
The Impact of Recipient Demographics on Outcomes from Living Donor Kidneys: Systematic Review and Meta-Analysis †

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Outcomes of Interest
2.4. Screening and Data Extraction
2.5. Risk of Bias Assessment
2.6. Meta-Analysis
3. Results
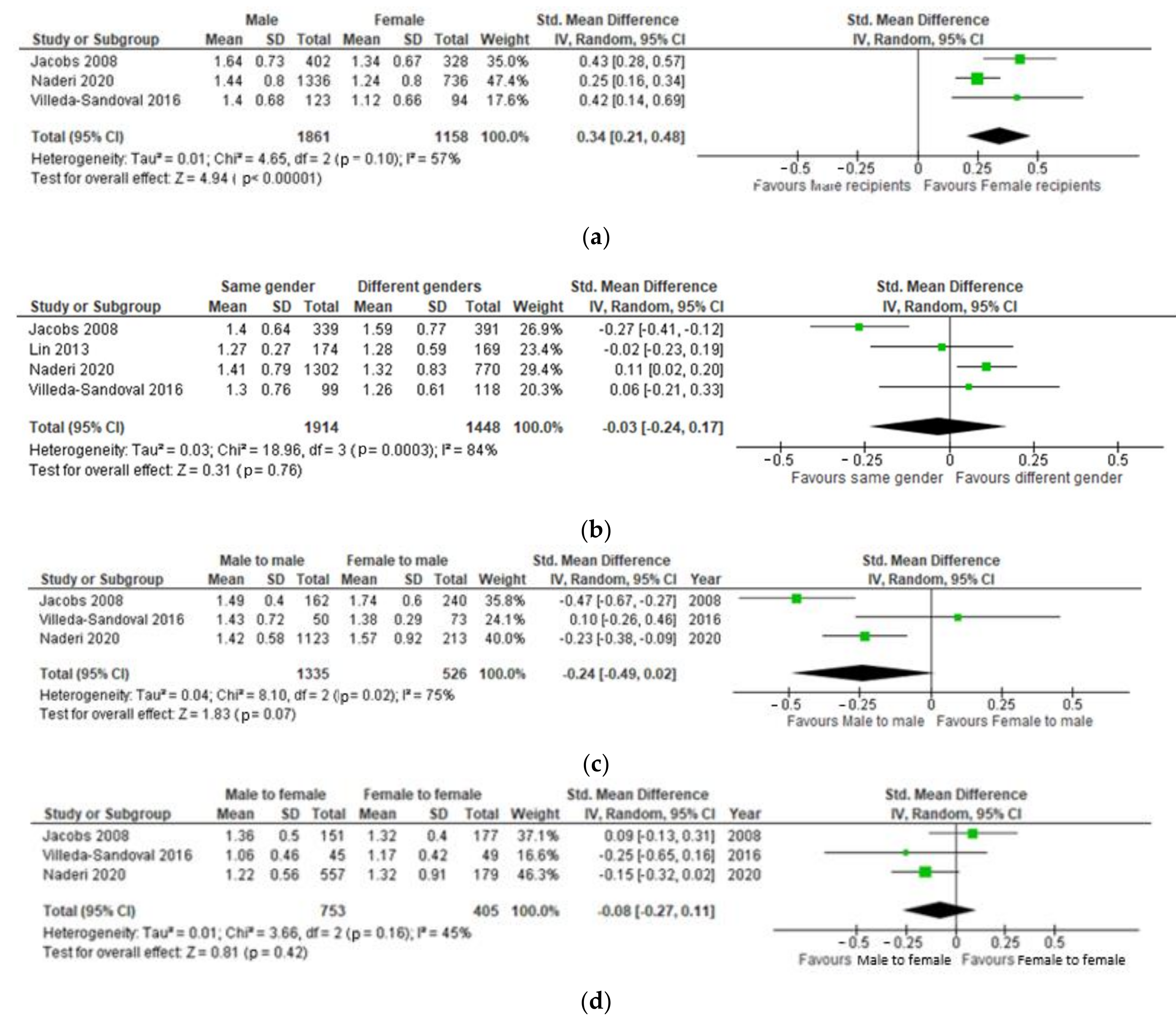
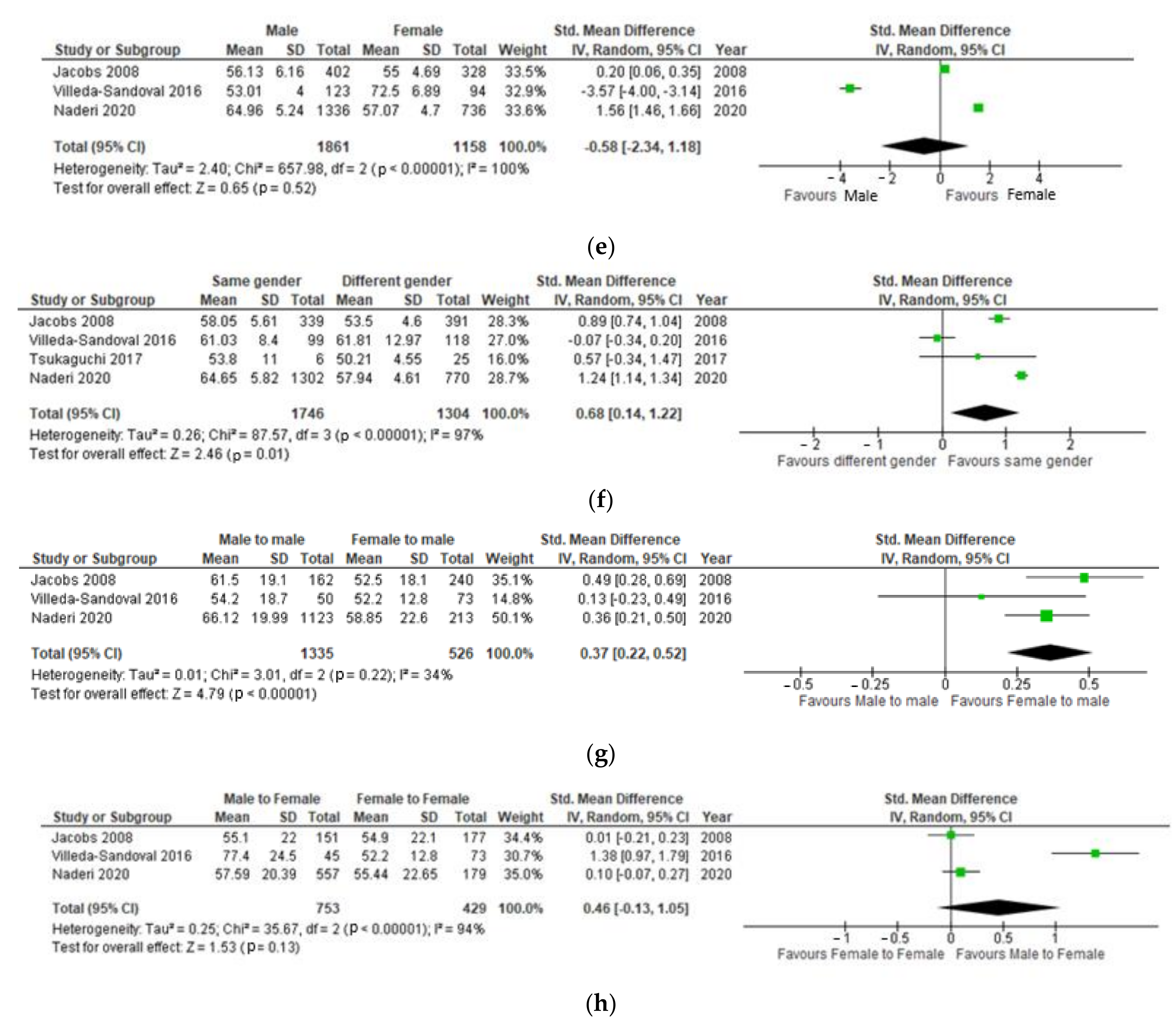
3.1. Recipient Sex
3.2. Recipient Ethnicity
3.3. Recipient Body Mass Index
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A. Search Strategy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Step | Input |
|---|---|
| 1 | gender/ or "gender and sex"/ |
| 2 | sex/ or sex difference/ |
| 3 | sex |
| 4 | age/ |
| 5 | ethnicit* |
| 6 | ethnic minorit* |
| 7 | BAME |
| 8 | exp "ethnic or racial aspects"/ |
| 9 | BMI/ |
| 10 | BMI or weight |
| 11 | genetic relationship/ |
| 12 | 1 or 2 or 3 or 4 |
| 13 | 5 or 6 or 7 or 8 or 9 or 10 or 11 |
| 14 | 12 and 13 |
| 15 | exp kidney donor/ |
| 16 | kidney transplantation/ |
| 17 | living donor/ |
| 18 | exp graft recipient/ |
| 19 | 15 or 16 or 17 or 18 |
| 20 | 14 and 19 |
| Step | Input |
|---|---|
| 1 | TS=(sex or gender) |
| 2 | TS=(sex and difference) |
| 3 | TS=age |
| 4 | TS=(ethnicit* or ethnic minorit*) |
| 5 | TS=BAME |
| 6 | TS=(ethnic* or race) |
| 7 | TS=(BMI or weight) |
| 8 | TS=genetic relationship |
| 9 | #1 or #2 or #3 |
| 10 | #4 or #5 or #6 or #7 or #8 |
| 11 | #9 and #10 |
| 12 | TS=kidney |
| 13 | TS=transplantation |
| 14 | TS=(living or live or non-deceased) |
| 15 | TS=(donor) |
| 16 | TS=graft |
| 17 | TS=recipient |
| 18 | #12 and #13 and #14 and #15 and #16 and #17 |
| 19 | #11 and #18 |
| Step | Input |
|---|---|
| 1 | MeSH descriptor: [Gender Identity] this term only |
| 2 | MeSH descriptor: [Sex] this term only |
| 3 | MeSH descriptor: [Sex Characteristics] this term only |
| 4 | (sex):ti,ab,kw |
| 5 | MeSH descriptor: [Age Factors] this term only |
| 6 | ethnicit* |
| 7 | ethnic minorit* |
| 8 | BAME |
| 9 | BMI |
| 10 | weight |
| 11 | MeSH descriptor: [Family] explode all trees |
| 12 | genetic relationship |
| 13 | MeSH descriptor: [Ethnic Groups] explode all trees |
| 14 | MeSH descriptor: [Continental Population Groups] explode all trees |
| 15 | #1 or #2 or #3 or #4 or #5 |
| 16 | #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 |
| 17 | #15 or #16 |
