AOTA Spress: Montgomery, MD, USA, 2020. [Google Scholar]
- Del Castillo, J.A.G.; Del Castillo-López, G.; López-Sánchez, C.; Dias, P.C. Conceptualización teórica de la resiliencia psicosocial y su relación con la salud. Health Addict. Drog. 2016, 16, 59–68. [Google Scholar] [CrossRef]
- Sitges, E.; Bonete, B. Desarrollo de un programa psicoeducativo en la inteligencia emocional para cuidadores principales de enfermos de Alzheimer. Eur. J. Investig. Health Psychol. Educ. 2015, 4, 257–266. [Google Scholar] [CrossRef]
- Colop, V.J.A. Relación Entre Inteligencia Emocional y Resiliencia. (Estudio Realizado con Adultos Jóvenes del Municipio de Cantel Departamento de Quetzaltenango). Ph.D. Thesis, Biblioteca Landivariana-Universidad Rafael Landívar, Quetzaltenango, Guatemala, October 2011. [Google Scholar]
- Martínez, A. Importancia de la Resiliencia e Inteligencia Emocional en el Consumo de Cocaína. Ph.D. Thesis, University of Castilla-La Mancha, Albacete, Spain, 2016. [Google Scholar]
- García-Maroto, S.; López, M.L.; Latorre, J.M. Ansiedad, resiliencia e inteligencia emocional percibida en un grupo de mujeres con cáncer de mama. Ansiedad y Estrés 2015, 21, 115–125. [Google Scholar]
- Palacio, C.G.; Krikorian, A.; Gómez-Romero, M.J.; Limonero, J.T. Resilience in Caregivers: A Systematic Review. Am. J. Hosp. Palliat. Med. 2019, 37, 648–658. [Google Scholar] [CrossRef] [PubMed]
- Durán-Gómez, N.; Guerrero-Martín, J.; Pérez-Civantos, D.; Jurado, C.F.L.; Palomo-López, P.; Cáceres, M.C. Understanding resilience factors among caregivers of people with alzheimer’s disease in Spain. Psychol. Res. Behav. Manag. 2020, 13, 1011–1025. [Google Scholar] [CrossRef]
- Vázquez, F.L.; Otero, P.; Díaz, O.; Sánchez, T.; Pomar, C. Emotional intelligence in women caregivers with depressive symptoms. Psychol. Rep. 2011, 108, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Weaving, J.; Orgeta, V.; Orrell, M.; Petrides, K.V. Predicting anxiety in carers of people with dementia: The role of trait emotional intelligence. Int. Psychogeriatr. 2014, 26, 1201–1209. [Google Scholar] [CrossRef] [Green Version]
- Páez, D.; Fernández, I.; Campos, M.; Zubieta, E.; Casullo, M.M. Apego seguro, vínculos parentales, clima familiar e inteligencia emocional: Socialización, regulación y bienestar. Ansiedad Estrés 2006, 12, 329–341. [Google Scholar]
- Simó, S.; Urbanowski, R. El Modelo Canadiense del Desempeño Ocupacional I. Rev. Gallega Ter. Ocup. TOG 2006, 3, 1–27. [Google Scholar]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Davidson, J.R.T. Connor-Davidson Resilience Scale (CDRISC) Manual. Available online: www.cdrisc.com (accessed on 15 June 2019).
