
Self-Collected Samples to Detect SARS-CoV-2: Direct Comparison of Saliva, Tongue Swab, Nasal Swab, Chewed Cotton Pads and Gargle Lavage

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment of Study Participants
2.2. Collection of Samples and Questionnaire
2.3. RT-PCR Analysis of Self-Collected Specimens
2.4. Mutation Screening of Self-Collected Specimens
2.5. Statistical Analysis
3. Results
3.1. Characterization of the Study Participants and Symptomology
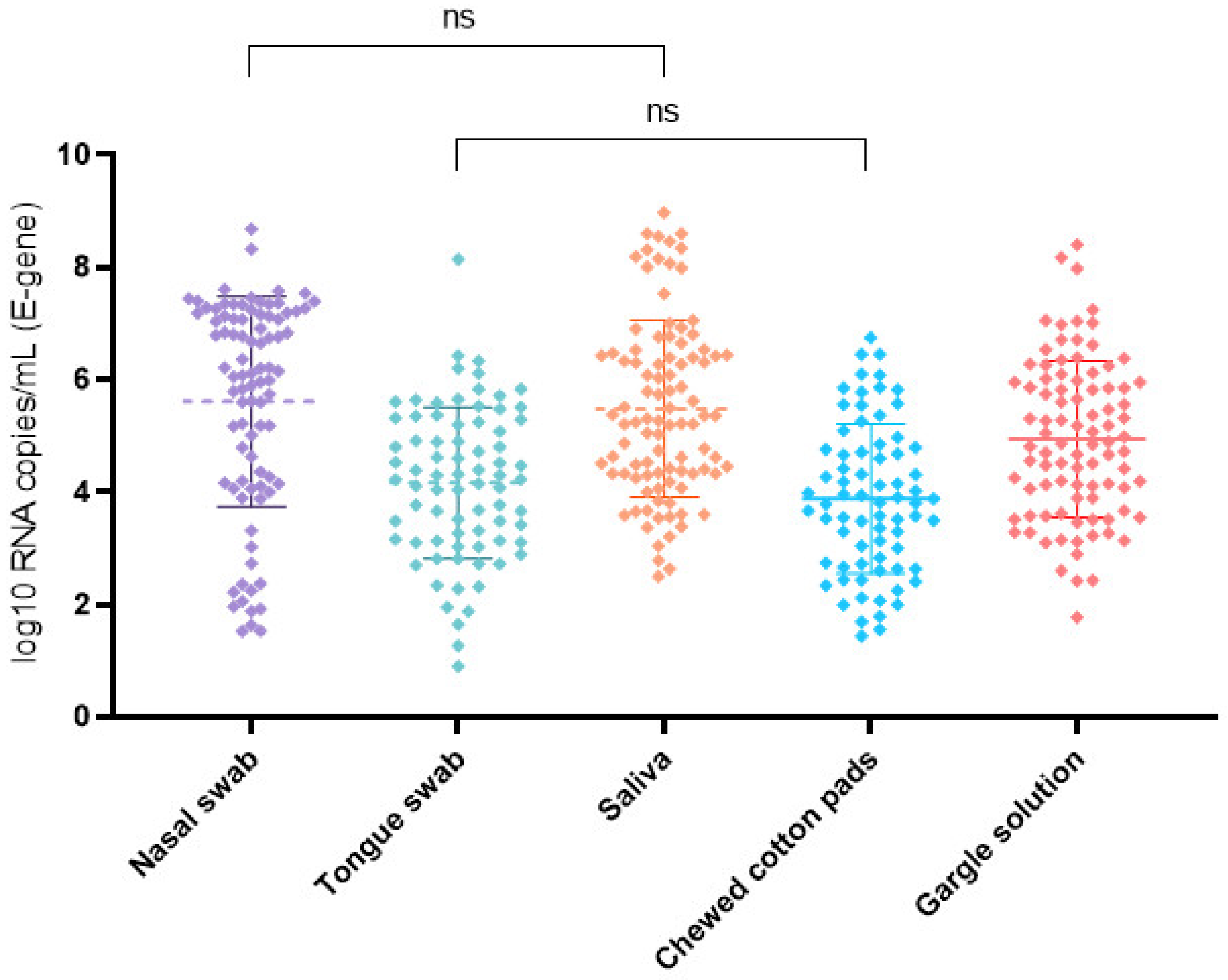
3.2. Specimen Sensitivity and Virus Concentration
3.3. Prevalence of the SARS-CoV-2 Variant Alpha and Mean Virus Concentration
3.4. Correlation of Symptoms and Testing Sensitivity of the Self-Collected Samples
3.5. Symptom Onset and Virus Concentration
3.6. Subjective Difficulty in Collecting the Samples
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rotondo, J.C.; Martini, F.; Maritati, M.; Mazziotta, C.; Mauro, G.D.; Lanzillotti, C.; Barp, N.; Gallerani, A.; Tognon, M.; Contini, C. SARS-CoV-2 Infection: New Molecular, Phylogenetic, and Pathogenetic Insights. Efficacy of Current Vaccines and the Potential Risk of Variants. Viruses 2021, 13, 1687. [Google Scholar] [CrossRef]
- Falzone, L.; Musso, N.; Gattuso, G.; Bongiorno, D.; Palermo, C.I.; Scalia, G.; Libra, M.; Stefani, S. Sensitivity Assessment of Droplet Digital PCR for SARS-CoV-2 Detection. Int. J. Mol. Med. 2020, 46, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Feng, J.; Zhang, Q.; Guo, D.; Zhang, L.; Suo, T.; Hu, W.; Guo, M.; Wang, X.; Huang, Z.; et al. Analytical Comparisons of SARS-COV-2 Detection by QRT-PCR and DdPCR with Multiple Primer/Probe Sets. Emerg. Microbes. Infec. 2020, 9, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.R.M.; Duval, A.; Pouwels, K.B.; Guillemot, D.; Fernandes, J.; Huynh, B.-T.; Temime, L.; Opatowski, L.; On behalf of the AP-HP/Universities/Inserm COVID-19 Research Collaboration. Optimizing COVID-19 Surveillance in Long-Term Care Facilities: A Modelling Study. BMC Med. 2020, 18, 386. [Google Scholar] [CrossRef] [PubMed]