| 18 | MeSH descriptor: [Kidney] explode all trees |
| 19 | MeSH descriptor: [Tissue Donors] explode all trees |
| 20 | MeSH descriptor: [Transplantation] explode all trees |
| 21 | MeSH descriptor: [Transplant Recipients] explode all trees |
| 22 | #18 and #19 |
| 23 | #18 and #20 |
| 24 | #18 and #21 |
| 25 | #22 or #23 or #24 |
| 26 | Kidney 51158 |
| 27 | donor or transplantation or recipient or transplant |
| 28 | #26 and #27 |
| 29 | #17 AND #25 |
| 30 | #17 AND #28 |
| 31 | #29 or #30 |
Appendix B. Risk of Bias Assessment
| Reference number | Country of study | Authors | 1. Was the resarch question clearly stated? | 2. Was the study population clearly specified and defined? | 3. Was the participation of eligible persons at least 50%? | 4. Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants? | 5. Was a sample size justification, power description, or variance and effect estimates provided? | 6. For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured? | 7. Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed? | 8. For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (e.g., categories of exposure, or exposure measured as continuous variable)? | 9. Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? | 10. Was the exposure(s) assessed more than once over time? | 11. Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? | 12. Were the outcome assessors blinded to the exposure status of participants? | 13. Was loss to follow-up after baseline 20% or less? | 14. Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)? | Quality Rating (Good, Fair or Poor) |
| [5] | USA | Redfield, R.R., et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | Yes | Good |
| [9] | Iran | Naderi, G., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | Not applicable | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [11] | USA | Jacobs, S.C., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | Not applicable | Yes | Not applicable | Yes | No | Yes | Yes | Good |
| [12] | Egypt | Wafa, E.W., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | Not applicable | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [13] | Mexico | Villeda-Sandoval, C.I., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | Not applicable | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [14] | China | Lin, J., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | Not applicable | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [15] | China | Xu, J., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | Not applicable | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [16] | China | Xie, L., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | Not applicable | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [17] | Japan | Yanishi, M., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | Not applicable | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [18] | South Korea | Oh, C.-K., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | Not applicable | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [19] | USA | Pfaff, W.W., et al. | No | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [20] | USA | Garvin, P.J., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [21] | USA | Modlin, C.S., et al. | YEs | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | Yes | Good |
| [22] | UK | Williams, A., et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | Yes | Good |
| [23] | USA | Isaacs, R.B., et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | yes | Good |
| [24] | USA | Ilyas, M., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [26] | USA | Koyama, H. et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | Yes | Good |
| [27] | USA | Smith, S.R. et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | Yes | Good |
| [28] | USA | Howard, R.J., et al. | YEs | Yes | No | Yes | No | Yes | Yes | No | Yes | Not applicable | Yes | No | Not stated | No | Fair |
| [29] | USA | Marks, W.H., et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [30] | USA | Mehta, R., et al. | Yes | Yes | YEs | Yes | No | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | No | Fair |
| [31] | Turkey | Erturk, T. et al. | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Not applicable | Yes | No | Not stated | No | Fair |
| [32] | China | Wang, K. et al. | No | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | ||
| [33] | USA | Kwan, J.M., et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Not applicable | Yes | No | Yes | Yes | Good |
References
- Policies and guidance ODT. Available online: https://www.odt.nhs.uk/transplantation/tools-policies-and-guidance/policies-and-guidance/ (accessed on 18 November 2021).
