
Implicit and Explicit Memory in Youths with High-Functioning Autism Spectrum Disorder: A Case-Control Study

 , , and
, , and 
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Implicit Memory Serial Reaction Time Task
2.2.2. Explicit Memory Serial Reaction Time Task
2.3. Statistical Analyses
3. Results
3.1. Demographics
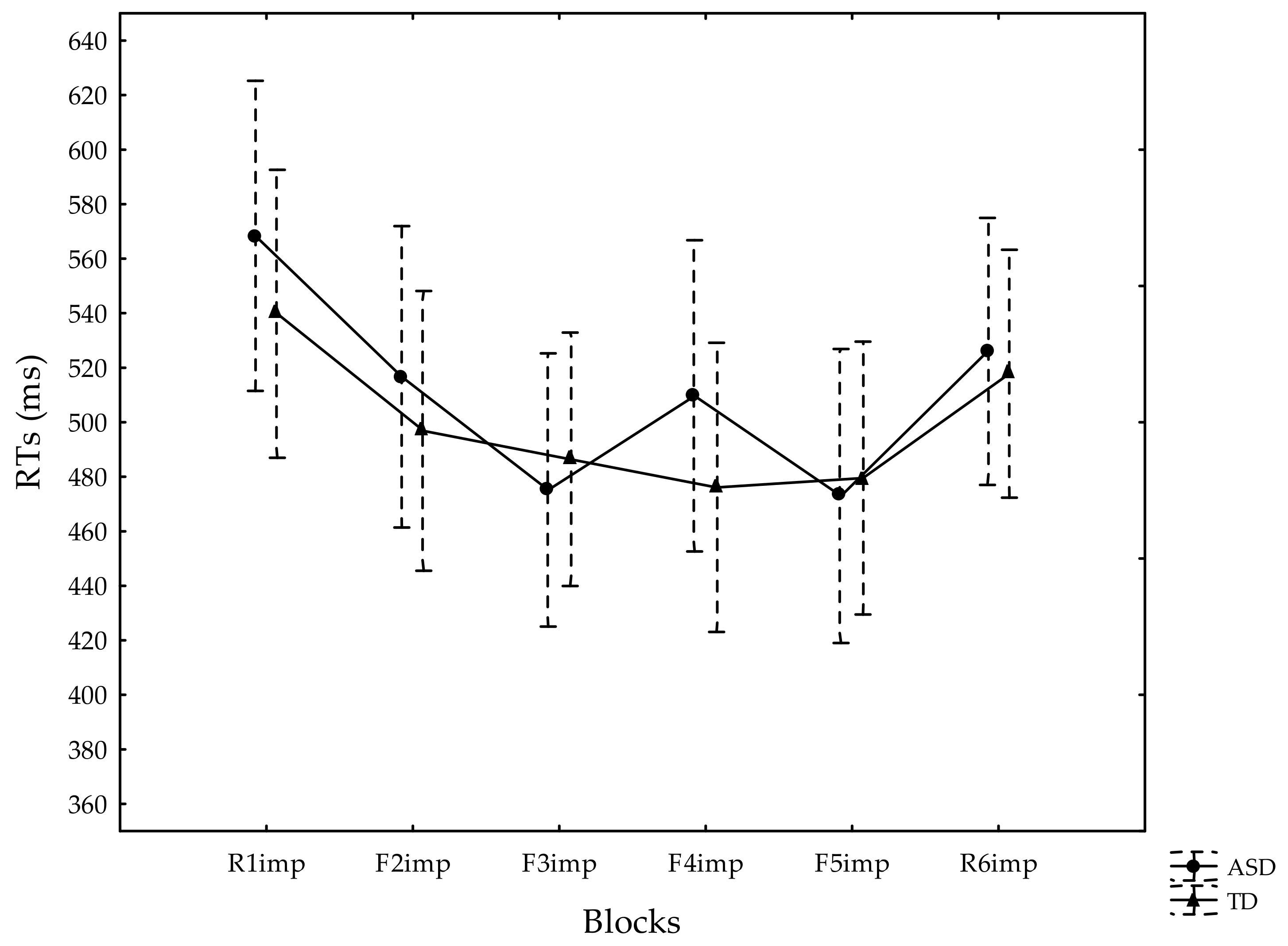
3.2. Implicit Memory Serial Reaction Time Task
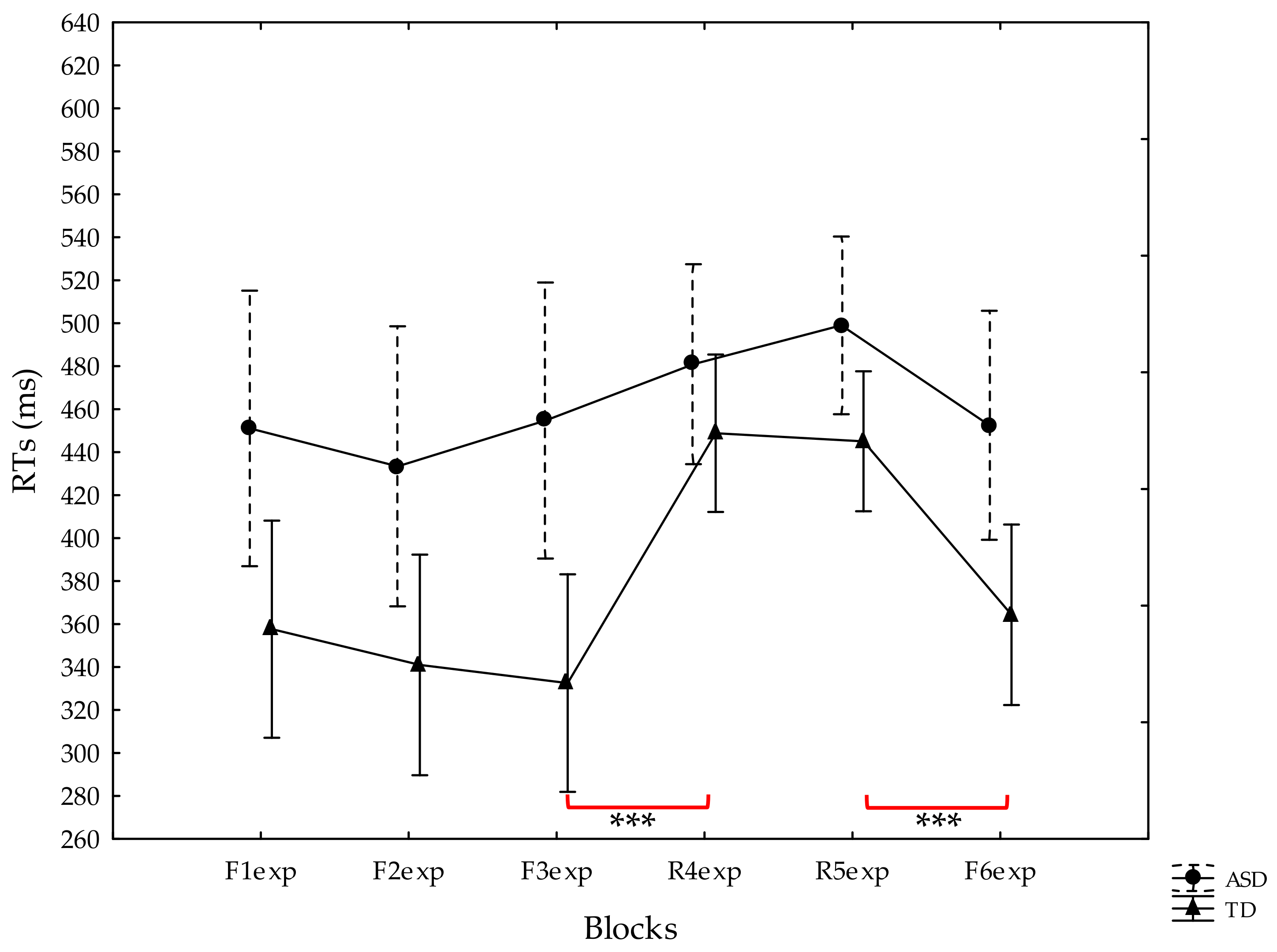
3.3. Explicit Memory Serial Reaction Time Task
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2016. MMWR Surveill Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- Narzisi, A.; Posada, M.; Barbieri, F.; Chericoni, N.; Ciuffolini, D.; Pinzino, M.; Romano, R.; Scattoni, M.; Tancredi, R.; Calderoni, S.; et al. Prevalence of autism spectrum disorder in a large Italian catchment area: A school-based population study within the ASDEU project. Epidemiol. Psychiatr. Sci. 2018, 29, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Chen, S.; Pang, N.; Deng, X.; Yang, L.; He, F.; Wu, L.; Chen, C.; Yin, F.; Peng, J. Neurological diseases with autism spectrum disorder: Role of ASD risk genes. Front. Neurosci. 2019, 13, 349. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.-C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Robertson, C.E.; Baron-Cohen, S. Sensory perception in autism. Nat. Rev. Neurosci. 2017, 18, 671–684. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Ashwin, E.; Ashwin, C.; Tavassoli, T.; Chakrabarti, B. Talent in autism: Hyper-systemizing, hyper-attention to detail and sensory hypersensitivity. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 1377–1383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mottron, L.; Dawson, M.; Soulières, I.; Hubert, B.; Burack, J. Enhanced perceptual functioning in autism: An update, and eight principles of autistic perception. J. Autism Dev. Disord. 2006, 36, 27–43. [Google Scholar] [CrossRef] [PubMed]
- Boucher, J.; Mayes, A.; Bigham, S. Memory in autistic spectrum disorder. Psychol. Bull. 2012, 138, 458–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, H.; Israeli, D.; Minshew, N.; Bonneh, Y.; Heeger, D.J.; Behrmann, M.; Sagi, D. Perceptual learning in autism: Over-specificity and possible remedies. Nat. Neurosci. 2015, 18, 1574–1576. [Google Scholar] [CrossRef]
- Marko, M.K.; Crocetti, D.; Hulst, T.; Donchin, O.; Shadmehr, R.; Mostofsky, S.H. Behavioural and neural basis of anomalous motor learning in children with autism. Brain 2015, 138, 784–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Zhang, Y.-B.; Liu, L.-L.; Cui, J.-F.; Wang, J.; Shum, D.H.K.; Van Amelsvoort, T.; Chan, R.C.K. A meta-analysis of working memory impairments in autism spectrum disorders. Neuropsychol. Rev. 2017, 27, 46–61. [Google Scholar] [CrossRef] [PubMed]
- Demetriou, E.A.; DeMayo, M.; Guastella, A.J. Executive function in autism spectrum disorder: History, theoretical models, empirical findings, and potential as an endophenotype. Front. Psychiatry 2019, 10, 753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, C.L.E.; Lau, Z.; Lui, S.S.Y.; Lok, E.; Tam, V.; Chan, Q.; Cheng, K.M.; Lam, S.M.; Cheung, E.F.C. Meta-analysis of neuropsychological measures of executive functioning in children and adolescents with high-functioning autism spectrum disorder. Autism Res. 2016, 10, 911–939. [Google Scholar] [CrossRef] [PubMed]