- Fernández, V.; Crespo, M. Resiliencia, personalidad resistente y crecimiento en cuidadores de personas con demencia en el entorno familiar: Una revisión. Clínica Salud 2011, 22, 21–40. [Google Scholar]
- Fernández-Lansac, V.; López, M.C.; Cáceres, R.; Rodríguez-Poyo, M. Resiliencia en cuidadores de personas con demencia: Estudio preliminar. Rev. Española Geriatría Gerontol. 2012, 47, 102–109. [Google Scholar] [CrossRef]
- Richardson, G.E. The metatheory of resilience and resiliency. J. Clin. Psychol. 2002, 58, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Berrocal, P.; Extremera, N.; Ramos, N. Validity and reliability of the spanish modified version of the trait meta-mood scale. Psychol. Rep. 2004, 94, 751–755. [Google Scholar] [CrossRef]
- Salovey, P.; Mayer, J.D.; Goldman, S.L.; Turvey, C.; Palfai, T.P. Emotional Attention, Clarity, and Repair: Exploring Emotional Intelligence Using the Trait Meta-Mood Scale; American Psychological Association: Washington, DC, USA, 1995; pp. 125–154. [Google Scholar] [CrossRef]
- Crespo, M.; Fernández, V.; Soberón, C. Adaptación española de la “Escala de resiliencia de Connor-Davidson” (CD-RISC) en situaciones de estrés crónico. Psicol. Conduct. 2014, 22, 219–238. [Google Scholar]
- Clark, P.C. Effects of individual and family hardiness on caregiver depression and fatigue. Res. Nurs. Health 2002, 25, 37–48. [Google Scholar] [CrossRef]
- Gaugler, J.E.; Kane, R.L.; Newcomer, R. Resilience and transitions from dementia caregiving. J. Gerontol. Ser. B 2007, 62, P38–P44. [Google Scholar] [CrossRef] [Green Version]
- Wilks, S.E.; Vonk, M.E. Private prayer among alzheimer’s caregivers: Mediating burden and resiliency. J. Gerontol. Soc. Work 2008, 50, 113–131. [Google Scholar] [CrossRef]
- Bull, M.J. Strategies for sustaining self used by family caregivers for older adults with dementia. J. Holist. Nurs. 2013, 32, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Donnellan, W.; Bennett, K.M.; Soulsby, L. What are the factors that facilitate or hinder resilience in older spousal dementia carers? A qualitative study. Aging Ment. Health 2014, 19, 932–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deist, M.; Greeff, A. Living with a parent with dementia: A family resilience study. Dementia 2016, 16, 126–141. [Google Scholar] [CrossRef] [PubMed]
