
Semi-Rigid Fixation Using a Sliding Plate for Treating Fractures of the Mandibular Condylar Process

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Selection Criteria
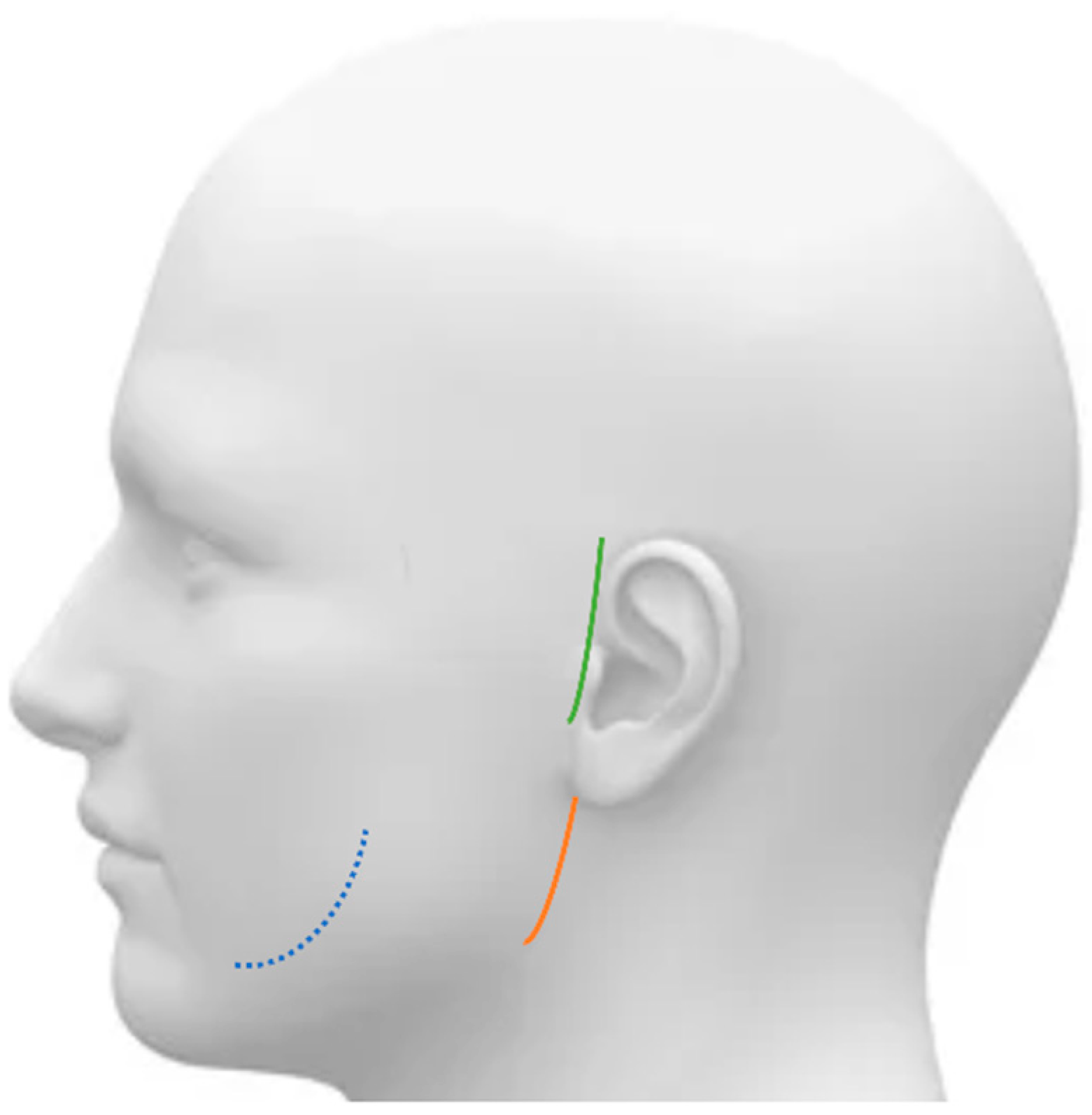
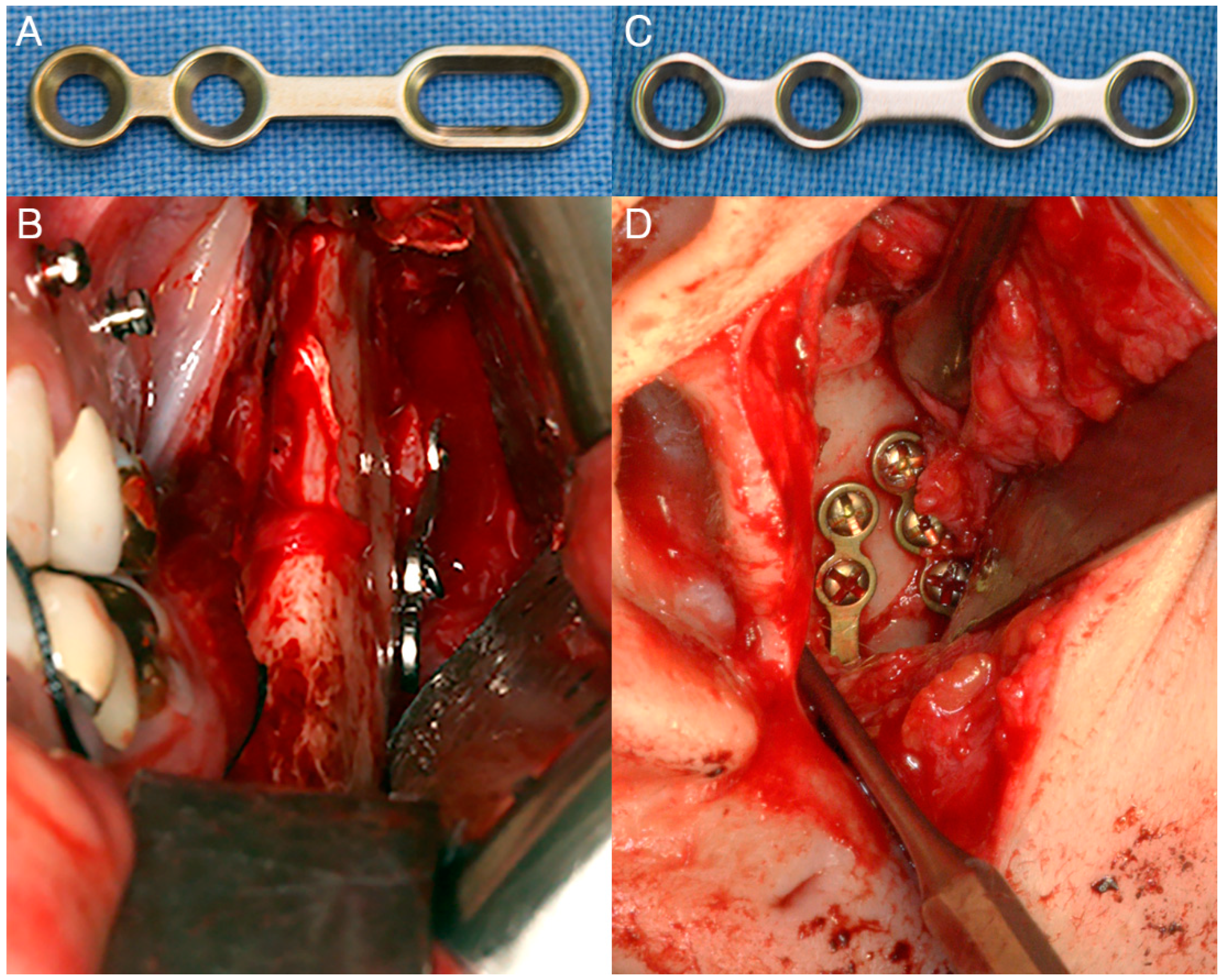
2.2. Surgical Procedures
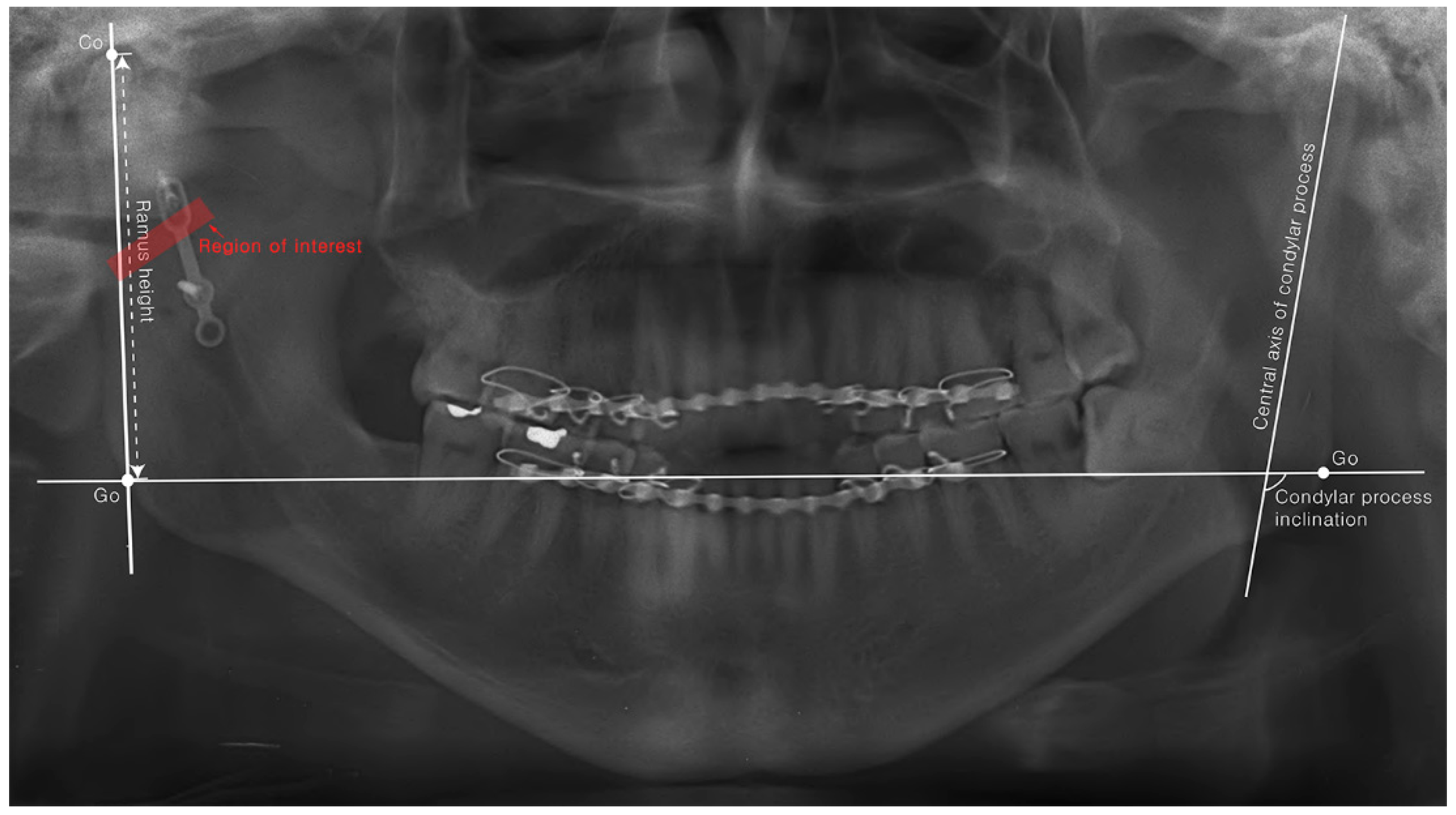
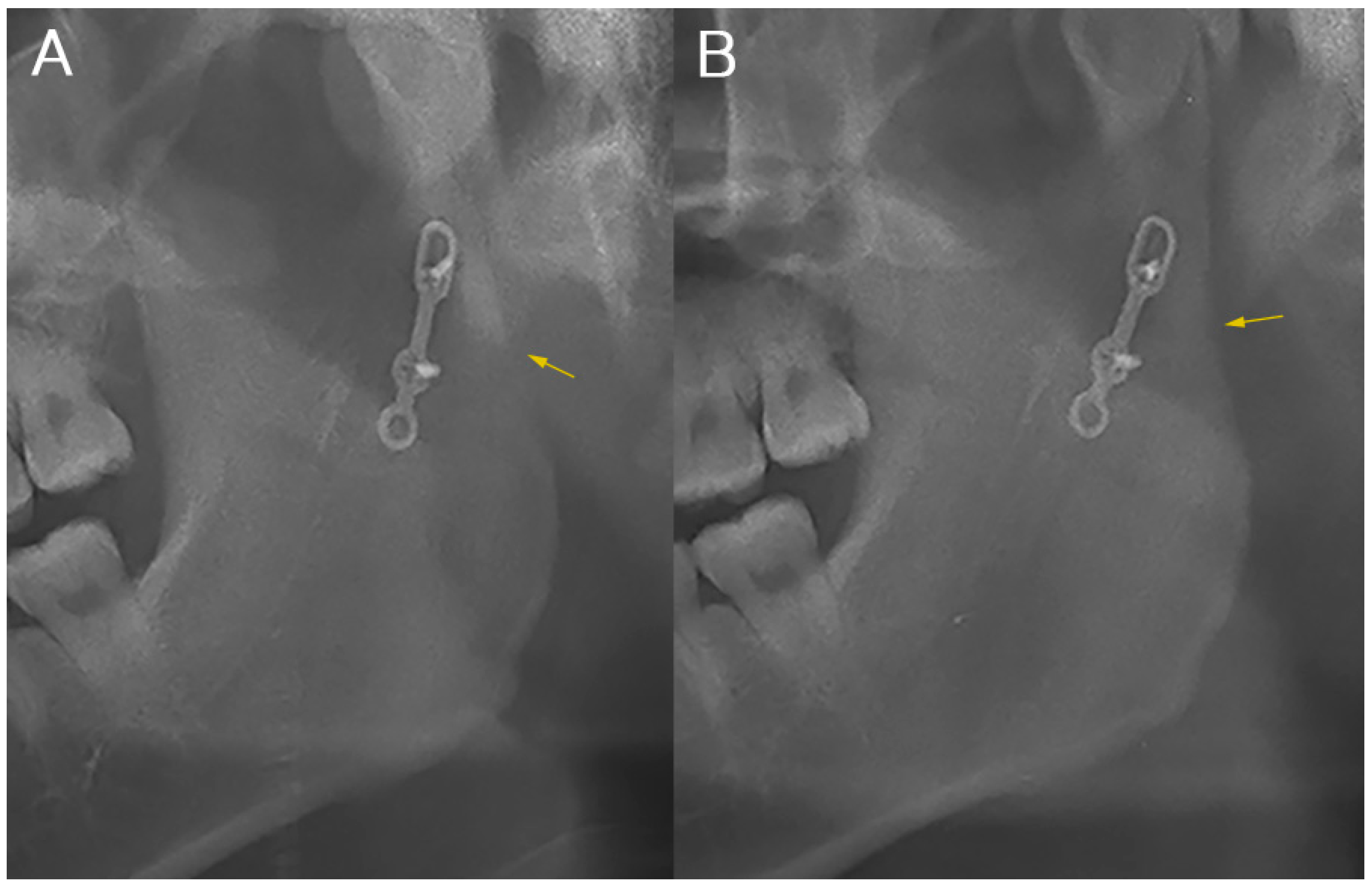
2.3. Clinical and Radiological Evaluation
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baker, A.W.; McMahon, J.; Moos, K.F. Current consensus on the management of fractures of the mandibular condyle. A method by questionnaire. Int. J. Oral Maxillofac. Surg. 1998, 27, 258–266. [Google Scholar] [CrossRef]
- Ellis, E.; Throckmorton, G.S. Treatment of mandibular condylar process fractures: Biological considerations. J. Oral Maxillofac. Surg. 2005, 63, 115–134. [Google Scholar] [CrossRef]
- Meyer, C.; Serhir, L.; Boutemi, P. Experimental evaluation of three osteosynthesis devices used for stabilizing condylar fractures of the mandible. J. Craniomaxillofac. Surg. 2006, 34, 173–181. [Google Scholar] [CrossRef]
- Lauer, G.; Schmelzeisen, R. Endoscope-assisted fixation of mandibular condylar process fractures. J. Oral Maxillofac. Surg. 1999, 57, 36–39. [Google Scholar] [CrossRef]
- Baek, R.M.; Lee, S.W. A new condyle repositionable plate for sagittal split ramus osteotomy. J. Craniofac. Surg. 2010, 21, 489–490. [Google Scholar] [CrossRef] [PubMed]
- Ghang, M.H.; Kim, H.M.; You, J.Y.; Kim, B.H.; Choi, J.P.; Kim, S.H.; Choung, P.H. Three-dimensional mandibular change after sagittal split ramus osteotomy with a semirigid sliding plate system for fixation of a mandibular setback surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 157–166. [Google Scholar] [CrossRef]