- Demetriou, E.A.; Lampit, A.; Quintana, D.S.; Naismith, S.; Song, Y.J.C.; Pye, J.E.; Hickie, I.; Guastella, A.J. Autism spectrum disorders: A meta-analysis of executive function. Mol. Psychiatry 2017, 23, 1198–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, W.; Ornstein, P.A. Determinants of memory development in childhood and adolescence. Int. J. Psychol. 2018, 54, 307–315. [Google Scholar] [CrossRef]
- Bennetto, L.; Pennington, B.F.; Rogers, S.J. Intact and impaired memory functions in autism. Child. Dev. 1996, 67, 1816–1835. [Google Scholar] [CrossRef]
- Seger, C.A. Implicit learning. Psychol. Bull. 1994, 115, 163–196. [Google Scholar] [CrossRef]
- Shanks, D.R. Implicit Learning. In Handbook of Cognition; Lamberts, K., Goldstone, R., Eds.; Sage Publications: London, UK, 2005; pp. 202–220. [Google Scholar]
- Perruchet, P.; Pacton, S. Implicit learning and statistical learning: One phenomenon, two approaches. Trends Cogn. Sci. 2006, 10, 233–238. [Google Scholar] [CrossRef]
- Conway, C.M.; Bauernschmidt, A.; Huang, S.S.; Pisoni, D.B. Implicit statistical learning in language processing: Word predictability is the key. Cognition 2010, 114, 356–371. [Google Scholar] [CrossRef] [Green Version]
- Kidd, E. Implicit statistical learning is directly associated with the acquisition of syntax. Dev. Psychol. 2012, 48, 171–184. [Google Scholar] [CrossRef] [Green Version]
- Funke, J.; Frensch, P.A. Complex Problem Solving: The European Perspective—10 Years After. In Learning to Solve Complex Scientific Problems; Jonassen, D.H., Ed.; Erlbaum: New York, NY, USA, 2007; pp. 25–47. [Google Scholar]
- Reber, A.S. Implicit learning and tacit knowledge. J. Exp. Psychol. Gen. 1969, 118, 219–235. [Google Scholar] [CrossRef]
- Kaufman, S.B.; DeYoung, C.G.; Gray, J.R.; Jiménez, L.; Brown, J.; Mackintosh, N. Implicit learning as an ability. Cognition 2010, 116, 321–340. [Google Scholar] [CrossRef]
- Vicari, S.; Piccini, G.; Mercuri, E.; Battini, R.; Chieffo, D.; Bulgheroni, S.; Pecini, C.; Lucibello, S.; Lenzi, S.; Moriconi, F.; et al. Implicit learning deficit in children with Duchenne muscular dystrophy: Evidence for a cerebellar cognitive impairment? PLoS ONE 2018, 13, e0191164. [Google Scholar] [CrossRef] [Green Version]
- Vicari, S.; Bellucci, S.; Carlesimo, G.A. Procedural learning deficit in children with Williams syndrome. Neuropsychologia 2001, 39, 665–677. [Google Scholar] [CrossRef]
- Gheysen, F.; Van Waelvelde, H.; Fias, W. Impaired visuo-motor sequence learning in Developmental Coordination Disorder. Res. Dev. Disabil. 2011, 32, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Vicari, S.; Marotta, L.; Menghini, D.; Molinari, M.; Petrosini, L. Implicit learning deficit in children with developmental dyslexia. Neuropsychologia 2002, 41, 108–114. [Google Scholar] [CrossRef]
- Vicari, S.; Finzi, A.; Menghini, D.; Marotta, L.; Baldi, S.; Petrosini, L. Do children with developmental dyslexia have an implicit learning deficit? J. Neurol. Neurosurg. Psychiatry 2005, 76, 1392–1397. [Google Scholar] [CrossRef] [Green Version]
