Translational Research in Retinopathy of Prematurity: From Bedside to Bench and Back Again


Abstract
:1. Introduction
1.1. Background
1.2. Unmet Medical Needs for ROP Treatment
2. Relationship between Oxygen Concentration and Retinal Neovascularization
2.1. The First ROP Epidemic: Learning from the Bedside
2.2. Advances in Respiratory Management: Reduction of Oxygen Supplementation
2.3. Establishment of the Animal Model of ROP: Learning from the Bench
3. Existing Treatments for ROP
3.1. Cryotherapy
3.2. Laser Photocoagulation
3.3. Anti-VEGF Therapy
3.3.1. Bioactivity of VEGF
3.3.2. VEGF Expression in Phase 1 and Phase 2
3.3.3. Clinical Trials with Anti-VEGF Therapy
4. Translational ROP Research: Previous and Ongoing Clinical Trials
4.1. Antioxidants
4.2. Vitamin A
4.3. Adrenocorticotropic Hormone and Steroids
4.4. Erythropoietin
4.5. Insulin-Like Growth Factor 1 and Insulin-Like Growth Factor Binding Protein 3
4.6. Non-Steroidal Anti-Inflammatory Drugs
4.7. ω-3-Polyunsaturated Fatty Acids
4.8. β-Blockers
4.9. Rho-Associated Protein Kinase
5. New Biomarkers and Candidate Targeted Molecules for ROP
5.1. Macrophage Inflammatory Protein-1β
5.2. Mast Cell Tryptase
5.3. Suppressor of Cytokine Signaling-3 and Retinoic Acid Receptor-Related Orphan Receptor Alpha
6. Clinical Trials in Preterm Infants: Differences from Adults
7. Future Prospects
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fielder, A.; Blencowe, H.; O’Connor, A.; Gilbert, C. Impact of retinopathy of prematurity on ocular structures and visual functions. Arch. Dis. Child. Fetal Neonatal Ed. 2014, 100, F179–F184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, C. Retinopathy of prematurity: A global perspective of the epidemics, population of babies at risk and implications for control. Early Hum. Dev. 2008, 84, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Blencowe, H.; Lawn, J.E.; Vazquez, T.; Fielder, A.; Gilbert, C. Preterm-associated visual impairment and estimates of retinopathy of prematurity at regional and global levels for 2010. Pediatr. Res. 2013, 74, 35–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, J.L.; Sorita, A.; Carey, W.A.; Colby, C.E.; Murad, M.H.; Alahdab, F. Interventions to Prevent Retinopathy of Prematurity: A Meta-analysis. Pediatrics 2016, 137, e20153387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.H.; et al. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [Green Version]
- Palmer, E.A.; Flynn, J.T.; Hardy, R.J.; Phelps, D.L.; Phillips, C.L.; Schaffer, D.B.; Tung, B.; Elsas, F.J.; Botsford, J.M.; Braune, K.W.; et al. Incidence and Early Course of Retlnonathy of Prematurity. Ophthalmology 1991, 98, 1628–1640. [Google Scholar] [CrossRef]
- Quinn, G.E.; Barr, C.; Bremer, D.; Fellows, R.; Gong, A.; Hoffman, R.; Repka, M.X.; Shepard, J.; Siatkowski, R.M.; Wade, K.; et al. Changes in course of retinopathy of prematurity from 1986 to 2013: Comparison of three studies in the United States. Ophthalmology 2016, 123, 1595–1600. [Google Scholar] [CrossRef] [Green Version]
- Provis, J.M. Development of the Primate Retinal Vasculature. Prog. Retin. Eye Res. 2001, 20, 799–821. [Google Scholar] [CrossRef]
- Dubis, A.M.; Costakos, D.M.; Subramaniam, C.D.; Godara, P.; Wirostko, W.J.; Carroll, J.; Provis, J.M. Evaluation of Normal Human Foveal Development Using Optical Coherence Tomography and Histologic Examination. Arch. Ophthalmol. 2012, 130, 1291–1300. [Google Scholar] [CrossRef]
- Fulton, A.B.; Hansen, R.M.; Moskowitz, A.; Akula, J.D. The neurovascular retina in retinopathy of prematurity. Prog. Retin. Eye Res. 2009, 28, 452–482. [Google Scholar] [CrossRef] [Green Version]
- Ecsedy, M.; Szamosi, A.; Karko, C.; Zubovics, L.; Varsanyi, B.; Nemeth, J.; Recsan, Z. A comparison of macular structure imaged by optical coherence tomog-raphy in preterm and full-term children. Investig. Ophthalmol. Vis. Sci. 2007, 48, 5207–5211. [Google Scholar] [CrossRef] [PubMed]
- Hammer, D.X.; Iftimia, N.V.; Ferguson, R.D.; Bigelow, C.E.; Ustun, T.E.; Barnaby, A.M.; Fulton, A.B. Foveal Fine Structure in Retinopathy of Prematurity: An Adaptive Optics Fourier Domain Optical Coherence Tomography Study. Investig. Opthalmol. Vis. Sci. 2008, 49, 2061–2070. [Google Scholar] [CrossRef] [PubMed]
- Fulton, A.B.; Hansen, R.M.; Moskowitz, A. The Cone Electroretinogram in Retinopathy of Prematurity. Investig. Opthalmol. Vis. Sci. 2008, 49, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Miki, A.; Yamada, Y.; Nakamura, M. The Size of the Foveal Avascular Zone Is Associated with Foveal Thickness and Structure in Premature Children. J. Ophthalmol. 2019, 2019, 8340729-5. [Google Scholar] [CrossRef]
- Ng, P.C.; Wong, S.P.S.; Chan, I.H.S.; Lam, H.S.; Lee, C.H.; Lam, C.W.K. A Prospective Longitudinal Study to Estimate the “Adjusted Cortisol Percentile” in Preterm Infants. Pediatr. Res. 2011, 69, 511–516. [Google Scholar] [CrossRef] [Green Version]
- Masumoto, K.; Kusuda, S.; Aoyagi, H.; Tamura, Y.; Obonai, T.; Yamasaki, C.; Sakuma, I.; Uchiyama, A.; Nishida, H.; Oda, S.; et al. Comparison of Serum Cortisol Concentrations in Preterm Infants with or Without Late-Onset Circulatory Collapse due to Adrenal Insufficiency of Prematurity. Pediatr. Res. 2008, 63, 686–690. [Google Scholar] [CrossRef] [Green Version]
- Ng, P.C. Adrenocortical insufficiency and refractory hypotension in preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2016, 101, F571–F576. [Google Scholar] [CrossRef]
- Kirchner, L.; Jeitler, V.; Pollak, A.; Müllner-Eidenböck, A.; Weinzettel, R.; Kraschl, R.; Waldhör, T.; Wald, M. Must screening examinations for retinopathy of prematurity necessarily be painful? Retina 2009, 29, 586–591. [Google Scholar] [CrossRef]
- Kleberg, A.; Warren, I.; Norman, E.; Morelius, E.; Berg, A.-C.; Mat-Ali, E.; Holm, K.; Fielder, A.; Nelson, N.; Hellström-Westas, L. Lower Stress Responses After Newborn Individualized Developmental Care and Assessment Program Care During Eye Screening Examinations for Retinopathy of Prematurity: A Randomized Study. Pediatrics 2008, 121, e1267–e1278. [Google Scholar] [CrossRef]
- Arima, M.; Tsukamoto, S.; Fujiwara, K.; Murayama, M.; Fujikawa, K.; Sonoda, K.-H. Late-onset Circulatory Collapse and Continuous Positive Airway Pressure are Useful Predictors of Treatment-requiring Retinopathy of Prematurity: A 9-year Retrospective Analysis. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Heller, M.J. DNA Microarray Technology: Devices, Systems, and Applications. Annu. Rev. Biomed. Eng. 2002, 4, 129–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, M.; Jensen, O.N. Proteomic analysis of post-translational modifications. Nat. Biotechnol. 2003, 21, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Ozsolak, F.; Milos, P.M. RNA sequencing: Advances, challenges and opportunities. Nat. Rev. Genet. 2010, 12, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Chari, R.V. Targeted Cancer Therapy: Conferring Specificity to Cytotoxic Drugs. Acc. Chem. Res. 2008, 41, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Ellis, L.M.; Hicklin, D.J. VEGF-targeted therapy: Mechanisms of anti-tumour activity. Nat. Rev. Cancer 2008, 8, 579–591. [Google Scholar] [CrossRef] [PubMed]
- Sawyers, C.L. Targeted cancer therapy. Nat. Cell Biol. 2004, 432, 294–297. [Google Scholar] [CrossRef]
- Levy-Clarke, G.; Jabs, D.A.; Read, R.W.; Rosenbaum, J.T.; Vitale, A.; Van Gelder, R.N. Expert Panel Recommendations for the Use of Anti–Tumor Necrosis Factor Biologic Agents in Patients with Ocular Inflammatory Disorders. Ophthalmology 2014, 121, 785–796.e3. [Google Scholar] [CrossRef]
- Andreoli, C.M.; Miller, J.W. Anti-vascular endothelial growth factor therapy for ocular neovascular disease. Curr. Opin. Ophthalmol. 2007, 18, 502–508. [Google Scholar] [CrossRef]
- Gillies, M.C.; Hunyor, A.P.; Arnold, J.J.; Guymer, R.H.; Wolf, S.; Ng, P.; Pecheur, F.L.; McAllister, I.L. Effect of ranibizumab and aflibercept on best-corrected visual acuity in treat-and-extend for neovascular age-related macular degeneration: A randomized clinical trial. JAMA Ophthalmol. 2019, 137, 372–379. [Google Scholar] [CrossRef]
- Tadayoni, R.; Waldstein, S.M.; Boscia, F.; Gerding, H.; Gekkieva, M.; Barnes, E.; Das Gupta, A.; Wenzel, A.; Pearce, I. Sustained benefits of ranibizumab with or without laser in branch retinal vein occlusion: 24-month results of the BRIGHTER study. Ophthalmology 2017, 124, 1778–1787. [Google Scholar] [CrossRef] [Green Version]
- Heier, J.S.; Korobelnik, J.F.; Brown, D.M.; Schmidt-Erfurth, U.; Do, D.V.; Midena, E.; Boyer, D.S.; Terasaki, H.; Kaiser, P.K.; Marcus, D.M.; et al. Intravitreal aflibercept for diabetic macular edema: 148-week results from the VISTA and VIVID studies. Ophthalmology 2016, 123, 2376–2385. [Google Scholar] [CrossRef] [PubMed]
- Garcia Gonzalez, J.M.; Snyder, L.; Blair, M.; Rohr, A.; Shapiro, M.; Greenwald, M. Prophylactic peripheral laser and fluorescein angiography afer bevacizumab for retinopathy of prematurity. Retina 2017, 38, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Snyder, L.L.; Garcia-Gonzalez, J.M.; Shapiro, M.J.; Blair, M.P. Very Late Reactivation of Retinopathy of Prematurity After Monotherapy with Intravitreal Bevacizumab. Ophthalmic Surg. Lasers Imaging Retin. 2016, 47, 280–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajrasouliha, A.R.; Garcia-Gonzales, J.M.; Shapiro, M.J.; Yoon, H.; Blair, M.P. Reactivation of Retinopathy of Prematurity Three Years After Treatment with Bevacizumab. Ophthalmic Surg. Lasers Imaging Retin. 2017, 48, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Blair, M.P.; Shapiro, M.J.; Lichtenstein, S.J.; Galasso, J.M.; Kapur, R. Reactivation of Retinopathy of Prematurity After Bevacizumab Injection. Arch. Ophthalmol. 2012, 130, 1000–1006. [Google Scholar] [CrossRef]
- Wu, W.-C.; Lien, R.; Liao, P.-J.; Wang, N.-K.; Chen, Y.-P.; Chao, A.-N.; Chen, K.-J.; Chen, T.-L.; Hwang, Y.-S.; Lai, C.-C. Serum Levels of Vascular Endothelial Growth Factor and Related Factors After Intravitreous Bevacizumab Injection for Retinopathy of Prematurity. JAMA Ophthalmol. 2015, 133, 391–397. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.-C.; Shih, C.-P.; Lien, R.; Wang, N.-K.; Chen, Y.-P.; Chao, A.-N.; Chen, K.-J.; Chen, T.-L.; Hwang, Y.-S.; Lai, C.-C. Serum vascular endothelial growth factor after bevacizumab or ranibizumab treatment for retinopathy of prematurity. Retina 2017, 37, 694–701. [Google Scholar] [CrossRef]