- Cienfuegos, R.; Cornelius, C.; Ellis, E. CMF Mandible—AO Surgery Reference; AO Foundation: Basel, Switzerland, 2008. [Google Scholar]
- Meyer, C.; Kahn, J.L.; Boutemi, P.; Wilk, A. Photoelastic analysis of bone deformation in the region of the mandibular condyle during mastication. J. Craniomaxillofac. Surg. 2002, 30, 160–169. [Google Scholar] [CrossRef]
- Neff, A.; Cornelius, C.P.; Rasse, M.; Torre, D.D.; Audige, L. The Comprehensive AOCMF Classification System: Condylar Process Fractures—Level 3 Tutorial. Craniomaxillofac. Trauma Reconstr. 2014, 7, S044–S058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, M.H.; Eo, M.Y.; Cho, Y.J.; Kim, S.M.; Lee, S.K. Autogenous Partial Bone Chip Grafting on the Exposed Inferior Alveolar Nerve After Cystic Enucleation. J. Craniofac. Surg. 2018, 29, 486–490. [Google Scholar] [CrossRef]
- Brandt, M.T.; Haug, R.H. Open versus closed reduction of adult mandibular condyle fractures: A review of the literature regarding the evolution of current thoughts on management. J. Oral Maxillofac. Surg. 2003, 61, 1324–1332. [Google Scholar] [CrossRef]
- Zachariades, N.; Mezitis, M.; Mourouzis, C.; Papadakis, D.; Spanou, A. Fractures of the mandibular condyle: A review of 466 cases. Literature review, reflections on treatment and proposals. J. Craniomaxillofac. Surg. 2006, 34, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Biglioli, F.; Colletti, G. Mini-retromandibular approach to condylar fractures. J. Craniomaxillofac. Surg. 2008, 36, 378–383. [Google Scholar] [CrossRef]
