
Dual Disorders in the Consultation Liaison Addiction Service: Gender Perspective and Quality of Life


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
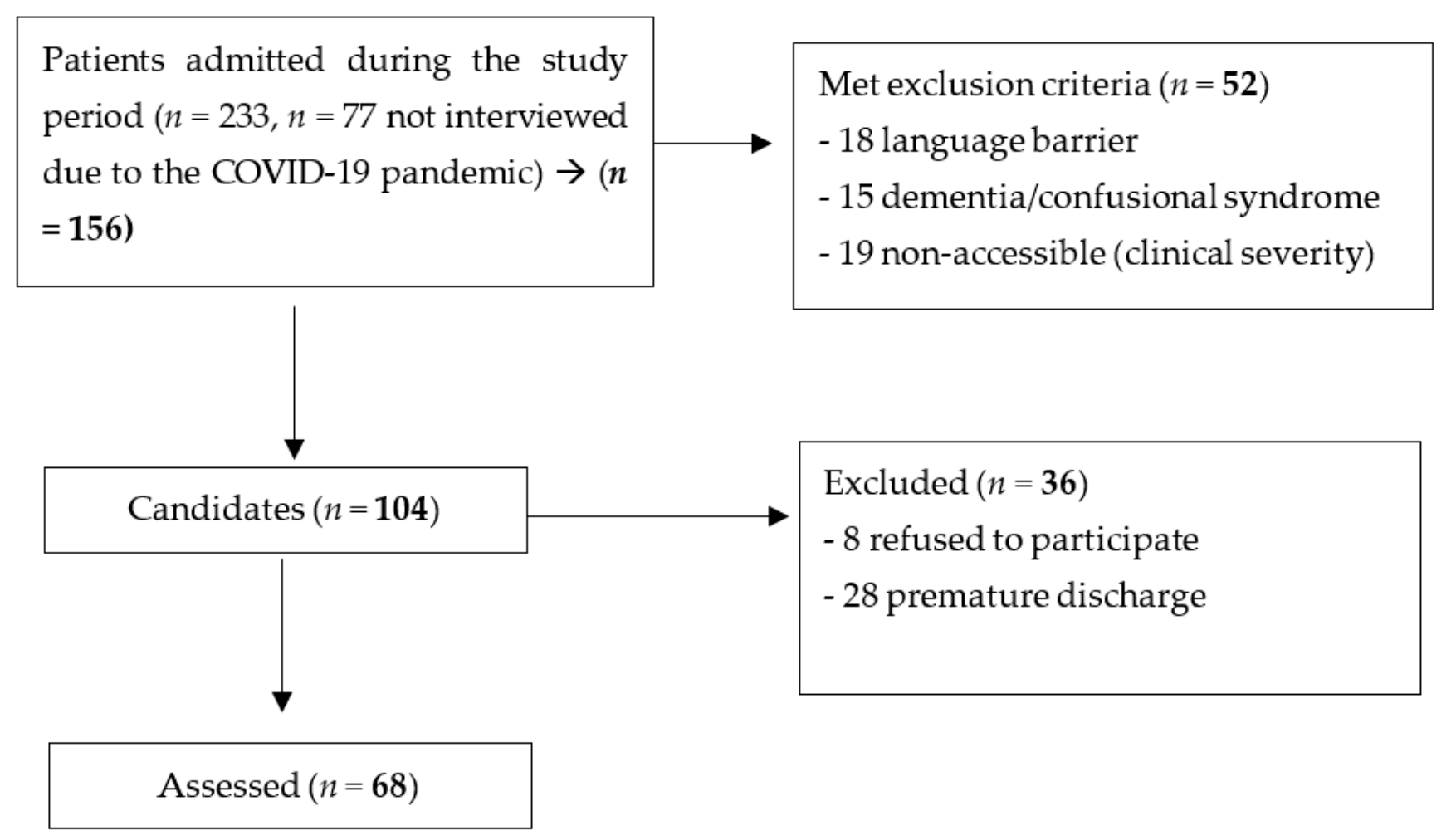
2.1. Participants
2.2. Inclusion and Exclusion Criteria
2.3. Assessment Instruments
2.4. Procedure
2.5. Analysis of Data
2.6. Ethics
3. Results
3.1. Sociodemographic Characteristics
3.2. Clinical Characteristics
3.3. Dual Disorder Assessment
3.4. Dual Disorder and Quality of Life
3.5. Dual Disorder and Severity of Addiction
3.6. Sociodemographic and Clinical Characteristics of Patients Attended during Lockdown Period
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Lexicon of Alcohol and Drug Terms; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Durvasula, R.; Miller, T.R. Substance abuse treatment in persons with HIV/AIDS: Challenges in managing triple diagnosis. IJBM 2014, 40, 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adan, A.; Torrens, M. Special issue: Diagnosis and management of addiction and other mental disorders (Dual Disorders). J. Clin. Med. 2021, 10, 1307. [Google Scholar] [CrossRef] [PubMed]
- Torres, G.N.; Cristóbal, J.P.; Martín, J.R. Dual Diagnosis: A Theoretical Approximation from Review of Literature. J. Drug Abuse 2019, 5, 4. [Google Scholar]
- Volkow, N.D.; Torrens, M.; Poznyak, V.; Sáenz, E.; Busse, A.; Kashino, W.; Krupchanka, D.; Kestel, D.; Campello, G.; Gerra, G. Managing dual disorders: A statement by the Informal Scientific Network, UN Commission on Narcotic Drugs. World Psychiatry 2020, 19, 396–397. [Google Scholar] [CrossRef]
- Torrens, M.; Mestre-Pintó, J.; Montanari, L.; Vicente, J.; Domingo-Salvany, A. Patología dual: Una perspectiva europea. Adicciones 2017, 29, 3–5. [Google Scholar] [CrossRef] [Green Version]
- Chahua, M.; Sanchez-Niubo, A.; Torrens, M.; Sordo, L.; Bravo, M.; Brugal, M.; Domingo-Salvany, A. Quality of life in a community sample of young cocaine and/or heroin users: The role of mental disorders. Qual. Life Res. 2015, 24, 2129–2137. [Google Scholar] [CrossRef] [Green Version]
