
The Reevaluation of Thrombin Time Using a Clot Waveform Analysis

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
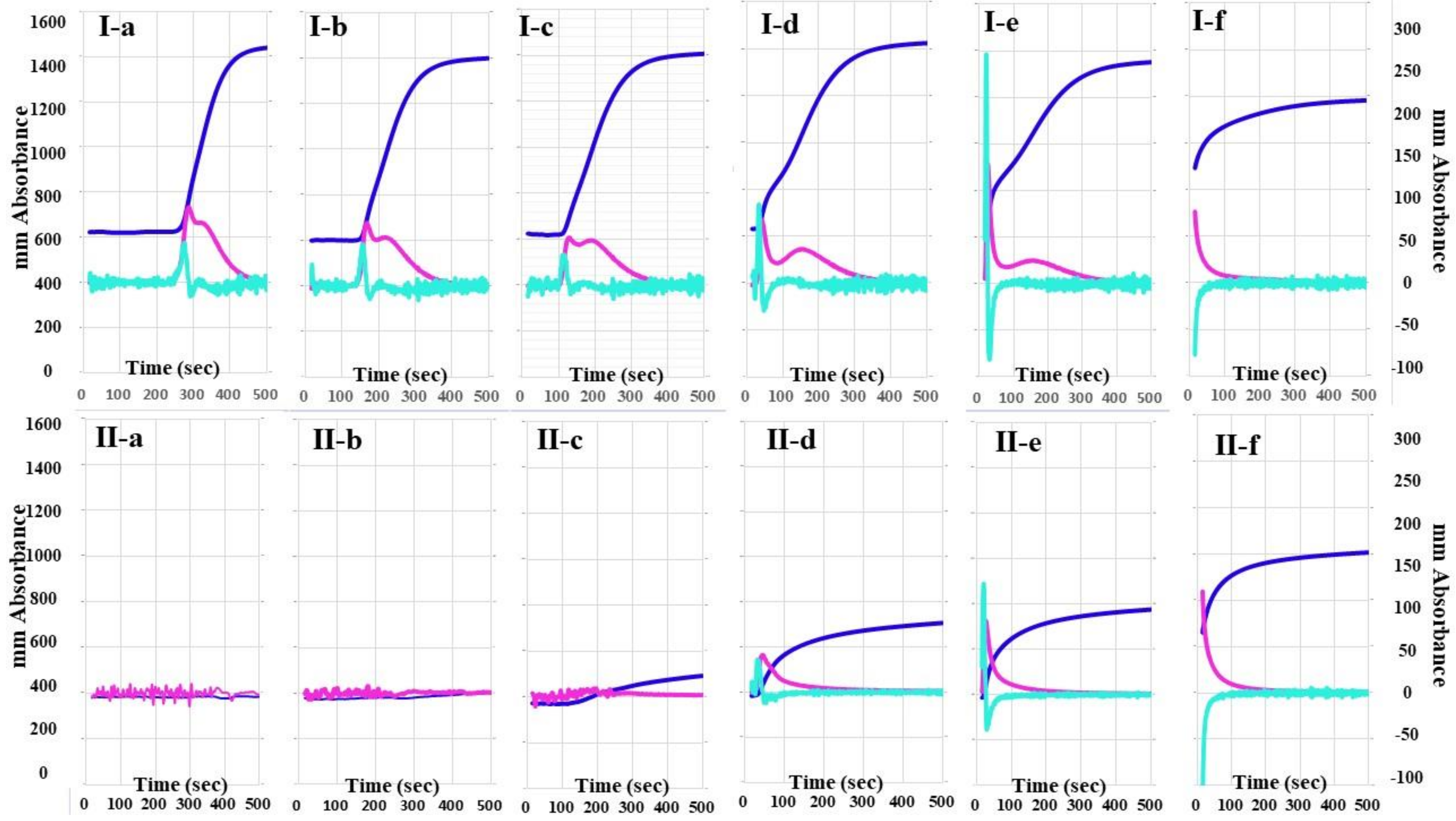
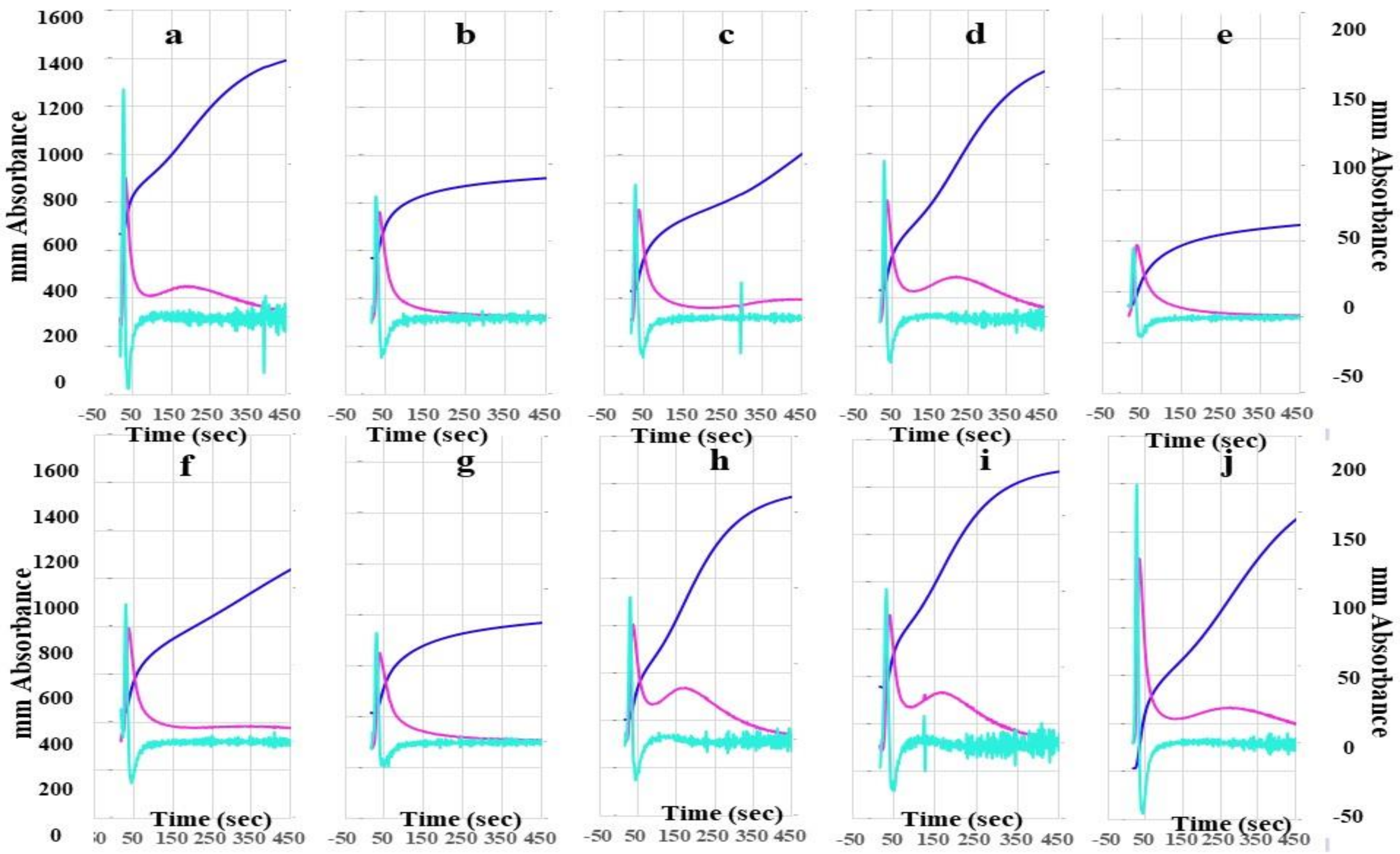
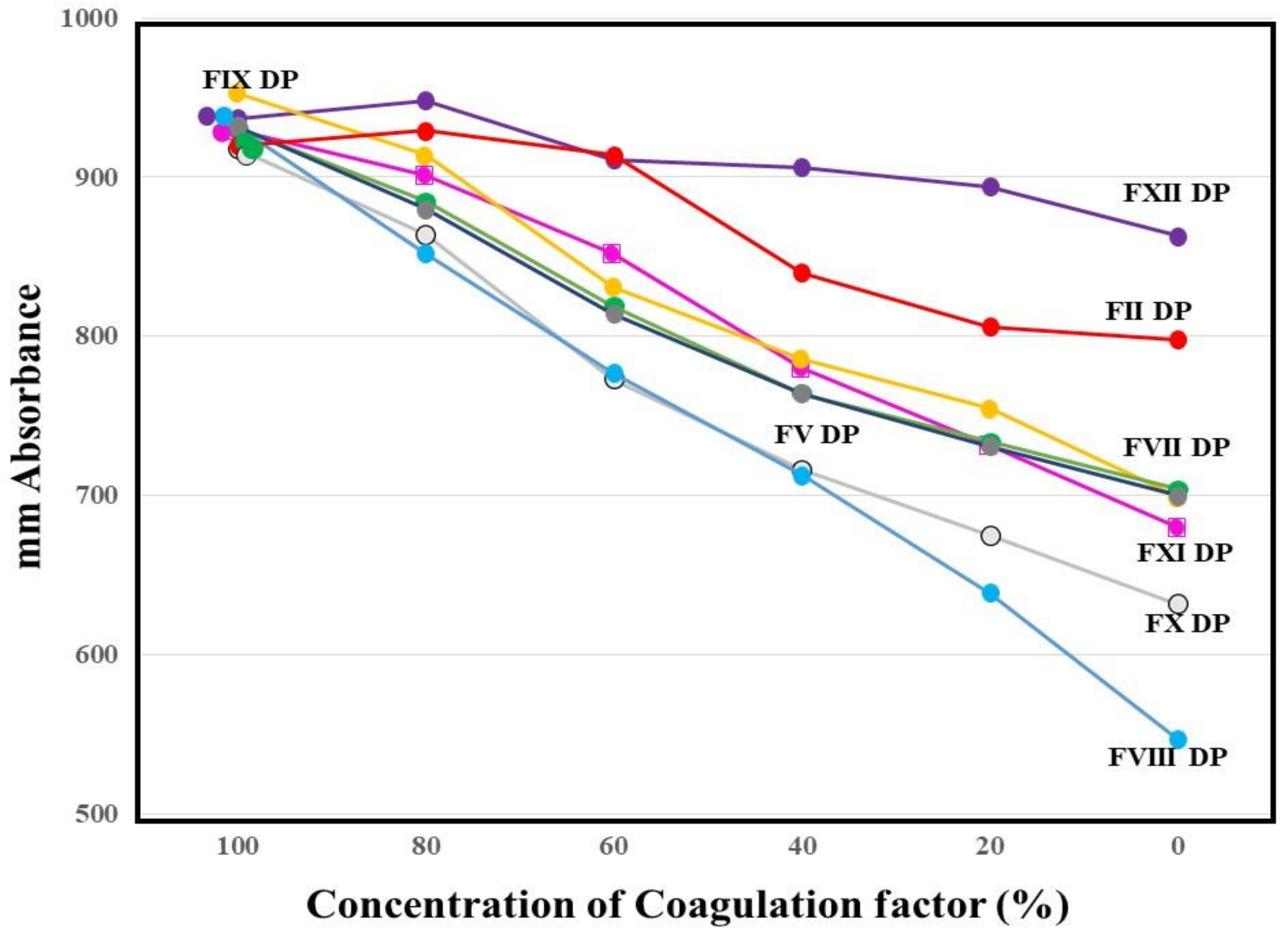
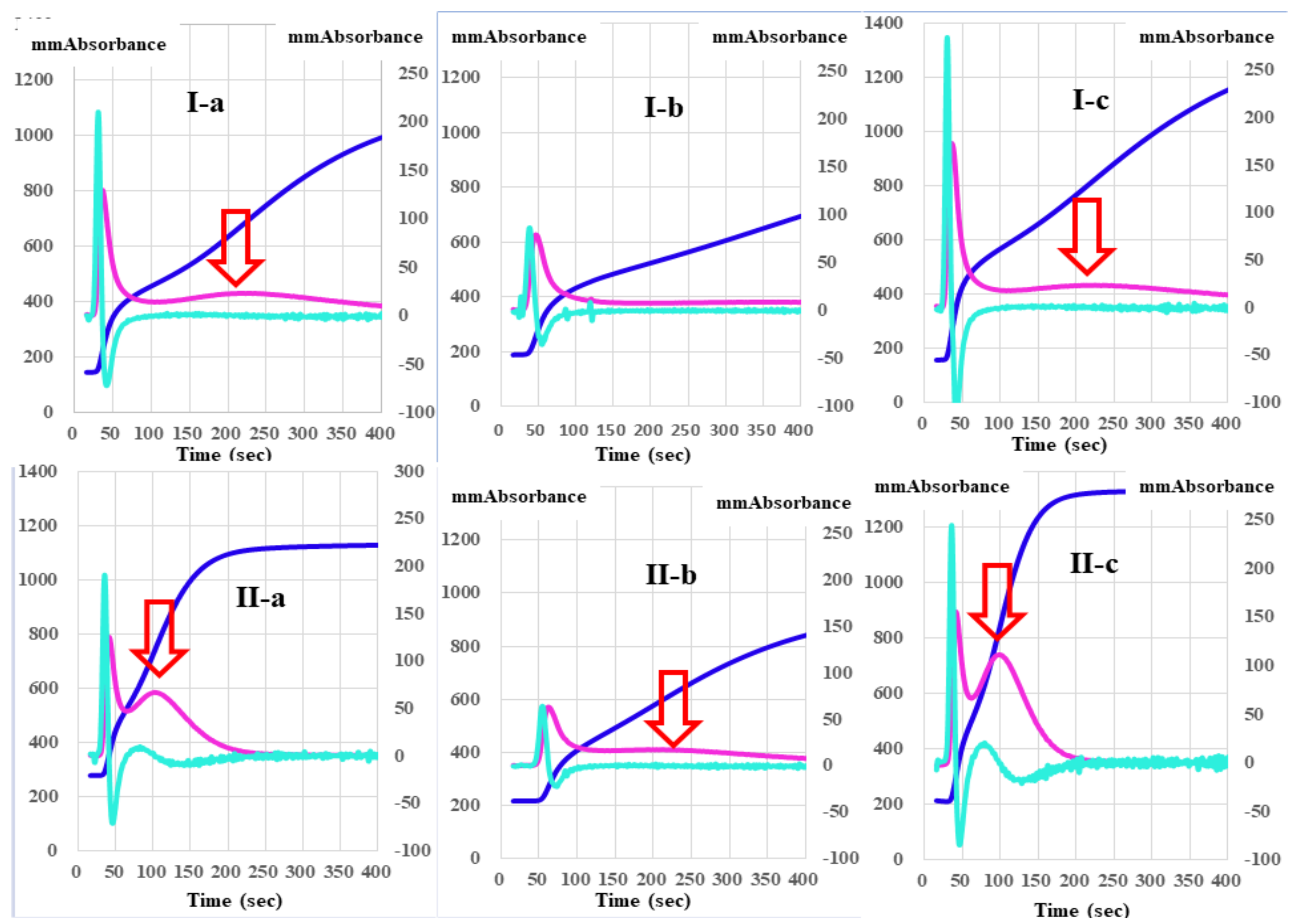
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Winter, W.E.; Greene, D.N.; Beal, S.G.; Isom, J.A.; Manning, H.; Wilkerson, G.; Harris, N. Clotting factors: Clinical biochemistry and their roles as plasma enzymes. Int. Rev. Cytol. 2020, 94, 31–84. [Google Scholar] [CrossRef]
- Berntorp, E.; Salvagno, G.L. Standardization and clinical utility of thrombin-generation assays. Semin. Thromb. Hemost. 2008, 34, 670–682. [Google Scholar] [CrossRef] [PubMed]
- Salvagno, G.L.; Berntorp, E. thrombin generation testing for monitoring hemophilia treatment: A clinical perspective. Semin. Thromb. Hemost. 2010, 36, 780–790. [Google Scholar] [CrossRef]
- Li, S.; Wang, M.; Li, X.; Xu, Q.; Liu, S.; Luo, S.; Chen, Y. Analysis of an Inherited dysfibrinogenemia pedigree associated with a heterozygous mutation in the FGA Gene. Hämostaseologie 2020, 40, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Marchi, R.; Neerman-Arbez, M.; Gay, V.; Mourey, G.; Fiore, M.; Mouton, C.; Gautier, P.; De Moerloose, P.; Casini, A. Comparison of different activators of coagulation by turbidity analysis of hereditary dysfibrinogenemia and controls. Blood Coagul. Fibrinolysis 2021, 32, 108–114. [Google Scholar] [CrossRef]