- Lien, R.; Yu, M.-H.; Hsu, K.-H.; Liao, P.-J.; Chen, Y.-P.; Lai, C.-C.; Wu, W.-C. Neurodevelopmental Outcomes in Infants with Retinopathy of Prematurity and Bevacizumab Treatment. PLoS ONE 2016, 11, e0148019. [Google Scholar] [CrossRef] [Green Version]
- Natarajan, G.; Shankaran, S.; Nolen, T.L.; Sridhar, A.; Kennedy, K.A.; Hintz, S.R.; Phelps, D.L.; DeMauro, S.B.; Carlo, W.A.; Gantz, M.G.; et al. Neurodevelopmental Outcomes of Preterm Infants with Retinopathy of Prematurity by Treatment. Pediatrics 2019, 144, e20183537. [Google Scholar] [CrossRef]
- Arima, M.; Akiyama, M.; Fujiwara, K.; Mori, Y.; Inoue, H.; Seki, E.; Nakama, T.; Tsukamoto, S.; Ochiai, M.; Ohga, S.; et al. Neurodevelopmental outcomes following intravitreal bevacizumab injection in Japanese preterm infants with type 1 retinopathy of prematurity. PLoS ONE 2020, 15, e0230678. [Google Scholar] [CrossRef]
- Wu, A.L.; Wu, W.C. Anti-VEGF for ROP and pediatric retinal diseases. Asia Pac. J. Ophthalmol. 2018, 7, 145–151. [Google Scholar] [CrossRef]
- McCourt, E.; Ying, G.-S.; Lynch, A.M.; Palestine, A.G.; Wagner, B.D.; Wymore, E.; Tomlinson, L.A.; Binenbaum, G. G-ROP Study Group Validation of the Colorado Retinopathy of Prematurity Screening Model. JAMA Ophthalmol. 2018, 136, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Pivodic, A.; Hård, A.L.; Löfqvist, C.; Smith, L.E.H.; Wu, C.; Bründer, M.C.; Lagrèze, W.A.; Stahl, A.; Holmström, G.; Albertsson-Wikland, K.; et al. Individual risk prediction for sight-threatening retinopathy of prematurity using birth characteristics. JAMA Ophthalmol. 2020, 138, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Ying, G.-S.; Vanderveen, D.K.; Daniel, E.; Quinn, G.E.; Baumritter, A. Telemedicine Approaches to Evaluating Acute-Phase Retinopathy of Prematurity Cooperative Group Risk Score for Predicting Treatment-Requiring Retinopathy of Prematurity (ROP) in the Telemedicine Approaches to Evaluating Acute-Phase ROP Study. Ophthalmology 2016, 123, 2176–2182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Löfqvist, C.; Andersson, E.; Sigurdsson, J.; Engström, E.; Hård, A.-L.; Niklasson, A.; Smith, L.E.H.; Hellström, A. Longitudinal Postnatal Weight and Insulin-like Growth Factor I Measurements in the Prediction of Retinopathy of Prematurity. Arch. Ophthalmol. 2006, 124, 1711–1718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellström, A.; Hård, A.-L.; Engström, E.; Niklasson, A.; Andersson, E.; Smith, L.; Löfqvist, C. Early Weight Gain Predicts Retinopathy in Preterm Infants: New, Simple, Efficient Approach to Screening. Pediatrics 2009, 123, e638–e645. [Google Scholar] [CrossRef] [Green Version]
- Eckert, G.U.; Filho, J.B.F.; Maia, M.; Procianoy, R.S. A predictive score for retinopathy of prematurity in very low birth weight preterm infants. Eye 2011, 26, 400–406. [Google Scholar] [CrossRef] [Green Version]
- Binenbaum, G.; Ying, G.-S.; Quinn, G.E.; Huang, J.; Dreiseitl, S.; Antigua, J.; Foroughi, N.; Abbasi, S. The CHOP Postnatal Weight Gain, Birth Weight, and Gestational Age Retinopathy of Prematurity Risk Model. Arch. Ophthalmol. 2012, 130, 1560–1565. [Google Scholar] [CrossRef]
- Van Sorge, A.J.; Schalij-Delfos, N.E.; Kerkhoff, F.T.; Van Rijn, L.J.; Van Hillegersberg, J.L.A.M.; Van Liempt, I.L.A.; Peer, P.G.M.; Simonsz, H.J.; Termote, J.U.M. Reduction in screening for retinopathy of prematurity through risk factor adjusted inclusion criteria. Br. J. Ophthalmol. 2013, 97, 1143–1147. [Google Scholar] [CrossRef] [Green Version]
- Greenwald, M.F.; Danford, I.D.; Shahrawat, M.; Ostmo, S.; Brown, J.; Kalpathy-Cramer, J.; Bradshaw, K.; Schelonka, R.; Cohen, H.S.; Chan, R.V.P.; et al. Evaluation of artificial intelligence-based telemedicine screening for retinopathy of prematurity. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2020, 160–162. [Google Scholar] [CrossRef]
- Brown, J.M.; Campbell, J.P.; Beers, A.; Chang, K.; Ostmo, S.; Chan, R.V.P.; Dy, J.; Erdoğmuş, D.; Ioannidis, S.; Kalpathy-Cramer, J.; et al. Automated Diagnosis of Plus Disease in Retinopathy of Prematurity Using Deep Convolutional Neural Networks. JAMA Ophthalmol. 2018, 136, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Robertson, A.F. Reflections on Errors in Neonatology: I. The “Hands-Off” Years, 1920 to 1950. J. Perinatol. 2003, 23, 48–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zacharias, L.; Reynolds, W.E.; Chisholm, J.F.; King, M.J. The incidence and severity of retrolental fibroplasia in relation to possible causative factors*. Am. J. Ophthalmol. 1954, 38, 317–336. [Google Scholar] [CrossRef]
- Terry, T. Extreme prematurity and fibroblastic overgrowth of persistent vascular sheath behind each crystalline lens. Am. J. Ophthalmol. 1942, 25, 203–204. [Google Scholar] [CrossRef]
- Terry, T.L. Ocular maldevelopment in extremely premature infants. J. Am. Med. Assoc. 1945, 128, 582–585. [Google Scholar] [CrossRef]
- Owens, W.C.; Owens, E.U. Retrolental Fibroplasia in Premature Infants*: II. Studies on the Prophylaxis of the Disease: The use of Alpha Tocopheryl Acetate. Am. J. Ophthalmol. 1949, 32, 1631–1637. [Google Scholar] [CrossRef]
- Reese, A.B.; Blodi, F.C. Retrolental fibroplasia. Am. J. Ophthalmol. 1951, 34, 1–24. [Google Scholar] [CrossRef]
- International Committee for the Classification of Retinopathy of Prematurity. The international classification of retinopathy of prematurity revisited. Arch. Ophthalmol. 2005, 123, 991–999. [Google Scholar] [CrossRef]
- The Committee for the Classification of Retinopathy of Prematurity. An international classification of retinopathy of prematurity. Arch. Ophthalmol. 1984, 102, 1130–1134. [Google Scholar] [CrossRef]
- Szewczyk, T.S. Retrolental fibroplasia; etiology and prophylaxis. Am. J. Ophthalmol. 1952, 35, 301–311. [Google Scholar] [CrossRef]
- Ingalls, T.H.; Tedeschi, C.G.; Helpern, M.M. Congenital malformations of the eye induced in mice by maternal anoxia; with particular reference to the problem of retrolental fibroplasia in man. Am. J. Ophthalmol. 1952, 35, 311–329. [Google Scholar] [CrossRef]
- Campbell, K. Intensive oxygen therapy as a possible cause of retrolental fibroplasia: A clinical approach. Med. J. Aust. 1951, 2, 48–50. [Google Scholar] [CrossRef] [PubMed]
- Silverman, W.A.; Blodi, F.C.; Locke, J.C.; Day, R.L.; Reese, A.B. Incidence of retrolental fibroplasia in a New York nursery. Arch. Ophthalmol. 1952, 48, 698–711. [Google Scholar] [CrossRef] [PubMed]
- Lanman, J.T.; Guy, L.P.; Dancis, J. Retrolental fibroplasia and oxygen therapy. J. Am. Med. Assoc. 1954, 155, 223–226. [Google Scholar] [CrossRef]
- Patz, A.; Hoeck, L.E.; De La Cruz, E. Studies on the Effect of High Oxygen Administration in Retrolental Fibroplasia*. Am. J. Ophthalmol. 1952, 35, 1248–1253. [Google Scholar] [CrossRef]
- Shohat, M.; Reisner, S.H.; Krikler, R.; Nissenkorn, I.; Yassur, Y.; Ben-Sira, I. Retinopathy of prematurity: Incidence and risk factors. Pediatrics 1983, 72, 159–163. [Google Scholar] [CrossRef]
- Bancalari, E.; Flynn, J.; Goldberg, R.N.; Bawol, R.; Cassady, J.; Schiffman, J.; Feuer, W.; Roberts, J.; Gillings, D.; Sim, E. Influence of transcutaneous oxygen monitoring on the incidence of retinopathy of prematurity. Pediatrics 1987, 79, 663–669. [Google Scholar]
- Kinsey, V.E.; Arnold, H.J.; Kalina, R.E.; Stern, L.; Stahlman, M.; Odell, G.; Driscoll, J.M.; Elliott, J.H.; Payne, J.; Patz, A. PaO2 levels and retrolental fibroplasia: A report of the cooperative study. Pediatrics 1977, 60, 655–668. [Google Scholar]
- Flynn, J.T.; Bancalari, E.; Bawol, R.; Goldberg, R.; Cassady, J.; Schiffman, J.; Feuer, W.; Roberts, J.; Gillings, D.; Sim, E.; et al. Retinopathy of prematurity: A randomized, prospective trial of transcutaneous oxygen monitoring. Ophthalmology 1987, 94, 630–638. [Google Scholar] [CrossRef]
- Jennis, M.S.; Peabody, J.L. Pulse oximetry: An alternative method for the assessment of oxygenation in newborn infants. Pediatrics 1987, 79, 524–528. [Google Scholar]
- Yoshiya, I.; Shimada, Y.; Tanaka, K. Spectrophotometric monitoring of arterial oxygen saturation in the fingertip. Med. Biol. Eng. Comput. 1980, 18, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Southall, D.P.; Bignall, S.; Stebbens, V.A.; Alexander, J.R.; Rivers, R.P.; Lissauer, T. Pulse oximeter and transcutaneous arterial oxygen measurements in neonatal and paediatric intensive care. Arch. Dis. Child. 1987, 62, 882–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flynn, J.T.; Bancalari, E.; Snyder, E.S.; Goldberg, R.N.; Feuer, W.; Cassady, J.; Schiffman, J.; Feldman, H.I.; Baghynski, B.; Buckley, E.; et al. A Cohort Study of Transcutaneous Oxygen Tension and the Incidence and Severity of Retinopathy of Prematurity. N. Engl. J. Med. 1992, 326, 1050–1054. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, B.; Whyte, R.K.; Asztalos, E.V.; Moddemann, D.; Poets, C.; Rabi, Y.; Solimano, A.; Roberts, R.S. Effects of targeting higher vs lower arterial oxygen saturations on death or disability in extremely preterm infants: A randomized clinical trial. JAMA 2013, 309, 2111–2120. [Google Scholar] [CrossRef]
- Phelps, D.L. Supplemental therapeutic oxygen for prethreshold retinopathy of prematurity (STOP-ROP), a randomized, controlled trial. I: Primary outcomes. Pediatrics 2000, 105, 295–310. [Google Scholar]
- Schaapveld, M.; Aleman, B.M.P.; van Eggermond, A.M.; Janus, C.P.M.; Krol, A.D.G.; van der Maazen, R.W.M.; Roesink, J.; Raemaekers, J.M.M.; de Boer, J.P.; Zijlstra, J.M.; et al. Target ranges of oxygen saturation in extremely preterm infants. N. Engl. J. Med. 2010, 362, 1959–1969. [Google Scholar]
- Askie, L.M.; Henderson-Smart, D.J.; Irwig, L.; Simpson, J.M. Oxygen-Saturation Targets and Outcomes in Extremely Preterm Infants. N. Engl. J. Med. 2003, 349, 959–967. [Google Scholar] [CrossRef] [Green Version]