- Team, E.P.H.E.; Danis, K.; Fonteneau, L.; Georges, S.; Daniau, C.; Bernard-Stoecklin, S.; Domegan, L.; O’Donnell, J.; Hauge, S.H.; Dequeker, S.; et al. High Impact of COVID-19 in Long-Term Care Facilities, Suggestion for Monitoring in the EU/EEA, May 2020. Eurosurveillance 2020, 25, 2000956. [Google Scholar] [CrossRef]
- Comber, L.; Walsh, K.A.; Jordan, K.; O’Brien, K.K.; Clyne, B.; Teljeur, C.; Drummond, L.; Carty, P.G.; Gascun, C.F.D.; Smith, S.M.; et al. Alternative Clinical Specimens for the Detection of SARS-CoV-2: A Rapid Review. Rev. Med. Virol. 2021, 31, e2185. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, Y.; Terada, J.; Kimura, M.; Moriya, A.; Motohashi, A.; Izumi, S.; Kawajiri, K.; Hakkaku, K.; Morishita, M.; Saito, S.; et al. Diagnostic Accuracy of Nasopharyngeal Swab, Nasal Swab and Saliva Swab Samples for the Detection of SARS-CoV-2 Using RT-PCR. Infect. Dis. 2021, 53, 1–9. [Google Scholar] [CrossRef]
- Saito, M.; Adachi, E.; Yamayoshi, S.; Koga, M.; Iwatsuki-Horimoto, K.; Kawaoka, Y.; Yotsuyanagi, H. Gargle Lavage as a Safe and Sensitive Alternative to Swab Samples to Diagnose COVID-19: A Case Report in Japan. Clin. Infect. Dis. 2020, 71, 893–894. [Google Scholar] [CrossRef] [Green Version]
- Carrouel, F.; Valette, M.; Perrier, H.; Bouscambert-Duchamp, M.; Dussart, C.; Tramini, P.; Bourgeois, D. Performance of Self-Collected Saliva Testing Compared with Nasopharyngeal Swab Testing for the Detection of SARS-CoV-2. Viruses 2021, 13, 895. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.W.; Yip, C.C.Y.; Lai, C.Y.W.; Wong, C.K.H.; Ho, D.T.Y.; Pang, P.K.P.; Ng, A.C.K.; Leung, K.-H.; Poon, R.W.S.; Chan, K.-H.; et al. Saliva as a Diagnostic Specimen for Testing Respiratory Virus by a Point-of-Care Molecular Assay: A Diagnostic Validity Study. Clin. Microbiol. Infec. 2019, 25, 372–378. [Google Scholar] [CrossRef] [Green Version]
- Wyllie, A.L.; Fournier, J.; Casanovas-Massana, A.; Campbell, M.; Tokuyama, M.; Vijayakumar, P.; Warren, J.L.; Geng, B.; Muenker, M.C.; Moore, A.J.; et al. Saliva or Nasopharyngeal Swab Specimens for Detection of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 1283–1286. [Google Scholar] [CrossRef] [PubMed]