- LaPointe, R.D.; Hays, R.; Baliga, P.; Cohen, D.J.; Cooper, M.; Danovitch, G.M.; Dew, M.A.; Gordon, E.J.; Mandelbrot, D.A.; McGuire, S.; et al. Consensus conference on best practices in live kidney donation: Recommendations to optimize education, access, and care. American journal of transplantation. Am. J. Transplant. 2015, 15, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Bellini, M.I.; Courtney, A.E.; McCaughan, J.A. Living Donor Kidney Transplantation Improves Graft and Recipient Survival in Patients with Multiple Kidney Transplants. J. Clin. Med. 2020, 9, 2118. [Google Scholar] [CrossRef]
- Kerr, K.F.; Morenz, E.R.; Thiessen-Philbrook, H.; Coca, S.G.; Wilson, F.P.; Reese, P.P.; Parikh, C.R. Quantifying Donor Effects on Transplant Outcomes Using Kidney Pairs from Deceased Donors. Clin. J. Am. Soc. Nephrol. 2019, 14, 1781–1787. [Google Scholar] [CrossRef]
- Redfield, R.R.; Scalea, J.R.; Zens, T.J.; Muth, B.; Kaufman, D.B.; Djamali, A.; Astor, B.C.; Mohamed, M. Predictors and outcomes of delayed graft function after living-donor kidney transplantation. Transpl. Int. 2016, 29, 81–87. [Google Scholar] [CrossRef]
- Bellini, M.I.; Paoletti, F.; Herbert, P.E. Obesity and bariatric intervention in patients with chronic renal disease. J. Int. Med. Res. 2019, 47, 2326–2341. [Google Scholar] [CrossRef] [PubMed]
- Bellini, M.I.; Koutroutsos, K.; Galliford, J.; Herbert, P.E. One-Year Outcomes of a Cohort of Renal Transplant Patients Related to BMI in a Steroid-Sparing Regimen. Transpl. Direct 2017, 3, e330. [Google Scholar] [CrossRef]
- Bellini, M.I.; Koutroutsos, K.; Nananpragasam, H.; Deurloo, E.; Galliford, J.; Herbert, P.E. Obesity affects graft function but not graft loss in kidney transplant recipients. J. Int. Med. Res. 2020, 48, 300060519895139. [Google Scholar] [CrossRef]
- Naderi, G.; Azadfar, A.; Yahyazadeh, S.R.; Khatami, F.; Aghamir, S.M.K. Impact of the donor-recipient gender matching on the graft survival from live donors. BMC Nephrol. 2020, 21, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purnell, T.S.; Luo, X.; Cooper, L.A.; Massie, A.B.; Kucirka, L.M.; Henderson, M.L.; Gordon, E.J.; Crews, D.C.; Boulware, E.; Segev, D.L. Association of Race and Ethnicity With Live Donor Kidney Transplantation in the United States From 1995 to 2014. Jama 2018, 319, 49–61. [Google Scholar] [CrossRef]
- Jacobs, S.C.; Nogueira, J.M.; Phelan, M.W.; Bartlett, S.T.; Cooper, M. Transplant recipient renal function is donor renal mass- and recipient gender-dependent. Transpl. Int. 2008, 21, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Wafa, E.W.; Shokeir, A.; Akl, A.; Hassan, N.; Fouda, M.A.; El Dahshan, K.; Ghoneim, M.A. Effect of donor and recipient variables on the long-term live-donor renal allograft survival in children. Arab. J. Urol. 2011, 9, 85–91. [Google Scholar] [CrossRef]
- Villeda-Sandoval, C.I.; Rodríguez-Covarrubias, F.; Martinez, A.G.-C.Y.; Lara-Nuñez, D.; Guinto-Nishimura, G.Y.; González-Sánchez, B.; Magaña-Rodríguez, J.D.; Alberú-Gómez, J.; Vilatobá-Chapa, M.; Gabilondo-Pliego, B. The impact of donor-to-recipient gender match and mismatch on the renal function of living donor renal graft recipients. Gac. Med. Mex. 2016, 152, 645–650. [Google Scholar]
- Lin, J.; Zheng, X.; Xie, Z.-L.; Sun, W.; Zhang, L.; Tian, Y.; Guo, Y.-W. Factors potentially affecting the function of kidney grafts. Chin. Med. J. 2013, 126, 1738–1742. [Google Scholar] [PubMed]