- Menghini, D.; Hagberg, G.E.; Caltagirone, C.; Petrosini, L.; Vicari, S. Implicit learning deficits in dyslexic adults: An fMRI study. NeuroImage 2006, 33, 1218–1226. [Google Scholar] [CrossRef]
- Lum, J.A.G.; Clark, G.M. Implicit manual and oculomotor sequence learning in developmental language disorder. Dev. Sci. 2021, e13156. [Google Scholar] [CrossRef]
- Zwart, F.S.; Vissers, C.T.; Kessels, R.P.; Maes, J.H. Implicit learning seems to come naturally for children with autism, but not for children with specific language impairment: Evidence from behavioral and ERP data. Autism Res. 2018, 11, 1050–1061. [Google Scholar] [CrossRef] [Green Version]
- Eichenbaum, H. The Cognitive Neuroscience of Memory: An Introduction, 2nd ed.; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Reber, P.J. The neural basis of implicit learning and memory: A review of neuropsychological and neuroimaging research. Neuropsychologia 2013, 51, 2026–2042. [Google Scholar] [CrossRef]
- Wyatt, B.S.; Conners, F.A. Implicit and explicit memory in individuals with mental retardation. Am. J. Ment. Retard. 1998, 102, 511–526. [Google Scholar] [CrossRef]
- Atwell, J.A.; Conners, F.A.; Merrill, E.C. Implicit and explicit learning in young adults with mental retardation. Am. J. Ment. Retard. 2003, 108, 56–68. [Google Scholar] [CrossRef]
- Lee, J.C. Episodic memory retrieval in adolescents with and without developmental language disorder (DLD). Int. J. Lang. Commun. Disord. 2017, 53, 271–281. [Google Scholar] [CrossRef]
- Andersen, P.N.; Egeland, J.; Øie, M. Learning and memory impairments in children and adolescents with attention-deficit/hyperactivity disorder. J. Learn. Disabil. 2012, 46, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Mostofsky, S.H.; Goldberg, M.C.; Landa, R.J.; Denckla, M.B. Evidence for a deficit in procedural learning in children and adolescents with autism: Implications for cerebellar contribution. J. Int. Neuropsychol. Soc. 2000, 6, 752–759. [Google Scholar] [CrossRef]
- Gaigg, S.B.; Bowler, D. Differential fear conditioning in Asperger’s syndrome: Implications for an amygdala theory of autism. Neuropsychologia 2007, 45, 2125–2134. [Google Scholar] [CrossRef] [PubMed]
- Schipul, S.E.; Just, M.A. Diminished neural adaptation during implicit learning in autism. NeuroImage 2015, 125, 332–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, R.M.; Tarpey, T.; Hamo, A.; Carberry, C.; Brouwer, G.; Lord, C. Statistical learning is associated with autism symptoms and verbal abilities in young children with autism. J. Autism Dev. Disord. 2018, 48, 3551–3561. [Google Scholar] [CrossRef]
- Katz-Nave, G.; Adini, Y.; Hetzroni, O.E.; Bonneh, Y.S. Sequence learning in minimally verbal children with ASD and the beneficial effect of vestibular stimulation. Autism Res. 2019, 13, 320–337. [Google Scholar] [CrossRef]
- Travers, B.G.; Klinger, M.R.; Mussey, J.L.; Klinger, L.G. Motor-linked implicit learning in persons with autism spectrum disorders. Autism Res. 2010, 3, 68–77. [Google Scholar] [CrossRef]
