
Effectiveness of Radial Extracorporeal Shockwave Therapy in Patients with Acute Low Back Pain—Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Schmidt, C.O.; Raspe, H.; Pfingsten, M.; Hasenbring, M.; Basler, H.D.; Eich, W.; Kohlmann, T. Back pain in the German adult population: Prevalence, severity, and sociodemographic correlates in a multiregional survey. Spine 2007, 32, 2005–2011. [Google Scholar] [CrossRef]
- Casser, H.-R.; Seddigh, S.; Rauschmann, M. Acute Lumbar Back Pain: Investigation, Differential Diagnosis, and Treatment. Dtsch. Arztebl. Int. 2016, 113, 223–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babatunde, O.O.; Jordan, J.L.; Van der Windt Danielle, A.; Hill, J.C.; Foster, N.E.; Protheroe, J. Effective treatment options for musculoskeletal pain in primary care: A systematic overview of current evidence. PLoS ONE 2017, 12, e0178621. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch Institut. Gesundheit in Deutschland. Gesundheitsberichterstattung des Bundes.: Gemeinsam Getragen von RKI und Destatis. Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GesInDtld/gesundheit_in_deutschland_2015.pdf?__blob=publicationFile (accessed on 23 November 2021).
- Bundesärztekammer (BÄK); Kassenärztliche Bundesvereinigung (KBV); Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften. Nationale VersorgungsLeitlinie Nicht-spezifischer Kreuzschmerz–Langfassung. Available online: https://www.awmf.org/uploads/tx_szleitlinien/nvl-007l_S3_Kreuzschmerz_2017-03.pdf (accessed on 23 November 2021).
- Wei, W.; Tang, H.-Y.; Li, Y.-Z.; Wang, T.-S. Effectiveness of extracorporeal shock wave for low back pain: A protocol of systematic review. Medicine 2019, 98, e14511. [Google Scholar] [CrossRef]
- Barker, K.L.; Elliott, C.J.; Sackley, C.M.; Fairbank, J.C.T. Treatment of chronic back pain by sensory discrimination training. A Phase I RCT of a novel device (FairMed) vs. TENS. BMC Musculoskelet. Disord. 2008, 9, 97. [Google Scholar] [CrossRef] [Green Version]
- Seco, J.; Kovacs, F.M.; Urrutia, G. The efficacy, safety, effectiveness, and cost-effectiveness of ultrasound and shock wave therapies for low back pain: A systematic review. Spine J. 2011, 11, 966–970. [Google Scholar] [CrossRef]