- Crespo, M.; Fernández-Lansac, V. Resiliencia en cuidadores familiares de personas mayores dependientes. Ann. Psychol. 2015, 31, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Cerquera, A.M.; Pabón, D.K. Resiliencia y variables asociadas en cuidadores informales de pacientes con alzheimer. Rev. Colomb. Psicol. 2016, 25, 33–46. [Google Scholar] [CrossRef]
- Ross, L.; Holliman, D.; Dixon, D.R. Resiliency in family caregivers: Implications for social work practice. J. Gerontol. Soc. Work 2003, 40, 81–96. [Google Scholar] [CrossRef]
- De Lucena, V.A.M.; Contador, I.; Ramos, F.; Fernández, B.; Hernández, L. Resiliencia y el modelo Burnout-Engagement en cuidadores formales de ancianos. Psicothema 2006, 18, 791–796. [Google Scholar]
- Olmo, J.G.; Pousa, S.L.; Franch, J.V.; Estrada, A.T.; Ferràndiz, M.H.; Gallego, M.L.; Tibau, C.F.; Vidal, O.P.; Muñoz, V.M.; Reina, M.D.M.C. Carga del cuidador y síntomas depresivos en pacientes con enfermedad de Alzheimer. Evolución a los 12 meses. Rev. Neurol. 2002, 34, 601. [Google Scholar] [CrossRef]
- Andrés, L.; Celia, N.-G.; Javier, L.; María, M.-G.; Estefanía, J.-G. Ayuda psicológica a cuidadores en diferentes escenarios. Inf. Psicológica 2013, 105, 60–77. [Google Scholar] [CrossRef]
- Boada, M.; Tárraga, L. La Memoria Está en los Besos; Ediciones Mayo: Barcelona, Spain, 2002. [Google Scholar]
- Gázquez, J.J.; Fuentes, M.D.C.P.; Molero, M.D.M.; Mercader, I. Inteligencia emocional y calidad de vida del cuidador familiar de pacientes con demencia. Rev. Comun. Salud RCyS 1970, 5, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Zijlmans, L.J.M.; Embregts, P.J.C.M.; Gerits, L.; Bosman, A.M.T.; Derksen, J.J.L. Training emotional intelligence related to treatment skills of staff working with clients with intellectual disabilities and challenging behaviour. J. Intellect. Disabil. Res. 2011, 55, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Portal, R. Inteligencia Emocional y Adaptación en Hijas que Cuidan a su Familiar con Demencia. Ph.D. Thesis, University of Granada, Córdoba, Spain, 2009. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Data | ||||
|---|---|---|---|---|
| Percentage(n) | ||||
| Mild | Moderate | Severe | ||
