
Evolution of the Use of Corticosteroids for the Treatment of Hospitalised COVID-19 Patients in Spain between March and November 2020: SEMI-COVID National Registry

 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. The SEMI-COVID-19 Registry
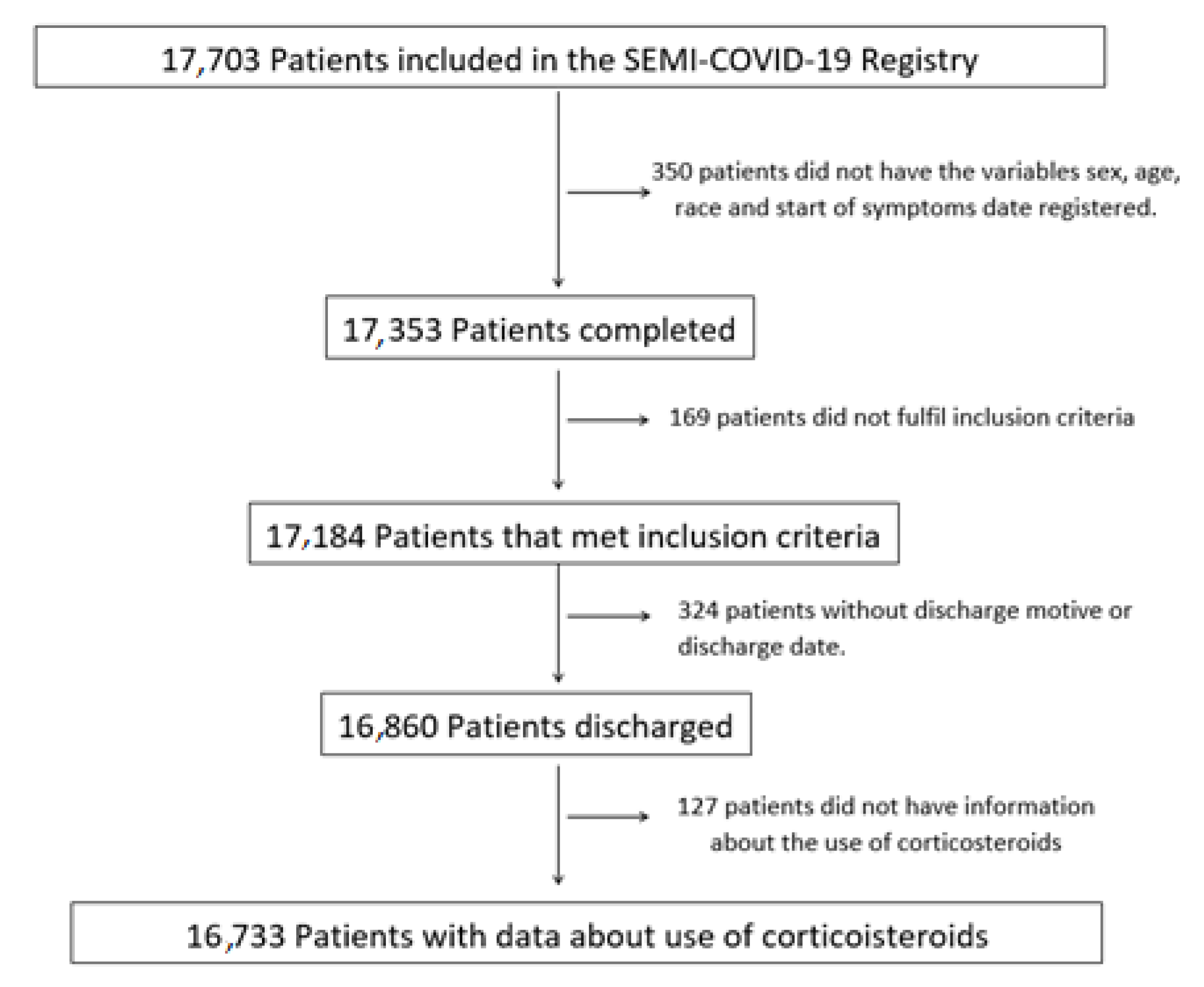
2.2. Procedures
2.3. Statistical Analysis