- Celik, A.; Altan, L.; Okmen, B.M. The Effects of Extracorporeal Shock Wave Therapy On Pain, Disability And Life Quality Of Chronic Low Back Pain Patients. Altern. Ther. Health Med. 2020, 26, 54–60. [Google Scholar] [PubMed]
- Notarnicola, A.; Maccagnano, G.; Gallone, M.F.; Mastromauro, L.; Rifino, F.; Pesce, V.; Covelli, I.; Moretti, B. Extracorporeal shockwave therapy versus exercise program in patients with low back pain: Short-term results of a randomised controlled trial. J. Biol. Regul. Homeost. Agents 2018, 32, 385–389. [Google Scholar]
- Chaussy, C.; Brendel, W.; Schmiedt, E. Extracorporeally induced destruction of kidney stones by shock waves. Lancet 1980, 2, 1265–1268. [Google Scholar] [CrossRef]
- Kertzman, P.; Császár, N.B.M.; Furia, J.P.; Schmitz, C. Radial extracorporeal shock wave therapy is efficient and safe in the treatment of fracture nonunions of superficial bones: A retrospective case series. J. Orthop. Surg. Res. 2017, 12, 164. [Google Scholar] [CrossRef] [Green Version]
- Speed, C. A systematic review of shockwave therapies in soft tissue conditions: Focusing on the evidence. Br. J. Sports Med. 2014, 48, 1538–1542. [Google Scholar] [CrossRef] [PubMed]
- Crupnik, J.; Silveti, S.; Wajnstein, N.; Rolon, A.; Vollhardt, A.; Stiller, P.; Schmitz, C. Is radial extracorporeal shock wave therapy combined with a specific rehabilitation program (rESWT + RP) more effective than sham-rESWT + RP for acute hamstring muscle complex injury type 3b in athletes? Study protocol for a prospective, randomized, double-blind, sham-controlled single centre trial. J. Orthop. Surg. Res. 2019, 14, 234. [Google Scholar] [PubMed]
- Torgerson, D.J.; Roberts, C. Understanding controlled trials. Randomisation methods: Concealment. BMJ 1999, 319, 375–376. [Google Scholar] [CrossRef]
- Siemonsma, P.C.; Walker, M.F. Practical guidelines for independent assessment in randomized controlled trials (RCTs) of rehabilitation. Clin. Rehabil. 1997, 11, 273–279. [Google Scholar] [CrossRef]
- Wheaton, L.; Pope, J. The minimally important difference for patient-reported outcomes in spondyloarthropathies including pain, fatigue, sleep, and Health Assessment Questionnaire. J. Rheumatol. 2010, 37, 816–822. [Google Scholar] [CrossRef]
- Lord, B.A.; Parsell, B. Measurement of pain in the prehospital setting using a visual analogue scale. Prehosp. Disaster. Med. 2003, 18, 353–358. [Google Scholar] [CrossRef]