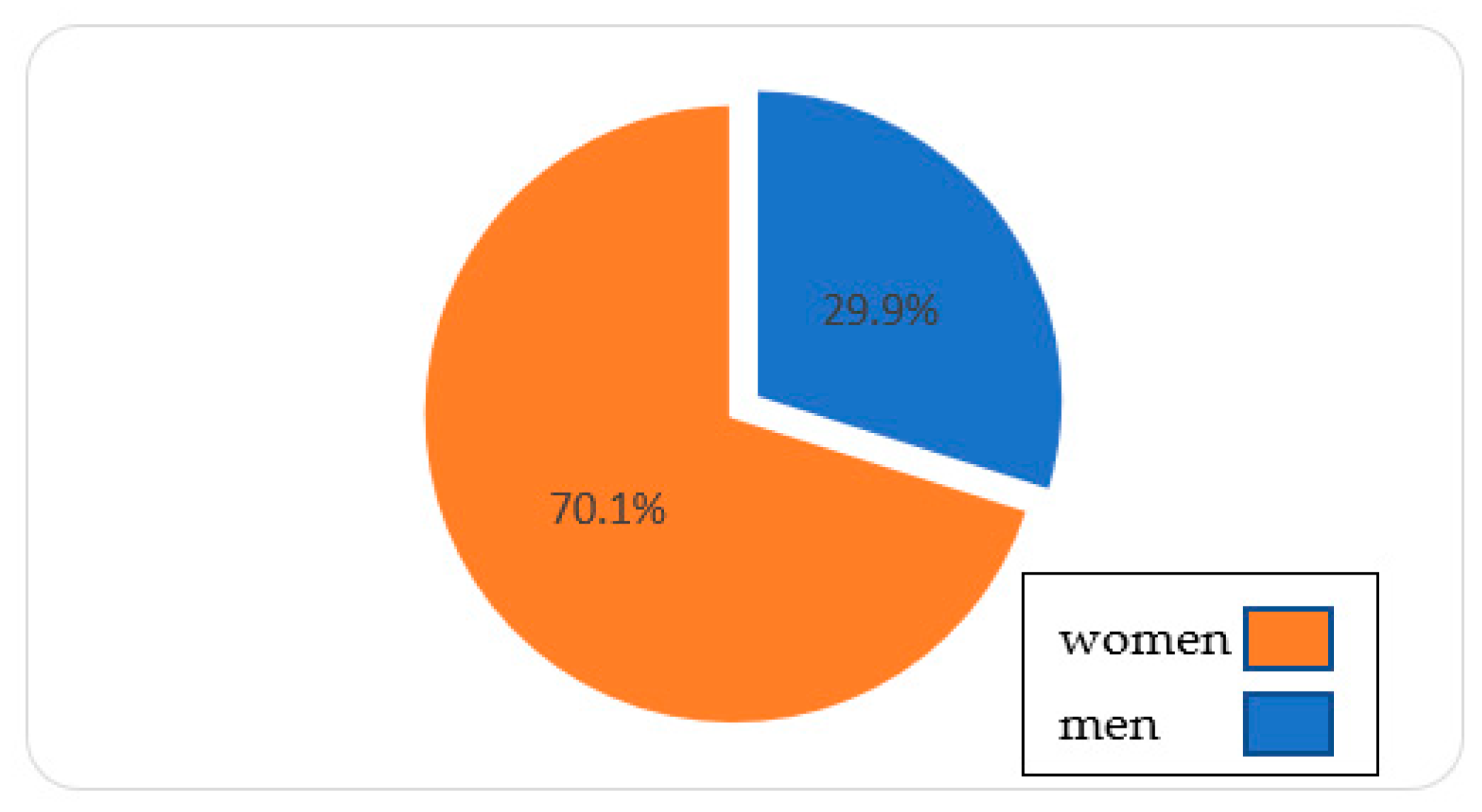
| Sex | Women | 68.5(13) | 70.5(62) | 70.3(26) |
| Men | 31.6(6) | 29.5(26) | 29.7(11) | |
| Level of Studies | Without studies | 5.3(1) | 17.0(15) | 10.8(4) |
| Basic Studies | 63.2(12) | 43.2(38) | 56.8(21) | |
| Baccalaureate | 26.3(5) | 25.0(22) | 13.5(5) | |
| Superior | 5.3(1) | 14.8(13) | 18.9(7) | |
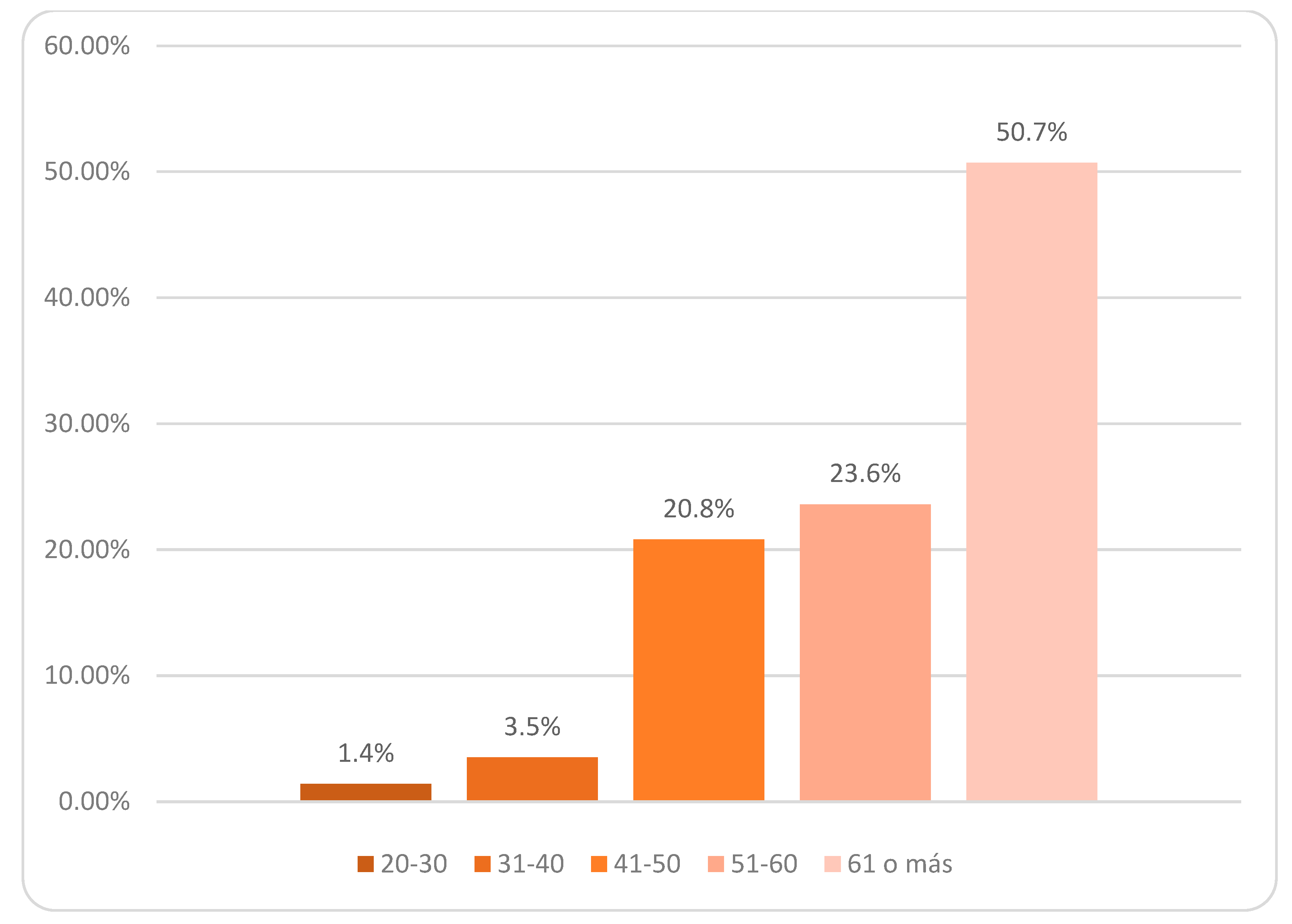
| Age | 20–30 | 5.3(1) | 1.1(1) | 0 |
| 31–40 | 5.3(1) | 2.3(2) | 5.4(2) | |
| 41–50 | 21.1(4) | 20.5(18) | 21.6(8) | |
| 51–60 | 21.1(4) | 25.0(22) | 21.6(8) | |
| 61 or more | 47.4(9) | 51.1(45) | 51.4(19) | |
| Relationship of Family Member With Dementia Patient | Mother | 36.8(7) | 47.7(42) | 40.5(15) |
| Spouse | 36.8(7) | 37.5(33) | 43.2(16) | |
| Father | 15.8(3) | 10.2(9) | 10.8(4) | |
| Father or Mother-in-law | 5.3(1) | 2.3(2) | 0 | |
| Brother or Sister | 5.3(1) | 1.1(1) | 2.7(1) | |
| Grandma or Grandpa | 0 | 1.1(1) | 0 | |
| Neighbor | 0 | 0 | 2.7(1) | |
| Occupational Questionnaire | Percentage(n) | Satisfaction | |
|---|---|---|---|
| Time dedicated to self-care | Not at all | 4.2(6) | 61.1% YES 38.9% NO |
| Little | 21.5(31) | ||
| Somewhat | 29.9(43) | ||
| Quite a bit | 31.9(46) | ||
| A lot | 12.5(18) | ||
| Time dedicated to productivity | Not at all | 4.9(7) | 65.3% YES 34.7% NO |
| Little | 4.2(6) | ||
| Somewhat | 22.9(33) | ||
| Quite a bit | 47.9(69) | ||
| A lot | 20.1(29) | ||
| Time dedicated to leisure activities | Not at all | 20.8(30) | >32.6% YES 67.4% NO |
| Little | 37.5(54) | ||
| Somewhat | 23.6(34) | ||
| Quite a bit | 13.9(20) | ||
| A lot | 4.2(6) | ||
| Sleep | M ± SD | Restful Sleep | |
| Hours of sleep per day | 6.39 ± 1.36 | 40.6% YES 59.4% NO |
| Global Sample | Minimum–Maximum | M ± SD | ||||
|---|---|---|---|---|---|---|
| Emotional Intelligence | 32–120 | 78.48 ± 4.82 | ||||
| Resilience | 28–97 | 64.01 ± 14.5 | ||||
| Phases | Mild Phase | Moderate Phase | Severe Phase | |||
| Min–Max | M ± SD | Min–Max | M ± SD | Min–Max | M ± SD | |
| Emotional Intelligence | 64–120 | 84.47 ± 12.85 | 32–117 | 75.58 ± 15.58 | 49–102 | 79.00 ± 13.96 |
| Resilience | 28–96 | 69.37 ± 14.19 | 28–97 | 62.61 ± 15.51 | 34–83 | 62.53 ± 12.02 |
| Occupational Performance | Resilience CD-RISC 25 | |
|---|---|---|
| r * | p-Value | |
