
Myocardial Work by Echocardiography: Principles and Applications in Clinical Practice

 ,
,  ,
, 
 , , , ,
, , , ,  ,
,  and
and
Abstract
:1. Introduction
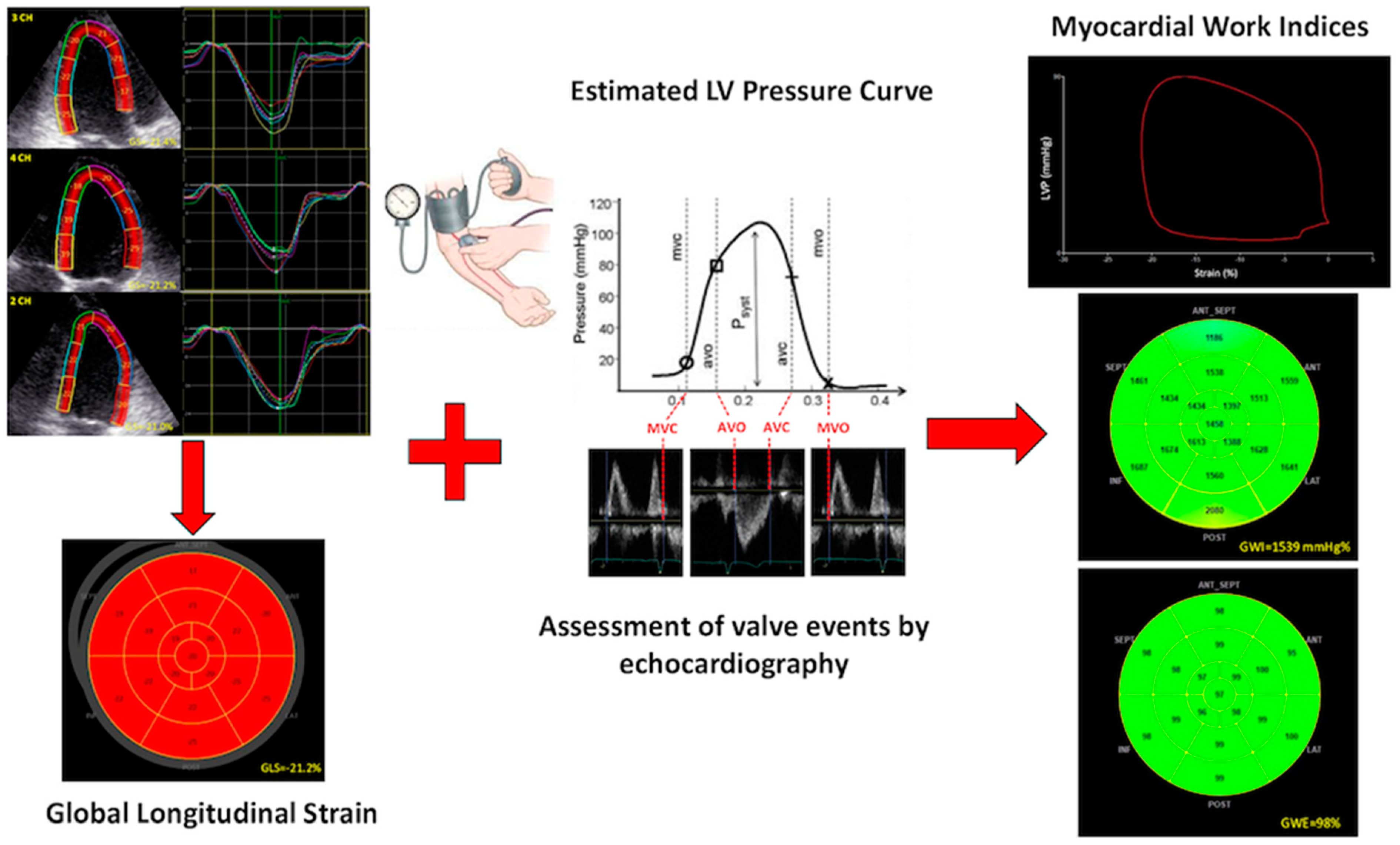
2. Evaluation of Myocardial Work from Estimated LV Pressure Curves
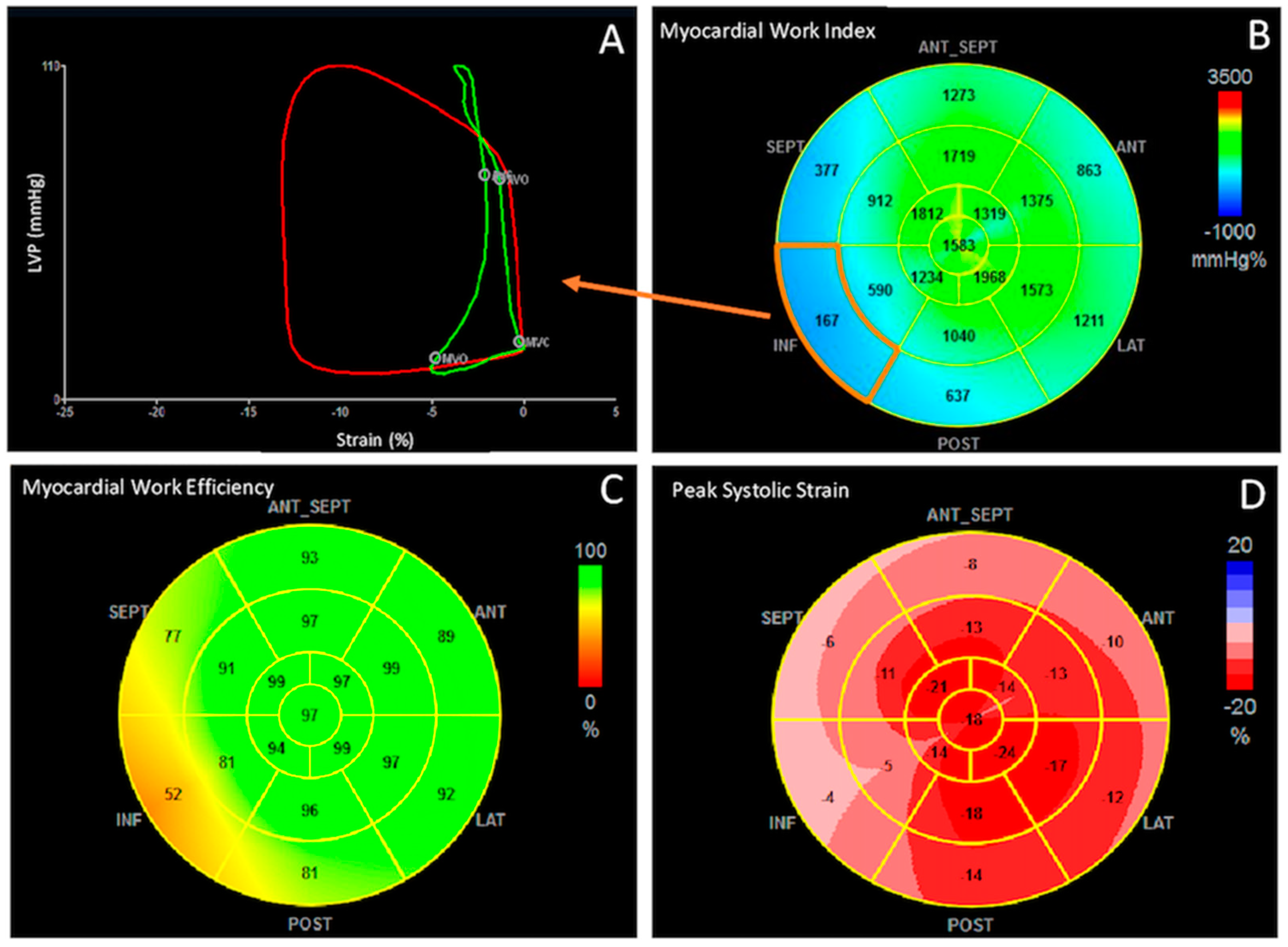
3. Quantification of Cardiac Work: Global Work Index, Constructive Work, Wasted Work and Work Efficiency
4. Clinical Applications
4.1. Heart Failure and Cardiac Resynchronization
4.2. Coronary Artery Disease
4.3. Hypertension and Diabetes Mellitus
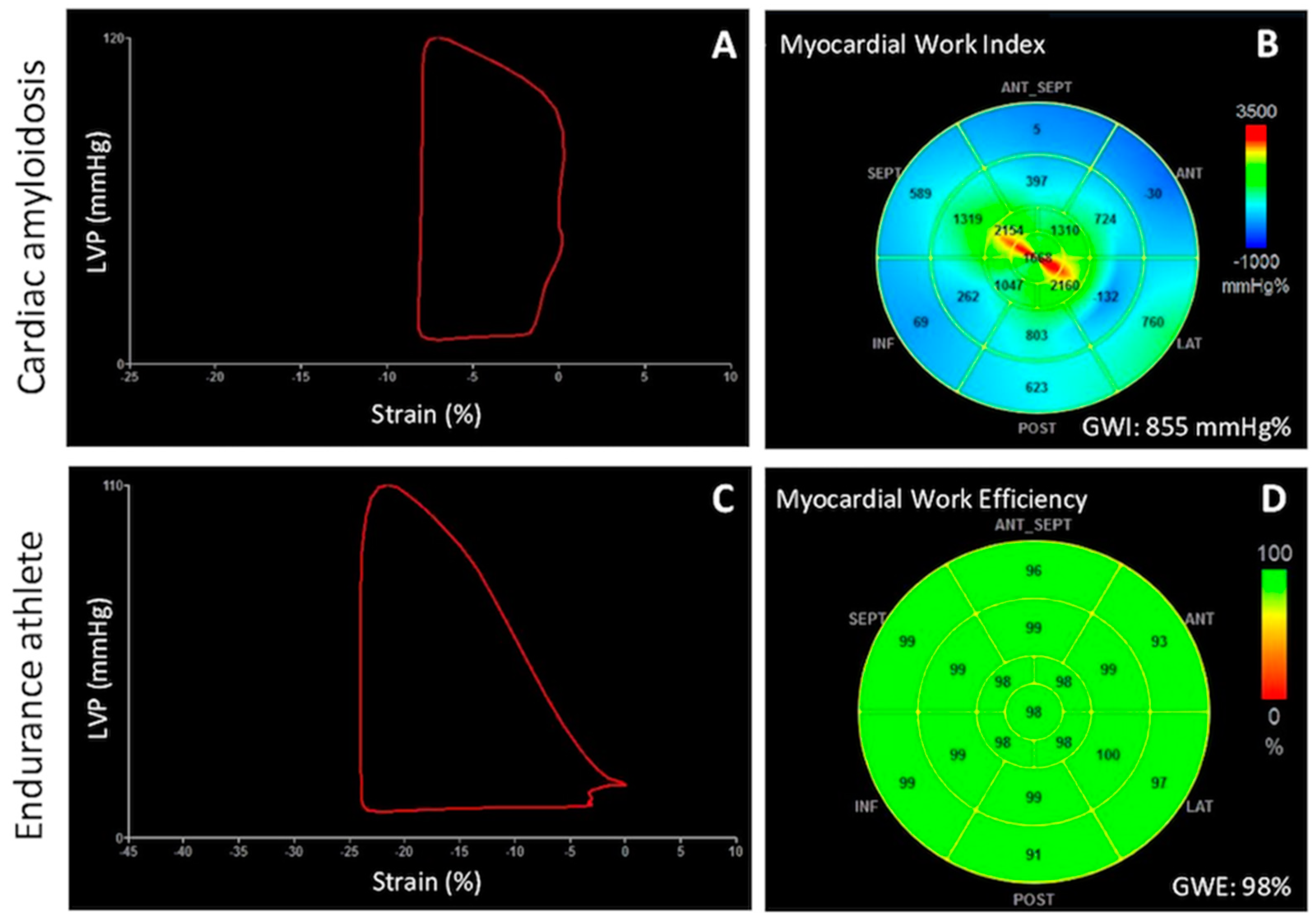
4.4. Cardiomyopathies
4.5. Athlete’s Heart
5. Emerging Areas of Application
5.1. Stress Echocardiography
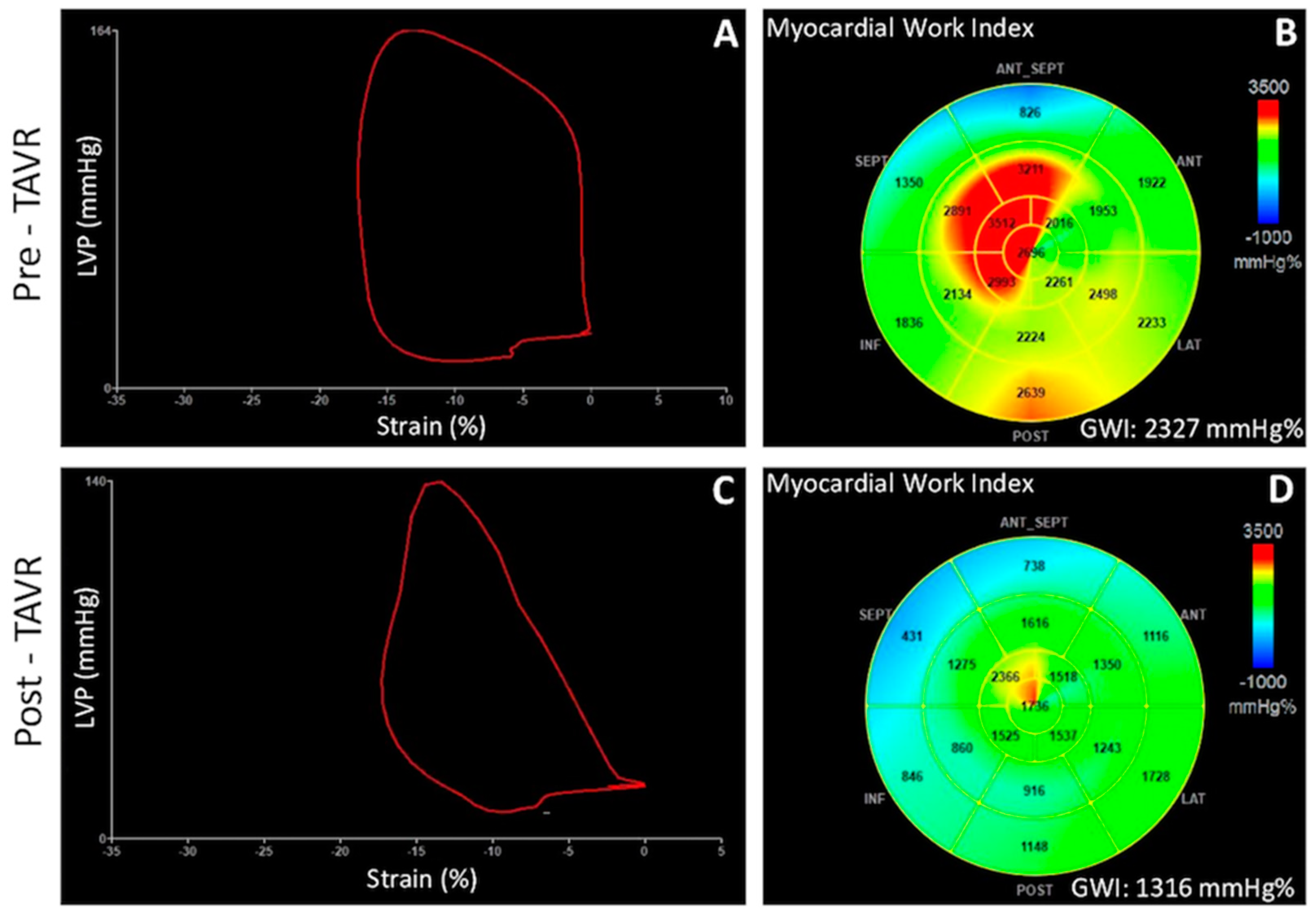
5.2. Valvular Heart Disease
5.3. Right Ventricular Myocardial Work
6. Limitations
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marwick, T.H. Ejection Fraction Pros and Cons: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 2360–2379. [Google Scholar] [CrossRef]
- Malm, S.; Frigstad, S.; Sagberg, E.; Larsson, H.; Skjaerpe, T. Accurate and reproducible measurement of left ventricular volume and ejection fraction by contrast echocardiography: A comparison with magnetic resonance imaging. J. Am. Coll. Cardiol. 2004, 44, 1030–1035. [Google Scholar] [CrossRef] [Green Version]
- Konstam, M.A.; Abboud, F.M. Ejection Fraction: Misunderstood and Overrated (Changing the Paradigm in Categorizing Heart Failure). Circulation 2017, 135, 717–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameli, M.; Mandoli, G.E.; Sciaccaluga, C.; Mondillo, S. More than 10 years of speckle tracking echocardiography: Still a novel technique or a definite tool for clinical practice? Echocardiography 2019, 36, 958–970. [Google Scholar] [CrossRef] [PubMed]
- van Dalen, B.M.; Soliman, O.I.; Vletter, W.B.; Kauer, F.; Van Der Zwaan, H.B.; Cate, F.J.T.; Geleijnse, M.L. Feasibility and reproducibility of left ventricular rotation parameters measured by speckle tracking echocardiography. Eur. J. Echocardiogr. 2009, 10, 669–676. [Google Scholar] [CrossRef] [Green Version]
- Geyer, H.; Caracciolo, G.; Abe, H.; Wilansky, S.; Carerj, S.; Gentile, F.; Nesser, H.-J.; Khandheria, B.; Narula, J.; Sengupta, P.P. Assessment of Myocardial Mechanics Using Speckle Tracking Echocardiography: Fundamentals and Clinical Applications. J. Am. Soc. Echocardiogr. 2010, 23, 351–369. [Google Scholar] [CrossRef]
- Yingchoncharoen, T.; Agarwal, S.; Popović, Z.; Marwick, T. Normal Ranges of Left Ventricular Strain: A Meta-Analysis. J. Am. Soc. Echocardiogr. 2013, 26, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Suga, H. Total mechanical energy of a ventricle model and cardiac oxygen consumption. Am. J. Physiol. Circ. Physiol. 1979, 236, H498–H505. [Google Scholar] [CrossRef]