- Lozano, O.M.; Rojas, A.J.; Fernandez, F. Psychiatric comorbidity and severity of dependence on substance users: How it impacts on their health-related quality of life? J. Ment. Health 2017, 26, 119–126. [Google Scholar] [CrossRef]
- Abdel-Baki, A.; Ouellet-Plamondon, C.; Salvat, É.; Grar, K.; Potvin, S. Symptomatic and funcional outcomes of substance use disorder persistence 2 years after admission to a first-episode psychosis program. Psychiatry Res. 2017, 247, 113–119. [Google Scholar] [CrossRef]
- Adan, A.; Marquez-Arrico, J.; Gilchrist, G. Comparison of health-related quality of life among men with different co-existing severe mental disorders in treatment for substance use. Health Qual. Life Outcomes 2017, 15, 209. [Google Scholar] [CrossRef] [Green Version]
- Torrens, M.; Mestre-Pintó, J.J.; Domingo-Salvany, A. Comorbidity of Substance Use and Mental Disorders in Europe; EMCDDA, Publications Office of the European Union: Luxembourg, 2015; ISBN 978-92-9168-834-0. [Google Scholar]
- Mancheño, J.J.; Navas, S.; Gutiérrez, M.L.; Rosa, A.; Cáceres, M.P.; Lozano, O.M. Analysis of the profiles of patients with dual pathology attending addiction centers, mental health centers, and a coordinated service. Ann. Psychol. 2019, 35, 233–241. [Google Scholar]
- García-Carretero, M.A.; Novalbos-Ruiz, J.P.; Robles-Martínez, M.; Jordán-Quintero, M.A.; O’Ferrall-González, C. Psychopathological profile and prevalence of dual pathology on patients with alcoholic dependence undergoing outpatient treatment. Actas Esp. Psiquiatr. 2017, 45, 1–11. [Google Scholar]
- Fonseca, F.; Robles-Martínez, M.; Tirado-Muñoz, J.; Alías-Ferri, M.; Mestre-Pintó, J.I.; Coratu, A.M.; Torrens, M. A gender perspective of addictive disorders. Curr. Addict. Rep. 2021, 8, 89–99. [Google Scholar] [CrossRef]
- McHugh, R.K.; Votaw, V.R.; Sugarman, D.E.; Greenfield, S.F. Sex and gender differences in substance use disorders. Psychol. Rev. 2018, 66, 12–23. [Google Scholar] [CrossRef]
- Frem, Y.; Torrens, M.; Domingo-Salvany, A.; Gilchrist, G. Gender differences in lifetime psychiatric and substance use disorders among people who use substances in Barcelona, Spain. Adv. Dual Diagn. 2017, 10, 45–56. [Google Scholar] [CrossRef] [Green Version]