- Stenson, B.J.; Tarnow-Mordi, W.O.; Darlow, B.A.; Simes, J.; Juszczak, E.; Askie, L.M.; Battin, M.R.; Bowler, U.; Broadbent, R.S.; Cairns, P.; et al. Oxygen Saturation and Outcomes in Preterm Infants. N. Engl. J. Med. 2013, 368, 2094–2104. [Google Scholar] [CrossRef] [Green Version]
- Tarnow-Mordi, W.; Stenson, B.; Kirby, A.; Juszczak, E.; Donoghoe, M.; Deshpande, S.; Morley, C.; King, A.; Doyle, L.W.; Fleck, B.W.; et al. Outcomes of two trials of oxygen-saturation targets in preterm infants. N. Engl. J. Med. 2016, 374, 749–760. [Google Scholar]
- Askie, L.M.; Darlow, B.A.; Finer, N.; Schmidt, B.; Stenson, B.; Tarnow-Mordi, W.; Davis, P.G.; Carlo, W.A.; Brocklehurst, P.; Davies, L.C.; et al. Association Between Oxygen Saturation Targeting and Death or Disability in Extremely Preterm Infants in the Neonatal Oxygenation Prospective Meta-analysis Collaboration. JAMA 2018, 319, 2190–2201. [Google Scholar] [CrossRef]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Pas, A.T.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; Simeoni, U.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome—2019 Update. Neonatology 2019, 115, 432–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummings, J.J.; Polin, R.A. Committee on Fetus and Newborn Oxygen Targeting in Extremely Low Birth Weight Infants. Pediatrics 2016, 138, e20161576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirpalani, H.; Millar, D.; Lemyre, B.; Yoder, B.A.; Chiu, A.; Roberts, R.S. A Trial Comparing Noninvasive Ventilation Strategies in Preterm Infants. N. Engl. J. Med. 2013, 369, 611–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, P.G.; Schmidt, B.; Roberts, R.S.; Doyle, L.W.; Asztalos, E.; Haslam, R.; Sinha, S.; Tin, W. Caffeine for Apnea of Prematurity Trial: Benefits May Vary in Subgroups. J. Pediatr. 2010, 156, 382–387.e3. [Google Scholar] [CrossRef] [PubMed]
- Finer, N.N.; Carlo, W.A.; Walsh, M.C.; Rich, W.; Gantz, M.G.; Laptook, A.R.; Yoder, B.A.; Faix, R.G.; Das, A.; Poole, W.K.; et al. Early CPAP versus surfactant in extremely preterm infants. N. Engl. J. Med. 2010, 362, 1970–1979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennefather, P.M.; Tin, W.; Clarke, M.P.; Fritz, S.; Strong, N.P. Retinopathy of prematurity in a controlled trial of prophylactic surfactant treatment. Br. J. Ophthalmol. 1996, 80, 420–424. [Google Scholar] [CrossRef]
- Kinsey, V.E.; Jacobus, J.T.; Hemphill, F.M. Retrolental Fibroplasia. A.M.A. Arch. Ophthalmol. 1956, 56, 481–543. [Google Scholar] [CrossRef]
- Lucey, J.F.; Dangman, B. A reexamination of the role of oxygen in retrolental fibroplasia. Pediatrics 1984, 73, 82–96. [Google Scholar]
- Ashton, N.; Ward, B.; Serpell, G. Effect of Oxygen on Developing Retinal Vessels with Particular Reference to the Problem of Retrolental Fibroplasia. Br. J. Ophthalmol. 1954, 38, 397–432. [Google Scholar] [CrossRef] [Green Version]
- Ashton, N. Retinal Vascularization in Health and Disease. Am. J. Ophthalmol. 1957, 44, 7–17. [Google Scholar] [CrossRef]
- Dollery, C.T.; Hill, D.W.; Mailer, C.M.; Ramalho, P.S. High oxygen pressureand the retinal blood-vessels. Lancet 1964, 2, 291–292. [Google Scholar] [CrossRef]
- Dollery, C.T.; Bulpitt, C.J.; Kohner, E.M. Oxygen supply to the retina from the retinal and choroidal circulations at normal and increased arterial oxygen tensions. Investig. Ophthalmol. 1969, 8, 588–594. [Google Scholar]
- Wellard, J.; Lee, D.; Valter, K.; Stone, J. Photoreceptors in the rat retina are specifically vulnerable to both hypoxia and hyperoxia. Vis. Neurosci. 2005, 22, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Fulton, A.B.; Reynaud, X.; Hansen, R.M.; Lemere, C.A.; Parker, C.; Williams, T.P. Rod photoreceptors in infant rats with a history of oxygen exposure. Investig. Ophthalmol. Vis. Sci. 1999, 40, 168–174. [Google Scholar]
- Mezu-Ndubuisi, O.J.; Macke, E.L.; Kalavacherla, R.; Nwaba, A.A.; Suscha, A.; Zaitoun, I.S.; Ikeda, A.; Sheibani, N. Long-term evaluation of retinal morphology and function in a mouse model of oxygen-induced retinopathy. Mol. Vis 2020, 26, 257–276. [Google Scholar]
- Hellström, A.; Smith, L.E.H.; Dammann, O. Retinopathy of prematurity. Lancet 2013, 382, 1445–1457. [Google Scholar] [CrossRef] [Green Version]
- Kremer, I.; Kissun, R.; Nissenkorn, I.; Ben-Sira, I.; Garner, A. Oxygen-induced retinopathy in newborn kittens. A model for ischemic vasoproliferative retinopathy. Investig. Ophthalmol. Vis. Sci. 1987, 28, 126–130. [Google Scholar]
- Phelps, D.L. Reduced Severity of Oxygen-Induced Retinopathy in Kittens Recovered in 28% Oxygen. Pediatr. Res. 1988, 24, 106–109. [Google Scholar] [CrossRef] [Green Version]
- Flower, R.W.; Blake, D.A.; Wajer, S.D.; Egner, P.G.; McLeod, D.S.; Pitts, S.M. Retrolental Fibroplasia: Evidence for a Role of the Prostaglandin Cascade in the Pathogenesis of Oxygen-Induced Retinopathy in the Newborn Beagle. Pediatr. Res. 1981, 15, 1293–1302. [Google Scholar] [CrossRef] [Green Version]
- McLeod, D.S.; Brownstein, R.; Lutty, G.A. Vaso-obliteration in the canine model of oxygen-induced retinopathy. Investig. Ophthalmol. Vis. Sci. 1996, 37, 300–311. [Google Scholar]
- McLeod, D.S.; Crone, S.N.; Lutty, G.A. Vasoproliferation in the neonatal dog model of oxygen-induced retinopathy. Investig. Ophthalmol. Vis. Sci. 1996, 37, 1322–1333. [Google Scholar]
- McLeod, D.S.; D’Anna, S.A.; Lutty, G.A. Clinical and histopathologic features of canine oxygen-induced proliferative retinopathy. Investig. Ophthalmol. Vis. Sci. 1998, 39, 1918–1932. [Google Scholar]
- Penn, J.S.; Henry, M.M.; Tolman, B.L. Exposure to Alternating Hypoxia and Hyperoxia Causes Severe Proliferative Retinopathy in the Newborn Rat. Pediatr. Res. 1994, 36, 724–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, L.E.; Wesolowski, E.; McLellan, A.; Kostyk, S.K.; D’Amato, R.; Sullivan, R.; D’Amore, P.A. Oxygen-induced retinopathy in the mouse. Investig. Ophthalmol. Vis. Sci. 1994, 35, 101–111. [Google Scholar]
- Connor, K.M.; Krah, N.M.; Dennison, R.J.; Aderman, C.M.; Chen, J.; Guerin, K.I.; Sapieha, P.; Stahl, A.; Willett, K.L.; Smith, L.M. Quantification of oxygen-induced retinopathy in the mouse: A model of vessel loss, vessel regrowth and pathological angiogenesis. Nat. Protoc. 2009, 4, 1565–1573. [Google Scholar] [CrossRef] [Green Version]
- Patz, A. Oxygen Studies in Retrolental Fibroplasia. Am. J. Ophthalmol. 1954, 38, 291–308. [Google Scholar] [CrossRef]
- Ashton, N.; Blach, R. Studies on developing retinal vessels VIII. Effect of oxygen on the retinal vessels of the ratling. Br. J. Ophthalmol. 1961, 45, 321–340. [Google Scholar] [CrossRef] [Green Version]
- Penn, J.S.; Tolman, B.L.; Lowery, L.A. Variable oxygen exposure causes preretinal neovascularization in the newborn rat. Investig. Ophthalmol. Vis. Sci. 1993, 34, 576–585. [Google Scholar]
- Kubota, Y.; Takubo, K.; Shimizu, T.; Ohno, H.; Kishi, K.; Shibuya, M.; Saya, H.; Suda, T. M-CSF inhibition selectively targets pathological angiogenesis and lymphangiogenesis. J. Cell Biol. 2009, 185, i6. [Google Scholar] [CrossRef] [Green Version]
- Tasman, W.; Brown, G.C.; Schaffer, D.B.; Quinn, G.; Naidoff, M.; Benson, W.E.; Diamond, G. Cryotherapy for Active Retinopathy of Prematurity. Ophthalmology 1986, 93, 580–585. [Google Scholar] [CrossRef]
- Ben-Sira, I.; Nissenkorn, I.; Grunwald, E.; Yassur, Y. Treatment of acute retrolental fibroplasia by cryopexy. Br. J. Ophthalmol. 1980, 64, 758–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cryotherapy for Retinopathy of Prematurity Cooperative Group. Multicenter trial of cryotherapy for retinopathy of prematurity: Preliminary results. Pediatrics 1988, 81, 697–706. [Google Scholar]
- Cryotherapy for Retinopathy of Prematurity Cooperative Group. Multicenter trial of cryotherapy for retinopathy of prematurity: Ophthalmological outcomes at 10 years. Arch. Ophthalmol. 2001, 119, 1110–1118. [Google Scholar] [CrossRef] [Green Version]
- Good, W.V.; Hardy, R.J. The multicenter study of Early Treatment for Retinopathy of Prematurity (ETROP). Ophthalmology 2001, 108, 1013–1014. [Google Scholar] [CrossRef]
- Simpson, J.L.; Melia, M.; Yang, M.B.; Buffenn, A.N.; Chiang, M.F.; Lambert, S.R. Current role of cryotherapy in retinopathy of prematurity: A report by the American academy of ophthalmology. Ophthalmology 2012, 119, 873–877. [Google Scholar] [CrossRef]
- McNamara, J.A.; Tasman, W.; Brown, G.C.; Federman, J.L. Laser Photocoagulation for Stage 3+ Retinopathy of Prematurity. Ophthalmology 1991, 98, 576–580. [Google Scholar] [CrossRef]
- Vander, J.F.; Handa, J.; McNamara, J.A.; Trese, M.; Spencer, R.; Repka, M.X.; Rubsamen, P.; Li, H.; Morse, L.S.; Tasman, W.S. Early treatment of posterior retinopathy of prematurity: A controlled trial. Ophthalmology 1997, 104, 1731–1736. [Google Scholar] [CrossRef]
- McNamara, J.A.; Tasman, W.; Vander, J.F.; Brown, G.C. Diode laser photocoagulation for retinopathy of prematurity: Preliminary results. Arch. Ophthalmol. 1992, 110, 1714–1716. [Google Scholar] [CrossRef]
- Landers, M.B.; Toth, C.A.; Semple, H.C.; Morse, L.S. Treatment of Retinopathy of Prematurity with Argon Laser Photocoagulation. Arch. Ophthalmol. 1992, 110, 44–47. [Google Scholar] [CrossRef]
- Shalev, B.; Farr, A.K.; Repka, M.X. Randomized comparison of diode laser photocoagulation versus cryotherapy for threshold retinopathy of prematurity: Seven-year outcome. Am. J. Ophthalmol. 2001, 132, 76–80. [Google Scholar] [CrossRef]
- Ng, E.Y.; Connolly, B.P.; McNamara, J.; Regillo, C.D.; Vander, J.F.; Tasman, W. A comparison of laser photocoagulation with cryotherapy for threshold retinopathy of prematurity at 10 years. Ophthalmology 2002, 109, 928–934. [Google Scholar] [CrossRef]
- Connolly, B.P.; Ng, E.Y.; McNamara, J.A.; Regillo, C.D.; Vander, J.F.; Tasman, W. A comparison of laser photocoagulation with cryotherapy for threshold retinopathy of prematurity at 10 years: Part 2. Refractive outcome. Ophthalmology 2002, 109, 936–941. [Google Scholar] [CrossRef]
- Good, W.V. Early treatment for retinopathy of prematurity cooperative group. Final results of the early treatment for retinopathy of prematurity (ETROP) randomized trial. Trans. Am. Ophthalmol. Soc. 2004, 102, 233–250. [Google Scholar] [PubMed]