- Zander, J.; Scholtes, S.; Ottinger, M.; Kremer, M.; Kharazi, A.; Stadler, V.; Bickmann, J.; Zeleny, C.; Kuiper, J.W.P.; Hauck, C.R. Self-Collected Gargle Lavage Allows Reliable Detection of SARS-CoV-2 in an Outpatient Setting. Microbiol. Spectr. 2021, 9, e00361-21. [Google Scholar] [CrossRef]
- Trobajo-Sanmartín, C.; Adelantado, M.; Navascués, A.; Guembe, M.J.; Rodrigo-Rincón, I.; Castilla, J.; Ezpeleta, C. Self-Collection of Saliva Specimens as a Suitable Alternative to Nasopharyngeal Swabs for the Diagnosis of SARS-CoV-2 by RT-QPCR. J. Clin. Med. 2021, 10, 299. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.-P.; Jennings, R.; Hart, B.; Cangelosi, G.A.; Wood, R.C.; Wehber, K.; Verma, P.; Vojta, D.; Berke, E.M. Swabs Collected by Patients or Health Care Workers for SARS-CoV-2 Testing. N. Engl. J. Med. 2020, 383, 494–496. [Google Scholar] [CrossRef]
- LeBlanc, J.J.; Pettipas, J.; Quinzio, M.D.; Hatchette, T.F.; Patriquin, G. Reliable Detection of SARS-CoV-2 with Patient-Collected Swabs and Saline Gargles: A Three-Headed Comparison on Multiple Molecular Platforms. J. Virol. Methods 2021, 295, 114184. [Google Scholar] [CrossRef] [PubMed]
- Braz-Silva, P.H.; Mamana, A.C.; Romano, C.M.; Felix, A.C.; de Paula, A.V.; Fereira, N.E.; Buss, L.F.; Tozetto-Mendoza, T.R.; Caixeta, R.A.V.; Leal, F.E.; et al. Performance of At-Home Self-Collected Saliva and Nasal-Oropharyngeal Swabs in the Surveillance of COVID-19. J. Oral. Microbiol. 2020, 13, 1858002. [Google Scholar] [CrossRef] [PubMed]
- Visseaux, B.; Hingrat, Q.L.; Collin, G.; Ferré, V.; Storto, A.; Ichou, H.; Bouzid, D.; Poey, N.; de Montmollin, E.; Descamps, D.; et al. Evaluation of the RealStar® SARS-CoV-2 RT-PCR Kit RUO Performances and Limit of Detection. J. Clin. Virol. 2020, 129, 104520. [Google Scholar] [CrossRef]
- Caza, M.; Hogan, C.A.; Jassem, A.; Prystajecky, N.; Hadzic, A.; Wilmer, A. Evaluation of the Clinical and Analytical Performance of the Seegene AllplexTM SARS-CoV-2 Variants I Assay for the Detection of Variants of Concern (VOC) and Variants of Interests (VOI). J. Clin. Virol. 2021, 144, 104996. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- VassarStats: Website for Statistical Computing. Available online: http://www.vassarstats.net (accessed on 22 June 2021).