- Foti, F.I.; De Crescenzo, F.; Vivanti, G.; Menghini, D.; Vicari, S. Implicit learning in individuals with autism spectrum disorders: A meta-analysis. Psychol. Med. 2014, 45, 897–910. [Google Scholar] [CrossRef] [PubMed]
- Izadi-Najafabadi, S.; Mirzakhani-Araghi, N.; Miri-Lavasani, N.; Nejati, V.; Pashazadeh-Azari, Z. Implicit and explicit motor learning: Application to children with Autism Spectrum Disorder (ASD). Res. Dev. Disabil. 2015, 47, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Obeid, R.; Brooks, P.; Powers, K.L.; Gillespie-Lynch, K.; Lum, J.A. Statistical learning in specific language impairment and autism spectrum disorder: A meta-analysis. Front. Psychol. 2016, 7, 1245. [Google Scholar] [CrossRef] [PubMed]
- Clark, G.M.; Lum, J.A.G. Procedural learning in Parkinson’s disease, specific language impairment, dyslexia, schizophrenia, developmental coordination disorder, and autism spectrum disorders: A second-order meta-analysis. Brain Cogn. 2017, 117, 41–48. [Google Scholar] [CrossRef]
- Haebig, E.; Saffran, J.R.; Weismer, S.E. Statistical word learning in children with autism spectrum disorder and specific language impairment. J. Child. Psychol. Psychiatry 2017, 58, 1251–1263. [Google Scholar] [CrossRef]
- Boucher, J.; Mayes, A. Memory in ASD: Have we been barking up the wrong tree? Autism 2012, 16, 603–611. [Google Scholar] [CrossRef]
- Klinger, L.G.; Klinger, M.R.; Pohlig, R.L. Implicit Learning Impairments in Autism Spectrum Disorders. In New Developments in Autism: The Future is Today; Perez, J.M., Gonzalez, P.M., Com, M.L., Nieto, C., Eds.; Jessica Kingsley: London, UK, 2007; pp. 76–103. [Google Scholar]
- Ullman, M.T.; Pullman, M.Y. A compensatory role for declarative memory in neurodevelopmental disorders. Neurosci. Biobehav. Rev. 2015, 51, 205–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, K.; Ikeda, H.; Miyao, M. Learning eYcacy of explicit visuomotor sequences in children with attention-deWcit/hyperactivity disorder and Asperger syndrome. Exp. Brain Res. 2010, 203, 233–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowler, D.M.; Matthews, N.J.; Gardiner, J.M. Asperger’s syndrime and memory: Similarity to autism but not amnesia. Neuropsychologia 1997, 35, 65–70. [Google Scholar] [CrossRef]
- Gardiner, J.M.; Bowler, D.M.; Grice, S.J. Further evidence of preserved priming and impaired recall in adults with Asperger’s syndrome. J. Autism Dev. Disord. 2003, 33, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Hedley, D.; Young, R.; Brewer, N. Using eye movements as an index of implicit face recognition in autism spectrum disorder. Autism Res. 2012, 5, 363–379. [Google Scholar] [CrossRef]
- Bowler, D.M.; Gaigg, S.B.; Lind, S.E. Memory in Autism: Binding, Self and Brain. In Researching the Autism Spectrum: Contemporary Perspectives; Cambridge University Press: Cambridge, UK, 2011; pp. 316–346. [Google Scholar]
- Bruck, M.; London, K.; Landa, R.; Goodman, J. Autobiographical memory and suggestibility in children with autism spectrum disorder. Dev. Psychopathol. 2007, 19, 73–95. [Google Scholar] [CrossRef] [PubMed]