- O’Connor, A.R.; Stephenson, T.; Johnson, A.; Tobin, M.J.; Moseley, M.J.; Ratib, S.; Ng, Y.; Fielder, A.R. Long-Term Ophthalmic Outcome of Low Birth Weight Children with and Without Retinopathy of Prematurity. Pediatrics 2002, 109, 12–18. [Google Scholar] [CrossRef]
- Fielder, A.R.; Quinn, G.E. Myopia of prematurity: Nature, nurture, or disease? Br. J. Ophthalmol. 1997, 81, 2–3. [Google Scholar] [CrossRef] [Green Version]
- Houston, S.K.; Wykoff, C.C.; Berrocal, A.M.; Hess, D.J.; Murray, T.G. Laser treatment for retinopathy of prematurity. Lasers Med. Sci. 2013, 28, 683–692. [Google Scholar] [CrossRef]
- Yang, C.-S.; Wang, A.-G.; Shih, Y.-F.; Hsu, W.-M. Long-term biometric optic components of diode laser-treated threshold retinopathy of prematurity at 9 years of age. Acta Ophthalmol. 2013, 91, e276–e282. [Google Scholar] [CrossRef]
- Senger, D.R.; Galli, S.J.; Dvorak, A.M.; Perruzzi, C.A.; Harvey, V.S.; Dvorak, H.F. Tumor cells secrete a vascular permeability factor that promotes accumulation of ascites fluid. Science 1983, 219, 983–985. [Google Scholar] [CrossRef]
- Ferrara, N.; Henzel, W.J. Pituitary follicular cells secrete a novel heparin-binding growth factor specific for vascular endothelial cells. Biochem. Biophys. Res. Commun. 1989, 161, 851–858. [Google Scholar] [CrossRef]
- Keck, P.J.; Hauser, S.D.; Krivi, G.; Sanzo, K.; Warren, T.; Feder, J.; Connolly, D.T. Vascular permeability factor, an endothelial cell mitogen related to PDGF. Science 1989, 246, 1309–1312. [Google Scholar] [CrossRef]
- Leung, D.W.; Cachianes, G.; Kuang, W.J.; Goeddel, D.V.; Ferrara, N. Vascular endothelial growth factor is a secreted angiogenic mitogen. Science 1989, 246, 1306–1309. [Google Scholar] [CrossRef] [PubMed]
- Aiello, L.M.; Avery, R.L.; Arrigg, P.G.; Keyt, B.A.; Jampel, H.D.; Shah, S.T.; Pasquale, L.R.; Thieme, H.; Iwamoto, M.A.; Park, J.E.; et al. Vascular Endothelial Growth Factor in Ocular Fluid of Patients with Diabetic Retinopathy and Other Retinal Disorders. N. Engl. J. Med. 1994, 331, 1480–1487. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Kusaka, S.; Shimojo, H.; Fujikado, T. Simultaneous Analyses of Vitreous Levels of 27 Cytokines in Eyes with Retinopathy of Prematurity. Ophthalmology 2009, 116, 2165–2169. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, E.; Achen, M.G.; Breier, G.; Risau, W. Hypoxia-induced Transcriptional Activation and Increased mRNA Stability of Vascular Endothelial Growth Factor in C6 Glioma Cells. J. Biol. Chem. 1995, 270, 19761–19766. [Google Scholar] [CrossRef] [Green Version]
- Damert, A.; Ikeda, E.; Risau, W. Activator-protein-1 binding potentiates the hypoxia-induciblefactor-1-mediated hypoxia-induced transcriptional activation of vascular-endothelial growth factor expression in C6 glioma cells. Biochem. J. 1997, 327, 419–423. [Google Scholar] [CrossRef]
- Wang, G.L.; Semenza, G.L. Purification and Characterization of Hypoxia-inducible Factor 1. J. Biol. Chem. 1995, 270, 1230–1237. [Google Scholar] [CrossRef] [Green Version]
- Semenza, G.L. Life with Oxygen. Science 2007, 318, 62–64. [Google Scholar] [CrossRef]
- Pugh, C.W.; Ratcliffe, P.J. Regulation of angiogenesis by hypoxia: Role of the HIF system. Nat. Med. 2003, 9, 677–684. [Google Scholar] [CrossRef]
- Apte, R.S.; Chen, D.S.; Ferrara, N. VEGF in Signaling and Disease: Beyond Discovery and Development. Cell 2019, 176, 1248–1264. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, N. Vascular Endothelial Growth Factor: Basic Science and Clinical Progress. Endocr. Rev. 2004, 25, 581–611. [Google Scholar] [CrossRef]
- Shibuya, M.; Claesson-Welsh, L. Signal transduction by VEGF receptors in regulation of angiogenesis and lymphangiogenesis. Exp. Cell Res. 2006, 312, 549–560. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, N. Molecular and biological properties of vascular endothelial growth factor. J. Mol. Med. 1999, 77, 527–543. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, K.; Economides, D.; Soothill, P. Blood gases, pH, and lactate in appropriate- and small-for-gestational-age fetuses. Am. J. Obstet. Gynecol. 1989, 161, 996–1001. [Google Scholar] [CrossRef]
- Stone, J.; Itin, A.; Alon, T.; Pe’Er, J.; Gnessin, H.; Chan-Ling, T.; Keshet, E. Development of retinal vasculature is mediated by hypoxia-induced vascular endothelial growth factor (VEGF) expression by neuroglia. J. Neurosci. 1995, 15, 4738–4747. [Google Scholar] [CrossRef] [PubMed]
- Alon, T.; Hemo, I.; Itin, A.; Pe’Er, J.; Stone, J.; Keshet, E. Vascular endothelial growth factor acts as a survival factor for newly formed retinal vessels and has implications for retinopathy of prematurity. Nat. Med. 1995, 1, 1024–1028. [Google Scholar] [CrossRef]
- Pierce, E.A.; Avery, R.L.; Foley, E.D.; Aiello, L.P.; Smith, L.E. Vascular endothelial growth factor/vascular permeability factor expression in a mouse model of retinal neovascularization. Proc. Natl. Acad. Sci. USA 1995, 92, 905–909. [Google Scholar] [CrossRef] [Green Version]
- Hoppe, G.; Yoon, S.; Gopalan, B.; Savage, A.R.; Brown, R.; Case, K.; Vasanji, A.; Chan, E.R.; Silver, R.B.; Sears, J. Comparative systems pharmacology of HIF stabilization in the prevention of retinopathy of prematurity. Proc. Natl. Acad. Sci. USA 2016, 113, E2516–E2525. [Google Scholar] [CrossRef] [Green Version]
- Kusaka, S.; Shima, C.; Wada, K.; Arahori, H.; Shimojyo, H.; Sato, T.; Fujikado, T. Efficacy of intravitreal injection of bevacizumab for severe retinopathy of prematurity: A pilot study. Br. J. Ophthalmol. 2008, 92, 1450–1455. [Google Scholar] [CrossRef]
- Lalwani, G.A.; Berrocal, A.M.; Murray, T.G.; Buch, M.; Cardone, S.; Hess, D.; Johnson, R.A.; Puliafito, C.A. Off-label use of intravitreal bevacizumab (avastin) for salvage treatment in progressive threshold retinopathy of prematurity. Retina 2008, 28, S13–S18. [Google Scholar] [CrossRef] [Green Version]
- Dalma-Weiszhausz, J.; Martinez-Castellanos, M.A.; Hernandez-Rojas, M.L.; Salazar-Teran, N.; Chan, R.V.P. Antiangiogenic therapy with intravitreal bevacizumab for retinopathy of prematurity. Retina 2008, 28, S19–S25. [Google Scholar] [CrossRef]
- Honda, S.; Hirabayashi, H.; Tsukahara, Y.; Negi, A. Acute contraction of the proliferative membrane after an intravitreal injection of bevacizumab for advanced retinopathy of prematurity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2008, 246, 1061–1063. [Google Scholar] [CrossRef] [PubMed]
- Mintz-Hittner, H.A.; Kennedy, K.A.; Chuang, A.Z. Efficacy of Intravitreal Bevacizumab for Stage 3+ Retinopathy of Prematurity. N. Engl. J. Med. 2011, 364, 603–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, C.K.; Hubbard, G.B.; Hutchinson, A.K.; Lambert, S.R. Outcomes after intravitreal bevacizumab versus laser photocoagulation for retinopathy of prematurity: A 5-year retrospective analysis. Ophthalmology 2015, 122, 1008–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lepore, D.; Quinn, G.E.; Molle, F.; Baldascino, A.; Orazi, L.; Sammartino, M.; Purcaro, V.; Giannantonio, C.; Papacci, P.; Romagnoli, C. Intravitreal Bevacizumab versus Laser Treatment in Type 1 Retinopathy of Prematurity. Ophthalmology 2014, 121, 2212–2219. [Google Scholar] [CrossRef] [PubMed]
- Stahl, A.; Lepore, D.; Fielder, A.; Fleck, B.; Reynolds, J.D.; Chiang, M.F.; Li, J.; Liew, M.; Maier, R.; Zhu, Q.; et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): An open-label randomised controlled trial. Lancet 2019, 394, 1551–1559. [Google Scholar] [CrossRef]
- Geloneck, M.M.; Chuang, A.Z.; Clark, W.L.; Hunt, M.G.; Norman, A.A.; Packwood, E.A.; Tawansy, K.A.; Mintz-Hittner, H.A. Refractive Outcomes Following Bevacizumab Monotherapy Compared with Conventional Laser Treatment. JAMA Ophthalmol. 2014, 132, 1327–1333. [Google Scholar] [CrossRef]
- Recchia, F.M.; Capone, A. Contemporary understanding and management of retinopathy of prematurity. Retina 2004, 24, 283–292. [Google Scholar] [CrossRef]
- Wallace, D.K.; Dean, T.W.; Hartnett, M.E.; Kong, L.; Smith, L.E.; Hubbard, G.B.; McGregor, M.L.; Jordan, C.O.; Mantagos, I.S.; Bell, E.F.; et al. A dosing study of bevacizumab for retinopathy of prematurity: Late recurrences and additional treatments. Ophthalmology 2018, 125, 1961–1966. [Google Scholar] [CrossRef]
- Morin, J.; Luu, T.M.; Superstein, R.; Ospina, L.H.; Lefebvre, F.; Simard, M.-N.; Shah, V.; Shah, P.S.; Mb, E.N.K. The Canadian Neonatal Network and the Canadian Neonatal Follow-Up Network Investigators Neurodevelopmental Outcomes Following Bevacizumab Injections for Retinopathy of Prematurity. Pediatrics 2016, 137, e20153218. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.Y.; Huang, Y.S.; Huang, C.Y.; Hsu, J.F.; Shih, C.P.; Hwang, Y.S.; Yao, T.C.; Lai, C.C.; Wu, W.C. Neurodevelopmental outcomes after intravitreal bevacizumab therapy for retinopathy of prematurity: A prospective case-control study. Ophthalmology 2019, 4, 1–11. [Google Scholar] [CrossRef]
- Rodriguez, S.H.; Peyton, C.; Lewis, K.; Andrews, B.; Greenwald, M.J.; Schreiber, M.D.; Msall, M.E.; Blair, M.P. Neurodevelopmental Outcomes Comparing Bevacizumab to Laser for Type 1 ROP. Ophthalmic Surg. Lasers Imaging Retin. 2019, 50, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Eichmann, A.; Thomas, J.-L. Molecular Parallels between Neural and Vascular Development. Cold Spring Harb. Perspect. Med. 2012, 3, a006551. [Google Scholar] [CrossRef] [Green Version]
- Rosenstein, J.M.; Krum, J.M.; Ruhrberg, C. VEGF in the nervous system. Organogenesis 2010, 6, 107–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Q.; Zhang, Q.; Fei, P.; Xu, Y.; Lyu, J.; Ji, X.; Peng, J.; Li, Y.; Zhao, P. Ranibizumab injection as primary treatment in patients with retinopathy of prematurity: Anatomic outcomes and influencing factors. Ophthalmology 2017, 124, 1156–1164. [Google Scholar] [CrossRef] [Green Version]
- Vanderveen, D.K.; Melia, M.; Yang, M.B.; Hutchinson, A.K.; Wilson, L.B.; Lambert, S.R. Anti-Vascular Endothelial Growth Factor Therapy for Primary Treatment of Type 1 Retinopathy of Prematurity. Ophthalmology 2017, 124, 619–633. [Google Scholar] [CrossRef] [Green Version]