3. Results
3.1. Comorbidities
3.2. Biochemical and Gasometrical Parameters
3.3. Chest X-ray
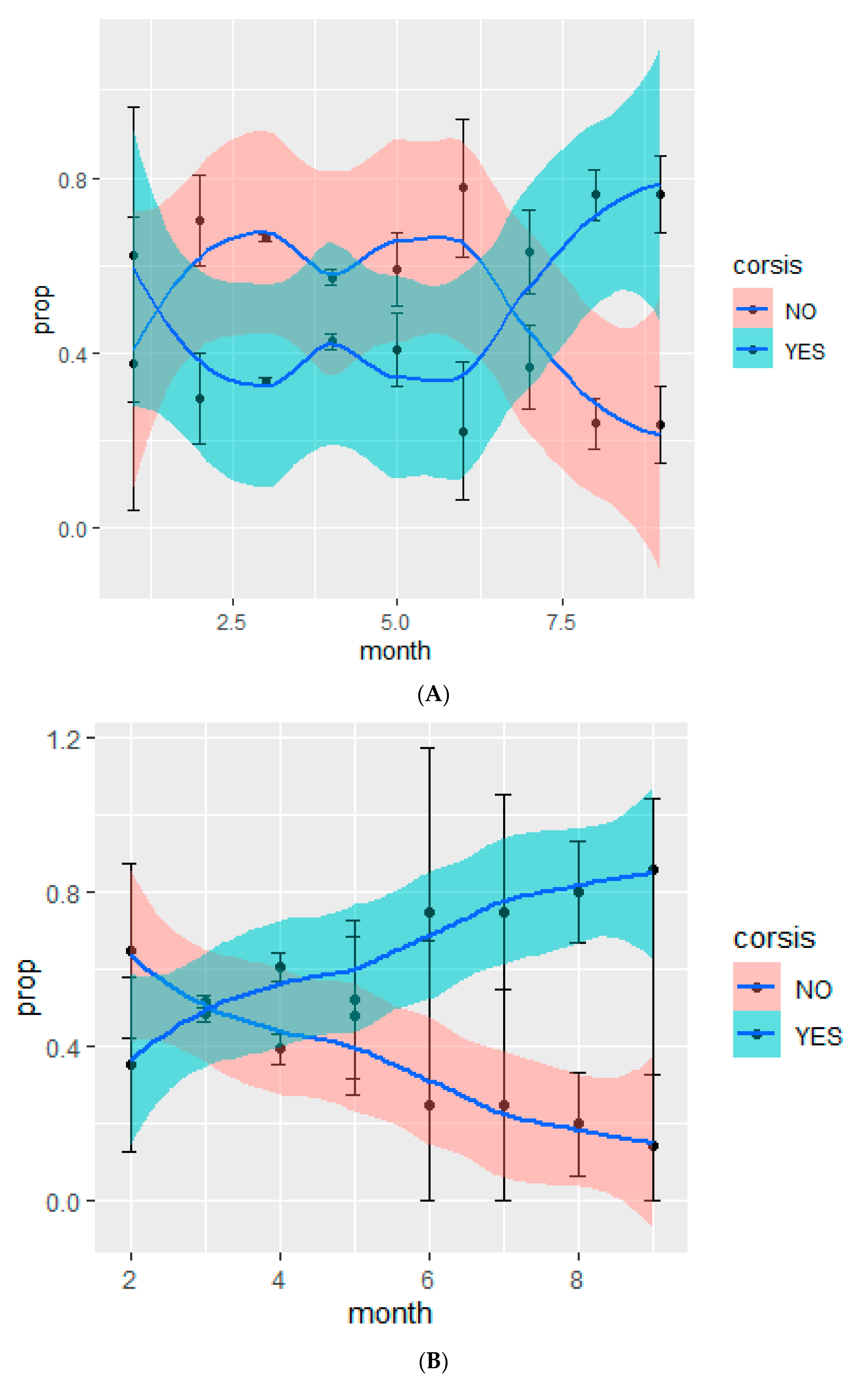
3.4. Administration of Corticosteroids during Pandemic
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- WHO. Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html (accessed on 30 March 2020).