- Hyde, N.; Manisali, M.; Aghabeigi, B.; Sneddon, K.; Newman, L. The role of open reduction and internal fixation in unilateral fractures of the mandibular condyle: A prospective study. Br. J. Oral Maxillofac. Surg. 2002, 40, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Lauer, G.; Eckelt, U. Surgical treatment of fractures of the mandibular condyle: A comparison of long-term results following different approaches–functional, axiographical, and radiological findings. J. Craniomaxillofac. Surg. 2007, 35, 151–160. [Google Scholar] [CrossRef]
- Takenoshita, Y.; Ishibashi, H.; Oka, M. Comparison of functional recovery after nonsurgical and surgical treatment of condylar fractures. J. Oral Maxillofac. Surg. 1990, 48, 1191–1195. [Google Scholar] [CrossRef]
- Norholt, S.E.; Krishnan, V.; Sindet-Pedersen, S.; Jensen, I. Pediatric condylar fractures: A long-term follow-up study of 55 patients. J. Oral Maxillofac. Surg. 1993, 51, 1302–1310. [Google Scholar] [CrossRef]
- Jin, K.S.; Lee, H.; Sohn, J.B.; Han, Y.S.; Jung, D.U.; Sim, H.Y.; Kim, H.S. Fracture patterns and causes in the craniofacial region: An 8-year review of 2076 patients. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 29. [Google Scholar] [CrossRef]
- Ellis, E., 3rd; Dean, J. Rigid fixation of mandibular condyle fractures. Oral Surg. Oral Med. Oral Pathol. 1993, 76, 6–15. [Google Scholar] [CrossRef]