- Papadopoulos, N.; Martin, J.; Ruan, Q.; Rafique, A.; Rosconi, M.P.; Shi, E.; Pyles, E.A.; Yancopoulos, G.D.; Stahl, N.; Wiegand, S.J. Binding and neutralization of vascular endothelial growth factor (VEGF) and related ligands by VEGF Trap, ranibizumab and bevacizumab. Angiogenesis 2012, 15, 171–185. [Google Scholar] [CrossRef] [Green Version]
- Carmeliet, P.; Moons, L.; Luttun, A.; Vincenti, V.; Compernolle, V.; De Mol, M.; Wu, Y.; Bono, F.; Devy, L.; Beck, H.; et al. Synergism between vascular endothelial growth factor and placental growth factor contributes to angiogenesis and plasma extravasation in pathological conditions. Nat. Med. 2001, 7, 575–583. [Google Scholar] [CrossRef]
- Takahashi, H.; Shibuya, M. The vascular endothelial growth factor (VEGF)/VEGF receptor system and its role under physiological and pathological conditions. Clin. Sci. 2005, 109, 227–241. [Google Scholar] [CrossRef] [Green Version]
- Sukgen, E.A.; Koçluk, Y. Comparison of clinical outcomes of intravitreal ranibizumab and aflibercept treatment for retinopathy of prematurity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 257, 49–55. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Lien, R.; Wang, N.-K.; Chao, A.-N.; Chen, K.-J.; Chen, T.-L.; Hwang, Y.-S.; Lai, C.-C.; Wu, W.-C. Changes in systemic vascular endothelial growth factor levels after intravitreal injection of aflibercept in infants with retinopathy of prematurity. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 479–487. [Google Scholar] [CrossRef]
- Owens, W.C.; Owens, E.U. Retrolental Fibroplasia in Premature Infants*. Am. J. Ophthalmol. 1949, 32, 1–21. [Google Scholar] [CrossRef]
- Hittner, H.M.; Godio, L.B.; Rudolph, A.J.; Adams, J.M.; Garcia-Prats, J.A.; Friedman, Z.; Kautz, J.A.; Monaco, W.A. Retrolental Fibroplasia: Efficacy of Vitamin E in a Double-Blind Clinical Study of Preterm Infants. N. Engl. J. Med. 1981, 305, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Phelps, D.L.; Rosenbaum, A.L.; Isenberg, S.J.; Leake, R.D.; Dorey, F.J. Tocopherol efficacy and safety for preventing retinopathy of prematurity: A randomized, controlled, double-masked trial. Pediatrics 1987, 79, 489–500. [Google Scholar] [PubMed]
- Brion, L.P.; Bell, E.F.; Raghuveer, T.S. Vitamin E supplementation for prevention of morbidity and mortality in preterm infants. Cochrane Database Syst. Rev. 2003, CD003665. [Google Scholar] [CrossRef] [PubMed]
- Raju, T.N.; Langenberg, P.; Bhutani, V.; Quinn, G.E. Vitamin E prophylaxis to reduce retinopathy of prematurity: A reappraisal of published trials. J. Pediatr. 1997, 131, 844–850. [Google Scholar] [CrossRef]
- Johnson, L.; Quinn, G.E.; Abbasi, S.; Otis, C.; Goldstein, D.; Sacks, L.; Porat, R.; Fong, E.; Delivoria-Papadopoulos, M.; Peckham, G.; et al. Effect of sustained pharmacologic vitamin E levels on incidence and severity of retinopathy of prematurity: A controlled clinical trial. J. Pediatr. 1989, 114, 827–838. [Google Scholar] [CrossRef]
- Finer, N.N.; Peters, K.L.; Hayek, Z.; Merkel, C.L. Vitamin E and necrotizing enterocolitis. Pediatrics 1984, 73, 387–393. [Google Scholar]
- Gu, X.; El-Remessy, A.B.; Brooks, S.E.; Al-Shabrawey, M.; Tsai, N.-T.; Caldwell, R.B. Hyperoxia induces retinal vascular endothelial cell apoptosis through formation of peroxynitrite. Am. J. Physiol. Physiol. 2003, 285, C546–C554. [Google Scholar] [CrossRef] [Green Version]
- Okuno, Y.; Nakamura-Ishizu, A.; Otsu, K.; Suda, T.; Kubota, Y. Pathological neoangiogenesis depends on oxidative stress regulation by ATM. Nat. Med. 2012, 18, 1208–1216. [Google Scholar] [CrossRef]
- Kojima, H.; Otani, A.; Oishi, A.; Makiyama, Y.; Nakagawa, S.; Yoshimura, N. Granulocyte colony-stimulating factor attenuates oxidative stress–induced apoptosis in vascular endothelial cells and exhibits functional and morphologic protective effect in oxygen-induced retinopathy. Blood 2011, 117, 1091–1100. [Google Scholar] [CrossRef]
- Kim, Y.-W.; Byzova, T.V. Oxidative stress in angiogenesis and vascular disease. Blood 2014, 123, 625–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nassi, P.; Ponziani, V.; Becatti, M.; Galvan, P.; Donzelli, G. Anti-oxidant enzymes and related elements in term and preterm newborns. Pediatr. Int. 2009, 51, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Buhimschi, I.A.; Buhimschi, C.S.; Pupkin, M.; Weiner, C.P. Beneficial impact of term labor: Nonenzymatic antioxidant reserve in the human fetus. Am. J. Obstet. Gynecol. 2003, 189, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Muller, D.P.R. Vitamin E therapy in retinopathy of prematurity. Eye 1992, 6, 221–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soghier, L.M.; Brion, L.P. Cysteine, cystine or N-acetylcysteine supplementation in parenterally fed neonates. Cochrane Database Syst. Rev. 2006, CD004869. [Google Scholar] [CrossRef] [PubMed]
- Manzoni, P.; Guardione, R.; Bonetti, P.; Priolo, C.; Maestri, A.; Mansoldo, C.; Mostert, M.; Anselmetti, G.; Sardei, D.; Bellettato, M.; et al. Lutein and Zeaxanthin Supplementation in Preterm Very Low-Birth-Weight Neonates in Neonatal Intensive Care Units: A Multicenter Randomized Controlled Trial. Am. J. Perinatol. 2012, 30, 025–032. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, J.D.; Hardy, R.J.; Kennedy, K.A.; Spencer, R.; Van Heuven, W.; Fielder, A.R. Lack of Efficacy of Light Reduction in Preventing Retinopathy of Prematurity. N. Engl. J. Med. 1998, 338, 1572–1576. [Google Scholar] [CrossRef]
- Qureshi, M.J.; Kumar, M. D-Penicillamine for preventing retinopathy of prematurity in preterm infants. Cochrane Database Syst. Rev. 2013, 2013, CD001073. [Google Scholar] [CrossRef]
- Tandon, M.; Dutta, S.; Dogra, M.R.; Brar, G.S. Oral D-penicillamine for the prevention of retinopathy of prematurity in very low birth weight infants: A randomized, placebo-controlled trial. Acta Paediatr. 2010, 99, 1324–1328. [Google Scholar] [CrossRef]
- Parad, R.B.; Allred, E.N.; Rosenfeld, W.N.; Davis, J.M. Reduction of Retinopathy of Prematurity in Extremely Low Gestational Age Newborns Treated with Recombinant Human Cu/Zn Superoxide Dismutase. Neonatology 2012, 102, 139–144. [Google Scholar] [CrossRef]
- Beharry, K.D.; Cai, C.L.; Siddiqui, F.; Chowdhury, S.; D’Agrosa, C.; Valencia, G.B.; Aranda, J.V. Comparative Effects of Coenzyme Q10 or n-3 Polyunsaturated Fatty Acid Supplementation on Retinal Angiogenesis in a Rat Model of Oxygen-Induced Retinopathy. Antioxidants 2018, 7, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akdogan, M.; Polat, O. Clinical Efficacy of Topical CoQ10 and Vitamin-E Eye-drop in Retinopathy of Prematurity. Med. Hypothesis. Discov. Innov. Ophthalmol. 2019, 8, 291–297. [Google Scholar] [PubMed]
- L’Abbe, M.R.; Friel, J.K. Superoxide Dismutase and Glutathione Peroxidase Content of Human Milk from Mothers of Premature and Full-Term Infants During the First 3 Months of Lactation. J. Pediatr. Gastroenterol. Nutr. 2000, 31, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Friel, J.K.; Martin, S.M.; Langdon, M.; Herzberg, G.R.; Buettner, G.R. Milk from Mothers of Both Premature and Full-Term Infants Provides Better Antioxidant Protection than Does Infant Formula. Pediatr. Res. 2002, 51, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Mactier, H.; Weaver, L.T. Vitamin A and preterm infants: What we know, what we don’t know, and what we need to know. Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, 103–108. [Google Scholar] [CrossRef]
- Shenai, J.P.; Chytil, F.; Stahlman, M.T. Liver Vitamin A Reserves of Very Low Birth Weight Neonates. Pediatr. Res. 1985, 19, 892–893. [Google Scholar] [CrossRef] [Green Version]
- Shenai, J.P.; Chytil, F.; Jhaveri, A.; Stahlman, M.T. Plasma vitamin A and retinol-binding protein in premature and term neonates. J. Pediatr. 1981, 99, 302–305. [Google Scholar] [CrossRef]
- Garofoli, F.; Barillà, D.; Angelini, M.; Mazzucchelli, I.; De Silvestri, A.; Guagliano, R.; Decembrino, L.; Tzialla, C. Oral vitamin A supplementation for ROP prevention in VLBW preterm infants. Ital. J. Pediatr. 2020, 46, 77. [Google Scholar] [CrossRef]
- Sun, H.; Cheng, R.; Wang, Z. Early vitamin a supplementation improves the outcome of retinopathy of prematurity in extremely preterm infants. Retina 2020, 40, 1176–1184. [Google Scholar] [CrossRef]
- Biesalski, H.K.; Nohr, D. Importance of vitamin-A for lung function and development. Mol. Asp. Med. 2003, 24, 431–440. [Google Scholar] [CrossRef]
- Tyson, J.E.; Wright, L.L.; Oh, W.; Kennedy, K.A.; Mele, L.; Ehrenkranz, R.A.; Stoll, B.J.; Lemons, J.A.; Stevenson, D.K.; Bauer, C.R.; et al. Vitamin A Supplementation for Extremely-Low-Birth-Weight Infants. N. Engl. J. Med. 1999, 340, 1962–1968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shenai, J.P.; Kennedy, K.A.; Chytil, F.; Stahlman, M.T. Clinical trial of vitamin A supplementation in infants susceptible to bronchopulmonary dysplasia. J. Pediatr. 1987, 111, 269–277. [Google Scholar] [CrossRef]
- Araki, S.; Kato, S.; Namba, F.; Ota, E. Vitamin A to prevent bronchopulmonary dysplasia in extremely low birth weight infants: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0207730. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.U.; Miras-Baldo, M.; Jerez-Calero, A.; Narbona-López, E. Effectiveness of Vitamin A in the Prevention of Complications of Prematurity. Pediatr. Neonatol. 2014, 55, 358–362. [Google Scholar] [CrossRef] [Green Version]
- Lingen, M.W.; Polverini, P.J.; Bouck, N.P. Inhibition of squamous cell carcinoma angiogenesis by direct interaction of retinoic acid with endothelial cells. Lab. Investig. 1996, 74, 476–483. [Google Scholar]
- Hoffmann, S.; Rockenstein, A.; Ramaswamy, A.; Celik, I.; Wunderlich, A.; Lingelbach, S.; Hofbauer, L.C.; Zielke, A. Retinoic acid inhibits angiogenesis and tumor growth of thyroid cancer cells. Mol. Cell. Endocrinol. 2007, 264, 74–81. [Google Scholar] [CrossRef]
- Ozkan, H.; Duman, N.; Kumral, A.; Kasap, B.; Ozer, E.A.; Lebe, B.; Yaman, A.; Berk, T.; Yilmaz, O.; Ozer, E. Inhibition of vascular endothelial growth factor-induced retinal neovascularization by retinoic acid in experimental retinopathy of prematurity. Physiol. Res. 2005, 55, 267–275. [Google Scholar]
