
Increased Geriatric Treatment Frequency Improves Mobility and Secondary Fracture Prevention in Older Adult Hip Fracture Patients—An Observational Cohort Study of 23,828 Patients from the Registry for Geriatric Trauma (ATR-DGU)

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
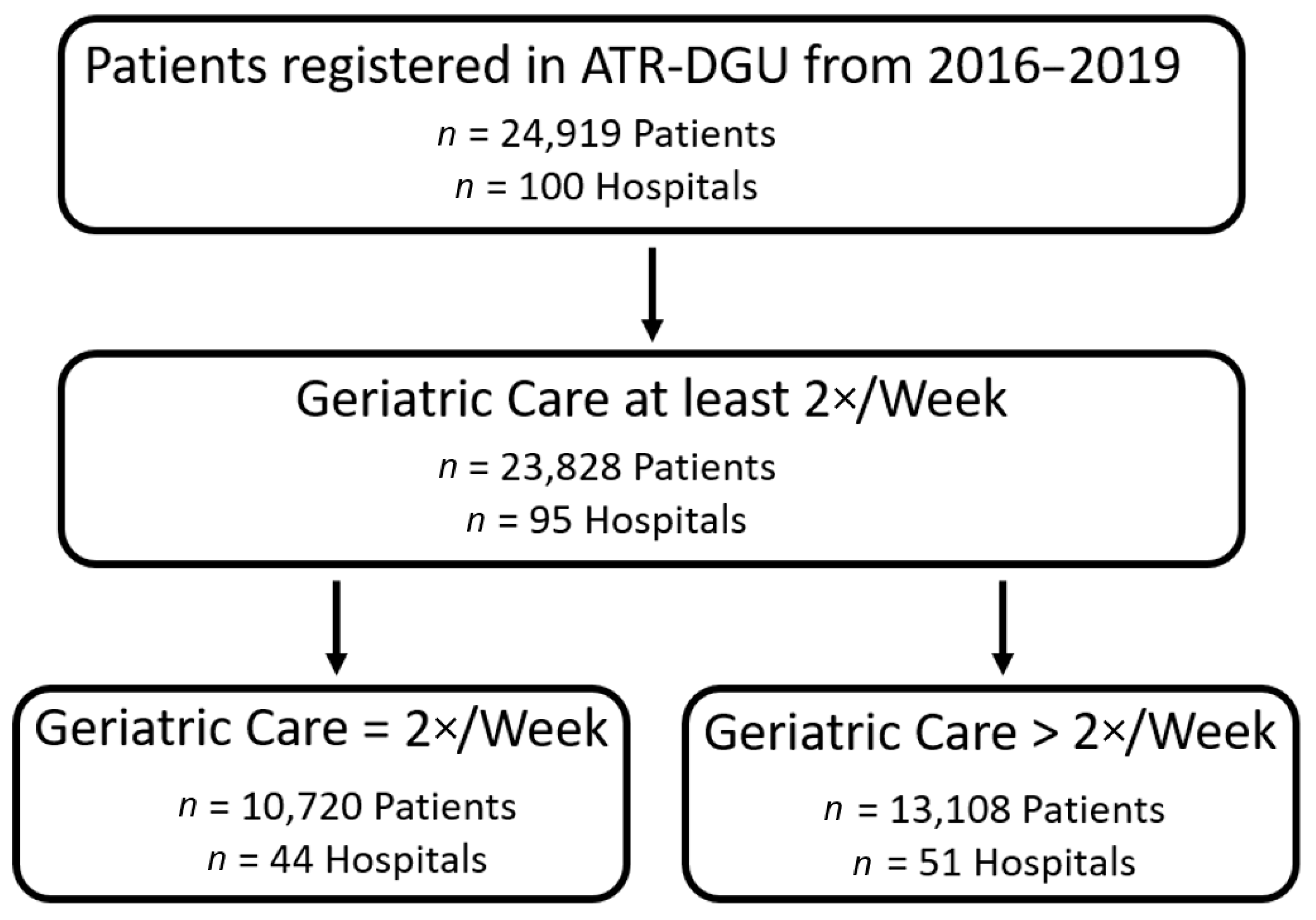
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neuerburg, C.; Förch, S.; Gleich, J.; Böcker, W.; Gosch, M.; Kammerlander, C.; Mayr, E. Improved outcome in hip fracture patients in the aging population following co-managed care compared to conventional surgical treatment: A retrospective, dual-center cohort study. BMC Geriatr. 2019, 19, 330. [Google Scholar] [CrossRef]
- Prestmo, A.; Hagen, G.; Sletvold, O.; Helbostad, J.L.; Thingstad, P.; Taraldsen, K.; Lydersen, S.; Halsteinli, V.; Saltnes, T.; Lamb, S.E.; et al. Comprehensive geriatric care for patients with hip fractures: A prospective, randomised, controlled trial. Lancet 2015, 385, 1623–1633. [Google Scholar] [CrossRef] [Green Version]
- Rapp, K.; Becker, C.; Todd, C.; Rothenbacher, D.; Schulz, C.; König, H.-H.; Liener, U.; Hartwig, E.; Büchele, G. The Association Between Orthogeriatric Co-Management and Mortality Following Hip Fracture. Dtsch. Aerzteblatt. Online 2020, 117, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Castelli, A.; Daidone, S.; Jacobs, R.; Kasteridis, P.; Street, A.D. The Determinants of Costs and Length of Stay for Hip Fracture Patients. PLoS ONE 2015, 10, e0133545. [Google Scholar] [CrossRef]
- Guzon-Illescas, O.; Fernandez, E.P.; Villarias, N.C.; Donate, F.J.Q.; Peña, M.; Alonso-Blas, C.; Vadillo, A.G.; Mazzucchelli, R. Mortality after osteoporotic hip fracture: Incidence, trends, and associated factors. J. Orthop. Surg. Res. 2019, 14, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downey, C.; Kelly, M.; Quinlan, J.F. Changing trends in the mortality rate at 1-year post hip fracture—A systematic review. World J. Orthop. 2019, 10, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Hagen, G.; Magnussen, J.; Tell, G.; Omsland, T. Estimating the future burden of hip fractures in Norway. A NOREPOS study. Bone 2020, 131, 115156. [Google Scholar] [CrossRef] [PubMed]
- Uriz-Otano, F.; Uriz-Otano, J.I.; Malafarina, V. Factors Associated With Short-Term Functional Recovery in Elderly People with a Hip Fracture. Influence of Cognitive Impairment. J. Am. Med. Dir. Assoc. 2015, 16, 215–220. [Google Scholar] [CrossRef]