- Goddard, L.; Howlin, P.; Dritschel, B.; Patel, T. Autobiographical memory and social problem-solving in Asperger syndrome. J. Autism Dev. Disord. 2007, 37, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Crane, L.; Pring, L.; Jukes, K.; Goddard, L. Patterns of autobiographical memory in adults with autism spectrum disorder. J. Autism Dev. Disord. 2012, 42, 2100–2112. [Google Scholar] [CrossRef] [PubMed]
- Nissen, M.J.; Bullemer, P. Attentional requirements of learning: Evidence from performance measures. Cogn. Psychol. 1987, 19, 1–32. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S.L. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2) Manual (Part. 1): Modules 1–4; Western Psychological Services: Torrence, CA, USA, 2012. [Google Scholar]
- Roid, G.H.; Miller, L.J.; Pomplun, M.; Koch, C. Leiter International Performance Scale, Third Edition (Leiter-3); Cornoldi, C., Giofrè, D., Belacchi, C., Eds.; Italian ed.; Western Psychological Services: Los Angeles, CA, USA; Giunti Organizzazioni Speciali: Florence, Italy, 2013. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children, 4th Edition (WISC-IV); Orsini, A., Pezzuti, L., Picone, L., Eds.; Italian ed.; Psychological Corporation: San Antonio, TX, USA; Giunti Organizzazioni Speciali: Florence, Italy, 2003. [Google Scholar]
- Vicari, S.; Verucci, L.; Carlesimo, G.A. Implicit memory is independent from IQ and age but not from etiology: Evidence from Down and Williams syndromes. J. Intellect. Disabil. Res. 2007, 51, 932–941. [Google Scholar] [CrossRef]
- Travers, B.G.; Kana, R.K.; Klinger, L.G.; Klein, C.L.; Klinger, M.R. Motor learning in individuals with autism spectrum disorder: Activation in superior parietal lobule related to learning and repetitive behaviors. Autism Res. 2014, 8, 38–51. [Google Scholar] [CrossRef]
- Sharer, E.A.; Mostofsky, S.H.; Pascual-Leone, A.; Oberman, L.M. Isolating visual and proprioceptive components of motor sequence learning in ASD. Autism Res. 2015, 9, 563–569. [Google Scholar] [CrossRef] [Green Version]
- Vicari, S.; Bellucci, S.; Carlesimo, G.A. Implicit and explicit memory: A functional dissociation in persons with Down syndrome. Neuropsychologia 2000, 38, 240–251. [Google Scholar] [CrossRef]
- Willingham, D.B.; Nissen, M.J.; Bullemer, P. On the development of procedural knowledge. J. Exp. Psychol. Learn. Mem. Cogn. 1989, 15, 1047–1060. [Google Scholar] [CrossRef]
- Chun, M.M.; Jiang, Y. Contextual cueing: Implicit learning and memory of visual context guides spatial attention. Cognit. Psychol. 1998, 36, 28–71. [Google Scholar] [CrossRef] [Green Version]
- Eslinger, P.; Damasio, A.R. Preserved motor learning in Alzheimer’s disease: Implications for anatomy and behavior. J. Neurosc. 1986, 6, 3006–3009. [Google Scholar] [CrossRef] [Green Version]
- Heindel, W.; Salmon, D.; Shults, C.; Walicke, P.; Butters, N. Neuropsychological evidence for multiple implicit memory systems: A comparison of Alzheimer’s, Huntington’s, and Parkinson’s disease patients. J. Neurosc. 1989, 9, 582–587. [Google Scholar] [CrossRef]
- Gabrieli, J.D.; Stebbins, G.T.; Singh, J.; Willingham, D.B.; Goetz, C.G. Intact mirror-tracing and impaired rotary pursuit skill learning in patients with Huntington’s disease: Evidence for dissociable memory systems in skill learning. Neuropsychology 1989, 11, 272–281. [Google Scholar] [CrossRef]