- Calvert, M.; Blazeby, J.; Altman, D.G.; Revicki, D.A.; Moher, D.; Brundage, M.D. Reporting of patient-reported outcomes in randomized trials: The CONSORT PRO extension. JAMA 2013, 309, 814–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zambito Marsala, S.; Pistacchi, M.; Tocco, P.; Gioulis, M.; Fabris, F.; Brigo, F.; Tinazzi, M. Pain perception in major depressive disorder: A neurophysiological case-control study. J. Neurol. Sci. 2015, 357, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lee, D.; Park, J. Effects of extracorporeal shockwave therapy on patients with chronic low back pain and their dynamic balance ability. J. Phys. Ther. Sci. 2014, 26, 7–10. [Google Scholar] [CrossRef] [Green Version]
- Han, H.; Lee, D.; Lee, S.; Jeon, C.; Kim, T. The effects of extracorporeal shock wave therapy on pain, disability, and depression of chronic low back pain patients. J. Phys. Ther. Sci. 2015, 27, 397–399. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.-J. Extracorporeal shockwave therapy in musculoskeletal disorders. J. Orthop. Surg. Res. 2012, 7, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.-J. An overview of shock wave therapy in musculoskeletal disorders. Chang Gung Med. J. 2003, 26, 220–232. [Google Scholar] [PubMed]
- Saggini, R.; Di Stefano, A.; Saggini, A.; Bellomo, R.G. Clinical application of shock wave therapy in musculoskeletal disorders: Part I. J. Biol. Regul. Homeost. Agents 2015, 29, 533–545. [Google Scholar]
- Schmitz, C.; Császár, N.B.; Milz, S.; Schieker, M.; Maffulli, N.; Rompe, J.D.; Furia, J.P. Efficacy and safety of extracorporeal shock wave therapy for orthopedic conditions: A systematic review on studies listed in the PEDro database. Br. Med. Bull. 2015, 116, 115–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saggini, R.; Di Stefano, A.; Saggini, A.; Bellomo, R.G. Clinical application of shock wave therapy in musculoskeletal disorders: Part II related to myofascial and nerve apparatus. J. Biol. Regul. Homeost. Agents 2015, 29, 771–785. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
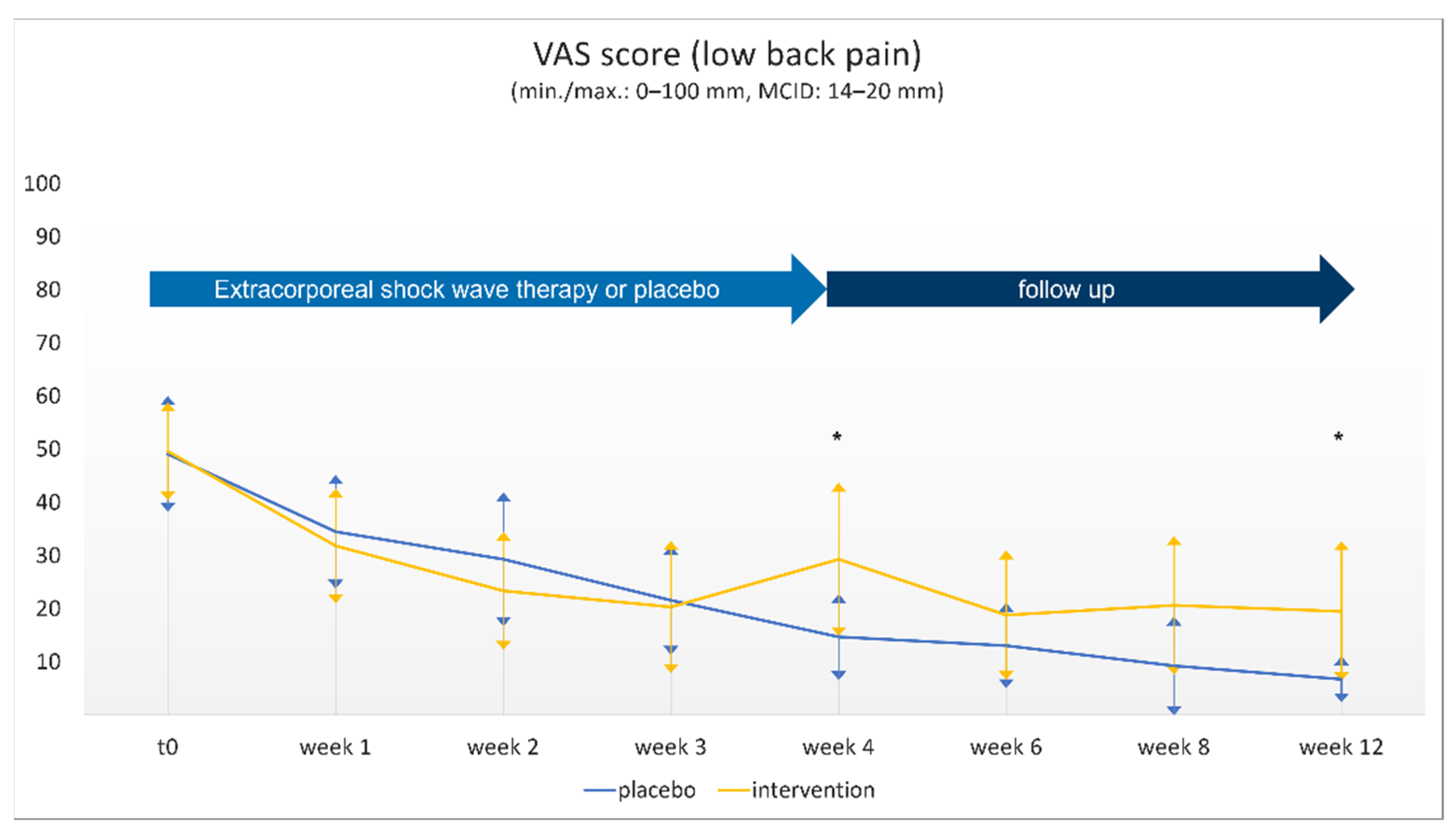
| Questionnaire | t0 | Week 1 | Week 2 | Week 3 | Week 4 | Week 6 | Week 8 | Week 12 |
|---|---|---|---|---|---|---|---|---|
| mean ± SD | ||||||||
| VAS-LBP | ||||||||