- Dini, F.L.; Buralli, S.; Gallina, S.; Galderisi, M.; Mele, D.; Mondillo, S.; Agricola, E.; Di Bello, V.; Sciomer, S.; Ansalone, G.; et al. Principles of cardiovascular dynamics in the perspective of echocardiography. G. Ital. Cardiol. 2008, 9, 536–544. [Google Scholar]
- Suga, H.; Hayashi, T.; Shirahata, M. Ventricular systolic pressure-volume area as predictor of cardiac oxygen consumption. Am. J. Physiol. Circ. Physiol. 1981, 240, H39–H44. [Google Scholar] [CrossRef]
- Takaoka, H.; Takeuchi, M.; Odake, M.; Yokoyama, M. Assessment of myocardial oxygen consumption (Vo2) and systolic pressure-volume area (PVA) in human hearts. Eur. Hear. J. 1992, 13 (Suppl. E), 85–90. [Google Scholar] [CrossRef]
- Hisano, R.; Cooper, I.V.G. Correlation of force-length area with oxygen consumption in ferret papillary muscle. Circ. Res. 1987, 61, 318–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Haugaa, K.H.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A novel clinical method for quantification of regional left ventricular pressure–strain loop area: A non-invasive index of myocardial work. Eur. Heart J. 2012, 33, 724–733. [Google Scholar] [CrossRef] [Green Version]
- Hubert, A.; Le Rolle, V.; Leclercq, C.; Galli, E.; Samset, E.; Casset, C.; Mabo, P.; Hernandez, A.; Donal, E. Estimation of myocardial work from pressure–strain loops analysis: An experimental evaluation. Eur. Hear. J. Cardiovasc. Imaging 2018, 19, 1372–1379. [Google Scholar] [CrossRef] [PubMed]
- Manganaro, R.; Marchetta, S.; Dulgheru, R.; Ilardi, F.; Sugimoto, T.; Robinet, S.; Cimino, S.; Go, Y.Y.; Bernard, A.; Kacharava, G.; et al. Echocardiographic reference ranges for normal non-invasive myocardial work indices: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Manganaro, R.; Marchetta, S.; Dulgheru, R.; Sugimoto, T.; Tsugu, T.; Ilardi, F.; Cicenia, M.; Ancion, A.; Postolache, A.; Martinez, C.; et al. Correlation between non-invasive myocardial work indices and main parameters of systolic and diastolic function: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 533–541. [Google Scholar] [CrossRef]
- Bouali, Y.; Donal, E.; Gallard, A.; Laurin, C.; Hubert, A.; Bidaut, A.; Leclercq, C.; Galli, E. Prognostic Usefulness of Myocardial Work in Patients With Heart Failure and Reduced Ejection Fraction Treated by Sacubitril/Valsartan. Am. J. Cardiol. 2020, 125, 1856–1862. [Google Scholar] [CrossRef] [PubMed]
- Fortuni, F.; Butcher, S.C.; van der Kley, F.; Lustosa, R.P.; Karalis, I.; de Weger, A.; Priori, S.G.; van der Bijl, P.; Bax, J.J.; Delgado, V.; et al. Left Ventricular Myocardial Work in Patients with Severe Aortic Stenosis. J. Am. Soc. Echocardiogr. 2020, 34, 257–266. [Google Scholar] [CrossRef]
- Przewlocka-Kosmala, M.; Marwick, T.H.; Mysiak, A.; Kosowski, W.; Kosmala, W. Usefulness of myocardial work measurement in the assessment of left ventricular systolic reserve response to spironolactone in heart failure with preserved ejection fraction. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 1138–1146. [Google Scholar] [CrossRef]