- Congrave-Wilson, Z.; Lee, Y.; Jumarang, J.; Perez, S.; Bender, J.M.; Bard, J.D.; Pannaraj, P.S. Change in Saliva RT-PCR Sensitivity Over the Course of SARS-CoV-2 Infection. JAMA 2021, 326, 1065–1067. [Google Scholar] [CrossRef] [PubMed]
- Kandel, C.E.; Young, M.; Serbanescu, M.A.; Powis, J.E.; Bulir, D.; Callahan, J.; Katz, K.; McCready, J.; Racher, H.; Sheldrake, E.; et al. Detection of Severe Acute Respiratory Coronavirus Virus 2 (SARS-CoV-2) in Outpatients: A Multicenter Comparison of Self-Collected Saline Gargle, Oral Swab, and Combined Oral–Anterior Nasal Swab to a Provider Collected Nasopharyngeal Swab. Infect. Control. Hosp. Epidemiol. 2021, 42, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Lindner, A.K.; Nikolai, O.; Kausch, F.; Wintel, M.; Hommes, F.; Gertler, M.; Krüger, L.J.; Gaeddert, M.; Tobian, F.; Lainati, F.; et al. Head-to-Head Comparison of SARS-CoV-2 Antigen-Detecting Rapid Test with Self-Collected Nasal Swab versus Professional-Collected Nasopharyngeal Swab. Eur. Respir. J. 2021, 57, 2003961. [Google Scholar] [CrossRef]
- Hoch, M.; Vogel, S.; Eberle, U.; Kolberg, L.; Gruenthaler, V.; Fingerle, V.; Ackermann, N.; Sing, A.; Liebl, B.; Huebner, J.; et al. Feasibility and Diagnostic Accuracy of Saliva-Based SARS-CoV-2 Screening in Educational Settings and Children Aged <12 Years. Diagnostics 2021, 11, 1797. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.M.; Benoit, N.; Dormoi, J.; Amalvict, R.; Gomez, N.; Tissot-Dupont, H.; Million, M.; Pradines, B.; Granjeaud, S.; Almeras, L. Salivette, a Relevant Saliva Sampling Device for SARS-CoV-2 Detection. J. Oral. Microbiol. 2021, 13, 1920226. [Google Scholar] [CrossRef] [PubMed]
- Basso, D.; Aita, A.; Padoan, A.; Cosma, C.; Navaglia, F.; Moz, S.; Contran, N.; Zambon, C.-F.; Cattelan, A.M.; Plebani, M. Salivary SARS-CoV-2 Antigen Rapid Detection: A Prospective Cohort Study. Clin. Chim. Acta 2021, 517, 54–59. [Google Scholar] [CrossRef]
- Aita, A.; Basso, D.; Cattelan, A.M.; Fioretto, P.; Navaglia, F.; Barbaro, F.; Stoppa, A.; Coccorullo, E.; Farella, A.; Socal, A.; et al. SARS-CoV-2 Identification and IgA Antibodies in Saliva: One Sample Two Tests Approach for Diagnosis. Clin. Chim. Acta 2020, 510, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.C.; Biele, G.; Mühlemann, B.; Veith, T.; Schneider, J.; Beheim-Schwarzbach, J.; Bleicker, T.; Tesch, J.; Schmidt, M.L.; Sander, L.E.; et al. Estimating Infectiousness throughout SARS-CoV-2 Infection Course. Science 2021, 373, 6551. [Google Scholar] [CrossRef]
- Kidd, M.; Richter, A.; Best, A.; Cumley, N.; Mirza, J.; Percival, B.; Mayhew, M.; Megram, O.; Ashford, F.; White, T.; et al. S-Variant SARS-CoV-2 Lineage B1.1.7 Is Associated with Significantly Higher Viral Loads in Samples Tested by ThermoFisher TaqPath RT-QPCR. J. Infect. Dis. 2021, 223, 82. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Symptom | Present in Number of Patients, Out of 101 | % |
|---|---|---|