- Haupt, L.; Vieira, M.; Brits, H.; de Beer, J.; Erasmus, E.; Esterhuyse, W.; Fraser, R.; Joubert, G. An audit of disseminated intravascular coagulation screen requests at an academic hospital laboratory in central South Africa. Int. J. Lab. Hematol. 2021, 43, 1174–1180. [Google Scholar] [CrossRef]
- Martinez, J.; Macdonald, K.A.; Palascak, J.E. The role of sialic acid in the dysfibrinogenemia associated with liver disease: Distribution of sialic acid on the constituent chains. Blood 1983, 61, 1196–1202. [Google Scholar] [CrossRef] [Green Version]
- Winter, W.E.; Flax, S.D.; Harris, N.S. Coagulation Testing in the Core Laboratory. Lab. Med. 2017, 48, 295–313. [Google Scholar] [CrossRef]
- Van Cott, E.M.; Roberts, A.J.; Dager, W.E. Laboratory monitoring of parenteral direct thrombin inhibitors. Semin. Thromb. Hemost. 2017, 43, 270–276. [Google Scholar]
- Konstantinidi, A.; Sokou, R.; Parastatidou, S.; Lampropoulou, K.; Katsaras, G.; Boutsikou, T.; Gounaris, A.K.; Tsantes, A.E.; Iacovidou, N. Clinical Application of Thromboelastography/Thromboelastometry (TEG/TEM) in the Neonatal Population: A Narrative Review. Semin. Thromb. Hemost. 2019, 45, 449–457. [Google Scholar] [CrossRef]
- Tripodi, A. Thrombin Generation Assay and Its Application in the Clinical Laboratory. Clin. Chem. 2016, 62, 699–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bendetowicz, A.V.; Kai, H.; Knebel, R.; Caplain, H.; Hemker, H.C.; Lindhout, T.; Béguin, S. The effect of subcutaneous injection of unfractionated and low molecular weight heparin on thrombin generation in platelet rich plasma—A study in human volunteers. Thromb. Haemost. 