
Thyroid Disfunction in Critically Ill COVID-19 Patients. Relationship with In-Hospital Mortality


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Outcomes
2.3. Measurement of Thyroid Hormones
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maiden, M.J.; Torpy, D.J. Thyroid Hormones in Critical Illness. Crit. Care Clin. 2019, 35, 375–388. [Google Scholar] [CrossRef]
- Van den Berghe, G. Non-thyroidal illness in the ICU: A syndrome with different faces. Thyroid 2014, 24, 1456–1465. [Google Scholar] [CrossRef]
- Peeters, R.P.; van der Geyten, S.; Wouters, P.J.; Darras, V.M.; van Toor, H.; Kaptein, E.; Visser, T.J.; Van den Berghe, G. Tissue thyroid hormone levels in critical illness. J. Clin. Endocrinol. Metab. 2005, 90, 6498–6507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrer, R. COVID-19 Pandemic: The greatest challenge in the history of critical care. Med. Intensiva 2020, 44, 323–324. [Google Scholar] [CrossRef]
- Pal, R.; Banerjee, M. COVID-19 and the endocrine system: Exploring the unexplored. J. Endocrinol. Investig. 2020, 43, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Li, M.Y.; Li, L.; Zhang, Y.; Wang, X.S. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect. Dis. Poverty 2020, 9, 45. [Google Scholar] [CrossRef]
- Zou, R.; Wu, C.; Zhang, S.; Wang, G.; Zhang, Q.; Yu, B.; Wu, Y.; Dong, H.; Wu, G.; Wu, S.; et al. Euthyroid Sick Syndrome in Patients With COVID-19. Front. Endocrinol. (Lausanne) 2020, 11, 566439. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Zhou, W.; Xu, W. Thyroid Function Analysis in 50 Patients with COVID-19: A Retrospective Study. Thyroid 2021, 31, 8–11. [Google Scholar] [CrossRef]