- Gilchrist, G.; Blánquez, A.; Torrens, M. Psychiatric, Behavioural and Social Risk Factors for HIV Infection among Female Drug Users. AIDS Behav. 2011, 10, 3–10. [Google Scholar] [CrossRef]
- Tirado-Muñoz, J.; Gilchrist, G.; Fischer, G.; Taylor, A.; Moskalewicz, J.; Giammarchi, C.; Köchl, B.; Munro, A.; Dąbrowska, K.; Shaw, A.; et al. Psychiatric comorbidity and intimate partner violence among women who inject drugs in Europe: A cross-sectional study. Arch. Womens Ment. Health 2017, 21, 259–269. [Google Scholar] [CrossRef]
- Caldentey, C.; Tirado-Muñoz, J.; Ferrer, T.; Fonseca, F.; Rossi, P.; Mestre-Pintó, J.I.; Torrens, M. Violencia de género en mujeres con consumo de sustancias ingresadas en el hospital general: Cribado y prevalencia. Adicciones 2017, 29, 172–179. [Google Scholar] [CrossRef] [Green Version]
- Weaver, T.L.; Gilbert, L.; El-Bassel, N.; Resnick, H.S.; Noursi, S. Identifying and intervening with substance-using women exposed to intimate partner violence: Phenomenology, comorbidities, and integrated approaches within primary care and other agency Settings. J. Womens Health 2015, 24, 51–56. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 2013. Available online: https://doi.org/10.1176/appi.books.9780890425596 (accessed on 25 November 2021).
- Ojeda, N.; Del Pino, R.; Ibarretxe-Bilbao, N.; Schretlen, D.J.; Pena, J. Test de evaluacion cognitiva de Montreal: Normalizacion y estandarizacion de la prueba en poblacion española [Montreal Cognitive Assessment Test: Normalization and standardization for Spanish population]. Rev Neurol. 2016, 63, 488–496. [Google Scholar]
- Mestre-Pintó, J.I.; Domingo-Salvany, A.; Martín-Santos, R.; Torrens, M.; PsyCoBarcelona Group. Dual Diagnosis Screening Interview to Identify Psychiatric Comorbidity in Substance Users: Development and Validation of a Brief Instrument. Eur. Addict. Res. 2014, 20, 41–48. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Use of Well-Being Measures in Primary Health Care/ TheDepCare Project. 1998. Available online: https://www.euro.who.int/__data/assets/pdf_file/0016/130750/E60246.pdf (accessed on 25 November 2021).