- Pfeufer, D.; Zeller, A.; Mehaffey, S.; Böcker, W.; Kammerlander, C.; Neuerburg, C. Weight-bearing restrictions reduce postoperative mobility in elderly hip fracture patients. Arch. Orthop. Trauma Surg. 2019, 139, 1253–1259. [Google Scholar] [CrossRef]
- Sheehan, K.J.; Goubar, A.; Almilaji, O.; Martin, F.C.; Potter, C.; Jones, G.D.; Sackley, C.; Ayis, S. Discharge after hip fracture surgery by mobilisation timing: Secondary analysis of the UK National Hip Fracture Database. Age Ageing 2021, 50, 415–422. [Google Scholar] [CrossRef]
- Wu, C.-H.; Tu, S.-T.; Chang, Y.-F.; Chan, D.-C.; Chien, J.-T.; Lin, C.-H.; Singh, S.; Dasari, M.; Chen, J.-F.; Tsai, K.-S. Fracture liaison services improve outcomes of patients with osteoporosis-related fractures: A systematic literature review and meta-analysis. Bone 2018, 111, 92–100. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, N.T.; Kates, S.L. Co-managed Care: The Gold Standard for Geriatric Fracture Care. Curr. Osteoporos. Rep. 2012, 10, 312–316. [Google Scholar] [CrossRef]
- Johansen, A.; Boulton, C.; Hertz, K.; Ellis, M.; Burgon, V.; Rai, S.; Wakeman, R. The National Hip Fracture Database (NHFD)—Using a national clinical audit to raise standards of nursing care. Int. J. Orthop. Trauma Nurs. 2017, 26, 3–6. [Google Scholar] [CrossRef]
- Kristensen, P.K.; Röck, N.D.; Christensen, H.C.; Pedersen, A.B. The Danish Multidisciplinary Hip Fracture Registry 13-Year Results from a Population-Based Cohort of Hip Fracture Patients. Clin. Epidemiol. 2020, 12, 9–21. [Google Scholar] [CrossRef] [Green Version]
- Ojeda-Thies, C.; Rnfc, O.B.O.T.P.I.T.; Sáez-López, P.; Currie, C.; Tarazona-Santalbina, F.; Alarcón, T.; Muñoz-Pascual, A.; Pareja, T.; Gómez-Campelo, P.; Montero-Fernández, N.; et al. Spanish National Hip Fracture Registry (RNFC): Analysis of its first annual report and international comparison with other established registries. Osteoporos. Int. 2019, 30, 1243–1254. [Google Scholar] [CrossRef]
- Tan, A.C.; Armstrong, E.; Close, J.; Harris, I.A. Data quality audit of a clinical quality registry: A generic framework and case study of the Australian and New Zealand Hip Fracture Registry. BMJ Open Qual. 2019, 8, e000490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoeneberg, C.; Knobe, M.; Babst, R.; Friess, T.; Volland, R.; Hartwig, E.; Schmidt, W.; Lendemans, S.; Buecking, B. 120-day follow-up after proximal femoral fractures-first results from the Geriatric Trauma Registry DGU(R). Unfallchirurg 2020, 123, 375–385. [Google Scholar] [CrossRef]