- Galli, E.; Leclercq, C.; Hubert, A.; Bernard, A.; A Smiseth, O.; Mabo, P.; Samset, E.; Hernandez, A.; Donal, E. Role of myocardial constructive work in the identification of responders to CRT. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1010–1018. [Google Scholar] [CrossRef]
- Vecera, J.; Penicka, M.; Eriksen, M.; Russell, K.; Bartunek, J.; Vanderheyden, M.; Smiseth, O. Wasted septal work in left ventricular dyssynchrony: A novel principle to predict response to cardiac resynchronization therapy. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 624–632. [Google Scholar] [CrossRef] [Green Version]
- Edwards, N.F.A.; Scalia, G.M.; Shiino, K.; Sabapathy, S.; Anderson, B.; Chamberlain, R.; Khandheria, B.K.; Chan, J. Global Myocardial Work Is Superior to Global Longitudinal Strain to Predict Significant Coronary Artery Disease in Patients With Normal Left Ventricular Function and Wall Motion. J. Am. Soc. Echocardiogr. 2019, 32, 947–957. [Google Scholar] [CrossRef]
- Boe, E.; Russell, K.; Eek, C.; Eriksen, M.; Remme, E.W.; Smiseth, O.A.; Skulstad, H. Non-invasive myocardial work index identifies acute coronary occlusion in patients with non-ST-segment elevation-acute coronary syndrome. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1247–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- el Mahdiui, M.; van der Bijl, P.; Abou, R.; Ajmone Marsan, N.; Delgado, V.; Bax, J.J. Global Left Ventricular Myocardial Work Effi-ciency in Healthy Individuals and Patients with Cardiovascular Disease. J. Am. Soc. Echocardiogr. 2019, 32, 1120–1127. [Google Scholar] [CrossRef] [PubMed]
- Lustosa, R.P.; van der Bijl, P.; El Mahdiui, M.; Montero-Cabezas, J.M.; Kostyukevich, M.V.; Marsan, N.A.; Bax, J.J.; Delgado, V. Noninvasive Myocardial Work Indices 3 Months after ST-Segment Elevation Myocardial Infarction: Prevalence and Characteristics of Patients with Postinfarction Cardiac Remodeling. J. Am. Soc. Echocardiogr. 2020, 33, 1172–1179. [Google Scholar] [CrossRef] [PubMed]
- Meimoun, P.; Abdani, S.; Stracchi, V.; Elmkies, F.; Boulanger, J.; Botoro, T.; Zemir, H.; Clerc, J. Usefulness of Noninvasive Myocardial Work to Predict Left Ventricular Recovery and Acute Complications after Acute Anterior Myocardial Infarction Treated by Percutaneous Coronary Intervention. J. Am. Soc. Echocardiogr. 2020, 33, 1180–1190. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.; Edwards, N.F.A.; Khandheria, B.K.; Shiino, K.; Sabapathy, S.; Anderson, B.; Chamberlain, R.; Scalia, G.M. A new approach to assess myocardial work by non-invasive left ventricular pressure–strain relations in hypertension and dilated cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Tadic, M.; Cuspidi, C.; Pencic, B.; Grassi, G.; Celic, V. Myocardial work in hypertensive patients with and without diabetes: An echocardiographic study. J. Clin. Hypertens. 2020, 22, 2121–2127. [Google Scholar] [CrossRef]