| placebo | 49.1 ± 21.81 | 34.5 ± 21.42 | 29.3 ± 25.22 | 21.6 ± 20.62 | 14.7 ± 16.25 | 13.1 ± 16.11 | 9.2 ± 18.66 | 6.7 ± 8.74 |
| intervention | 49.6 ± 18.47 | 31.8 ± 21.74 | 23.4 ± 22.26 | 20.3 ± 24.88 | 29.3 ± 28.90 | 18.8 ± 24.38 | 20.6 ± 26.14 | 19.5 ± 26.36 |
| p | 0.933 | 0.670 | 0.377 | 0.848 | * 0.029 | 0.322 | 0.079 | * 0.026 |
| EQ5D-3L | ||||||||
| mobility | ||||||||
| placebo | 1.4 ± 0.51 | 1.3 ± 0.44 | 1.2 ± 0.43 | 1.1 ± 0.33 | 1.0 ± 0.34 | 1.1 ± 0.27 | 1.0 ± 0.00 | 1.0 ± 0.00 |
| intervention | 1.4 ± 0.50 | 1.1 ± 0.37 | 1.1 ± 0.36 | 1.0 ± 0.28 | 1.2 ± 0.36 | 1.1 ± 0.30 | 1.1 ± 0.20 | 1.1 ± 0.20 |
| p | 1.000 | 0.088 | 0.115 | 0.348 | 0.248 | 0.646 | 0.163 | 0.146 |
| self care | ||||||||
| placebo | 1.1 ± 0.28 | 1.0 ± 0.20 | 1.1 ± 0.27 | 1.0 ± 0.00 | 1.0 ± 0.20 | 1.0 ± 0.00 | 1.0 ± 0.00 | 1.0 ± 0.00 |
| intervention | 1.1 ± 0.28 | 1.0 ± 0.19 | 1.0 ± 0.00 | 1.0 ± 0.00 | 1.0 ± 0.00 | 1.0 ± 0.00 | 1.0 ± 0.00 | 1.0 ± 0.00 |
| p | 1.000 | 0.934 | 0.147 | - | 0.322 | - | - | - |
| activity | ||||||||
| placebo | 1.6 ± 0.51 | 1.3 ± 0.47 | 1.4 ± 0.57 | 1.2 ± 0.37 | 1.0 ± 0.20 | 1.1 ± 0.33 | 1.0 ± 0.20 | 1.0 ± 0.20 |
| intervention | 1.5 ± 0.51 | 1.2 ± 0.40 | 1.1 ± 0.32 | 1.1 ± 0.29 | 1.1 ± 0.27 | 1.1 ± 0.33 | 1.2 ± 0.37 | 1.2 ± 0.41 |
| p | 0.580 | 0.335 | * 0.035 | 0.455 | 0.561 | 1.000 | 0.175 | 0.075 |
| pain | ||||||||
| placebo | 2.0 ± 0.35 | 1.9 ± 0.46 | 1.7 ± 0.55 | 1.4 ± 0.51 | 1.4 ± 0.50 | 1.3 ± 0.49 | 1.1 ± 0.33 | 1.2 ± 0.44 |
| intervention | 2.0 ± 0.32 | 1.8 ± 0.44 | 1.6 ± 0.53 | 1.3 ± 0.49 | 1.5 ± 0.50 | 1.4 ± 0.49 | 1.5 ± 0.50 | 1.5 ± 0.48 |
| p | 0.662 | 0.465 | 0.350 | 0.454 | 0.412 | 0.779 | * 0.014 | 0.113 |
| anxiety | ||||||||
| placebo | 1.0 ± 0.20 | 1.0 ± 0.00 | 1.0 ± 0.00 | 1.0 ± 0.00 | 1.0 ± 0.20 | 1.0 ± 0.00 | 1.0 ± 0.00 | 1.0 ± 0.00 |
| intervention | 1.1 ± 0.33 | 1.0 ± 0.19 | 1.0 ± 0.19 | 1.0 ± 0.00 | 1.0 ± 0.20 | 1.0 ± 0.00 | 1.0 ± 0.20 | 1.0 ± 0.20 |
| p | 0.307 | 0.361 | 0.331 | - | 0.163 | - | 0.332 | 0.312 |
| EQ-VAS | ||||||||
| placebo | 67.4 ± 22.45 | 71.6 ± 20.99 | 75.3 ± 22.21 | 79.5 ± 21.61 | 78.8 ± 21.37 | 87.2 ± 13.03 | 91.8 ± 8.32 | 90.2 ± 14.25 |
| intervention | 69.8 ± 15.72 | 79.1 ± 12.18 | 83.3 ± 13.78 | 83.9 ± 20.30 | 83.7 ± 16.51 | 86.5 ± 16.50 | 84.8 ± 17.87 | 85.4 ± 18.96 |
| p | 0.669 | 0.122 | 0.120 | 0.471 | 0.368 | 0.867 | 0.081 | 0.318 |