| Rhinitis | 79 | 78.2 |
| Cough | 79 | 78.2 |
| Sore throat | 68 | 67.3 |
| Fever | 50 | 59.5 |
| Gastrointestinal symptoms | 41 | 40.6 |
| Loss of smell or taste | 14 | 13.9 |
| Not reporting symptoms | 1 | 0.9 |
| Chewed Cotton Pads | Nasal Swab | Saliva | Tongue Swab | Gargle Solution | ||
|---|---|---|---|---|---|---|
| Sensitivity % | all samples (n = 102) | 70.1% (68/97) (59.8–78.8% 95% CI) | 85.1% (86/101) (76.4–91.2% 95% CI) | 92.8% (90/97) (85.2–96.8% 95% CI) | 74.2% (72/97) (64.2–82.3% 95% CI) | 89.1% (90/101) (81.0–94.2% 95% CI) |
| selected nasopharyngeal swabs containing ≥6 log10 RNA copies/mL (n = 17) * | 70.6% (12/17) (44–88.6% 95% CI) | 88.2% (15/17) (62.3–97.9% 95% CI) | 94.1% (16/17) (69.2–99.7% 95% CI) | 76.5% (13/17) (49.8–92.2% 95% CI) | 88.2% (15/17) (62.3–97.9% 95% CI) |
| Alpha Variant | Non-Alpha Variant | p-Value * | ||
|---|---|---|---|---|
| (a) | Chewed cotton pads | 3.97 (3.57–4.36 95% CI) (n = 46) | 3.7 (3.14–4.25 95% CI) (n = 25) | 0.423 |
| (b) | Nasal swab | 6.35 (6.00–6.71 95% CI) (n = 52) | 4.84 (4.11–5.58 95% CI) (n = 30) | <0.0001 |
| (c) | Saliva | 5.79 (5.38–6.21 95% CI) (n = 53) | 5.12 (4.6–5.65 95% CI) (n = 40) | 0.0443 |
| (d) | Tongue swab | 4.24 (3.90–4.58) (n = 48) | 4.01 (3.38–4.64 95% CI) (n = 28) | 0.474 |
| (e) | Gargle lavage | 5.36 (4.98–5.74 95% CI) (n = 51) | 4.4 (3.97–4.83 95% CI) (n = 37) | 0.00012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kohmer, N.; Eckermann, L.; Böddinghaus, B.; Götsch, U.; Berger, A.; Herrmann, E.; Kortenbusch, M.; Tinnemann, P.; Gottschalk, R.; Hoehl, S.; et al. Self-Collected Samples to Detect SARS-CoV-2: Direct Comparison of Saliva, Tongue Swab, Nasal Swab, Chewed Cotton Pads and Gargle Lavage. J. Clin. Med. 2021, 10, 5751. https://doi.org/10.3390/jcm10245751
Kohmer N, Eckermann L, Böddinghaus B, Götsch U, Berger A, Herrmann E, Kortenbusch M, Tinnemann P, Gottschalk R, Hoehl S, et al. Self-Collected Samples to Detect SARS-CoV-2: Direct Comparison of Saliva, Tongue Swab, Nasal Swab, Chewed Cotton Pads and Gargle Lavage. Journal of Clinical Medicine. 2021; 10(24):5751. https://doi.org/10.3390/jcm10245751
Chicago/Turabian StyleKohmer, Niko, Lisa Eckermann, Boris Böddinghaus, Udo Götsch, Annemarie Berger, Eva Herrmann, Marhild Kortenbusch, Peter Tinnemann, Rene Gottschalk, Sebastian Hoehl, and et al. 2021. "Self-Collected Samples to Detect SARS-CoV-2: Direct Comparison of Saliva, Tongue Swab, Nasal Swab, Chewed Cotton Pads and Gargle Lavage" Journal of Clinical Medicine 10, no. 24: 5751. https://doi.org/10.3390/jcm10245751
APA StyleKohmer, N., Eckermann, L., Böddinghaus, B., Götsch, U., Berger, A., Herrmann, E., Kortenbusch, M., Tinnemann, P., Gottschalk, R., Hoehl, S., & Ciesek, S. (2021). Self-Collected Samples to Detect SARS-CoV-2: Direct Comparison of Saliva, Tongue Swab, Nasal Swab, Chewed Cotton Pads and Gargle Lavage. Journal of Clinical Medicine, 10(24), 5751. https://doi.org/10.3390/jcm10245751