- Stockman, L.J.; Bellamy, R.; Garner, P. SARS: Systematic Review of Treatment Effects. PLoS Med. 2006, 3, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auyeung, T.W.; Lee, J.S.; Lai, W.K.; Choi, C.H.; Lee, H.K.; Li, P.C.; Lok, K.H.; Ng, Y.Y.; Wong, W.M. The Use of Corticosteroid as Treatment in SARS was Associated with Adverse Outcomes: A Retrospective Cohort Study. J. Infect. 2005, 51, 98–102. [Google Scholar] [CrossRef]
- Long, Y.; Xu, Y.; Wang, B.; Zhang, L.; Jia, D.; Xue, F.; Duan, G.; He, J.; Xia, J.-Y.; Xu, D. Clinical Recommendations from an Observational Study on MERS: Glucocorticoids was Benefit in Treating SARS Patients. Int. J. Clin. Exp. Med. 2016, 9, 8865–8873. [Google Scholar]
- Lee, N.; Chan, K.A.; Hui, D.; Ng, E.K.; Wu, A.; Chiu, R.W.; Wong, V.W.; Chan, P.; Wong, K.; Wong, E.; et al. Effects of Early Corticosteroid Treatment on Plasma SARS-Associated Coronavirus RNA Concentrations in Adult Patients. J. Clin. Virol. 2004, 31, 304–309. [Google Scholar] [CrossRef]
- The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2020, 384, 693–704. [Google Scholar] [CrossRef]
- She, J.; Hou, D.; He, H.; Song, Y. Corticosteroids: A Controversial Therapy for Coronavirus Disease 2019. J. Transl. Intern. Med. 2020, 8, 115–118. [Google Scholar] [CrossRef]
- Moore, J.B.; June, C.H. Cytokine Release Syndrome in Severe COVID-19. Science 2020, 368, 473–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary Post-Mortem Findings in a Series of COVID-19 Cases from Northern Italy: A Two-Centre Descriptive Study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef]
- Ye, Q.; Wang, B.; Mao, J. The Pathogenesis and Treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Meng, Z. Immunomodulation for Severe COVID-19 Pneumonia: The State of the Art. Front. Immunol. 2020, 11, 577442. [Google Scholar] [CrossRef]
- WHO. Corticosteroids for COVID-19: Living Guidance. 2020. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Corticosteroids-2020.1 (accessed on 9 November 2020).
- Xiong, B.; He, L.-M.; Qin, Y.-Y.; Du, H.; Zhan, Z.; Zhou, Y.-H.; Chen, Y.-K.; Zhang, A. Effectiveness of Adjunctive Corticosteroid Therapy in Patients with Severe COVID-19: A Retrospective Cohort Study. World J. Clin. Cases 2020, 9, 3546–3558. [Google Scholar] [CrossRef]
- Bhimraj, A.; Morgan, R.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.-C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with Coronavirus Disease 2019 (COVID-19). Clin. Infect. Dis. 2020. [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casas-Rojo, J.M.; Antón-Santos, J.M.; Millán-Núñez-Cortés, J.; Lumbreras-Bermejo, C.; Ramos-Rincón, J.M.; Roy-Vallejo, E.; Artero-Mora, A.; Arnalich-Fernández, F.; García-Bruñén, J.M.; Vargas-Núñez, J.A.; et al. Clinical Characteristics of Patients Hospitalized with COVID-19 in Spain: Results from the SEMI-COVID-19 Network. Rev. Clin. Esp. 2020, 220, 480–494. [Google Scholar] [CrossRef] [PubMed]