- Gao, W.; Guo, W.; Guo, Y.; Shi, M.; Dong, G.; Wang, G.; Ge, Q.; Zhu, J.; Zhou, X. Thyroid hormone concentrations in severely or critically ill patients with COVID-19. J. Endocrinol. Investig. 2021, 44, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Lui, D.T.W.; Lee, C.H.; Chow, W.S.; Lee, A.C.H.; Tam, A.R.; Fong, C.H.Y.; Law, C.Y.; Leung, E.K.H.; To, K.K.W.; Tan, K.C.B.; et al. Role of non-thyroidal illness syndrome in predicting adverse outcomes in COVID-19 patients predominantly of mild-to-moderate severity. Clin. Endocrinol. (Oxf.) 2021, 95, 469–477. [Google Scholar] [CrossRef]
- Lui, D.T.W.; Lee, C.H.; Chow, W.S.; Lee, A.C.H.; Tam, A.R.; Fong, C.H.Y.; Law, C.Y.; Leung, E.K.H.; To, K.K.W.; Tan, K.C.B.; et al. Thyroid Dysfunction in Relation to Immune Profile, Disease Status, and Outcome in 191 Patients with COVID-19. J. Clin. Endocrinol. Metab. 2021, 106, e926–e935. [Google Scholar] [CrossRef]
- Bello, G.; Pennisi, M.A.; Montini, L.; Silva, S.; Maviglia, R.; Cavallaro, F.; Bianchi, A.; De Marinis, L.; Antonelli, M. Nonthyroidal illness syndrome and prolonged mechanical ventilation in patients admitted to the ICU. Chest 2009, 135, 1448–1454. [Google Scholar] [CrossRef] [Green Version]
- Chinga-Alayo, E.; Villena, J.; Evans, A.T.; Zimic, M. Thyroid hormone levels improve the prediction of mortality among patients admitted to the intensive care unit. Intensive Care Med. 2005, 31, 1356–1361. [Google Scholar] [CrossRef] [PubMed]
- Meyer, S.; Schuetz, P.; Wieland, M.; Nusbaumer, C.; Mueller, B.; Christ-Crain, M. Low triiodothyronine syndrome: A prognostic marker for outcome in sepsis? Endocrine 2011, 39, 167–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peeters, R.P.; Wouters, P.J.; van Toor, H.; Kaptein, E.; Visser, T.J.; Van den Berghe, G. Serum 3,3′,5′-triiodothyronine (rT3) and 3,5,3′-triiodothyronine/rT3 are prognostic markers in critically ill patients and are associated with postmortem tissue deiodinase activities. J. Clin. Endocrinol. Metab. 2005, 90, 4559–4565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoo, B.; Tan, T.; Clarke, S.A.; Mills, E.G.; Patel, B.; Modi, M.; Phylactou, M.; Eng, P.C.; Thurston, L.; Alexander, E.C.; et al. Thyroid Function Before, During, and After COVID-19. J. Clin. Endocrinol. Metab. 2021, 106, e803–e811. [Google Scholar] [CrossRef] [PubMed]