| ODI | ||||||||
| placebo | 27.3 ± 10.13 | 16.7 ± 10.12 | 13.8 ± 14.18 | 10.2 ± 13.28 | 7.0 ± 8.32 | 6.3 ± 9.01 | 3.8 ± 6.51 | 3.2 ± 5.66 |
| intervention | 27.3 ± 10.91 | 14.9 ± 7.05 | 8.9 ± 6.11 | 5.9 ± 6.09 | 7.0 ± 8.07 | 4.3 ± 4.89 | 6.5 ± 8.42 | 6.1 ± 7.51 |
| p | 0.987 | 0.453 | 0.108 | 0.139 | 0.987 | 0.315 | 0.191 | 0.127 |
| RDQ | ||||||||
| placebo | 7.9 ± 4.14 | 6.0 ± 4.67 | 5.1 ± 4.92 | 3.2 ± 3.78 | 2.0 ± 2.49 | 1.7 ± 2.28 | 1.0 ± 1.27 | 0.8 ± 0.80 |
| intervention | 7.0 ± 4.17 | 3.6 ± 2.33 | 2.9 ± 2.41 | 1.9 ± 2.35 | 2.0 ± 2.29 | 1.7 ± 1.69 | 2.1 ± 2.79 | 2.0 ± 3.31 |
| p | 0.482 | * 0.019 | * 0.041 | 0.138 | 1 | 0.945 | 0.065 | 0.107 |
| BDI-II | ||||||||
| placebo | 5.4 ± 5.70 | 3.9 ± 4.59 | 4.0 ± 5.24 | 2.4 ± 4.36 | 2.0 ± 3.48 | 1.7 ± 3.19 | 1.2 ± 2.87 | 1.4 ± 3.01 |
| intervention | 5.2 ± 4.72 | 3.7 ± 4.11 | 2.3 ± 3.46 | 1.4 ± 3.45 | 1.8 ± 3.63 | 0.9 ± 2.14 | 1.4 ± 3.17 | 2.0 ± 5.16 |
| p | 0.874 | 0.856 | 0.177 | 0.345 | 0.85 | 0.263 | 0.797 | 0.615 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lange, T.; Deventer, N.; Gosheger, G.; Lampe, L.P.; Bockholt, S.; Schulze Boevingloh, A.; Schulte, T.L. Effectiveness of Radial Extracorporeal Shockwave Therapy in Patients with Acute Low Back Pain—Randomized Controlled Trial. J. Clin. Med. 2021, 10, 5569. https://doi.org/10.3390/jcm10235569
Lange T, Deventer N, Gosheger G, Lampe LP, Bockholt S, Schulze Boevingloh A, Schulte TL. Effectiveness of Radial Extracorporeal Shockwave Therapy in Patients with Acute Low Back Pain—Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(23):5569. https://doi.org/10.3390/jcm10235569
Chicago/Turabian StyleLange, Tobias, Niklas Deventer, Georg Gosheger, Lukas P Lampe, Sebastian Bockholt, Albert Schulze Boevingloh, and Tobias L Schulte. 2021. "Effectiveness of Radial Extracorporeal Shockwave Therapy in Patients with Acute Low Back Pain—Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 23: 5569. https://doi.org/10.3390/jcm10235569
APA StyleLange, T., Deventer, N., Gosheger, G., Lampe, L. P., Bockholt, S., Schulze Boevingloh, A., & Schulte, T. L. (2021). Effectiveness of Radial Extracorporeal Shockwave Therapy in Patients with Acute Low Back Pain—Randomized Controlled Trial. Journal of Clinical Medicine, 10(23), 5569. https://doi.org/10.3390/jcm10235569