- Miller, G.A. Free recall of redundant strings of letters. J. Exp. Psychol. 1958, 56, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Reber, A.S. Implicit learning of artificial grammars. J. Verbal Learn. Verbal Behav. 1967, 6, 855–863. [Google Scholar] [CrossRef]
- Saffran, J.R.; Aslin, R.N.; Newport, E.L. Statistical learning by 8-month-old infants. Science 1996, 13, 1926–1928. [Google Scholar] [CrossRef] [Green Version]
- Fiser, J.; Aslin, R.N. Unsupervised statistical learning of higher- order spatial structures from visual scenes. Psychol. Sci. 2001, 12, 499–504. [Google Scholar] [CrossRef]
- Estes, W.K.; Burke, C.J.; Atkinson, R.C.; Frankmann, J.P. Probabilistic discrimination learning. J. Exp. Psychol. 1957, 54, 233–239. [Google Scholar] [CrossRef]
- Vivanti, G.; Barbaro, J.; Hudry, K.; Dissanayake, C.; Prior, M. Intellectual development in autism spectrum disorders: New insights from longitudinal studies. Front. Hum. Neurosci. 2013, 7, 354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vivanti, G.; Dissanayake, C. Propensity to imitate in autism is not modulated by the model’s gaze direction: An eye-tracking study. Autism Res. 2014, 7, 392–399. [Google Scholar] [CrossRef]
- Vivanti, G.; Rogers, S.J. Autism and the mirror neuron system: Insights from learning and teaching. Philos. Trans. R Soc. Lond. B Biol. Sci. 2014, 369, 20130184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruffman, T.; Taumoepeau, M.; Perkins, C. Statistical learning as a basis for social understanding in children. Br. J. Dev. Psychol. 2011, 30, 87–104. [Google Scholar] [CrossRef] [PubMed]
- Monroy, C.; Meyer, M.; Gerson, S.; Hunnius, S. Statistical learning in social action contexts. PLoS ONE 2017, 5, e0177261. [Google Scholar] [CrossRef] [PubMed]
- Callenmark, B.; Kjellin, L.; Rönnqvist, L.; Bölte, S. Explicit versus implicit social cognition testing in autism spectrum disorder. Autism 2013, 18, 684–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guivarch, J.; Murdymootoo, V.; Elissalde, S.-N.; Salle-Collemiche, X.; Tardieu, S.; Jouve, E.; Poinso, F. Impact of an implicit social skills training group in children with autism spectrum disorder without intellectual disability: A before-and-after study. PLoS ONE 2017, 12, e0181159. [Google Scholar] [CrossRef] [Green Version]
- Masi, A.; DeMayo, M.; Glozier, N.; Guastella, A.J. An overview of autism spectrum disorder, heterogeneity and treatment options. Neurosci. Bull. 2017, 33, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Boucher, J.; Bowler, D.M. Memory in Autism: Theory and Evidence; Cambridge University Press: Cambridge, UK, 2008. [Google Scholar]
- Cooper, R.A.; Simons, J.S. Exploring the neurocognitive basis of episodic recollection in autism. Psychon. Bull. Rev. 2018, 26, 163–181. [Google Scholar] [CrossRef]
- Greimel, E.; Nehrkorn, B.; Fink, G.R.; Kukolja, J.; Kohls, G.; Müller, K.; Piefke, M.; Kamp-Becker, I.; Remschmidt, H.; Herpertz-Dahlmann, B.; et al. Neural mechanisms of encoding social and non-social context information in autism spectrum disorder. Neuropsychologia 2012, 50, 3440–3449. [Google Scholar] [CrossRef]