- Xu, J.; Xu, L.; Wei, X.; Li, X.; Cai, M. Incidence and Risk Factors of Posttransplantation Diabetes Mellitus in Living Donor Kidney Transplantation: A Single-Center Retrospective Study in China. Transplant. Proc. 2018, 50, 3381–3385. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Tang, W.; Wang, X.; Wang, L.; Lu, Y.; Lin, T. Pretransplantation Risk Factors Associated With New-onset Diabetes After Living-donor Kidney Transplantation. Transplant. Proc. 2016, 48, 3299–3302. [Google Scholar] [CrossRef] [PubMed]
- Yanishi, M.; Tsukaguchi, H.; Huan, N.T.; Koito, Y.; Taniguchi, H.; Yoshida, K.; Mishima, T.; Sugi, M.; Kinoshita, H.; Matsuda, T. Correlation of whole kidney hypertrophy with glomerular over-filtration in live, gender-mismatched renal transplant allografts. Nephrology 2017, 22, 1002–1007. [Google Scholar] [CrossRef] [PubMed]
- Oh, C.-K.; Lee, B.M.; Jeon, K.O.; Kim, H.J.; Pelletier, S.J.; Kim, S.I.; Kim, Y.S. Gender-related differences of renal mass supply and metabolic demand after living donor kidney transplantation. Clin. Transplant. 2006, 20, 163–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfaff, W.W.; Morehead, R.A.; Fennell, R.S.; Mars, D.R.; Thomas, J.M.; Brient, B.W. The role of various risk factors in living related donor renal transplant success. Ann. Surg. 1980, 191, 617–625. [Google Scholar] [CrossRef]
- Garvin, P.J.; Castaneda, M.; Codd, J.E.; Mauller, K. Recipient race as a risk factor in renal transplantation. Arch. Surg. 1983, 118, 1441–1444. [Google Scholar] [CrossRef]
- Modlin, C.S.; Alster, J.M.; Saad, I.R.; Tiong, H.Y.; Mastroianni, B.; Savas, K.M.; Zaramo, C.E.; Kerr, H.L.; Goldfarb, D.; Flechner, S.M. Renal Transplantations in African Americans: A Single-center Experience of Outcomes and Innovations to Improve Access and Results. Urology 2014, 84, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Richardson, C.; McCready, J.; Anderson, B.; Khalil, K.; Tahir, S.; Nath, J.; Sharif, A. Black Ethnicity is Not a Risk Factor for Mortality or Graft Loss After Kidney Transplant in the United Kingdom. Exp. Clin. Transpl. 2018, 16, 682–689. [Google Scholar]
- Isaacs, R.B.; Nock, S.L.; Spencer, C.E.; Connors, A.F.; Wang, X.-Q.; Sawyer, R.; Lobo, P.I. Racial disparities in renal transplant outcomes. Am. J. Kidney Dis. 1999, 34, 706–712. [Google Scholar] [CrossRef]
- Ilyas, M.; Ammons, J.D.; Gaber, A.O.; Iii., S.R.; Batisky, D.L.; Chesney, R.W.; Jones, D.P.; Wyatt, R. Comparable renal graft survival in African-American and Caucasian recipients. Pediatric Nephrol. 1998, 12, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Sumrani, N.; Delaney, V.; Hong, J.H.; Daskalakis, P.; Markell, M.; Friedman, E.A.; Sommer, B.G. Racial differences in renal transplant outcome of insulin-dependent diabetic recipients in the cyclosporine era. ASAIO Trans. 1991, 37, M304–M305. [Google Scholar] [PubMed]
- Koyama, H.; Cecka, J.M.; Terasaki, P.I. Kidney transplants in black recipients. HLA matching and other factors affecting long-term graft survival. Transplantation 1994, 57, 1064–1068. [Google Scholar] [CrossRef]
- Smith, S.R.; Butterly, D.W. Declining influence of race on the outcome of living-donor renal transplantation. Am. J. Transpl. 2002, 2, 282–286. [Google Scholar] [CrossRef]