- Vesnaver, A.; Gorjanc, M.; Eberlinc, A.; Dovsak, D.A.; Kansky, A.A. The periauricular transparotid approach for open reduction and internal fixation of condylar fractures. J. Craniomaxillofac. Surg. 2005, 33, 169–179. [Google Scholar] [CrossRef]
- Wagner, A.; Krach, W.; Schicho, K.; Undt, G.; Ploder, O.; Ewers, R. A 3-dimensional finite-element analysis investigating the biomechanical behavior of the mandible and plate osteosynthesis in cases of fractures of the condylar process. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 678–686. [Google Scholar] [CrossRef]
- Conci, R.A.; Tomazi, F.H.; Noritomi, P.Y.; da Silva, J.V.; Fritscher, G.G.; Heitz, C. Comparison of Neck Screw and Conventional Fixation Techniques in Mandibular Condyle Fractures Using 3-Dimensional Finite Element Analysis. J. Oral Maxillofac. Surg. 2015, 73, 1321–1327. [Google Scholar] [CrossRef]
- Jung, H.D.; Kim, S.Y.; Park, H.S.; Jung, Y.S. Orthognathic surgery and temporomandibular joint symptoms. Maxillofac. Plast. Reconstr. Surg. 2015, 37, 14. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; You, H.S.; Huh, J.K.; Park, K.H. Is There a Difference in Condyle Position Changing Pattern Between Deviated and Non-Deviated Sides After Intraoral Vertical Ramus Osteotomy in Facial Asymmetry? J. Oral Maxil. Surg. 2020, 78, 629.e1–629.e10. [Google Scholar] [CrossRef] [PubMed]
- Gursoytrak, B.; Unsal, N.; Demetoglu, U.; Simsek, H.O.; Saglam, H.; Dolanmaz, D. Biomechanical evaluation of hybrid fixation method of sagittal split ramus osteotomy in mandibular advancement. J. Craniomaxillofac. Surg. 2018, 46, 2063–2068. [Google Scholar] [CrossRef]