- WHO. Laboratory Testing for Coronavirus Disease 2019 (COVID19) in Suspected Human Cases. 2020. Available online: https://www.who.int/publications/i/item/laboratory-testing-for-2019-novel-coronavirus in-suspected-human-cases-20200117 (accessed on 19 March 2020).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a Combined Comorbidity Index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Tadic, M.; Cuspidi, C.; Grassi, G.; Mancia, G. COVID-19 and Arterial Hypertension: Hypothesis or Evidence? J. Clin. Hypertens. 2020, 22, 1120–1126. [Google Scholar] [CrossRef]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of Comorbidities in the Novel Wuhan Coronavirus (COVID-19) Infection: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Emami, A.; Javanmardi, F.; Pirbonyeh, N.; Akbari, A. Prevalence of Underlying Diseases in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Arch. Acad. Emerg. Med. 2020, 8, e35. [Google Scholar]
- Rodilla, E.; Saura, A.; Jiménez, I.; Mendizábal, A.; Pineda-Cantero, A.; Lorenzo-Hernández, E.; Fidalgo-Montero, M.D.P.; López-Cuervo, J.F.; Gil-Sánchez, R.; Rabadán-Pejenaute, E.; et al. Association of Hypertension with All-Cause Mortality among Hospitalized Patients with COVID-19. J. Clin. Med. 2020, 9, 3136. [Google Scholar] [CrossRef]
- Tadic, M.; Cuspidi, C.; Sala, C. COVID-19 and Diabetes: Is There Enough Evidence? J. Clin. Hypertens. 2020, 22, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Banegas, J.R.; Conde-Gijon, T. Epidemiología de la Hipertensión Arterial. Hipertens. Y Riesgo Vascular. 2017, 34, 2–4. [Google Scholar] [CrossRef]
- Danwang, C.; Endomba, F.T.; Nkeck, J.R.; Wouna, D.L.A.; Robert, A.; Noubiap, J.J. A Meta-Analysis of Potential Biomarkers Associated with Severity of Coronavirus Disease 2019 (COVID-19). Biomark. Res. 2020, 8, 6161. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Confalonieri, M.; Pastores, S.M.; Meduri, G.U. Rationale for Prolonged Corticosteroid Treatment in the Acute Respiratory Distress Syndrome Caused by Coronavirus Disease 2019. Crit. Care Explor. 2020, 2, e0111. [Google Scholar] [CrossRef] [Green Version]
- Corral-Gudino, L.; Bahamonde, A.; Arnaiz-Revillas, F.; Gómez-Barquero, J.; Abadía-Otero, J.; García-Ibarbia, C.; Mora, V.; Cerezo-Hernández, A.; Hernández, J.L.; López-Muñíz, G.; et al. GLUCOCOVID: A Controlled Trial of Methylprednisolone in Adults Hospitalized with COVID-19 Pneumonia. Medrxiv 2020. [Google Scholar] [CrossRef]
- Wikman-Jorgensen, P.E.; Blanquer, E.; Esteban Giner, M.J.; Delgado, E.; Gómez, C.; Palacios, S.; Bonet Tur, D.; Giner-Galvañ, V. Corticoides en la Infección por SARS-COV-2: Un Estudio de Cohortes Retrospectivas. Rev. Clin. Esp. 2021, 221, 259. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total Cohort | CT | nCT | p-Value |