- Howard, R.J.; Thai, V.B.; Patton, P.R.; Hemming, A.W.; Reed, A.; Van Der Werf, W.J.; Fujita, S.; Karlix, J.L.; Scornik, J.C. Obesity does not portend a bad outcome for kidney transplant recipients. Transplantation 2002, 73, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Marks, W.H.; Florence, L.S.; Chapman, P.H.; Precht, A.F.; Perkinson, D.T. Morbid obesity is not a contraindication to kidney transplantation. Am. J. Surg. 2004, 187, 635–638. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Shah, G.; Leggat, J.; Hubbell, C.; Roman, A.; Kittur, D.; Narsipur, S. Impact of recipient obesity on living donor kidney transplant outcomes: A single-center experience. Transpl. Proc. 2007, 39, 1421–1423. [Google Scholar] [CrossRef]
- Erturk, T.; Berber, I.; Cakir, U. Effect of Obesity on Clinical Outcomes of Kidney Transplant Patients. Transpl. Proc. 2019, 51, 1093–1095. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Liu, Q.Z. Effect Analysis of 1-Year Posttransplant Body Mass Index on Chronic Allograft Nephropathy in Renal Recipients. Transplant. Proc. 2011, 43, 2592–2595. [Google Scholar] [CrossRef]
- Kwan, J.M.; Hajjiri, Z.; Metwally, A.; Finn, P.W.; Perkins, D.L. Effect of the Obesity Epidemic on Kidney Transplantation: Obesity Is Independent of Diabetes as a Risk Factor for Adverse Renal Transplant Outcomes. PLoS ONE 2016, 11, e0165712. [Google Scholar] [CrossRef]
- Hariharan, S.; Israni, A.K.; Danovitch, G. Long-Term Survival after Kidney Transplantation. N. Engl. J. Med. 2021, 385, 729–743. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Alrukhaimi, M.; Liu, Z.-H.; Zakharova, E.; Levin, A. What We Do and Do Not Know about Women and Kidney Diseases; Questions Unanswered and Answers Unquestioned: Reflection on World Kidney Day and International Women’s Day. Nephron 2018, 138, 249–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kayler, L.K.; Rasmussen, C.S.; Dykstra, D.M.; Ojo, A.O.; Port, F.K.; Wolfe, R.A.; Merion, R.M. Gender imbalance and outcomes in living donor renal transplantation in the United States. Am. J. Transpl. 2003, 3, 452–458. [Google Scholar] [CrossRef]
- Tan, J.C.; Wadia, P.P.; Coram, M.; Grumet, F.C.; Kambham, N.; Miller, K.; Pereira, S.; Vayntrub, T.; Miklos, D.B. H-Y antibody development associates with acute rejection in female patients with male kidney transplants. Transplantation 2008, 86, 75–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graňák, K.; Kováčiková, L.; Skálová, P.; Vnučák, M.; Miklušica, J.; Laca, .; Mokáň, M.; Dedinská, I. Kidney Transplantation and "Sex Mismatch": A 10-Year Single-Center Analysis. Ann. Transpl. 2020, 25, e921117. [Google Scholar] [CrossRef]
- Bellini, M.I.; Charalmpidis, S.; Brookes, P.; Hill, P.; Dor, F.J.M.F.; Papalois, V. Bilateral Nephrectomy for Adult Polycystic Kidney Disease Does Not Affect the Graft Function of Transplant Patients and Does Not Result in Sensitisation. Biomed Res. Int. 2019, 2019, 7423158. [Google Scholar] [CrossRef] [Green Version]
- Tan, J.C.; Kim, J.P.; Chertow, G.M.; Grumet, F.C. Donor–Recipient Sex Mismatch in Kidney Transplantation. Gend. Med. 2012, 9, 335–347. [Google Scholar] [CrossRef] [Green Version]