- Kim, S.S.; Kwak, K.H.; Ko, C.C.; Park, S.B.; Son, W.S.; Kim, Y.I. Comparison of postoperative changes in the distal and proximal segments between conventional and sliding mini-plate fixation following mandibular setback. Korean J. Orthod. 2016, 46, 372–378. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.G.; Agpoon, K.J.; Besana, A.N.; Lim, H.K.; Jang, H.S.; Lee, E.S. Mandibular stability using sliding or conventional four-hole plates for fixation after bilateral sagittal split ramus osteotomy for mandibular setback. Br. J. Oral Maxillofac. Surg. 2017, 55, 378–382. [Google Scholar] [CrossRef]
- Roh, Y.C.; Shin, S.H.; Kim, S.S.; Sandor, G.K.; Kim, Y.D. Skeletal stability and condylar position related to fixation method following mandibular setback with bilateral sagittal split ramus osteotomy. J. Cranio-Maxillofac. Surg. 2014, 42, 1958–1963. [Google Scholar] [CrossRef] [PubMed]
- Larson, B.E.; Lee, N.K.; Jang, M.J.; Jo, D.W.; Yun, P.Y.; Kim, Y.K. Comparative evaluation of the sliding plate technique for fixation of a sagittal split ramus osteotomy: Finite element analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, E148–E152. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Yamamoto, K.; Sugiura, T.; Horita, S.; Matsusue, Y.; Kirita, T. Computed Tomography-Based 3-Dimensional Finite Element Analyses of Various Types of Plates Placed for a Virtually Reduced Unilateral Condylar Fracture of the Mandible of a Patient. J. Oral Maxillofac. Surg. 2017, 75, 1239.e1–1239.e11. [Google Scholar] [CrossRef]