| Global Sample (N = 144) | ||
| Time dedicated to self-care | 0.196 | 0.019 |
| Time dedicated to productivity | 0.091 | 0.278 |
| Time dedicated to leisure activities | 0.172 | 0.040 |
| Dementia in mild phase (N = 19) | ||
| Time dedicated to self-care | −0.036 | 0.882 |
| Time dedicated to productivity | 0.327 | 0.172 |
| Time dedicated to leisure activities | −0.037 | 0.881 |
| Dementia in moderate phase (N = 88) | ||
| Time dedicated to self-care | 0.227 | 0.033 |
| Time dedicated to productivity | −0.045 | 0.679 |
| Time dedicated to leisure activities | 0.262 | 0.014 |
| Dementia in severe phase (N = 37) | ||
| Time dedicated to self-care | 0.214 | 0.210 |
| Time dedicated to productivity | 0.355 | 0.034 |
| Time dedicated to leisure activities | 0.066 | 0.700 |
| Occupational Performance | Emotional Intelligence TMMS-24 | |
|---|---|---|
| r * | p-Value | |
| Global Sample (N = 144) | ||
| Time dedicated to self-care | 0.233 | 0.005 |
| Time dedicated to productivity | 0.056 | 0.508 |
| Time dedicated to leisure activities | 0.073 | 0.387 |
| Dementia in mild phase (N = 19) | ||
| Time dedicated to self-care | 0.093 | 0.705 |
| Time dedicated to productivity | 0.125 | 0.611 |
| Time dedicated to leisure activities | −0.095 | 0.698 |
| Dementia in moderate phase (N = 88) | ||
| Time dedicated to self-care | 0.214 | 0.046 |
| Time dedicated to productivity | 0.026 | 0.807 |
| Time dedicated to leisure activities | 0.103 | 0.340 |
| Dementia in severe phase (N = 37) | ||
| Time dedicated to self-care | 0.398 | 0.016 |
| Time dedicated to productivity | 0.130 | 0.449 |
| Time dedicated to leisure activities | 0.073 | 0.672 |
| Global Sample (N = 144) | |||||||
|---|---|---|---|---|---|---|---|
| Emotional Intelligence | Occupational Performance | ||||||
| Self-Care | Productivity | Leisure Time | |||||
| M ± SD | p-Value * | M ± SD | p-Value * | M ± SD | p-Value * | ||
| Attention | Should improve their attention; gives poor attention | 3.16 ± 1.0 | 0.338 | 3.77 ± 1.0 | 0.553 | 2.30 ± 0.9 | 0.455 |
| Adequate attention | 3.36 ± 1.1 | 3.75 ± 0.9 | 2.55 ± 1.2 | ||||
| Should improve their attention: gives too much attention | 3.50 ± 0.9 | 3.60 ± 0.8 | 2.70 ± 1.5 | ||||
| Clarity | Should improve their clarity | 3.24 ± 1.1 | 0.951 | 3.67 ± 1.0 | 0.451 | 2.50 ± 1.1 | 0.404 |