1994, 72, 705–712. [Google Scholar] [CrossRef]
- Maeda, K.; Wada, H.; Shinkai, T.; Tanemura, A.; Matsumoto, T.; Mizuno, S. Evaluation of hemostatic abnormalities in patients who underwent major hepatobiliary pancreatic surgery using activated partial thromboplastin time-clot waveform analysis. Thromb. Res. 2021, 201, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Wada, H.; Matsumoto, T.; Ohishi, K.; Shiraki, K.; Shimaoka, M. Update on the clot waveform analysis. Clin. Appl. Thromb. 2020, 26. [Google Scholar] [CrossRef] [PubMed]
- Wada, H.; Shiraki, K.; Matsumoto, T.; Ohishi, K.; Shimpo, H.; Shimaoka, M. Effects of platelet and phospholipids on clot formation activated by a small amount of tissue factor. Thromb. Res. 2020, 193, 146–153. [Google Scholar] [CrossRef]
- Matsumoto, T.; Fukuda, K.; Kubota, Y.; Tanaka, I.; Nishiya, K.; Giles, A.R.; Yoshioka, A.; Shima, M. The Utility of activated Partial Thromboplastin Time (aPTT) Clot Waveform Analysis in the Investigation of Hemophilia A Patients with very Low Levels of Factor VIII Activity (FVIII:C). Thromb. Haemost. 2002, 87, 436–441. [Google Scholar] [CrossRef]
- Matsumoto, T.; Nogami, K.; Shima, M. A combined approach using global coagulation assays quickly differentiates coagulation disorders with prolonged aPTT and low levels of FVIII activity. Int. J. Hematol. 2016, 105, 174–183. [Google Scholar] [CrossRef]