- McCusker, J.; Bellavance, F.; Cardin, S.; Trepanier, S.; Verdon, J.; Ardman, O. Detection of Older People at Increased Risk of Adverse Health Outcomes After an Emergency Visit: The ISAR Screening Tool. J. Am. Geriatr. Soc. 1999, 47, 1229–1237. [Google Scholar] [CrossRef] [PubMed]
- Pugely, A.J.; Martin, C.T.; Harwood, J.; Ong, K.L.; Bozic, K.J.; Callaghan, J.J. Database and Registry Research in Orthopaedic Surgery: Part 2: Clinical Registry Data. J. Bone Jt. Surg. Am 2015, 97, 1799–1808. [Google Scholar] [CrossRef] [PubMed]
- Newgard, C.D.; Caughey, A.; McConnell, K.J.; Lin, A.; Eckstrom, E.; Griffiths, D.; Malveau, S.; Bulger, E. Comparison of Injured Older Adults Included in vs Excluded From Trauma Registries With 1-Year Follow-up. JAMA Surg. 2019, 154, e192279. [Google Scholar] [CrossRef]
- Said, C.M.; Delahunt, M.; Ciavarella, V.; Al Maliki, D.; Boys, A.-M.; Vogrin, S.; Berney, S. Factors Impacting Early Mobilization Following Hip Fracture: An Observational Study. J. Geriatr. Phys. Ther. 2021, 44, 88–93. [Google Scholar] [CrossRef]
- Wall, B.T.; Dirks, M.; van Loon, L.J. Skeletal muscle atrophy during short-term disuse: Implications for age-related sarcopenia. Ageing Res. Rev. 2013, 12, 898–906. [Google Scholar] [CrossRef]
- Hvid, L.; Suetta, C.; Nielsen, J.; Jensen, M.; Frandsen, U.; Ørtenblad, N.; Kjaer, M.; Aagaard, P. Aging impairs the recovery in mechanical muscle function following 4days of disuse. Exp. Gerontol. 2014, 52, 1–8. [Google Scholar] [CrossRef]
- Xue, Q.L.; Bandeen-Roche, K.; Varadhan, R.; Zhou, J.; Fried, L.P. Initial manifestations of frailty criteria and the development of frailty phenotype in the Women’s Health and Aging Study II. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 984–990. [Google Scholar] [CrossRef] [Green Version]
- Lim, K.K.; Matchar, D.B.; Chong, J.L.; Yeo, W.; Howe, T.S.; Koh, J.S.B. Pre-discharge prognostic factors of physical function among older adults with hip fracture surgery: A systematic review. Osteoporos. Int. 2019, 30, 929–938. [Google Scholar] [CrossRef]
- Ryg, J.; Rejnmark, L.; Overgaard, S.; Brixen, K.; Vestergaard, P. Hip Fracture Patients at Risk of Second Hip Fracture: A Nationwide Population-Based Cohort Study of 169,145 Cases During 1977–2001. J. Bone Miner. Res. 2009, 24, 1299–1307. [Google Scholar] [CrossRef]