| Adequate clarity | 3.27 ± 1.1 | 3.74 ± 1.0 | 2.47 ± 1.1 | ||||
| Excellent clarity | 3.38 ± 0.9 | 4.06 ± 0.8 | 2.13 ± 1.1 | ||||
| Repair | Should improve their repair tactics | 3.00 ± 0.9 | 0.075 | 3.87 ± 1.0 | 0.627 | 2.22 ± 1.0 | 0.019 |
| Adequate repair tactics | 3.38 ± 1.2 | 3.68 ± 1.0 | 2.4 ± 1.1 | ||||
| Excellent repair tactics | 3.50 ± 0.9 | 3.75 ± 0.9 | 3.19 ± 1.2 | ||||
| Mild Dementia (N = 19) | |||||||
| Attention | Should improve their attention; gives poor attention | 3.50 ± 0.6 | 0.778 | 3.75 ± 0.5 | 0.752 | 2.75 ± 1.0 | 0.787 |
| Adequate attention | 3.0 ± 1.2 | 3.69 ± 1.1 | 2.38 ± 1.0 | ||||
| Should improve their attention: gives too much attention | 3.50 ± 0.7 | 3.50 ± 0.7 | 2.50 ± 0.7 | ||||
| Clarity | Should improve their clarity | 2.60 ± 1.5 | 0.203 | 3.40 ± 1.3 | 0.306 | 2.80 ± 0.8 | 0.554 |
| Adequate clarity | 3.50 ± 0.7 | 3.67 ± 0.8 | 2.42 ± 0.9 | ||||
| Excellent clarity | 2.50 ± 0.7 | 4.50 ± 0.7 | 2.00 ± 1.4 | ||||
| Repair | Should improve their repair tactics | 3.67 ± 0.6 | 0.614 | 3.67 ± 1.5 | 0.911 | 2.33 ± 0.6 | 0.727 |
| Adequate repair tactics | 3.07 ± 1.1 | 3.67 ± 009 | 2.47 ± 1.0 | ||||
| Excellent repair tactics | 3.00 ** | 4.00 ** | 3.00 ** | ||||
| Moderate Dementia (N = 88) | |||||||
| Attention | Should improve their attention; gives poor attention | 3.24 ± 1.0 | 0.483 | 3.76 ± 1.1 | 0.924 | 2.37 ± 0.9 | 0.266 |
| Adequate attention | 3.47 ± 1.1 | 3.79 ± 0.9 | 2.74 ± 1.2 | ||||
| Should improve their attention: gives too much attention | 3.50 ± 1.3 | 3.75 ± 1.0 | 3.00 ± 1.6 | ||||
| Clarity | Should improve their clarity | 3.39 ± 1.0 | 0.825 | 3.64 ± 1.0 | 0.459 | 2.67 ± 1.1 | 0.639 |
| Adequate clarity | 3.29 ± 1.2 | 3.88 ± 1.0 | 2.48 ± 1.1 | ||||
| Excellent clarity | 3.50 ± 0.9 | 3.80 ± 0.6 | 2.50 ± 1.1 | ||||
| Repair | Should improve their repair tactics | 3.00 ± 0.9 | 0.029 | 3.94 ± 0.9 | 0.506 | 2.34 ± 1.1 | 0.305 |
| Adequate repair tactics | 3.60 ± 1.2 | 3.62 ± 1.1 | 2.62 ± 1.0 | ||||
| Excellent repair tactics | 3.36 ± 0.9 | 3.91 ± 0.7 | 2.91 ± 1.3 | ||||
| Severe Dementia (N = 37) | |||||||
| Attention | Should improve their attention; gives poor attention | 2.89 ± 1.0 | 0.360 | 3.79 ± 1.1 | 0.721 | 2.05 ± 1.1 | 0.963 |