|---|---|---|---|---|
| Participants, n (%) | 16,717 | 6053 (36.21) | 10,664 (63.79) | <0.001 |
| Age (years), Mean (SD) | 67.33 (16.13) | 69.65 (14.58) | 66.01 (16.80) | <0.001 |
| Men, n (%) | 9595 (57.39) | 3840 (63.44) | 5755 (54.07) | <0.001 |
| HBP, n (%) | 8542 (51.1) | 3450 (57) | 5092 (47.75) | <0.001 |
| DMnEOD, n (%) | 2416 (14.45) | 983 (16.24) | 1433 (13.44) | <0.001 |
| DMEOD, n (%) | 896 (5.36) | 363 (6) | 533 (5) | 0.0071 |
| DLP, n (%) | 6612 (39.55) | 2601 (43.02) | 4011 (37.64) | <0.001 |
| Alcohol abuse, n (%) | 751 (4.62) | 313 (5.35) | 438 (4.22) | <0.001 |
| Smoking, n (%) | ||||
| Never | 11,137 (69.49) | 3765 (65.12) | 533 (5.20) | |
| Ex-smoker | 4053 (25.29) | 1714 (29.64) | 2339 (22.83) | <0.001 |
| Smoker | 835 (5.2) | 302 (5.22) | 7372 (71.96) | |
| AF, n (%) | 1840 (11.01) | 711 (11.76) | 1129 (10.59) | 0.022 |
| Anxiety disorder, n (%) | 1292 (7.74) | 486 (8.05) | 806 (7.57) | 0.273 |
| Depression, n (%) | 1757 (10.5) | 669 (11.09) | 1083 (10.17) | 0.069 |
| Obesity, n (%) | 3359 (20.09) | 1463 (26.37) | 1896 (19.33) | <0.001 |
| Neurodegenerative disease, n (%) | 1484 (8.88) | 540 (8.92) | 944 (8.85) | 0.899 |
| Angina, n (%) | 591 (3.53) | 258 (4.26) | 333 (3.12) | 0.001 |
| HF, n (%) | 1187 (7.1) | 491 (8.11) | 696 (6.53) | 0.001 |
| COPD, n (%) | 1132 (6.77) | 585 (9.67) | 547 (5.13) | <0.001 |
| Asthma, n (%) | 1185 (7.09) | 474 (7.8) | 711 (6.67) | 0.006 |
| TIA, n (%) | 789 (4.72) | 322 (5.32) | 467 (4.38) | 0.007 |
| Stroke, n (%) | 462 (2.76) | 177 (2.92) | 285 (2.67) | 0.372 |
| Hemiplegia, n (%) | 272 (1.62) | 165 (1.54) | 107 (1.76) | 0.310 |
| Dementia, n (%) | 1659 (9.9) | 559 (9.24) | 1100 (10.3) | 0.03 |
| PAD, n (%) | 765 (4.58) | 315 (5.21) | 450 (4.23) | 0.004 |
| Cirrhosis, n (%) | 175 (1.04) | 72 (1.19) | 103 (0.97) | 0.19 |
| CKD, n (%) | 1008 (6.18) | 440 (7.28) | 568 (5.33) | <0.001 |
| Active Neoplasm, n (%) | 1034 (6.18) | 405 (6.69) | 629 (5.9) | 0.05 |
| Leukaemia, n (%) | 194 (1.1) | 96 (1.59) | 98 (0.92) | <0.001 |
| Lymphoma n (%) | 220 (1.3) | 95 (1.57) | 125 (1.17) | 0.04 |
| CTD, n (%) | 416 (2.49) | 204 (3.37) | 212 (1.99) | <0.001 |
| Lupus, n (%) | 31 (0.1) | 19 (0.31) | 12 (0.11) | <0.001 |
| Rheumatoid arthritis, n (%) | 240 (1.43) | 118 (1.95) | 128 (1.2) | <0.001 |
| AIDS, n (%) | 51 (3.05) | 28 (0.46) | 23 (0.22) | 0.009 |
| AHS, n (%) | 575 (6.16) | 451 (7.5) | 555 (5.2) | <0.001 |
| CCI > 3, n (%) | 2899 (17.73) | 1225 (20.6) | 1674 (16.1) | <0.001 |
| Variable | Total Cohort | Corticosteroids | Not Corticosteroids | p-Value |
|---|---|---|---|---|
| O2 saturation %, SD | 92.9 ± 5.9 | 91.3 ± 6.68 | 93.8 ± 5.31 | <0.001 |
| O2 sat < 93% n (%) | 5590 (34.3) | 2812 (47.6) | 2778 (26.8) | <0.001 |