- Galli, E.; Vitel, E.; Schnell, F.; Le Rolle, V.; Hubert, A.; Lederlin, M.; Donal, E. Myocardial constructive work is impaired in hypertrophic cardiomyopathy and predicts left ventricular fibrosis. Echocardiography 2019, 36, 74–82. [Google Scholar] [CrossRef] [Green Version]
- Hiemstra, Y.L.; van der Bijl, P.; el Mahdiui, M.; Bax, J.J.; Delgado, V.; Marsan, N.A. Myocardial Work in Nonobstructive Hypertrophic Cardiomyopathy: Implications for Outcome. J. Am. Soc. Echocardiogr. 2020, 33, 1201–1208. [Google Scholar] [CrossRef]
- Cui, C.; Liu, L.; Li, Y.; Liu, Y.; Huang, D.; Hu, Y.; Zhang, L. Left Ventricular Pressure–Strain Loop-Based Quantitative Examination of the Global and Regional Myocardial Work of Patients with Dilated Cardiomyopathy. Ultrasound Med. Biol. 2020, 46, 2834–2845. [Google Scholar] [CrossRef] [PubMed]
- Clemmensen, T.S.; Eiskjær, H.; Mikkelsen, F.; Granstam, S.-O.; Flachskampf, F.A.; Sørensen, J.; Poulsen, S.H. Left Ventricular Pressure-Strain–Derived Myocardial Work at Rest and during Exercise in Patients with Cardiac Amyloidosis. J. Am. Soc. Echocardiogr. 2020, 33, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Roger-Rollé, A.; Cariou, E.; Rguez, K.; Fournier, P.; Lavie-Badie, Y.; Blanchard, V.; Roncalli, J.; Galinier, M.; Carrié, D.; Lairez, O. Can myocardial work indices contribute to the exploration of patients with cardiac amyloidosis? Open Heart 2020, 7, e001346. [Google Scholar] [CrossRef]
- Clemmensen, T.S.; Eiskjær, H.; Ladefoged, B.; Mikkelsen, F.; Sørensen, J.; Granstam, S.-O.; Rosengren, S.; A Flachskampf, F.; Poulsen, S.H. Prognostic implications of left ventricular myocardial work indices in cardiac amyloidosis. Eur. Hear. J. Cardiovasc. Imaging 2021, 22, 695–704. [Google Scholar] [CrossRef]
- D’Andrea, A.; Radmilovic, J.; Carbone, A.; Mandoli, G.E.; Santoro, C.; Evola, V.; Bandera, F.; D’Ascenzi, F.; Bossone, E.; the Echocardiography Study Group of the Italian Society of Cardiology; et al. Speckle tracking evaluation in endurance athletes: The “optimal” myocardial work. Int. J. Cardiovasc. Imaging 2020, 36, 1679–1688. [Google Scholar] [CrossRef]
- Halabi, A.; Wright, L.; Marwick, T.H. Measurement of Global Myocardial Work with Exercise Testing. J. Am. Soc. Echocardiogr. 2020, 33, 631–632. [Google Scholar] [CrossRef]
- Mansour, M.; AlJaroudi, W.; Mansour, L.; Nehme, A.; Hamoui, O.; Ayoub, W.; Chammas, E. Value of myocardial work for assessment of myocardial adaptation to increased afterload in patients with high blood pressure at peak exercise. Int. J. Cardiovasc. Imaging 2020, 36, 1647–1656. [Google Scholar] [CrossRef]
- D’Andrea, A.; Sperlongano, S.; Formisano, T.; Tocci, G.; Cameli, M.; Tusa, M.; Novo, G.; Corrado, G.; Ciampi, Q.; Citro, R.; et al. Stress Echocardiography and Strain in Aortic Regurgitation (SESAR protocol): Left ventricular contractile reserve and myocardial work in asymptomatic patients with severe aortic regurgitation. Echocardiography 2020, 37, 1213–1221. [Google Scholar] [CrossRef]