- Tokutake, T.; Baba, H.; Shimada, Y.; Takeda, W.; Sato, K.; Hiroshima, Y.; Kirihara, T.; Shimizu, I.; Nakazawa, H.; Kobayashi, H.; et al. Exogenous magnesium chloride reduces the activated partial thromboplastin times of lupus anticoagulant-positive patients. PLoS ONE. 2016, 11, e0157835. [Google Scholar] [CrossRef]
- Matsumoto, T.; Wada, H.; Fujimoto, N.; Toyoda, J.; Abe, Y.; Ohishi, K.; Yamashita, Y.; Ikejiri, M.; Hasegawa, K.; Suzuki, K.; et al. An evaluation of the activated partial thromboplastin time waveform. Clin. Appl. Thromb. 2017, 24, 764–770. [Google Scholar] [CrossRef]
- Hasegawa, M.; Wada, H.; Tone, S.; Yamaguchi, T.; Wakabayashi, H.; Ikejiri, M.; Watanabe, M.; Fujimoto, N.; Matsumoto, T.; Ohishi, K.; et al. Monitoring of hemostatic abnormalities in major orthopedic surgery patients treated with edoxaban by APTT waveform. Int. J. Lab. Hematol. 2017, 40, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Wada, H.; Matsumoto, T.; Ikejiri, M.; Ohishi, K.; Yamashita, Y.; Imai, H.; Iba, T. Katayama N: Usefulness of the APTT waveform for the diagnosis of DIC and prediction of the outcome or bleeding risk. Thromb. J. 2019, 17, 12. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, Y.; Nogami, K. The C-terminal acidic region in the A1 domain of factor VIII facilitates thrombin-catalyzed activation and cleavage at Arg 372. J. Thromb. Haemost. 2021, 19, 677–688. [Google Scholar] [CrossRef]