| PO2 mmHg | 68.82 ± 21.8 | 66.2 ± 21.4 | 70.9 ± 21.9 | <0.001 |
| PCO2 mmHg | 35.52 ± 8.68 | 35.3 ± 8.8 | 35.7 ± 8.59 | 0.01 |
| pH | 7.43 ± 0.18 | 7.44 ± 0.14 | 7.43 ± 0.22 | 0.03 |
| PaO2/FiO2 | 282.82 ± 98.29 | 266 ± 91.1 | 301 ± 101 | <0.001 |
| Leucocytes 106/L | 6300 (4800–8600) | 6700 (4978–9250) | 6110 (4700–8160) | <0.001 |
| Lymphocytes 106/L | 940 (690–1300) | 860 (600–1200) | 1000 (700–1360) | 0.14 |
| Neutrophils 106/L | 4600 (3220–6720) | 5100 (3500–7552) | 4340 (3100–6292) | <0.001 |
| Platelets 109/L | 190 (148–247) | 187 (146–246) | 192 (149–247) | 0.078 |
| Haemoglobin gr/dL | 13.8 (12.6–15) | 13.6 ± 1.96 | 13.7 ± 1.85 | 0.047 |
| CRP (C-reactive protein mg/dL) | 61.5 (20.2–129.79) | 86 (32.7–160) | 49.3 (16–109) | <0.001 |
| Creatinine (mg/dL) | 0.9 (0.73–1.16) | 0.97 (0.78–1.25) | 0.87 (0.71–1.1) | <0.001 |
| Urea (mg/dL) | 37 (27–55) | 42 (30–62) | 35 (26–51) | <0.001 |
| LDH (lactate dehydrogenase UI/L) | 321 (247–431) | 353 (268–468) | 305 (237–411) | <0.001 |
| Ferritin (µg/mL) | 608 (285–1230.8) | 791 (393–1534) | 470 (236–996) | <0.001 |
| Procalcitonin (ng/mL) | 0.1 (0.05–0.22) | 0.13 (0.07–0.3) | 0.09 (0.05–0.18) | <0.001 |
| Dimer-D (ng/mL) | 669 (373–1261) | 750 (430–1400) | 617 (345–1180) | <0.001 |
| X-ray consolidation | ||||
| No | 8687 (52.6) | 3001 (50.1) | 5679 (54) | <0.001 |
| Unilateral | 2796 (16.9) | 920 (15.4) | 1881 (17.9) | |
| Bilateral | 5016 (30.4) | 2068 (34.5) | 2950 (28.1) | |
| X-ray interstitial infiltrates/ground glass opacities | ||||
| No | 5915 (35.84) | 1877 (31.3) | 4038 (38.4) | <0.001 |
| Unilateral | 1699 (10.29) | 515 (8.59) | 1184 (11.3) | |
| Bilateral | 8889 (53.86) | 3604 (60.1) | 5285 (50.3) | |
| Pleural effusion | ||||
| No | 15,727 (95.32) | 5712 (95.3) | 10,015 (95.4) | 0.58 |
| Unilateral | 497 (3.01) | 189 (3.15) | 308 (2.93) | |
| Bilateral | 274 (1.6) | 94 (1.57) | 180 (1.71) | |
| Outcome | ||||
| Discharge home | 12,119 (72.42) | 3946 (65.12) | 8173 (76.6) | <0.001 |
| Discharge care centre | 1226 (7.32) | 422 (6.96) | 804 (7.55) | |
| Death | 3388 (20.24) | 1692 (27.92) | 1696 (15.9) | |
| Variable | Oxygen Saturation above 94 | Oxygen Saturation between 94–91% | Oxygen Saturation Less or Equal to 90% | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| APED (accumulated prednisone equivalent dose) 200–400 | 2.1 (1.5–2.9) | <0.001 | 1.2 (0.9–1.7) | 0.19 | 1 (0.8–1.4) | 0.7 |
| APED 400–600 | 1.7 (1.2–2.4) | 0.003 | 1.3 (0.9–1.8) | 0.12 | 0.7 (0.5–0.9) | 0.007 |
| APED 600–800 | 1.9 (1.3–2.8) | 0.001 | 0.88 (0.6–1.4) | 0.59 | 0.5 (0.4–0.8) | 0.0006 |
| APED > 800 | 2.0 (1.4–2.7) | <0.001 | 0.9 (0.7–1.3) | 0.66 | 0.6 (0.5–0.8) | 0.0002 |
| Charlson index >= 3 | 2.4 | <0.001 | 2.1 (1.7–2.6) | <0.001 | 1.9 (1.6-2.3)) | <0.001 |