- Jain, R.; Bajwa, T.; Roemer, S.; Huisheree, H.; Allaqaband, S.Q.; Kroboth, S.; Moreno, A.C.P.; Tajik, A.J.; Khandheria, B.K. Myocardial work assessment in severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur. Heart J. Cardiovasc. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Auricchio, A.; Baron-Esquivias, G.; Bordachar, P.; Boriani, G.; Breithardt, O.-A.; Cleland, J.G.F.; Deharo, J.-C.; Delgado, V.; Elliott, P.M.; et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: The Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur. Heart J. 2013, 34, 2281–2329. [Google Scholar] [CrossRef] [Green Version]
- Chung, E.S.; Leon, A.R.; Tavazzi, L.; Sun, J.-P.; Nihoyannopoulos, P.; Merlino, J.; Abraham, W.T.; Ghio, S.; Leclercq, C.; Bax, J.J.; et al. Results of the Predictors of Response to CRT (PROSPECT) Trial. Circulation 2008, 117, 2608–2616. [Google Scholar] [CrossRef] [Green Version]
- Lim, P.; Donal, E.; Lafitte, S.; Derumeaux, G.; Habib, G.; Réant, P.; Thivolet, S.; Lellouche, N.; Grimm, R.A.; Gueret, P. Multicentre study using strain delay index for predicting response to cardiac resynchronization therapy (MUSIC study). Eur. J. Heart Fail. 2011, 13, 984–991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-Montero, A.; Tayal, B.; Goda, A.; Ryo, K.; Marek, J.J.; Sugahara, M.; Qi, Z.; Althouse, A.D.; Saba, S.; Schwartzman, D.; et al. Additive Prognostic Value of Echocardiographic Global Longitudinal and Global Circumferential Strain to Electrocardiographic Criteria in Patients with Heart Failure Undergoing Cardiac Resynchronization Therapy. Circ. Cardiovasc. Imaging 2016, 9, e004241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, H.; Hara, H.; Saba, S.; Gorcsan, J. Prediction of Response to Cardiac Resynchronization Therapy by Speckle Tracking Echocardiography Using Different Software Approaches. J. Am. Soc. Echocardiogr. 2009, 22, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Iwano, H.; Yamada, S.; Watanabe, M.; Mitsuyama, H.; Mizukami, K.; Nishino, H.; Yokoyama, S.; Kaga, S.; Okada, K.; Nishida, M.; et al. Strain Rate Dispersion Index Can Predict Changes in Left Ventricular Volume and Adverse Cardiac Events Following Cardiac Resynchronization Therapy. Circ. J. 2013, 77, 2757–2765. [Google Scholar] [CrossRef] [Green Version]
- Ciampi, Q.; Pratali, L.; Citro, R.; Piacenti, M.; Villari, B.; Picano, E. Identification of responders to cardiac resynchronization therapy by contractile reserve during stress echocardiography. Eur. J. Heart Fail. 2009, 11, 489–496. [Google Scholar] [CrossRef] [Green Version]
- Aalen, J.M.; Donal, E.; Larsen, C.K.; Duchenne, J.; Lederlin, M.; Cvijic, M.; Hubert, A.; Voros, G.; Leclercq, C.; Bogaert, J.; et al. Imaging predictors of response to cardiac resynchronization therapy: Left ventricular work asymmetry by echocardiography and septal viability by cardiac magnetic resonance. Eur. Heart J. 2020, 41, 3813–3823. [Google Scholar] [CrossRef]