- Pal, S.; Iruela-Arispe, M.; Harvey, V.; Zeng, H.; Nagy, J.A.; Dvorak, H.F.; Mukhopadhyay, D. Retinoic Acid Selectively Inhibits the Vascular Permeabilizing Effect of VPF/VEGF, an Early Step in the Angiogenic Cascade. Microvasc. Res. 2000, 60, 112–120. [Google Scholar] [CrossRef]
- Reese, A.B.; Blodi, F.C.; Locke, J.C.; Silverman, W.A.; Day, R.L. Results of use of corticotropin (ACTH) in treatment of retrolental fibroplasia. Arch. Ophthalmol. 1952, 47, 551–555. [Google Scholar] [CrossRef]
- Gilstrap, L.C. Effect of corticosteroids for fetal maturation on perinatal outcomes. NIH consensus development panel on the effect of corticosteroids for fetal maturation on perinatal outcomes. JAMA 1995, 273, 413–418. [Google Scholar] [CrossRef]
- Mesiano, S.; Jaffe, R.B. Developmental and Functional Biology of the Primate Fetal Adrenal Cortex. Endocr. Rev. 1997, 18, 378–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez, E.; Montman, R.; Watterberg, K. ACTH and cortisol response to critical illness in term and late preterm newborns. J. Perinatol. 2008, 28, 797–802. [Google Scholar] [CrossRef] [Green Version]
- Niwa, F.; Kawai, M.; Kanazawa, H.; Iwanaga, K.; Matsukura, T.; Shibata, M.; Hasegawa, T.; Heike, T. Limited response to CRH stimulation tests at 2 weeks of age in preterm infants born at less than 30 weeks of gestational age. Clin. Endocrinol. 2013, 78, 724–729. [Google Scholar] [CrossRef] [PubMed]
- Kawai, M. Late-onset circulatory collapse of prematurity. Pediatr. Int. 2017, 59, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Thompson, E. Gene regulation by the glucocorticoid receptor: Structure:function relationship. J. Steroid Biochem. Mol. Biol. 2005, 94, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Jonat, C.; Rahmsdorf, H.J.; Park, K.-K.; Cato, A.C.; Gebel, S.; Ponta, H.; Herrlich, P. Antitumor promotion and antiinflammation: Down-modulation of AP-1 (Fos/Jun) activity by glucocorticoid hormone. Cell 1990, 62, 1189–1204. [Google Scholar] [CrossRef]
- Tsurufuji, S.; Sugio, K.; Takemasa, F. The role of glucocorticoid receptor and gene expression in the anti-inflammatory action of dexamethasone. Nat. Cell Biol. 1979, 280, 408–410. [Google Scholar] [CrossRef]
- Hoekstra, M.; Ye, D.; Hildebrand, R.B.; Zhao, Y.; Lammers, B.; Stitzinger, M.; Kuiper, J.; Van Berkel, T.J.C.; Van Eck, M. Scavenger receptor class B type I-mediated uptake of serum cholesterol is essential for optimal adrenal glucocorticoid production. J. Lipid Res. 2009, 50, 1039–1046. [Google Scholar] [CrossRef] [Green Version]
- Console, V.; Gagliardi, L.; De Giorgi, A.; De Ponti, E. Retinopathy of prematurity and antenatal corticosteroids. The Italian ROP Study Group. Acta. Biomed. Ateneo. Parm. 1997, 68, 75–79. [Google Scholar]
- Higgins, R.D.; Mendelsohn, A.L.; Defeo, M.J.; Ucsel, R.; Hendricks-Munoz, K.D. Antenatal dexamethasone and decreased severity of retinopathy of prematurity. Arch. Ophthalmol. 1998, 116, 601–605. [Google Scholar] [CrossRef] [Green Version]
- Doyle, L.W.; Cheong, J.L.; Ehrenkranz, R.A.; Halliday, H.L. Late (>7 days) systemic postnatal corticosteroids for prevention of bronchopulmonary dysplasia in preterm infants. Cochrane Database Syst. Rev. 2017, 10, CD001145. [Google Scholar] [CrossRef]
- Doyle, L.W.; Cheong, J.L.; Ehrenkranz, R.A.; Halliday, H.L. Early (<8 days) systemic postnatal corticosteroids for prevention of bronchopulmonary dysplasia in preterm infants. Cochrane Database Syst. Rev. 2017, 10, CD001146. [Google Scholar] [CrossRef]
- Baud, O.; Maury, L.; LeBail, F.; Ramful, D.; El Moussawi, F.; Nicaise, C.; Zupan-Simunek, V.; Coursol, A.; Beuchée, A.; Bolot, P.; et al. Effect of early low-dose hydrocortisone on survival without bronchopulmonary dysplasia in extremely preterm infants (PREMILOC): A double-blind, placebo-controlled, multicentre, randomised trial. Lancet 2016, 387, 1827–1836. [Google Scholar] [CrossRef]
- Jelkmann, W. Erythropoietin: Structure, control of production, and function. Physiol. Rev. 1992, 72, 449–489. [Google Scholar] [CrossRef]
- Watanabe, D.; Suzuma, K.; Matsui, S.; Kurimoto, M.; Kiryu, J.; Kita, M.; Suzuma, I.; Ohashi, H.; Ojima, T.; Murakami, T.; et al. Erythropoietin as a Retinal Angiogenic Factor in Proliferative Diabetic Retinopathy. N. Engl. J. Med. 2005, 353, 782–792. [Google Scholar] [CrossRef]
- Semenza, G.L.; Wang, G.L. A nuclear factor induced by hypoxia via de novo protein synthesis binds to the human erythropoietin gene enhancer at a site required for transcriptional activation. Mol. Cell. Biol. 1992, 12, 5447–5454. [Google Scholar] [CrossRef] [Green Version]
- Rex, T.S.; Allocca, M.; Domenici, L.; Surace, E.M.; Maguire, A.M.; Lyubarsky, A.; Cellerino, A.; Bennett, J.; Auricchio, A. Systemic but not intraocular Epo Gene Transfer Protects the Retina from Light-and Genetic-Induced Degeneration. Mol. Ther. 2004, 10, 855–861. [Google Scholar] [CrossRef]
- Junk, A.K.; Mammis, A.; Savitz, S.I.; Singh, M.; Roth, S.; Malhotra, S.; Rosenbaum, P.S.; Cerami, A.; Brines, M.; Rosenbaum, D.M. Erythropoietin administration protects retinal neurons from acute ischemia-reperfusion injury. Proc. Natl. Acad. Sci. USA 2002, 99, 10659–10664. [Google Scholar] [CrossRef] [Green Version]
- Anagnostou, A.; Lee, E.S.; Kessimian, N.; Levinson, R.; Steiner, M. Erythropoietin has a mitogenic and positive chemotactic effect on endothelial cells. Proc. Natl. Acad. Sci. USA 1990, 87, 5978–5982. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Connor, K.M.; Aderman, C.M.; Smith, L. Erythropoietin deficiency decreases vascular stability in mice. J. Clin. Investig. 2008, 118, 526–533. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Connor, K.M.; Aderman, C.M.; Willett, K.L.; Aspegren, O.P.; Smith, L.E.H. Suppression of Retinal Neovascularization by Erythropoietin siRNA in a Mouse Model of Proliferative Retinopathy. Investig. Opthalmol. Vis. Sci. 2009, 50, 1329–1335. [Google Scholar] [CrossRef]
- Yang, Z.; Wang, H.; Jiang, Y.; Hartnett, M.E. VEGFA activates erythropoietin receptor and enhances VEGFR2-mediated pathological angiogenesis. Am. J. Pathol. 2014, 184, 1230–1239. [Google Scholar] [CrossRef] [Green Version]
- Suk, K.K.; Dunbar, J.A.; Liu, A.; Daher, N.S.; Leng, C.K.; Leng, J.K.; Lim, P.; Weller, S.; Fayard, E. Human recombinant erythropoietin and the incidence of retinopathy of prematurity: A multiple regression model. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2008, 12, 233–238. [Google Scholar] [CrossRef]
- Brown, M.S.; Barón, A.E.; France, E.K.; Hamman, R.F. Association Between Higher Cumulative Doses of Recombinant Erythropoietin and Risk for Retinopathy of Prematurity. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2006, 10, 143–149. [Google Scholar] [CrossRef]
- Romagnoli, C.; Zecca, E.; Gallini, F.; Girlando, P.; Zuppa, A.A. Do recombinant human erythropoietin and iron supplementation increase the risk of retinopathy of prematurity? Eur. J. Nucl. Med. Mol. Imaging 2000, 159, 627–628. [Google Scholar] [CrossRef]
- Ohls, R.K.; Christensen, R.D.; Kamath-Rayne, B.D.; Rosenberg, A.; Wiedmeier, S.E.; Roohi, M.; Lacy, C.B.; Lambert, D.K.; Burnett, J.J.; Pruckler, B.; et al. A Randomized, Masked, Placebo-Controlled Study of Darbepoetin Alfa in Preterm Infants. Pediatrics 2013, 132, e119–e127. [Google Scholar] [CrossRef] [Green Version]
- Juul, S.E.; Comstock, B.A.; Wadhawan, R.; Mayock, D.E.; Courtney, S.E.; Robinson, T.; Ahmad, K.A.; Bendel-Stenzel, E.; Baserga, M.; LaGamma, E.F.; et al. A Randomized Trial of Erythropoietin for Neuroprotection in Preterm Infants. N. Engl. J. Med. 2020, 382, 233–243. [Google Scholar] [CrossRef]
- Ohlsson, A.; Aher, S.M. Early erythropoietin for preventing red blood cell transfusion in preterm and/or low birth weight infants. Cochrane Database Syst. Rev. 2014, 26, CD004863. [Google Scholar] [CrossRef]
- Aher, S.M.; Ohlsson, A. Late erythropoietin for preventing red blood cell transfusion in preterm and/or low birth weight infants. Cochrane Database Syst. Rev. 2014, 23, CD004868. [Google Scholar] [CrossRef]
- Smith, L.E.H.; Kopchick, J.J.; Chen, W.; Knapp, J.; Kinose, F.; Daley, D.; Foley, E.; Smith, R.G.; Schaeffer, J.M. Essential Role of Growth Hormone in Ischemia-Induced Retinal Neovascularization. Science 1997, 276, 1706–1709. [Google Scholar] [CrossRef]
- Smith, L.E.H.; Shen, W.; Perruzzi, C.; Soker, S.; Kinose, F.; Xu, X.; Robinson, G.; Driver, S.; Bischoff, J.; Zhang, B.; et al. Regulation of vascular endothelial growth factor-dependent retinal neovascularization by insulin-like growth factor-1 receptor. Nat. Med. 1999, 5, 1390–1395. [Google Scholar] [CrossRef]
- Hellstrom, A.; Perruzzi, C.; Ju, M.; Engström, E.; Hård, A.-L.; Liu, J.-L.; Albertsson-Wikland, K.; Carlsson, B.; Niklasson, A.; Sjödell, L.; et al. Low IGF-I suppresses VEGF-survival signaling in retinal endothelial cells: Direct correlation with clinical retinopathy of prematurity. Proc. Natl. Acad. Sci. USA 2001, 98, 5804–5808. [Google Scholar] [CrossRef] [Green Version]
- Löfqvist, C.; Chen, J.; Connor, K.M.; Smith, A.C.H.; Aderman, C.M.; Liu, N.; Pintar, J.E.; Ludwig, T.; Hellström, A.; Smith, L.E.H. IGFBP3 suppresses retinopathy through suppression of oxygen-induced vessel loss and promotion of vascular regrowth. Proc. Natl. Acad. Sci. USA 2007, 104, 10589–10594. [Google Scholar] [CrossRef] [Green Version]
- Hansen-Pupp, I.; Hellström-Westas, L.; Cilio, C.M.; Andersson, S.; Fellman, V.; Ley, D. Inflammation at birth and the insulin-like growth factor system in very preterm infants. Acta Paediatr. Int. J. Paediatr. 2007, 96, 830–836. [Google Scholar] [CrossRef]
- Ley, D.; Hansen-Pupp, I.; Niklasson, A.; Domellöf, M.; Friberg, L.E.; Borg, J.; Löfqvist, C.; Hellgren, G.; Smith, L.E.H.; Hård, A.-L.; et al. Longitudinal infusion of a complex of insulin-like growth factor-I and IGF-binding protein-3 in five preterm infants: Pharmacokinetics and short-term safety. Pediatr. Res. 2013, 73, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Sugioka, K.; Saito, A.; Kusaka, S.; Kuniyoshi, K.; Shimomura, Y. Identification of vitreous proteins in retinopathy of prematurity. Biochem. Biophys. Res. Commun. 2017, 488, 483–488. [Google Scholar] [CrossRef]