| Lymphocytes > 1000 cells/mL | 0.6 (0.5-0.7) | <0.001 | 0.6 (0.5–0.8) | <0.001 | 0.7 (0.6–0.8)) | <0.001 |
| Age 60–70 y | 2.7 (1.8–4.1) | <0.001 | 2.2 (1.5–3.5) | <0.001 | 2.4 (1.7–3.4) | <0.001 |
| Age 70–80 y | 7.3 (5.2–10.6) | <0.001 | 8.4 (5.9–12.3) | <0.001 | 6.0 (4.4–8.2) | <0.001 |
| Age >80 y | 23.7 (16.9–33.9) | <0.001 | 18.6 (13.1–27.2) | <0.001 | 13.9 (10.3–19.2) | <0.001 |
| LDH (lacate dehydrogenase) 250–500 IU/L | 1.5 (1.2–1.9) | 0.0005 | 1.66 (1.3–4.1) | <0.001 | 2.5 (1.9–3.2) | <0.001 |
| LDH > 500 IU/L | 3.8 (2.9–5.1) | <0.001 | 3.1 (2.3–4.1) | <0.001 | 6.5 (4.9–8.7) | <0.001 |
| Woman | 0.8 (0.7–1.0) | 0.13 | 0.7 (0.6–0.9) | 0.0006 | 0.7 (0.6–0.8) | <0.001 |
| Tocilizumab | 2.5 (1.7–3.5) | <0.001 | 2.7 (2.0–3.6) | <0.001 | 1.09 (0.8–1.8) | 0.47 |
| Remdesivir | 0.4 (0.1–1.0) | 0.08 | 0.5 (0.2–1.0) | 0.069 | 0.8 (0.3–1.8) | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balaz, D.; Wikman-Jorgensen, P.E.; Galvañ, V.G.; Rubio-Rivas, M.; de Miguel Campo, B.; López, M.N.; Caleya, J.F.L.; Huelgas, R.G.; Fontán, P.M.P.; Bailón, M.M.; et al. Evolution of the Use of Corticosteroids for the Treatment of Hospitalised COVID-19 Patients in Spain between March and November 2020: SEMI-COVID National Registry. J. Clin. Med. 2021, 10, 4610. https://doi.org/10.3390/jcm10194610
Balaz D, Wikman-Jorgensen PE, Galvañ VG, Rubio-Rivas M, de Miguel Campo B, López MN, Caleya JFL, Huelgas RG, Fontán PMP, Bailón MM, et al. Evolution of the Use of Corticosteroids for the Treatment of Hospitalised COVID-19 Patients in Spain between March and November 2020: SEMI-COVID National Registry. Journal of Clinical Medicine. 2021; 10(19):4610. https://doi.org/10.3390/jcm10194610
Chicago/Turabian StyleBalaz, David, Philip Erick Wikman-Jorgensen, Vicente Giner Galvañ, Manuel Rubio-Rivas, Borja de Miguel Campo, Mariam Noureddine López, Juan Francisco López Caleya, Ricardo Gómez Huelgas, Paula María Pesqueira Fontán, Manuel Méndez Bailón, and et al. 2021. "Evolution of the Use of Corticosteroids for the Treatment of Hospitalised COVID-19 Patients in Spain between March and November 2020: SEMI-COVID National Registry" Journal of Clinical Medicine 10, no. 19: 4610. https://doi.org/10.3390/jcm10194610
APA StyleBalaz, D., Wikman-Jorgensen, P. E., Galvañ, V. G., Rubio-Rivas, M., de Miguel Campo, B., López, M. N., Caleya, J. F. L., Huelgas, R. G., Fontán, P. M. P., Bailón, M. M., Fernández-Garcés, M., Cruz, A. F., García, G. M. G., Rhyman, N., Corral-Gudino, L., Rodríguez-Mancheño, A. L., De La Chica, M. N., García, A. T., Alcalá, J. N., ... on behalf of the SEMI-COVID-19 Network. (2021). Evolution of the Use of Corticosteroids for the Treatment of Hospitalised COVID-19 Patients in Spain between March and November 2020: SEMI-COVID National Registry. Journal of Clinical Medicine, 10(19), 4610. https://doi.org/10.3390/jcm10194610