- Campi, I.; Bulgarelli, I.; Dubini, A.; Perego, G.B.; Tortorici, E.; Torlasco, C.; Torresani, E.; Rocco, L.; Persani, L.; Fugazzola, L.; et al. The spectrum of thyroid function tests during hospitalization for SARS COV-2 infection. Eur. J. Endocrinol. 2021, 184, 699–709. [Google Scholar] [CrossRef]
- Bacci, V.; Schussler, G.C.; Kaplan, T.B. The relationship between serum triiodothyronine and thyrotropin during systemic illness. J. Clin. Endocrinol. Metab. 1982, 54, 1229–1235. [Google Scholar] [CrossRef] [PubMed]
- Hamblin, P.S.; Dyer, S.A.; Mohr, V.S.; Le Grand, B.A.; Lim, C.F.; Tuxen, D.V.; Topliss, D.J.; Stockigt, J.R. Relationship between thyrotropin and thyroxine changes during recovery from severe hypothyroxinemia of critical illness. J. Clin. Endocrinol. Metab. 1986, 62, 717–722. [Google Scholar] [CrossRef]
- Pantos, C.; Kostopanagiotou, G.; Armaganidis, A.; Trikas, A.; Tseti, I.; Mourouzis, I. Triiodothyronine for the treatment of critically ill patients with COVID-19 infection: A structured summary of a study protocol for a randomised controlled trial. Trials 2020, 21, 573. [Google Scholar] [CrossRef] [PubMed]
- Koulouri, O.; Moran, C.; Halsall, D.; Chatterjee, K.; Gurnell, M. Pitfalls in the measurement and interpretation of thyroid function tests. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 745–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chachques, J.C.; Mazzini, L.; Mitrecic, D.; Zavan, B.; Rogante, M.; Latremouille, C.; Rustichelli, F. Cardiovascular, hematological and neurosensory impact of COVID-19 and variants. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3350–3364. [Google Scholar] [CrossRef] [PubMed]