| Adequate attention | 3.38 ± 1.3 | 3.69 ± 1.2 | 2.15 ± 1.2 | ||||
| Should improve their attention: gives too much attention | 3.50 ± 1.0 | 3.50 ± 1.0 | 2.50 ± 1.2 | ||||
| Clarity | Should improve their clarity | 3.08 ± 1.0 | 0.806 | 3.85 ± 0.9 | 0.195 | 1.92 ± 1.0 | 0.138 |
| Adequate clarity | 3.11 ± 1.2 | 3.47 ± 1.2 | 2.47 ± 1.3 | ||||
| Excellent clarity | 3.50 ± 1.3 | 4.50 ± 1.0 | 1.25 ± 0.5 | ||||
| Repair | Should improve their repair tactics | 2.80 ± 0.9 | 0.184 | 3.70 ± 1.3 | 0.546 | 1.80 ± 0.6 | 0.014 |
| Adequate repair tactics | 3.14 ± 1.2 | 3.82 ± 1.0 | 1.95 ± 1.2 | ||||
| Excellent repair tactics | 4.00 ± 0.8 | 3.25 ± 1.3 | 4.00 ± 1.2 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Trinidad, M.N.; Chimpén-López, C.A.; Rodríguez-Santos, L.; Moral, M.A.; Rodríguez-Mansilla, J. Resilience, Emotional Intelligence, and Occupational Performance in Family Members Who Are the Caretakers of Patients with Dementia in Spain: A Cross-Sectional, Analytical, and Descriptive Study. J. Clin. Med. 2021, 10, 4262. https://doi.org/10.3390/jcm10184262
Gómez-Trinidad MN, Chimpén-López CA, Rodríguez-Santos L, Moral MA, Rodríguez-Mansilla J. Resilience, Emotional Intelligence, and Occupational Performance in Family Members Who Are the Caretakers of Patients with Dementia in Spain: A Cross-Sectional, Analytical, and Descriptive Study. Journal of Clinical Medicine. 2021; 10(18):4262. https://doi.org/10.3390/jcm10184262
Chicago/Turabian StyleGómez-Trinidad, María Nieves, Carlos Alexis Chimpén-López, Laura Rodríguez-Santos, Manuel Alfredo Moral, and Juan Rodríguez-Mansilla. 2021. "Resilience, Emotional Intelligence, and Occupational Performance in Family Members Who Are the Caretakers of Patients with Dementia in Spain: A Cross-Sectional, Analytical, and Descriptive Study" Journal of Clinical Medicine 10, no. 18: 4262. https://doi.org/10.3390/jcm10184262
APA StyleGómez-Trinidad, M. N., Chimpén-López, C. A., Rodríguez-Santos, L., Moral, M. A., & Rodríguez-Mansilla, J. (2021). Resilience, Emotional Intelligence, and Occupational Performance in Family Members Who Are the Caretakers of Patients with Dementia in Spain: A Cross-Sectional, Analytical, and Descriptive Study. Journal of Clinical Medicine, 10(18), 4262. https://doi.org/10.3390/jcm10184262