- Aspenberg, P.; Malouf, J.; Tarantino, U.; García-Hernández, P.A.; Corradini, C.; Overgaard, S.; Stepan, J.J.; Borris, L.; Lespessailles, E.; Frihagen, F.; et al. Effects of Teriparatide Compared with Risedronate on Recovery After Pertrochanteric Hip Fracture: Results of a Randomized, Active-Controlled, Double-Blind Clinical Trial at 26 Weeks. J. Bone Jt. Surg. Am. 2016, 98, 1868–1878. [Google Scholar] [CrossRef]
- Driessen, A.; Partners, T.; Schäfer, N.; Albrecht, V.; Schenk, M.; Fröhlich, M.; Stürmer, E.K.; Maegele, M. Infrastructure and clinical practice for the detection and management of trauma-associated haemorrhage and coagulopathy. Eur. J. Trauma Emerg. Surg. 2014, 41, 413–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forni, S.; Pieralli, F.; Sergi, A.; Lorini, C.; Bonaccorsi, G.; Vannucci, A. Mortality after hip fracture in the elderly: The role of a multidisciplinary approach and time to surgery in a retrospective observational study on 23,973 patients. Arch. Gerontol. Geriatr. 2016, 66, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Neuburger, J.; Currie, C.; Wakeman, R.; Johansen, A.; Tsang, C.; Plant, F.; Wilson, H.; Cromwell, D.A.; van der Meulen, J.; De Stavola, B.L. Increased orthogeriatrician involvement in hip fracture care and its impact on mortality in England. Age Ageing 2016, 46, 187–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Geriatric Treatment >2×/Week | Geriatric Treatment 2×/Week | p-Value | |
|---|---|---|---|
| Total Patients | n = 13,108 | n = 10,720 | |
| Age (years) | (n = 12,979) | (n = 10,623) | 0.016 |
| median (IQR) | 85 (80; 89) | 84 (80; 89) | |
| Sex | (n = 13,082) | (n = 10,687) | 0.325 |
| Female | 9503 (72.6%) | 7701 (72.1%) | |
| ASA | (n = 12,909) | (n = 10,566) | 0.009 |
| 1 | 147 (1.1%) | 113 (1.1%) | |
| 2 | 2780 (21.5%) | 2454 (23.2%) | |
| 3 | 8943 (69.3%) | 7240 (68.5%) | |
| 4 | 1031 (8%) | 751 (7.1%) | |
| 5 | 8 (0.1%) | 8 (0.1%) | |
| ISAR Score | (n = 8220) | (n = 7260) | 0.001 |
| 0 | 773 (5.0%) | 493 (3.2%) | |
| 1 | 1036 (6.7%) | 830 (5.4%) | |
| 2 | 1833 (11.8%) | 1507 (9.7%) | |
| 3 | 1915 (12.4%) | 1887 (12.2%) | |
| 4 | 1698 (11.0%) | 1549 (10.0%) | |
| 5 | 748 (4.8%) | 728 (4.7%) | |
| 6 | 217 (1.4%) | 266 (1.7%) | |
| Walking ability pre-fracture | (n = 12,091) | (n = 10,035) | 0.002 |
| Without aids | 4214 (34.9%) | 3273 (32.6%) | |
| With one crutch/cane | 1587 (13.1%) | 1279 (12.7%) | |
| With 2 crutches/walker | 3841 (31.8%) | 3368 (33.6%) | |
| Only at home | 2041 (16.9%) | 1787 (17.8%) | |
| none | 408 (3.4%) | 328 (3.3%) | |