- Duchenne, J.; Aalen, J.M.; Cvijic, M.; Larsen, C.K.; Galli, E.; Bézy, S.; Beela, A.S.; Ünlü, S.; Pagourelias, E.D.; Winter, S.; et al. Acute redistribution of regional left ventricular work by cardiac resynchronization therapy determines long-term remodelling. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 619–628. [Google Scholar] [CrossRef]
- Wang, Y.; Zhou, R.; Lu, C.; Chen, Q.; Xu, T.; Li, D. Effects of the angiotensin-receptor neprilysin inhibitor on cardiac reverse re-modeling: Meta-analysis. J. Am. Heart Assoc. 2019, 8, e012272. [Google Scholar] [CrossRef] [Green Version]
- Pfau, D.; Thorn, S.L.; Zhang, J.; Mikush, N.; Renaud, J.; Klein, R.; Dekemp, R.A.; Wu, X.; Hu, X.; Sinusas, A.J.; et al. Angiotensin Receptor Neprilysin Inhibitor Attenuates Myocardial Remodeling and Improves Infarct Perfusion in Experimental Heart Failure. Sci. Rep. 2019, 9, 5791. [Google Scholar] [CrossRef]
- Pugliese, N.R.; Fabiani, I.; Santini, C.; Rovai, I.; Pedrinelli, R.; Natali, A.; Dini, F.L. Value of combined cardiopulmonary and echocardiography stress test to characterize the haemodynamic and metabolic responses of patients with heart failure and mid-range ejection fraction. Eur Heart J Cardiovasc Imaging 2019, 20, 828–836. [Google Scholar] [CrossRef]
- D’Andrea, A.; Ilardi, F.; D’Ascenzi, F.; Bandera, F.; Benfari, G.; Esposito, R.; Malagoli, A.; Mandoli, G.E.; Santoro, C.; Russo, V.; et al. Impaired myocardial work efficiency in heart failure with preserved ejection fraction. Eur. Heart J. Cardiovasc. Imaging 2021. [Google Scholar] [CrossRef] [PubMed]
- Ilardi, F.; Ferrone, M.; Avvedimento, M.; Servillo, G.; Gargiulo, G. Complete Revascularization in Acute and Chronic Coronary Syndrome. Cardiol. Clin. 2020, 38, 491–505. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-O.; Cho, S.W.; Bin Song, Y.; Song, B.G.; Lee, S.-C.; Park, S.W. Longitudinal 2D strain at rest predicts the presence of left main and three vessel coronary artery disease in patients without regional wall motion abnormality. Eur. J. Echocardiogr. 2009, 10, 695–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skulstad, H.; Edvardsen, T.; Urheim, S.; Rabben, S.I.; Stugaard, M.; Lyseggen, E.; Ihlen, H.; Smiseth, O.A. Postsystolic Shortening in Ischemic Myocardium. Circulation 2002, 106, 718–724. [Google Scholar] [CrossRef] [Green Version]
- Azevedo, P.S.; Minicucci, M.F.; Santos, P.P.; Paiva, S.; Zornoff, L. Energy Metabolism in Cardiac Remodeling and Heart Failure. Cardiol. Rev. 2013, 21, 135–140. [Google Scholar] [CrossRef]
- Skaarup, K.G.; Lassen, M.C.H.; Marott, J.L.; Biering-Sørensen, S.R.; Jørgensen, P.G.; Appleyard, M.; Berning, J.; Høst, N.; Jensen, G.; Schnohr, P.; et al. The impact of cardiovascular risk factors on global longitudinal strain over a decade in the general population: The copenhagen city heart study. Int. J. Cardiovasc. Imaging 2020, 36, 1907–1916. [Google Scholar] [CrossRef]