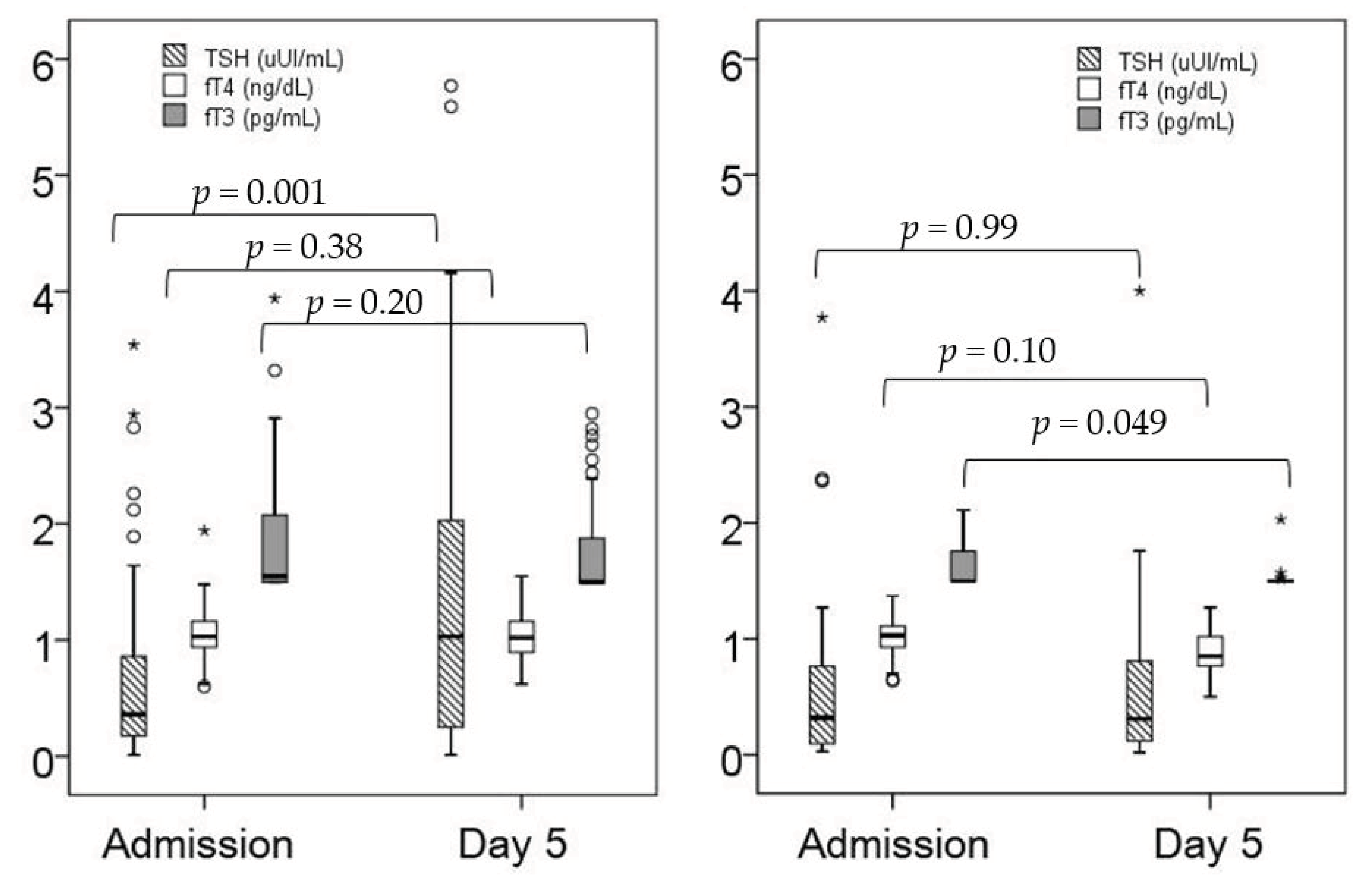{kind=link}
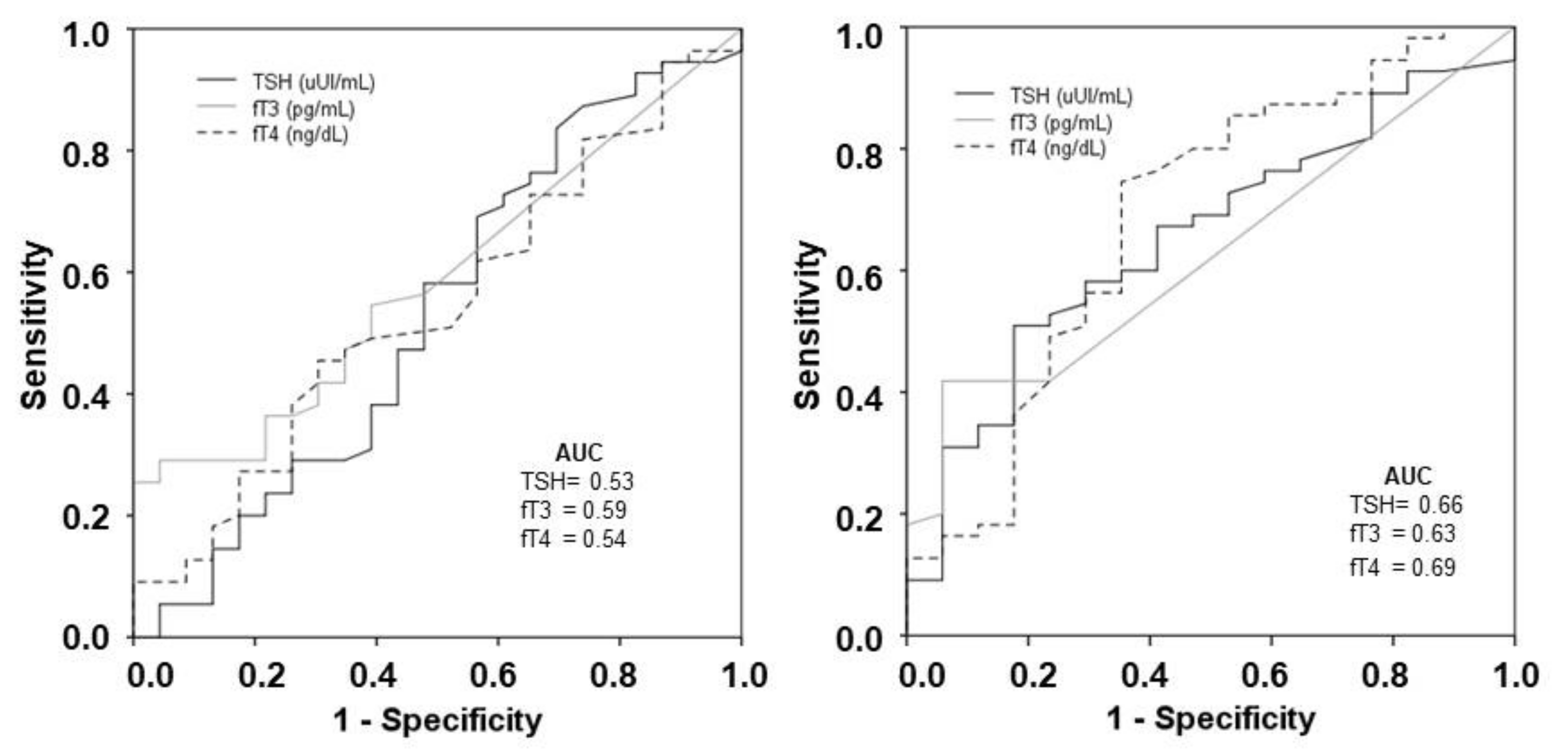{kind=link}
| Survivors N: 55 | Non-Survivors N: 23 | p Value | |
|---|---|---|---|
| Female, n (%) | 17 (30.9) | 6 (26.1) | 0.79 |
| Age (years) | 59 ± 12 | 68 ± 12 | 0.002 |
| Weight (kg) | 86 ± 20 | 80 ± 14 | 0.10 |
| Height (cm) | 170 ± 11 | 167 ± 10 | 0.27 |
| Body mass index | 29.8 ± 6.6 | 29.4 ± 5.1 | 0.74 |
| Symptoms to sampling, days | 10 (7–13) | 9 (6–11) | 0.58 |
| SAPS II | 38 (31–47) | 42 (37–50) | 0.01 |
| APACHE II | 17 (12–23) | 21 (15–24) | 0.08 |
| Admission SOFA | 5 (4–7) | 5 (4–8) | 0.33 |
| Comorbidities, n (%) | |||
| Hypertension | 26 (47.3) | 17 (73.9) | 0.04 |
| Diabetes mellitus | 12 (21.8) | 8 (34.8) | 0.26 |
| Dyslipidemia | 23 (41.8) | 14 (60.9) | 0.14 |
| COPD | 6 (10.9) | 4 (17.4) | 0.47 |
| Chronic kidney disease | 4 (7.3) | 5 (21.7) | 0.11 |
| Chronic liver disease | 1 (1.8) | 3 (13.0) | 0.07 |
| Chronic cardiac disease | 4 (7.3) | 8 (34.8) | 0.004 |
| Cancer (active) | 5 (9.1) | 4 (17.4) | 0.44 |
| Prior treatment, n (%) | |||
| Beta-blockers | 5 (9.1) | 8 (34.8) | 0.02 |
| ACE inhibitors | 9 (16.4) | 8 (34.8) | 0.13 |
| ARBs | 12 (21.8) | 7 (30.4) | 0.56 |
| Statins | 18 (32.7) | 12 (52.2) | 0.13 |
| Survivors | Non-Survivors | p Value | |
|---|---|---|---|
| Thyroid profile ICU admission | n: 55 | n: 23 | |
| TSH, uUI/mL | 0.68 ± 0.79 | 0.70 ± 0.94 | 0.91 |
| fT3, pg/mL * | 1.8 ± 0.5 | 1.6 ± 0.2 | 0.02 |
| fT4, ng/dL | 1.1 ± 0.2 | 1.0 ± 0.2 | 0.40 |
| Reverse fT3, ng/mL | 0.69 ± 0.23 | 0.65 ± 0.26 | 0.64 |
| NTIS, n (%) | 24 (43.6) | 12 (52.2) | 0.62 |
| Thyroid profile day 5 | n: 55 | n: 17 | |
| TSH, uUI/mL | 1.46 ± 1.69 | 0.70 ± 0.99 | 0.08 |
| fT3, pg/mL * | 1.8 ± 0.4 | 1.5 ± 0.1 | 0.001 |
| fT4, ng/dL | 1.0 ± 0.2 | 0.9 ± 0.2 | 0.02 |