- Gossop, M.; Darke, S.; Griffiths, P.; Hando, J.; Powis, B.; Hall, W.; Strang, J. The Severity of Dependence Scale (SDS): Psychometric properties of the SDS in English and Australian samples of heroin, cocaine and amphetamine users. Addiction 1995, 90, 607–614. [Google Scholar] [CrossRef] [PubMed]
- González-Saiz, F.; de Las Cuevas, C.; Barrio, G.; Domingo-Salvany, A. Versión española consensuada de la Severity of Dependence Scale (SDS) [Spanish version of the Severity of Dependence Scale (SDS)]. Med. Clin. 2008, 131, 797–798. [Google Scholar] [CrossRef]
- Walker, J.; Burke, K.; Wanat, M.; Fisher, R.; Fielding, J.; Mulick, A.; Puntis, S.; Sharpe, J.; Esposti, M.D.; Harriss, E.; et al. The prevalence of depression in general hospital inpatients: A systematic review and meta-analysis of interview-based studies. Psychol. Med. 2018, 48, 2285–2298. [Google Scholar] [CrossRef] [PubMed]
- Campuzano-Cortina, C.; Feijoó-Fonnegra, L.M.; Manzur-Pineda, K.; Palacio-Muñoz, M.; Rendón-Fonnegra, J.; Montoya, L.; Berrouet, M.C.; Restrepo, D. Comorbidity between depressive symptoms and substance use in-patients hospitalized for non-psychiatric diseases. Rev. Colomb. Psiquiatr. (Engl. Ed.) 2021, 50, 130–137. [Google Scholar] [CrossRef]
- Farré, A.; Tirado-Muñoz, J.; Torrens, M. Dual Depression: A Sex Perspective. Addict. Disord. Their Treat. 2017, 16, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Laudet, A.B.; Becker, J.B.; White, W.L. Don’t wanna go through that madness no more: Quality of life satisfaction as predictor of sustained remission from illicit drug misuse. Subst. Use Misuse 2009, 44, 227–252. [Google Scholar] [CrossRef]
- McHugh, R.K.; Wigderson, S.; Greenfield, S.F. Epidemiology of substance use in reproductive-age women. Obstet. Gynecol. Clin. N. Am. 2014, 41, 177–189. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Women n = 13 | Men n = 55 | Participants n = 68 | ||
|---|---|---|---|---|
| n (%) | n (%) | n (%) | p | |
| Age (mean ± SD) years | 47.92 ± 10.15 | 51.71 ± 11.97 | 50.99 ± 11.67 | 0.310 |
| Civil status | 0.433 | |||
| Single | 5 (41.7) | 23 (43.4) | 28 (41.1) | |
| Married/partner | 3 (25) | 13 (24.5) | 16 (23.5) | |
| Others | 5 (38.4) | 19 (34.5) | 24 (35.2) | |
| Origin | 0.217 | |||
| National | 11 (84.6) | 37 (67.3) | 48 (70.6) | |
| Employment situation | 0.740 | |||
| Employed | 1 (8.3) | 7 (12.7) | 8 (11.7) | |
| Unemployed | 8 (66.7) | 25 (45.4) | 33 (48.5) | |
| Retired | 4 (25) | 11 (20) | 15 (22.1) | |
| Others | 0 | 12 (21.8) | 12 (17.6) | |
| Living with | 0.336 | |||
| Nobody | 0 | 13 (23.6) | 13 (19.7) | |
| Family | 9 (69.2) | 21 (38.1) | 30 (45.5) | |
| Homeless | 3 (23.1) | 13 (23.6) | 16 (24.2) | |
| Others | 1 (7.7) | 8 (15.5) | 9 (13.2) | |
| Criminal records | 0.559 | |||
| No | 8 (72.7) | 35 (67.3) | 43 (63.2) |
| Women (n = 13) | Men (n = 55) | Participants (n = 68) | |||
|---|---|---|---|---|---|
| n% | n% | n% | p | ||
| Main drug: | Opiates | 5 (38.5) | 21 (38.2) | 26 (38.2) | 0.896 |
| Alcohol | 6 (46.2) | 26 (47.3) | 32 (47.1) | ||
| Cocaine | 2 (15.4) | 5 (9.1) | 7 (10.3) | ||
| Amphetamines | 0 | 2 (3.6) | 2 (3) | ||
| Tobacco | 0 | 1 (1.8) | 1 (1.5) | ||