- Morris, D.A.; Otani, K.; Bekfani, T.; Takigiku, K.; Izumi, C.; Yuda, S.; Sakata, K.; Ohte, N.; Tanabe, K.; Friedrich, K.; et al. Multidirectional Global Left Ventricular Systolic Function in Normal Subjects and Patients with Hypertension: Multicenter Evaluation. J. Am. Soc. Echocardiogr. 2014, 27, 493–500. [Google Scholar] [CrossRef]
- Loncaric, F.; Marciniak, M.; Nunno, L.; Mimbrero, M.; Fernandes, J.F.; Fabijanovic, D.; Sanchis, L.; Doltra, A.; Montserrat, S.; Cikes, M.; et al. Distribution of myocardial work in arterial hypertension: Insights from non-invasive left ventricular pressure-strain relations. Int. J. Cardiovasc. Imaging 2021, 37, 145–154. [Google Scholar] [CrossRef]
- Sengupta, S.; Jain, R.; Burkule, N.; Olet, S.; Khandheria, B.K. Myocardial Work Index: A Novel Method for Assessment of Myo-cardial Function in South Asian Recreational Athletes. J. Patient Cent. Res. Rev. 2020, 7, 147–156. [Google Scholar] [CrossRef]
- Snader, C.E.; Marwick, T.H.; Pashkow, F.J.; Harvey, S.A.; Thomas, J.D.; Lauer, M.S. Importance of Estimated Functional Capacity as a Predictor of All-Cause Mortality Among Patients Referred for Exercise Thallium Single-Photon Emission Computed To-mography: Report of 3,400 Patients From a Single Center. J. Am. Coll. Cardiol. 1997, 30, 641–648. [Google Scholar] [CrossRef]
- Ekelund, L.-G.; Haskell, W.L.; Johnson, J.L.; Whaley, F.S.; Criqui, M.H.; Sheps, D.S. The Lipid Research Clinics Mortality Follow-up Study Physical Fitness as a Predictor of Cardiovascular Mortality in Asymptomatic North American Men. N. Engl. J. Med. 1988, 319, 1379–1384. [Google Scholar] [CrossRef]
- Dahl, J.; Magne, J.; Pellikka, P.A.; Donal, E.; Marwick, T.H. Assessment of Subclinical Left Ventricular Dysfunction in Aortic Stenosis. JACC Cardiovasc. Imaging 2019, 12, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Ilardi, F.; Marchetta, S.; Martinez, C.; Sprynger, M.; Ancion, A.; Manganaro, R.; Sugimoto, T.; Tsugu, T.; Postolache, A.; Piette, C.; et al. Impact of aortic stenosis on layer-specific longitudinal strain: Relationship with symptoms and outcome. Eur. Heart J. Cardiovasc. Imaging 2019, 21, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Butcher, S.C.; Fortuni, F.; Montero-Cabezas, J.M.; Abou, R.; El Mahdiui, M.; Van Der Bijl, P.; Van Der Velde, E.T.; Marsan, N.A.; Bax, J.J.; Delgado, V. Right ventricular myocardial work: Proof-of-concept for non-invasive assessment of right ventricular function. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 142–152. [Google Scholar] [CrossRef]
- Buonauro, A.; Santoro, C.; Galderisi, M.; Canora, A.; Sorrentino, R.; Esposito, R.; Lembo, M.; Canonico, M.E.; Ilardi, F.; Fazio, V.; et al. Impaired Right and Left Ventricular Longitudinal Function in Patients with Fibrotic Interstitial Lung Diseases. J. Clin. Med. 2020, 9, 587. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Determinants | Reference Values [15] | ||