| Reverse fT3, ng/mL | 0.49 ± 0.24 | 0.38 ± 0.17 | 0.19 |
| NTIS, n (%) | 30 (54.5) | 13 (56.5) | 1.0 |
| OR | 95% CI | p Value | |
|---|---|---|---|
| ICU admission | |||
| Age | 1.07 | 1.02 to 1.14 | 0.01 |
| Beta-blocker therapy | 4.25 | 1.15 to 15.76 | 0.03 |
| Day 5 | |||
| Age | 1.09 | 1.02 to 1.17 | 0.01 |
| fT4 | 0.02 | 0.001 to 0.53 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballesteros Vizoso, M.A.; Castilla, A.F.; Barceló, A.; Raurich, J.M.; Argente del Castillo, P.; Morell-García, D.; Velasco, J.; Pérez-Bárcena, J.; Llompart-Pou, J.A. Thyroid Disfunction in Critically Ill COVID-19 Patients. Relationship with In-Hospital Mortality. J. Clin. Med. 2021, 10, 5057. https://doi.org/10.3390/jcm10215057
Ballesteros Vizoso MA, Castilla AF, Barceló A, Raurich JM, Argente del Castillo P, Morell-García D, Velasco J, Pérez-Bárcena J, Llompart-Pou JA. Thyroid Disfunction in Critically Ill COVID-19 Patients. Relationship with In-Hospital Mortality. Journal of Clinical Medicine. 2021; 10(21):5057. https://doi.org/10.3390/jcm10215057
Chicago/Turabian StyleBallesteros Vizoso, María Antonieta, Albert Figueras Castilla, Antonia Barceló, Joan Maria Raurich, Paula Argente del Castillo, Daniel Morell-García, Julio Velasco, Jon Pérez-Bárcena, and Juan Antonio Llompart-Pou. 2021. "Thyroid Disfunction in Critically Ill COVID-19 Patients. Relationship with In-Hospital Mortality" Journal of Clinical Medicine 10, no. 21: 5057. https://doi.org/10.3390/jcm10215057
APA StyleBallesteros Vizoso, M. A., Castilla, A. F., Barceló, A., Raurich, J. M., Argente del Castillo, P., Morell-García, D., Velasco, J., Pérez-Bárcena, J., & Llompart-Pou, J. A. (2021). Thyroid Disfunction in Critically Ill COVID-19 Patients. Relationship with In-Hospital Mortality. Journal of Clinical Medicine, 10(21), 5057. https://doi.org/10.3390/jcm10215057