- Wang, Z.; Dabrosin, C.; Yin, X.; Fuster, M.M.; Arreola, A.; Rathmell, W.K.; Generali, D.; Nagaraju, G.P.; El-Rayes, B.; Ribatti, D.; et al. Broad targeting of angiogenesis for cancer prevention and therapy. Semin. Cancer Biol. 2015, 35, S224–S243. [Google Scholar] [CrossRef]
- Nakao, S.; Kuwano, T.; Tsutsumi-Miyahara, C.; Ueda, S.; Kimura, Y.N.; Hamano, S.; Sonoda, K.; Saijo, Y.; Nukiwa, T.; Strieter, R.M.; et al. Infiltration of COX-2-expressing macrophages is a prerequisite for IL-1 beta-induced neovascularization and tumor growth. J. Clin. Investig. 2005, 115, 2979–2991. [Google Scholar] [CrossRef]
- Simmons, D.L.; Botting, R.M.; Hla, T. Cyclooxygenase Isozymes: The Biology of Prostaglandin Synthesis and Inhibition. Pharmacol. Rev. 2004, 56, 387–437. [Google Scholar] [CrossRef] [Green Version]
- Hyde, C.; Missailidis, S. Inhibition of arachidonic acid metabolism and its implication on cell proliferation and tumour-angiogenesis. Int. Immunopharmacol. 2009, 9, 701–715. [Google Scholar] [CrossRef] [Green Version]
- Nandgaonkar, B.N.; Rotschild, T.; Yu, K.; Higgins, R.D. Indomethacin improves oxygen-induced retinopathy in the mouse. Pediatr. Res. 1999, 46, 184–188. [Google Scholar] [CrossRef] [Green Version]
- Sennlaub, F.; Valamanesh, F.; Vazquez-Tello, A.; El-Asrar, A.; Checchin, D.; Brault, S.; Gobeil, F.; Beauchamp, M.; Mwaikambo, B.; Courtois, Y.; et al. Cyclooxygenase-2 in Human and Experimental Ischemic Proliferative Retinopathy. Circulation 2003, 108, 198–204. [Google Scholar] [CrossRef] [Green Version]
- Yanni, S.E.; Barnett, J.M.; Clark, M.L.; Penn, J.S. The Role of PGE2Receptor EP4in Pathologic Ocular Angiogenesis. Investig. Opthalmol. Vis. Sci. 2009, 50, 5479–5486. [Google Scholar] [CrossRef] [Green Version]
- Gersony, W.M.; Peckham, G.J.; Ellison, R.C.; Miettinen, O.S.; Nadas, A.S. Effects of indomethacin in premature infants with patent ductus arteriosus: Results of a national collaborative study. J. Pediatr. 1983, 102, 895–906. [Google Scholar] [CrossRef]
- Bandstra, E.S.; Montalvo, B.M.; Goldberg, R.N.; Pacheco, I.; Ferrer, P.L.; Flynn, J.; Gregorios, J.B.; Bancalari, E. Prophylactic indomethacin for prevention of intraventricular hemorrhage in premature infants. Pediatrics 1988, 82, 533–542. [Google Scholar]
- Bolling, J.; Feman, S.S.; Mellander, M.; Cotton, R. The Influence of Indomethacin on Retinopathy of Prematurity. Am. J. Ophthalmol. 1983, 96, 254–255. [Google Scholar] [CrossRef]
- Schmidt, B.; Davis, P.; Moddemann, D.; Ohlsson, A.; Roberts, R.S.; Saigal, S.; Solimano, A.; Vincer, M.; Wright, L.L. Long-Term Effects of Indomethacin Prophylaxis in Extremely-Low-Birth-Weight Infants. N. Engl. J. Med. 2001, 344, 1966–1972. [Google Scholar] [CrossRef] [Green Version]
- Jegatheesan, P.; Ianus, V.; Buchh, B.; Yoon, G.; Chorne, N.; Ewig, A.; Lin, E.; Fields, S.; Moon-Grady, A.; Tacy, T.; et al. Increased Indomethacin Dosing for Persistent Patent Ductus Arteriosus in Preterm Infants: A Multicenter, Randomized, Controlled Trial. J. Pediatr. 2008, 153, 183–189. [Google Scholar] [CrossRef]
- Aranda, J.V.; Clyman, R.; Cox, B.; Van Overmeire, B.; Wozniak, P.; Sosenko, I.; Carlo, W.A.; Ward, R.M.; Shalwitz, R.; Baggs, G.; et al. A Randomized, Double-Blind, Placebo-Controlled Trial on Intravenous Ibuprofen L-Lysine for the Early Closure of Nonsymptomatic Patent Ductus Arteriosus within 72 Hours of Birth in Extremely Low-Birth-Weight Infants. Am. J. Perinatol. 2008, 26, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Clyman, R.I.; Liebowitz, M.; Kaempf, J.; Erdeve, O.; Bulbul, A.; Håkansson, S.; Lindqvist, J.; Farooqi, A.; Katheria, A.; Sauberan, J.; et al. PDA-TOLERATE Trial: An Exploratory Randomized Controlled Trial of Treatment of Moderate-to-Large Patent Ductus Arteriosus at 1 Week of Age. J. Pediatr. 2019, 205, 41–48. [Google Scholar] [CrossRef]
- Dani, C.; Bertini, G.; Reali, M.F.; Murru, P.; Fabris, C.; Vangi, V.; Rubaltelli, F.F. Prophylaxis of patent ductus arteriosus with ibuprofen in preterm infants. Acta Paediatr. 2000, 89, 1369–1374. [Google Scholar] [CrossRef] [PubMed]
- Avila-Vazquez, M.; Maffrand, R.; Sosa, M.; Franco, M.; De Alvarez, B.V.; Cafferata, M.L.; Bergel, E. Treatment of Retinopathy of Prematurity with topical ketorolac tromethamine: A preliminary study. BMC Pediatr. 2004, 4, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannantonio, C.; Papacci, P.; Purcaro, V.; Cota, F.; Tesfagabir, M.G.; Molle, F.; Lepore, D.; Baldascino, A.; Romagnoli, C. Effectiveness of Ketorolac Tromethamine in Prevention of Severe Retinopathy of Prematurity. J. Pediatr. Ophthalmol. Strabismus 2010, 48, 247–251. [Google Scholar] [CrossRef] [PubMed]
- SanGiovanni, J.P.; Chew, E.Y. The role of omega-3 long-chain polyunsaturated fatty acids in health and disease of the retina. Prog. Retin. Eye Res. 2005, 24, 87–138. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Polyunsaturated fatty acids and inflammation. Prostaglandins Leukot. Essent. Fat. Acids 2006, 75, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Connor, K.M.; SanGiovanni, J.P.; Lofqvist, C.; Aderman, C.M.; Chen, J.; Higuchi, A.; Hong, S.; Pravda, E.A.; Majchrzak, S.; Carper, D.; et al. Increased dietary intake of ω-3-polyunsaturated fatty acids reduces pathological retinal angiogenesis. Nat. Med. 2007, 13, 868–873. [Google Scholar] [CrossRef] [Green Version]
- Sapieha, P.; Stahl, A.; Chen, J.; Seaward, M.R.; Willett, K.L.; Krah, N.M.; Dennison, R.J.; Connor, K.M.; Aderman, C.M.; Liclican, E.; et al. 5-Lipoxygenase metabolite 4-HDHA is a mediator of the antiangiogenic effect of ω-3 polyunsaturated fatty acids. Sci. Transl. Med. 2011, 3, 69ra12. [Google Scholar] [CrossRef] [Green Version]
- Beken, S.; Dilli, D.; Fettah, N.D.; Kabataş, E.U.; Zenciroǧlu, A.; Okumuş, N. The influence of fish-oil lipid emulsions on retinopathy of prematurity in very low birth weight infants: A randomized controlled trial. Early Hum. Dev. 2014, 90, 27–31. [Google Scholar] [CrossRef]
- Khalesi, N.; Bordbar, A.; Khosravi, N.; Kabirian, M.; Karimi, A. The Efficacy of Omega-3 Supplement on Prevention of Retinopathy of Prematurity in Premature Infants: A Randomized Double-blinded Controlled trial. Curr. Pharm. Des. 2018, 24, 1845–1848. [Google Scholar] [CrossRef]
- Pawlik, D.; Lauterbach, R.; Walczak, M.; Hurkała, J.; Sherman, M.P. Fish-oil fat emulsion supplementation reduces the risk of retinopathy in very low birth weight infants: A prospective, randomized study. J. Parenter. Enter. Nutr. 2014, 38, 711–716. [Google Scholar] [CrossRef]
- Najm, S.; Löfqvist, C.; Hellgren, G.; Engström, E.; Lundgren, P.; Hård, A.-L.; Lapillonne, A.; Sävman, K.; Nilsson, A.K.; Andersson, M.X.; et al. Effects of a lipid emulsion containing fish oil on polyunsaturated fatty acid profiles, growth and morbidities in extremely premature infants: A randomized controlled trial. Clin. Nutr. ESPEN 2017, 20, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Löfqvist, C.A.; Najm, S.; Hellgren, G.; Engström, E.; Sävman, K.; Nilsson, A.K.; Andersson, M.X.; Hård, A.-L.; Smith, L.E.H.; Hellström, A. Association of retinopathy of prematurity with low levels of arachidonic acid. JAMA Ophthalmol. 2018, 136, 271–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricci, B.; Calogero, G.; Caprilli, A.; Quaranta-Leoni, F.M. Reduced severity of oxygen-induced retinopathy in the newborn rat after topical administration of timolol maleate—A preliminary study. Doc. Ophthalmol. 1991, 77, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Ricci, B.; Minicucci, G.; Manfredi, A.; Santo, A. Oxygen-induced retinopathy in the newborn rat: Effects of hyperbarism and topical administration of timolol maleate. Graefe’s Arch. Clin. Exp. Ophthalmol. 1995, 233, 226–230. [Google Scholar] [CrossRef]
- Lutgendorf, S.K.; Cole, S.; Costanzo, E.; Bradley, S.; Coffin, J.; Jabbari, S.; Rainwater, K.; Ritchie, J.M.; Yang, M.; Sood, A.K. Stress-related mediators stimulate vascular endothelial growth factor secretion by two ovarian cancer cell lines. Clin. Cancer Res. 2003, 9, 4514–4521. [Google Scholar]
- Léauté-Labrèze, C.; De La Roque, E.D.; Hubiche, T.; Boralevi, F.; Thambo, J.-B.; Taieb, A. Propranolol for Severe Hemangiomas of Infancy. N. Engl. J. Med. 2008, 358, 2649–2651. [Google Scholar] [CrossRef]
- Weil, J.; Benndorf, R.; Fredersdorf, S.; Griese, D.P.; Eschenhagen, T. Norepinephrine Upregulates Vascular Endothelial Growth Factor in Rat Cardiac Myocytes by a Paracrine Mechanism. Angiogenesis 2003, 6, 303–309. [Google Scholar] [CrossRef]
- Yang, E.V.; Sood, A.K.; Chen, M.; Li, Y.; Eubank, T.D.; Marsh, C.B.; Jewell, S.; Flavahan, N.A.; Morrison, C.; Yeh, P.-E.; et al. Norepinephrine Up-regulates the Expression of Vascular Endothelial Growth Factor, Matrix Metalloproteinase (MMP)-2, and MMP-9 in Nasopharyngeal Carcinoma Tumor Cells. Cancer Res. 2006, 66, 10357–10364. [Google Scholar] [CrossRef] [Green Version]
- Martini, D.; Monte, M.D.; Ristori, C.; Cupisti, E.; Mei, S.; Fiorini, P.; Filippi, L.; Bagnoli, P. Antiangiogenic effects of β2-adrenergic receptor blockade in a mouse model of oxygen-induced retinopathy. J. Neurochem. 2011, 119, 1317–1329. [Google Scholar] [CrossRef]
- Ristori, C.; Filippi, L.; Monte, M.D.; Martini, D.; Cammalleri, M.; Fortunato, P.; La Marca, G.; Fiorini, P.; Bagnoli, P. Role of the Adrenergic System in a Mouse Model of Oxygen-Induced Retinopathy: Antiangiogenic Effects of β-Adrenoreceptor Blockade. Investig. Opthalmol. Vis. Sci. 2011, 52, 155–170. [Google Scholar] [CrossRef] [Green Version]
- Ozturk, M.A.; Korkmaz, L. The efficacy of propranolol in very preterm infants at the risk of retinopathy of prematurity: Which newborn and when? Int. Ophthalmol. 2018, 39, 1921–1930. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, L.; Baştuğ, O.; Ozdemir, A.; Korkut, S.; Karaca, C.; Akin, M.A.; Gunes, T.; Kurtoglu, S.; Ozturk, M.A. The Efficacy of Propranolol in Retinopathy of Prematurity and its Correlation with the Platelet Mass Index. Curr. Eye Res. 2016, 42, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Makhoul, I.R.; Peleg, O.; Miller, B.; Bar-Oz, B.; Kochavi, O.; Mechoulam, H.; Mezer, E.; Ulanovsky, I.; Smolkin, T.; Yahalom, C.; et al. Oral propranolol versus placebo for retinopathy of prematurity: A pilot, randomised, double-blind prospective study. Arch. Dis. Child. 2013, 98, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Bancalari, A.; Schade, R.; Muñoz, T.; Lazcano, C.; Parada, R.; Peña, R. Oral propranolol in early stages of retinopathy of prematurity. J. Périnat. Med. 2016, 44, 499–503. [Google Scholar] [CrossRef]