- Darwich, M.A.; Albogha, M.H.; Abdelmajeed, A.; Darwich, K. Assessment of the Biomechanical Performance of 5 Plating Techniques in Fixation of Mandibular Subcondylar Fracture Using Finite Element Analysis. J. Oral Maxillofac. Surg. 2016, 74, e791–e798. [Google Scholar] [CrossRef]
- Liokatis, P.; Tzortzinis, G.; Gerasimidis, S.; Smolka, W. Finite Element Analysis of Different Titanium Plates for Internal Fixation of Fractures of the Mandibular Condylar Neck. J. Oral Maxillofac. Surg. 2021, 79, 665.e1–665.e11. [Google Scholar] [CrossRef]
- De Jesus, G.P.; Vaz, L.G.; Gabrielli, M.F.; Passeri, L.A.; Oliveira, T.V.; Noritomi, P.Y.; Jurgens, P. Finite element evaluation of three methods of stable fixation of condyle base fractures. Int. J. Oral Maxillofac. Surg. 2014, 43, 1251–1256. [Google Scholar] [CrossRef]
- Woo, I.H.; Kim, J.W.; Kim, J.Y.; Yang, B.E. A New Method of Fixation with the Yang’s Keyhole Plate System for the Treatment of Mandible Fractures. J. Craniofac. Surg. 2017, 28, 508–512. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Semi-Rigid Fixation Group (n = 17) | Rigid Fixation Group (n = 17) | |
|---|---|---|
| Condylar neck fracture | 7 | 6 |
| Condylar process base fracture | 10 | 11 |
| Intraoral approach | 12 | 10 |
| Retromandibular approach | 4 | 1 |
| Preauricular approach | 1 | 6 |
| Complications | Semi-Rigid Fixation Group (n = 17) | Rigid Fixation Group (n = 17) |
|---|---|---|
| Mouth-opening limitation | 4 | 6 |
| Early occlusal interference | 2 | 3 |
| Facial nerve damage | 0 | 3 |
| Acute infection | 0 | 0 |
| Condylar head resorption | 0 | 0 |
| Malunion | 0 | 0 |
| POD 1D | POD 6M | p-Value | ||
|---|---|---|---|---|
| Differences in ramus height (mm) | Semi-rigid | 4.91 ± 3.79 | 5.50 ± 4.70 | 0.705 |