| Commencement age of main drug (± SD), years | 23 ± 8.26 | 17.83 ± 5.91 | 18.71 ± 6.59 | 0.018 | |
| Total abstinence time ( ± SD), months | 18.73 ± 24.50 | 25.31 ± 37.28 | 24.15 ± 35.27 | 0.903 | |
| Time since last consumption of the main drug (± SD), months | 6.08 ± 20.76 | 3.98 ± 14.30 | 4.37 ± 15.54 | 0.850 | |
| Patients previously involved in an addiction treatment | 10 (76.9) | 30 (55.6) | 40 (58.9) | 0.159 | |
| Age at first addiction treatment (± SD) years | 35.75 ± 13.26 | 34.39 ± 14.9 | 34.74 ± 14.29 | 0.572 | |
| HIV antibodies positive | 3 (23.1) | 10 (18.2) | 13 (19.1) | 0.702 | |
| Ab HCV serology positive | 4 (30.8) | 16 (29.1) | 20 (29.4) | 0.954 | |
| Ab core HBV serology positive | 4 (30.8) | 10 (18.2) | 14 (20.6) | 0.601 | |
| Ag surface HBV positive | 0 | 2 (3.6) | 2 (2.9) | 0.728 | |
| Chronic liver disease | 5 (38.5) | 19 (34.5) | 24 (35.3) | 0.909 | |
| Women n = 13 | Men n = 55 | Participants n = 68 | ||
|---|---|---|---|---|
| Psychiatric Diagnoses | n (%) | n (%) | n (%) | p |
| Dual Disorder | 7 (53.8) | 18 (32.7) | 25 (36.8) | 0.156 |
| Panic | 6 (46.2) | 7 (12.7) | 13 (19.1) | 0.019 |
| Generalized anxiety | 5 (38.5) | 6 (10.9) | 11 (16.2) | 0.049 |
| Simple phobia | 3 (23.1) | 3 (5.5) | 6 (8.8) | 0.104 |
| Social phobia | 1 (7.7) | 4 (7.3) | 5 (7.4) | 0.958 |
| Agoraphobia | 1 (7.7) | 2 (3.6) | 3 (4.4) | 0.522 |
| Dysthymia | 3 (23.1) | 4 (7.3) | 7 (10.3) | 0.092 |
| Depression | 6 (46.2) | 17 (30.9) | 23 (33.8) | 0.296 |
| Mania | 3 (23.1) | 8 (14.5) | 11 (16.2) | 0.174 |
| Psychosis | 4 (30.8) | 9 (16.4) | 13 (19.1) | 0.445 |
| ADHD | 3 (23.1) | 6 (10.9) | 9 (13.2) | 0.479 |
| PTSD | 1 (7.7) | 8 (14.5) | 9 (13.2) | 0.512 |
| DD | Women (n = 13) | Men (n = 55) | Total (n = 68) | p | |
|---|---|---|---|---|---|
| WHO ( ± SD) | No | 62 ± 23.83 | 52.32 ± 30.9 | 53.67 ± 30.03 | 0.404 |
| Yes | 21.71 ± 21.52 | 50 ± 31.02 | 42.08 ± 31.0 | 0.020 | |
| SDS ( ± SD) | No | 4.5 ± 3.27 | 6.92 ± 4.14 | 6.58 ± 4.08 | 0.146 |
| Yes | 10.14 ± 3.72 | 7.39 ± 4.65 | 8.16 ± 4.52 | 0.145 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrer-Farré, T.; Dinamarca, F.; Mestre-Pintó, J.I.; Fonseca, F.; Torrens, M. Dual Disorders in the Consultation Liaison Addiction Service: Gender Perspective and Quality of Life. J. Clin. Med. 2021, 10, 5572. https://doi.org/10.3390/jcm10235572
Ferrer-Farré T, Dinamarca F, Mestre-Pintó JI, Fonseca F, Torrens M. Dual Disorders in the Consultation Liaison Addiction Service: Gender Perspective and Quality of Life. Journal of Clinical Medicine. 2021; 10(23):5572. https://doi.org/10.3390/jcm10235572
Chicago/Turabian StyleFerrer-Farré, Teresa, Fernando Dinamarca, Joan Ignasi Mestre-Pintó, Francina Fonseca, and Marta Torrens. 2021. "Dual Disorders in the Consultation Liaison Addiction Service: Gender Perspective and Quality of Life" Journal of Clinical Medicine 10, no. 23: 5572. https://doi.org/10.3390/jcm10235572
APA StyleFerrer-Farré, T., Dinamarca, F., Mestre-Pintó, J. I., Fonseca, F., & Torrens, M. (2021). Dual Disorders in the Consultation Liaison Addiction Service: Gender Perspective and Quality of Life. Journal of Clinical Medicine, 10(23), 5572. https://doi.org/10.3390/jcm10235572