- Suzuki, A.; Suzuki, N.; Kanematsu, T.; Shinohara, S.; Arai, N.; Kikuchi, R.; Matsushita, T. Clot waveform analysis in Clauss fibrinogen assay contributes to classification of fibrinogen disorders. Thromb. Res. 2019, 174, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Tone, S.; Wada, H.; Naito, Y.; Matsumoto, T.; Yamashita, Y.; Shimaoka, M.; Sudo, A. The evaluation of hemostatic abnormalities using a CWA-Small amount tissue factor induced fix activation assay in major orthopedic surgery patients. Clin. Appl. Thromb. 2021, 27. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Wada, H.; Toyoda, H.; Hirayama, M.; Yamashita, Y.; Katayama, N. Modified clot waveform analysis to measure plasma coagulation potential in the presence of the anti-factor IXa/factor X bispecific antibody emicizumab: Comment. J. Thromb. Haemost. 2018, 16, 1665–1666. [Google Scholar] [CrossRef] [Green Version]
- Keshava, S.; Pendurthi, U.R.; Esmon, C.T.; Rao, L.V.M. Vijaya Mohan Rao: Therapeutic doses of recombinant factor VIIa in hemophilia generates thrombin in platelet-dependent and -independent mechanisms. J. Thromb. Haemost. 2020, 18, 1911–1921. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2nd DPT (seconds) | 2nd DPH (mm ABS) | 1st DPT-1 (seconds) | 1st DPH-1 (mm ABS) | 1st DPT-2 (seconds) | 1st DPH-2 (mm ABS) | FFCT (seconds) | FFCH (mm ABS) | |
|---|---|---|---|---|---|---|---|---|