| Rigid | 3.99 ± 2.85 | 5.35 ± 3.12 | 0.124 | |
| p-Value | 0.734 | 0.786 | ||
| Differences in condylar process inclination (degree) | Semi-rigid | 6.77 ± 5.06 | 6.76 ± 8.36 | 0.723 |
| Rigid | 8.73 ± 10.61 | 12.30 ± 13.07 | 0.246 | |
| p-Value | 1.000 | 0.708 | ||
| Radio-density (Mean grayscale value of ROI) | Semi-rigid | 100.5 ± 17.4 | 102.5 ± 18.4 | 0.035 |
| Rigid | 120.7 ± 31.4 | 124.1 ± 28.7 | 0.044 | |
| p-Value | 0.041 | 0.013 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
So, B.-K.; Ko, K.-S.; Kim, D.-H.; Jang, H.-S.; Lee, E.-S.; Lim, H.-K. Semi-Rigid Fixation Using a Sliding Plate for Treating Fractures of the Mandibular Condylar Process. J. Clin. Med. 2021, 10, 5782. https://doi.org/10.3390/jcm10245782
So B-K, Ko K-S, Kim D-H, Jang H-S, Lee E-S, Lim H-K. Semi-Rigid Fixation Using a Sliding Plate for Treating Fractures of the Mandibular Condylar Process. Journal of Clinical Medicine. 2021; 10(24):5782. https://doi.org/10.3390/jcm10245782
Chicago/Turabian StyleSo, Byung-Kyu, Kyeong-Soo Ko, Dong-Hyuck Kim, Hyon-Seok Jang, Eui-Seok Lee, and Ho-Kyung Lim. 2021. "Semi-Rigid Fixation Using a Sliding Plate for Treating Fractures of the Mandibular Condylar Process" Journal of Clinical Medicine 10, no. 24: 5782. https://doi.org/10.3390/jcm10245782
APA StyleSo, B. -K., Ko, K. -S., Kim, D. -H., Jang, H. -S., Lee, E. -S., & Lim, H. -K. (2021). Semi-Rigid Fixation Using a Sliding Plate for Treating Fractures of the Mandibular Condylar Process. Journal of Clinical Medicine, 10(24), 5782. https://doi.org/10.3390/jcm10245782