| Place of residence pre-fracture | (n = 3420) | (n = 2709) | <0.001 |
| At home | 3039 (88.9%) | 2409 (88.9%) | |
| Nursing Home | 198 (5.8%) | 107 (3.9%) | |
| Hospital (Inpatient fracture) | 78 (2.3%) | 57 (2.1%) | |
| Other | 105 (3.1%) | 136 (5%) | |
| Type of fracture | (n = 13,071) | (n = 10,683) | 0.135 |
| femoral neck | 5602 (42.9%) | 4674 (43.8%) | |
| pertrochanteric | 6024 (46.2%) | 4874 (45.6%) | |
| subtrochanteric | 540 (4.1%) | 393 (3.7%) | |
| periprosthetic | 709 (5.4%) | 589 (5.5%) | |
| other | 196 (1.5%) | 153 (1.4%) | |
| Osteoporosis treatment pre-fracture | (n = 12,564) | (n = 10,375) | <0.001 |
| Yes | 2886 (23.0%) | 1787 (17.2%) | |
| Mobilization 1 day after surgery | (n = 12,883) | (n = 10,609) | 0.078 |
| Yes | 10,355 (80.4%) | 8428 (79.4%) | |
| Walking ability 7 days after surgery | (n = 12,585) | (n = 10,297) | <0.001 |
| No mobility | 9699 (77.1%) | 8201 (79.6%) | |
| Able to walk (with/without assistance) | 2886 (22.9%) | 2096 (20.4%) | |
| Osteoporosis treatment | (n = 13,031) | (n = 10,672) | <0.001 |
| 7 days after surgery | |||
| Yes | 9622 (73.8%) | 5623 (52.7%) | |
| Initiation of early | (n = 11,089) | (n = 9352) | <0.001 |
| complex geriatric care | |||
| Yes | 7150 (64.5%) | 5428 (58.0%) | |
| Time to surgery | (n = 12,979) | (n = 10,612) | 0.002 |
| Median (IQR) in hours | 18.1 (7.75; 26.7) | 17.8 (7.0; 24.8) | |
| Revision surgery | (n = 13,090) | (n = 10,709) | 0.0089 |
| Yes | 483 (3.7%) | 328 (3.1%) | |
| Mortality | (n = 12,733/5392) | (n = 10,395/3249) | 0.0643 |
| inpatient | 737 (5.8%) | 543(5.2%) | 0.0639 |
| 120 day follow-up | 625 (11.6%) | 365 (11.2%) | |
| Discharge Location | (n = 12,966) | (n = 10,645) | <0.0001 |
| Home | 2880 (22.2%) | 2357 (22.1%) | |
| Nursing Home | 3700 (28.5%) | 2532 (23.8%) | |
| Rehabilitation clinic | 5164 (39.9%) | 4904 (46.2) | |
| Other Hospital | 233 (1.8%) | 250 (2.3%) | |
| Other hospital ward | 44 (0.3%) | 28 (0.3%) | |
| Other | 208 (1.6%) | 31 (0.3%) | |
| Died in-house | 737 (5.7%) | 543 (5.1%) |
| Impact of Geriatric Treatment Frequency on | N | OR | 95%-CI | p-Value |
|---|---|---|---|---|
| Mobilization 1 day after surgery | 23,383 | 1.07 | (1.00; 1.14) | 0.040 |
| Walking ability 7 days after surgery | 22,768 | 1.14 | (1.07; 1.22) | <0.001 |
| Osteoporosis treatment 7 days after surgery | 22,735 | 2.54 | (2.40; 2.70] | <0.001 |
| Initiation of early complex geriatric care | 20,422 | 1.32 | (1.24; 1.39) | <0.001 |