| PPP (n = 18) | 30.1 *** (28.9–30.9) | 164 (137–219) | 36.3 ** (35.0–37.5) | 113 * (96.5–132) | 234 *** (220–278) | 18.1 *** (15.4–22.9) | 194 *** (185–204) | 615 ** (560–664) |
| PRP (n = 18) | 37.4 *** (33.1–43.3) | 124 (110–180) | 45.4 ** (39.2–50.2) | 101 * (82.5–120) | 134 *** (112–137) | 45.3 *** (40.0–62.1) | 127 *** (115–139) | 730 ** (700–843) |
| 2nd DPT (seconds) | 2nd DPH (mm ABS) | 1st DPT-1 (seconds) | 1st DPH-1 (mm ABS) | 1st DPT-2 (seconds) | 1st DPH-2 (mm ABS) | FFCT (seconds) | FFCH (mm ABS) | |
|---|---|---|---|---|---|---|---|---|
| Healthy volunteers (n = 18) | 37.4 (33.1–43.3) | 124 (110–180) | 45.4 (39.2–50.2) | 101 (82.5–120) | 134 (112–137) | 45.3 (40.0–62.1) | 127 (115–139) | 730 (700–842) |
| Thrombocytopenia (n = 12) | 35.6 (32.3–38.7) | 174 (98.6–219) | 43.9 (39.9–44.7) | 115 (73.6–140) | 188 *** (146–216) | 29.2 *** (26.6–34.4) | 153 * (131–198) | 763 (682–865) |
| Malignant diseases (n = 16) | 33.7 (30.1–38.5) | 268 ** (185–339) | 39.3 (34.7–43.0) | 154 *** (126–176) | 111 (104–129) | 82.2 *** (76.4–108) | 102 * (98.2–118) | 953 (813–1067) |
| 2nd DPT (seconds) | 2nd DPH (mm ABS) | 1st DPT-1 (seconds) | 1st DPH-1 (mm ABS) | 1st DPT-2 (seconds) | 1st DPH-2 (mm ABS) | FFCT (seconds) | FFCH (mm ABS) | |
|---|---|---|---|---|---|---|---|---|
| Healthy volunteers (n = 18) | 30.5 (28.9–30.9) | 164 (137–219) | 36.3 (35.0–37.5) | 113 (96.5–132) | 234 (220–278) | 18.1 (15.4–22.9) | 194 (185–204) | 615 (560–664) |