- Filippi, L.; Cavallaro, G.; Bagnoli, P.; Monte, M.D.; Fiorini, P.; Donzelli, G.; Tinelli, F.; Araimo, G.; Cristofori, G.; La Marca, G.; et al. Oral Propranolol for Retinopathy of Prematurity: Risks, Safety Concerns, and Perspectives. J. Pediatr. 2013, 163, 1570–1577.e6. [Google Scholar] [CrossRef]
- Filippi, L.; Cavallaro, G.; Bagnoli, P.; Monte, M.D.; Fiorini, P.; Berti, E.; Padrini, L.; Donzelli, G.; Araimo, G.; Cristofori, G.; et al. Propranolol 0.1% eye micro-drops in newborns with retinopathy of prematurity: A pilot clinical trial. Pediatr. Res. 2017, 81, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Filippi, L.; Cavallaro, G.; Berti, E.; Padrini, L.; Araimo, G.; Regiroli, G.; Raffaeli, G.; Bozzetti, V.; Tagliabue, P.; Tomasini, B.; et al. Propranolol 0.2% Eye Micro-Drops for Retinopathy of Prematurity: A Prospective Phase IIB Study. Front. Pediatr. 2019, 7, 180. [Google Scholar] [CrossRef] [Green Version]
- Matsui, T.; Amano, M.; Yamamoto, T.; Chihara, K.; Nakafuku, M.; Ito, M.; Nakano, T.; Okawa, K.; Iwamatsu, A.; Kaibuchi, K. Rho-associated kinase, a novel serine/threonine kinase, as a putative target for small GTP binding protein Rho. EMBO J. 1996, 15, 2208–2216. [Google Scholar] [CrossRef]
- Kishi, T.; Hirooka, Y.; Masumoto, A.; Ito, K.; Kimura, Y.; Inokuchi, K.; Tagawa, T.; Shimokawa, H.; Takeshita, A.; Sunagawa, K. Rho-Kinase Inhibitor Improves Increased Vascular Resistance and Impaired Vasodilation of the Forearm in Patients with Heart Failure. Circulation 2005, 111, 2741–2747. [Google Scholar] [CrossRef] [Green Version]
- Mueller, B.K.; Mack, H.; Teusch, N. Rho kinase, a promising drug target for neurological disorders. Nat. Rev. Drug Discov. 2005, 4, 387–398. [Google Scholar] [CrossRef]
- Kinoshita, S.; Koizumi, N.; Ueno, M.; Okumura, N.; Imai, K.; Tanaka, H.; Yamamoto, Y.; Nakamura, T.; Inatomi, T.; Bush, J.; et al. Injection of Cultured Cells with a ROCK Inhibitor for Bullous Keratopathy. N. Engl. J. Med. 2018, 378, 995–1003. [Google Scholar] [CrossRef] [PubMed]
- Rothschild, P.-R.; Salah, S.; Berdugo, M.; Gélizé, E.; Delaunay, K.; Naud, M.-C.; Klein, C.; Moulin, A.; Savoldelli, M.; Bergin, C.; et al. ROCK-1 mediates diabetes-induced retinal pigment epithelial and endothelial cell blebbing: Contribution to diabetic retinopathy. Sci. Rep. 2017, 7, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollanders, K.; Van Hove, I.; Sergeys, J.; Van Bergen, T.; Lefevere, E.; Kindt, N.; Castermans, K.; Vandewalle, E.; Van Pelt, J.; Moons, L.; et al. AMA0428, A Potent Rock Inhibitor, Attenuates Early and Late Experimental Diabetic Retinopathy. Curr. Eye Res. 2016, 42, 260–272. [Google Scholar] [CrossRef] [PubMed]
- Kita, T.; Hata, Y.; Arita, R.; Kawahara, S.; Miura, M.; Nakao, S.; Mochizuki, Y.; Enaida, H.; Goto, Y.; Shimokawa, H.; et al. Role of TGF-beta in proliferative vitreoretinal diseases and ROCK as a therapeutic target. Proc. Natl. Acad. Sci. USA 2008, 105, 17504–17509. [Google Scholar] [CrossRef] [Green Version]
- Arima, M.; Nakao, S.; Yamaguchi, M.; Feng, H.; Fujii, Y.; Shibata, K.; Wada, I.; Kaizu, Y.; Ahmadieh, H.; Ishibashi, T.; et al. Claudin-5 Redistribution Induced by Inflammation Leads to Anti-VEGF–Resistant Diabetic Macular Edema. Diabetes 2020, 69, 981–999. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Nakao, S.; Arita, R.; Kaizu, Y.; Arima, M.; Zhou, Y.; Kita, T.; Yoshida, S.; Kimura, K.; Isobe, T.; et al. Vascular Normalization by ROCK Inhibitor: Therapeutic Potential of Ripasudil (K-115) Eye Drop in Retinal Angiogenesis and Hypoxia. Investig. Opthalmol. Vis. Sci. 2016, 57, 2264. [Google Scholar] [CrossRef] [Green Version]
- Zandi, S.; Nakao, S.; Chun, K.-H.; Fiorina, P.; Sun, D.; Arita, R.; Zhao, M.; Kim, E.; Schueller, O.; Campbell, S.; et al. ROCK-Isoform-Specific Polarization of Macrophages Associated with Age-Related Macular Degeneration. Cell Rep. 2015, 10, 1173–1186. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Yoshida, S.; Nakao, S.; Yoshimura, T.; Kobayashi, Y.; Nakama, T.; Kubo, Y.; Miyawaki, K.; Yamaguchi, M.; Ishikawa, K.; et al. M2 Macrophages Enhance Pathological Neovascularization in the Mouse Model of Oxygen-Induced Retinopathy. Investig. Opthalmol. Vis. Sci. 2015, 56, 4767–4777. [Google Scholar] [CrossRef] [Green Version]
- Nakao, S.; Arima, M.; Ishikawa, K.; Kohno, R.; Kawahara, S.; Miyazaki, M.; Yoshida, S.; Enaida, H.; Hafezi-Moghadam, A.; Kono, T.; et al. Intravitreal Anti-VEGF Therapy Blocks Inflammatory Cell Infiltration and Re-Entry into the Circulation in Retinal Angiogenesis. Investig. Opthalmol. Vis. Sci. 2012, 53, 4323–4328. [Google Scholar] [CrossRef]
- Ishikawa, K.; Yoshida, S.; Kadota, K.; Nakamura, T.; Niiro, H.; Arakawa, S.; Yoshida, A.; Akashi, K.; Ishibashi, T. Gene Expression Profile of Hyperoxic and Hypoxic Retinas in a Mouse Model of Oxygen-Induced Retinopathy. Investig. Opthalmol. Vis. Sci. 2010, 51, 4307–4319. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, K.; Yoshida, S.; Nakao, S.; Sassa, Y.; Asato, R.; Kohno, R.; Arima, M.; Kita, T.; Yoshida, A.; Ohuchida, K.; et al. Bone marrow-derived monocyte lineage cells recruited by MIP-1β promote physiological revascularization in mouse model of oxygen-induced retinopathy. Lab. Investig. 2011, 92, 91–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soucek, L.; Lawlor, E.R.; Soto, D.; Shchors, K.; Swigart, L.B.; Evan, G.I. Mast cells are required for angiogenesis and macroscopic expansion of Myc-induced pancreatic islet tumors. Nat. Med. 2007, 13, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Muramatsu, M.; Katada, J.; Hayashi, I.; Majima, M. Chymase as a Proangiogenic Factor. J. Biol. Chem. 2000, 275, 5545–5552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuda, K.; Okamoto, N.; Kondo, M.; Arkwright, P.D.; Karasawa, K.; Ishizaka, S.; Yokota, S.; Matsuda, A.; Jung, K.; Oida, K.; et al. Mast cell hyperactivity underpins the development of oxygen-induced retinopathy. J. Clin. Investig. 2017, 127, 3987–4000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, N.; Lee, Y.F.; Ge, R. Novel endogenous angiogenesis inhibitors and their therapeutic potential. Acta Pharmacol. Sin. 2015, 36, 1177–1190. [Google Scholar] [CrossRef] [Green Version]
- Stahl, A.; Joyal, J.-S.; Chen, J.; Sapieha, P.; Juan, A.M.; Hatton, C.J.; Pei, D.T.; Hurst, C.G.; Seaward, M.R.; Krah, N.M.; et al. SOCS3 is an endogenous inhibitor of pathologic angiogenesis. Blood 2012, 120, 2925–2929. [Google Scholar] [CrossRef] [Green Version]
- Starr, R.; Willson, T.A.; Viney, E.M.; Murray, L.J.L.; Rayner, J.R.; Jenkins, B.J.; Gonda, T.J.; Alexander, W.S.; Metcalf, D.; Nicola, N.A.; et al. A family of cytokine-inducible inhibitors of signalling. Nat. Cell Biol. 1997, 387, 917–921. [Google Scholar] [CrossRef]
- Sun, Y.; Ju, M.; Lin, Z.; Fredrick, T.W.; Evans, L.P.; Tian, K.T.; Saba, N.J.; Morss, P.C.; Pu, W.T.; Chen, J.; et al. SOCS3 in retinal neurons and glial cells suppresses VEGF signaling to prevent pathological neovascular growth. Sci. Signal. 2015, 8, ra94. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Liu, C.-H.; SanGiovanni, J.P.; Evans, L.P.; Tian, K.T.; Zhang, B.; Stahl, A.; Pu, W.T.; Kamenecka, T.M.; Solt, L.A.; et al. Nuclear receptor RORα regulates pathologic retinal angiogenesis by modulating SOCS3-dependent inflammation. Proc. Natl. Acad. Sci. USA 2015, 112, 10401–10406. [Google Scholar] [CrossRef] [Green Version]
- Isenberg, S.J.; Apt, L.; Mccarty, J.; Cooper, L.L.; Lim, L.; Del Signore, M. Development of tearing in preterm and term neonates. Arch. Ophthalmol. 1998, 116, 773–776. [Google Scholar] [CrossRef] [Green Version]
- Kusari, A.; Ba, A.M.H.; Virgen, C.A.; Matiz, C.; Rasmussen, M.; Friedlander, S.F.; Eichenfield, D.Z. Evidence-based skin care in preterm infants. Pediatr. Dermatol. 2018, 36, 16–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salaets, T.; Turner, M.A.; Short, M.; Ward, R.M.; Hokuto, I.; Ariagno, R.L.; Klein, A.; Beauman, S.; Wade, K.; Thomson, M.; et al. Development of a neonatal adverse event severity scale through a Delphi consensus approach. Arch. Dis. Child. 2019, 104, 1167–1173. [Google Scholar] [CrossRef] [PubMed]



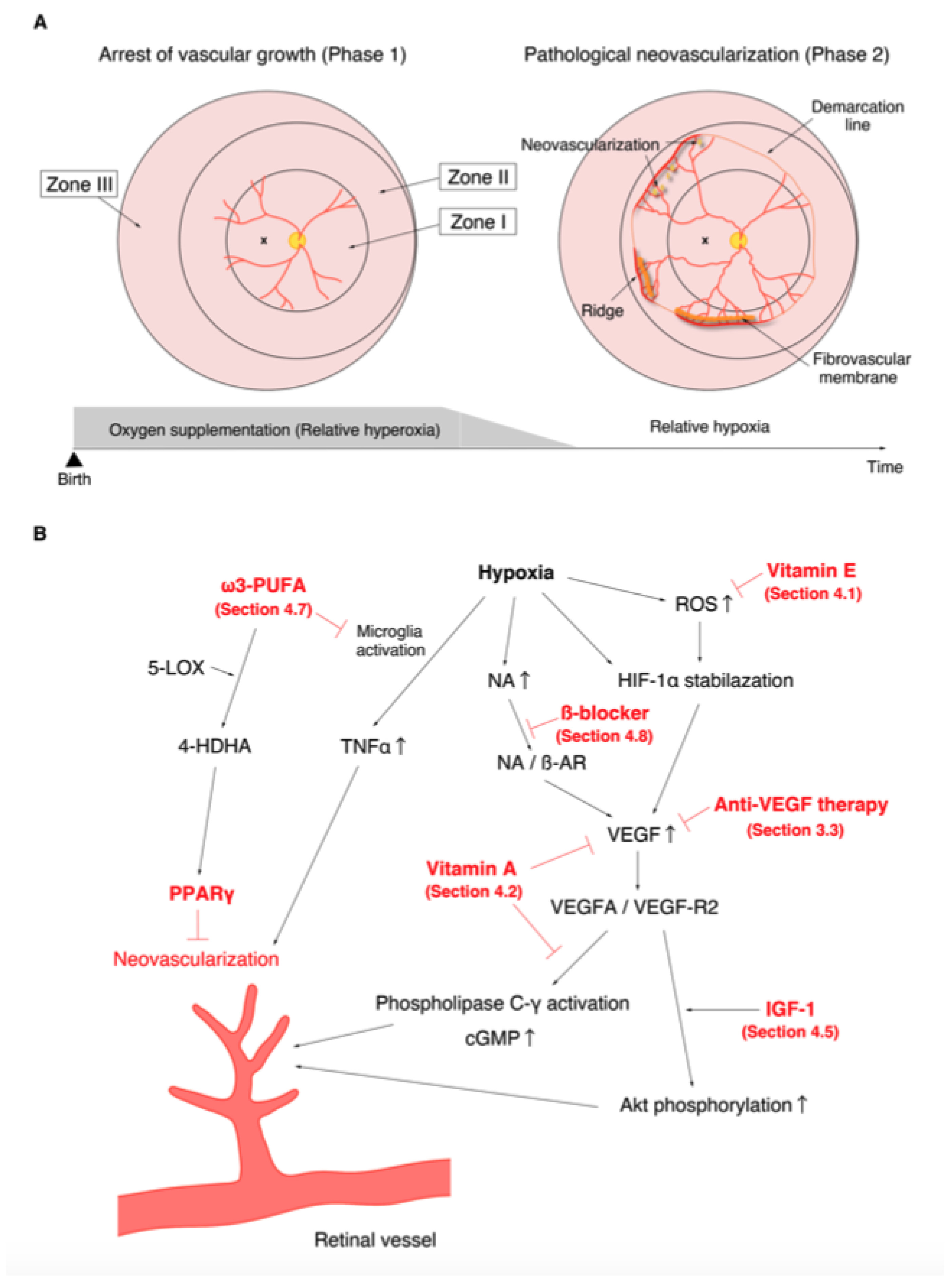{kind=link}
{kind=link}
| Location (see Figure 1) | Zone I | Circle centered on the optic disc with the radius of twice the distance from the optic disc to the fovea. |
| Zone II | Circle centered on the optic disc with the distance to the nasal ora serrata as the radius, excluding Zone I | |
| Zone III | Residual retina anterior to Zone II. | |
| Severity | Stage 1 | Demarcation line |
| Stage 2 | Ridge | |
| Stage 3 | Ridge with extra retinal fibrovascular proliferation | |
| Stage 4 | Subtotal retinal detachment | |
| Stage 5 | Total retinal detachment | |
| Plus disease | Venous dilation and arterial tortuosity of the posterior pole vessels |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arima, M.; Fujii, Y.; Sonoda, K.-H. Translational Research in Retinopathy of Prematurity: From Bedside to Bench and Back Again. J. Clin. Med. 2021, 10, 331. https://doi.org/10.3390/jcm10020331
Arima M, Fujii Y, Sonoda K-H. Translational Research in Retinopathy of Prematurity: From Bedside to Bench and Back Again. Journal of Clinical Medicine. 2021; 10(2):331. https://doi.org/10.3390/jcm10020331
Chicago/Turabian StyleArima, Mitsuru, Yuya Fujii, and Koh-Hei Sonoda. 2021. "Translational Research in Retinopathy of Prematurity: From Bedside to Bench and Back Again" Journal of Clinical Medicine 10, no. 2: 331. https://doi.org/10.3390/jcm10020331
APA StyleArima, M., Fujii, Y., & Sonoda, K. -H. (2021). Translational Research in Retinopathy of Prematurity: From Bedside to Bench and Back Again. Journal of Clinical Medicine, 10(2), 331. https://doi.org/10.3390/jcm10020331