|---|---|---|---|---|
| Total | Male | Female | ||
| GWI (mmHg%) | Amount of myocardial work performed by the left ventricle during systole => area of PSL from mitral valve closure to mitral valve opening | 1292–2505 | 1270–2428 | 1310–2538 |
| GCW (mmHg%) | Positive work performed in systole (shortening) + Negative work performed in isovolumetric relaxation (lengthening) | 1582–2881 | 1650–2807 | 1543–2924 |
| GWW (mmHg%) | Negative work performed in systole (lengthening) + Positive work performed in isovolumetric relaxation (shortening) | 226 ± 28 a | 238 ± 33 a | 239 ± 39 a |
| GWE (%) | Percentage (0–100%) of constructive work over total work => Constructive work/(constructive work + wasted work) | 91 ± 0.8 b | 90 ± 1.6 b | 91 ± 1 b |
| Clinical Setting | Diagnostic Role | Prognostic Role |
|---|---|---|
| Heart failure and reduced EF (HRrEF) |
| |
| Heart failure and preserved EF (HRpEF) |
| |
| Cardiac resynchronization | ||
| Coronary artery disease (CAD) |
| |
| Hypertension (HTN) and diabetes mellitus (DM) | ||
| Non-obstructive hypertrophic cardiomyopathy (HCM) | ||
| Dilated cardiomyopathy (DCM) |
|
|
| Cardiac amyloidosis | ||
| Athlete’s heart |
| |
| Stress echocardiography | ||
| Aortic regurgitation |
| |
| Aortic stenosis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilardi, F.; D’Andrea, A.; D’Ascenzi, F.; Bandera, F.; Benfari, G.; Esposito, R.; Malagoli, A.; Mandoli, G.E.; Santoro, C.; Russo, V.; et al. Myocardial Work by Echocardiography: Principles and Applications in Clinical Practice. J. Clin. Med. 2021, 10, 4521. https://doi.org/10.3390/jcm10194521
Ilardi F, D’Andrea A, D’Ascenzi F, Bandera F, Benfari G, Esposito R, Malagoli A, Mandoli GE, Santoro C, Russo V, et al. Myocardial Work by Echocardiography: Principles and Applications in Clinical Practice. Journal of Clinical Medicine. 2021; 10(19):4521. https://doi.org/10.3390/jcm10194521
Chicago/Turabian StyleIlardi, Federica, Antonello D’Andrea, Flavio D’Ascenzi, Francesco Bandera, Giovanni Benfari, Roberta Esposito, Alessandro Malagoli, Giulia Elena Mandoli, Ciro Santoro, Vincenzo Russo, and et al. 2021. "Myocardial Work by Echocardiography: Principles and Applications in Clinical Practice" Journal of Clinical Medicine 10, no. 19: 4521. https://doi.org/10.3390/jcm10194521
APA StyleIlardi, F., D’Andrea, A., D’Ascenzi, F., Bandera, F., Benfari, G., Esposito, R., Malagoli, A., Mandoli, G. E., Santoro, C., Russo, V., Crisci, M., Esposito, G., Cameli, M., & on behalf of the Working Group of Echocardiography of the Italian Society of Cardiology (SIC). (2021). Myocardial Work by Echocardiography: Principles and Applications in Clinical Practice. Journal of Clinical Medicine, 10(19), 4521. https://doi.org/10.3390/jcm10194521