- Bairey Merz, C.N.; Dember, L.M.; Ingelfinger, J.R.; Vinson, A.; Neugarten, J.; Sandberg, K.L.; Sullivan, J.C.; Maric-Bilkan, C.; Rankin, T.L.; et al.; on behalf of the participants of the National Institute of Diabetes and Digestive and Kidney Diseases Workshop on “Sex and the Kidneys” Sex and the kidneys: Current understanding and research opportunities. Nat. Rev. Nephrol. 2019, 15, 776–783. [Google Scholar] [CrossRef]
- Taylor, D.M.; Bradley, J.A.; Bradley, C.; Draper, H.; Dudley, C.; Fogarty, D.; Fraser, S.D.; Johnson, R.; Leydon, G.M.; Metcalfe, W.; et al. Limited health literacy is associated with reduced access to kidney transplantation. Kidney Int. 2019, 95, 1244–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellini, M.I.; Charalampidis, S.; Stratigos, I.; Dor, F.; Papalois, V. The Effect of Donors’ Demographic Characteristics in Renal Function Post-Living Kidney Donation. Analysis of a UK Single Centre Cohort. J. Clin. Med. 2019, 8, 883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pruthi, R.; Robb, M.L.; Oniscu, G.C.; Tomson, C.; Bradley, A.; Forsythe, J.L.; Metcalfe, W.; Bradley, C.; Dudley, C.; Johnson, R.J.; et al. Inequity in Access to Transplantation in the United Kingdom. Clin. J. Am. Soc. Nephrol. 2020, 15, 830–842. [Google Scholar] [CrossRef]
- Ku, E.; McCulloch, C.E.; Roll, G.R.; Posselt, A.; Grimes, B.A.; Johansen, K.L. Bariatric surgery prior to transplantation and risk of early hospital re-admission, graft failure, or death following kidney transplantation. Am. J. Transpl. 2021, 21, 3750–3757. [Google Scholar] [CrossRef] [PubMed]






| Proteinuria | Male to Male | Male to Female | Female to Female | Female to Male | Outcomes Reported in the Paper |
|---|---|---|---|---|---|
| Oh et al. Protein excretion (mg/d), 24 h urine post-op. | MM (n = 65): 23.4 +/− 61.6 | MF (n = 34): 81.9 +/− 354.4 | FF (=29): 9.7 +/− 51.6 | FM (n = 67): 36.1 +/− 123.8 | Independent sample t-test: MM-FM (p = 0.461), MF-FF (p = 0.282); MM-MF (p = 0.198), FM-FF: (p = 0.273). |
| Yanishi et al. (mg/day). Recipient proteinuria at 1-year post-surgery. | Group 1(same gender) n = 6: 135.2 ± 98.1 | Group 2: (male donor to female recipient) (n = 8). 63.7 ± 28.7 | Group 1(same gender) n= 6: 135.2 ± 98.1 | Group 3: female donor to male recipient (n = 17): 205.5 ± 35.2 | ANOVA between the 3 groups found the lowest proteinuria to be in the Male to Female group (p < 0.01). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellini, M.I.; Nozdrin, M.; Pengel, L.; Knight, S.; Papalois, V. The Impact of Recipient Demographics on Outcomes from Living Donor Kidneys: Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 5556. https://doi.org/10.3390/jcm10235556
Bellini MI, Nozdrin M, Pengel L, Knight S, Papalois V. The Impact of Recipient Demographics on Outcomes from Living Donor Kidneys: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(23):5556. https://doi.org/10.3390/jcm10235556
Chicago/Turabian StyleBellini, Maria Irene, Mikhail Nozdrin, Liset Pengel, Simon Knight, and Vassilios Papalois. 2021. "The Impact of Recipient Demographics on Outcomes from Living Donor Kidneys: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 23: 5556. https://doi.org/10.3390/jcm10235556
APA StyleBellini, M. I., Nozdrin, M., Pengel, L., Knight, S., & Papalois, V. (2021). The Impact of Recipient Demographics on Outcomes from Living Donor Kidneys: Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 10(23), 5556. https://doi.org/10.3390/jcm10235556