| Thrombocytopenia (n = 12) | 34.9 * (31.0–39.2) | 143 (78.5–255) | 43.2 * (37.6–47.5) | 106 * (70.2–157) | Not detectable | Not detectable | 202 (152–209) | 550 (492–637) |
| Malignant diseases (n = 16) | 30.3 (28.6–46.1) | 321 * (137–420) | 35.0 (33.7–52.7) | 166 *** (103–207) | 228 (173–273) | 28.5 ** (21.6–43.3) | 187 (157–236) | 738 ** (656–874) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wada, H.; Ichikawa, Y.; Ezaki, M.; Matsumoto, T.; Yamashita, Y.; Shiraki, K.; Shimaoka, M.; Shimpo, H. The Reevaluation of Thrombin Time Using a Clot Waveform Analysis. J. Clin. Med. 2021, 10, 4840. https://doi.org/10.3390/jcm10214840
Wada H, Ichikawa Y, Ezaki M, Matsumoto T, Yamashita Y, Shiraki K, Shimaoka M, Shimpo H. The Reevaluation of Thrombin Time Using a Clot Waveform Analysis. Journal of Clinical Medicine. 2021; 10(21):4840. https://doi.org/10.3390/jcm10214840
Chicago/Turabian StyleWada, Hideo, Yuhuko Ichikawa, Minoru Ezaki, Takeshi Matsumoto, Yoshiki Yamashita, Katsuya Shiraki, Motomu Shimaoka, and Hideto Shimpo. 2021. "The Reevaluation of Thrombin Time Using a Clot Waveform Analysis" Journal of Clinical Medicine 10, no. 21: 4840. https://doi.org/10.3390/jcm10214840
APA StyleWada, H., Ichikawa, Y., Ezaki, M., Matsumoto, T., Yamashita, Y., Shiraki, K., Shimaoka, M., & Shimpo, H. (2021). The Reevaluation of Thrombin Time Using a Clot Waveform Analysis. Journal of Clinical Medicine, 10(21), 4840. https://doi.org/10.3390/jcm10214840