- Cooper, R.; Richter, F.R.; Bays, P.M.; Plaisted-Grant, K.C.; Baron-Cohen, S.; Simons, J.S. Reduced hippocampal functional connectivity during episodic memory retrieval in autism. Cereb. Cortex 2017, 27, 888–902. [Google Scholar] [CrossRef] [Green Version]
- Bowler, D.M.; Gaigg, S.B.; Gardiner, J.M. Binding of multiple features in memory by high-functioning adults with autism spectrum disorder. J. Autism Dev. Disord. 2014, 44, 2355–2362. [Google Scholar] [CrossRef] [PubMed]
- Roelofs, R.L.; Visser, E.M.; Berger, H.J.C.; Prins, J.B.; Van Schrojenstein Lantman-De Valk, H.M.J.; Teunisse, J.P. Executive functioning in individuals with intellectual disabilities and autism spectrum disorders. J. Intellect. Disabil. Res. 2015, 59, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Durrleman, S.; Franck, J. Exploring links between language and cognition in autism spectrum disorders: Complement sentences, false belief, and executive functioning. J. Commun. Disord. 2015, 54, 15–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corbett, B.A.; Constantine, L.J.; Hendren, R.; Rocke, D.; Ozonoff, S. Examining executive functioning in children with autism spectrum disorder, attention deficit hyperactivity disorder and typical development. Psychiatry Res. 2009, 166, 210–222. [Google Scholar] [CrossRef] [Green Version]
- Kado, Y.; Sanada, S.; Yanagihara, M.; Ogino, T.; Ohno, S.; Watanabe, K.; Nakano, K.; Morooka, T.; Oka, M.; Ohtsuka, Y. Executive function in children with pervasive developmental disorder and attention-deficit/hyperactivity disorder assessed by the Keio version of the Wisconsin card sorting test. Brain Dev. 2012, 34, 354–359. [Google Scholar] [CrossRef]
- Friedman, N.P.; Miyake, A. The relations among inhibition and interference control functions: A latent variable analysis. J. Exp. Psychol. Gen. 2004, 133, 101–135. [Google Scholar] [CrossRef] [Green Version]
- Geurts, H.M.; Bergh, S.F.W.M.V.D.; Ruzzano, L. Prepotent response inhibition and interference control in autism spectrum disorders: Two meta-analyses. Autism Res. 2014, 7, 407–420. [Google Scholar] [CrossRef] [Green Version]
- Habib, A.; Harris, L.; Pollick, F.; Melville, C. A meta-analysis of working memory in individuals with autism spectrum disorders. PLoS ONE 2019, 14, e0216198. [Google Scholar] [CrossRef] [Green Version]
- Del Vecchio, N.; Liporace, J.; Nei, M.; Sperling, M.; Tracy, J. A dissociation between implicit and explicit verbal memory in left temporal lobe epilepsy. Epilepsia 2004, 45, 1124–1133. [Google Scholar] [CrossRef]
- Jiménez-Fernández, G.; Vaquero, J.M.M.; Jiménez, L.; Defior, S. Dyslexic children show deficits in implicit sequence learning, but not in explicit sequence learning or contextual cueing. Ann. Dyslexia 2010, 61, 85–110. [Google Scholar] [CrossRef]
- Schuchard, J.; Thompson, C.K. Implicit and explicit learning in individuals with agrammatic aphasia. J. Psycholinguist. Res. 2013, 43, 209–224. [Google Scholar] [CrossRef]
- Zachor, D.A.; Vardi, S.; Baron-Eitan, S.; Brodai-Meir, I.; Ginossar, N.; Ben-Itzchak, E. The effectiveness of an outdoor adventure programme for young children with autism spectrum disorder: A controlled study. Dev. Med. Child. Neurol. 2016, 59, 550–556. [Google Scholar] [CrossRef]