| Discharge to home | 21,496 | 1.05 | (0.98; 1.11) | 0.162 |
| Inpatient mortality | 23,615 | 1.09 | (0.96; 1.22) | 0.167 |
| N | β | |||
| Time to surgery (hours) | 23,468 | −0.03 | (−0.84; 0.77) | 0.934 |
| Impact of Geriatric Treatment Frequency on | N | OR | 95%-CI | p-Value |
|---|---|---|---|---|
| Walking ability | 7590 | 1.10 | (1.00; 1.21) | 0.047 |
| Osteoporosis treatment 120 days after treatment | 5351 | 1.68 | (1.50; 1.90) | <0.001 |
| Living at home | 7415 | 0.73 | (0.66; 0.82) | <0.001 |
| Death within follow-up | 8571 | 1.02 | (0.88; 1.17) | 0.527 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gleich, J.; Fleischhacker, E.; Rascher, K.; Friess, T.; Kammerlander, C.; Böcker, W.; Bücking, B.; Liener, U.; Drey, M.; Höfer, C.; et al. Increased Geriatric Treatment Frequency Improves Mobility and Secondary Fracture Prevention in Older Adult Hip Fracture Patients—An Observational Cohort Study of 23,828 Patients from the Registry for Geriatric Trauma (ATR-DGU). J. Clin. Med. 2021, 10, 5489. https://doi.org/10.3390/jcm10235489
Gleich J, Fleischhacker E, Rascher K, Friess T, Kammerlander C, Böcker W, Bücking B, Liener U, Drey M, Höfer C, et al. Increased Geriatric Treatment Frequency Improves Mobility and Secondary Fracture Prevention in Older Adult Hip Fracture Patients—An Observational Cohort Study of 23,828 Patients from the Registry for Geriatric Trauma (ATR-DGU). Journal of Clinical Medicine. 2021; 10(23):5489. https://doi.org/10.3390/jcm10235489
Chicago/Turabian StyleGleich, Johannes, Evi Fleischhacker, Katherine Rascher, Thomas Friess, Christian Kammerlander, Wolfgang Böcker, Benjamin Bücking, Ulrich Liener, Michael Drey, Christine Höfer, and et al. 2021. "Increased Geriatric Treatment Frequency Improves Mobility and Secondary Fracture Prevention in Older Adult Hip Fracture Patients—An Observational Cohort Study of 23,828 Patients from the Registry for Geriatric Trauma (ATR-DGU)" Journal of Clinical Medicine 10, no. 23: 5489. https://doi.org/10.3390/jcm10235489
APA StyleGleich, J., Fleischhacker, E., Rascher, K., Friess, T., Kammerlander, C., Böcker, W., Bücking, B., Liener, U., Drey, M., Höfer, C., & Neuerburg, C. (2021). Increased Geriatric Treatment Frequency Improves Mobility and Secondary Fracture Prevention in Older Adult Hip Fracture Patients—An Observational Cohort Study of 23,828 Patients from the Registry for Geriatric Trauma (ATR-DGU). Journal of Clinical Medicine, 10(23), 5489. https://doi.org/10.3390/jcm10235489