- Marro, B.M.; Kang, E.; Hauschild, K.M.; Normansell, K.M.; Abu-Ramadan, T.M.; Lerner, M.D. Social performance-based interventions promote gains in social knowledge in the absence of explicit training for youth with autism spectrum disorder. Bull. Menn. Clin. 2019, 83, 301–325. [Google Scholar] [CrossRef]
- Kamps, D.; Thiemann-Bourque, K.; Heitzman-Powell, L.; Schwartz, I.; Rosenberg, N.; Mason, R.; Cox, S. A comprehensive peer network intervention to improve social communication of children with autism spectrum disorders: A randomized trial in kindergarten and first grade. J. Autism Dev. Disord. 2014, 45, 1809–1824. [Google Scholar] [CrossRef]
- Chang, Y.-C.; Locke, J. A systematic review of peer-mediated interventions for children with autism spectrum disorder. Res. Autism Spectr. Disord. 2016, 27, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fantasia, V.; Markant, D.B.; Valeri, G.; Perri, N.; Ruggeri, A. Memory enhancements from active control of learning in children with autism spectrum disorder. Autism 2020, 24, 1995–2007. [Google Scholar] [CrossRef]
- Charlop-Christy, M.H.; Kelso, S.E. Teaching children with autism conversational speech using a cue card/written script program. Educ. Treat. Child. 2003, 26, 108–127. [Google Scholar]
- Ganz, J.B.; Kaylor, M.; Bourgeois, B.; Hadden, K. The impact of social scripts and visual cues on verbal communication in three children with autism spectrum disorders. Focus Autism Other Develop. Disabil. 2008, 23, 79–94. [Google Scholar] [CrossRef]
- Lang, R.; Regester, A.; Lauderdale, S.; Ashbaugh, K.; Haring, A. Treatment of anxiety in autism spectrum disorders using cognitive behaviour therapy: A systematic review. Dev. Neurorehabilit. 2010, 13, 53–63. [Google Scholar] [CrossRef]
- Thiemann, K.S.; Goldstein, H. Social stories, written text cues, and video feedback: Effects on social communication of children with autism. J. Appl. Behav. Anal. 2001, 34, 425–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fucà, E.; Lazzaro, G.; Costanzo, F.; Di Vara, S.; Menghini, D.; Vicari, S. Implicit and Explicit Memory in Youths with High-Functioning Autism Spectrum Disorder: A Case-Control Study. J. Clin. Med. 2021, 10, 4283. https://doi.org/10.3390/jcm10184283
Fucà E, Lazzaro G, Costanzo F, Di Vara S, Menghini D, Vicari S. Implicit and Explicit Memory in Youths with High-Functioning Autism Spectrum Disorder: A Case-Control Study. Journal of Clinical Medicine. 2021; 10(18):4283. https://doi.org/10.3390/jcm10184283
Chicago/Turabian StyleFucà, Elisa, Giulia Lazzaro, Floriana Costanzo, Silvia Di Vara, Deny Menghini, and Stefano Vicari. 2021. "Implicit and Explicit Memory in Youths with High-Functioning Autism Spectrum Disorder: A Case-Control Study" Journal of Clinical Medicine 10, no. 18: 4283. https://doi.org/10.3390/jcm10184283
APA StyleFucà, E., Lazzaro, G., Costanzo, F., Di Vara, S., Menghini, D., & Vicari, S. (2021). Implicit and Explicit Memory in Youths with High-Functioning Autism Spectrum Disorder: A Case-Control Study. Journal of Clinical Medicine, 10(18), 4283. https://doi.org/10.3390/jcm10184283