
Effects of an Eccentric Training Protocol Using Gliding Discs on Balance and Lower Body Strength in Healthy Adults




Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
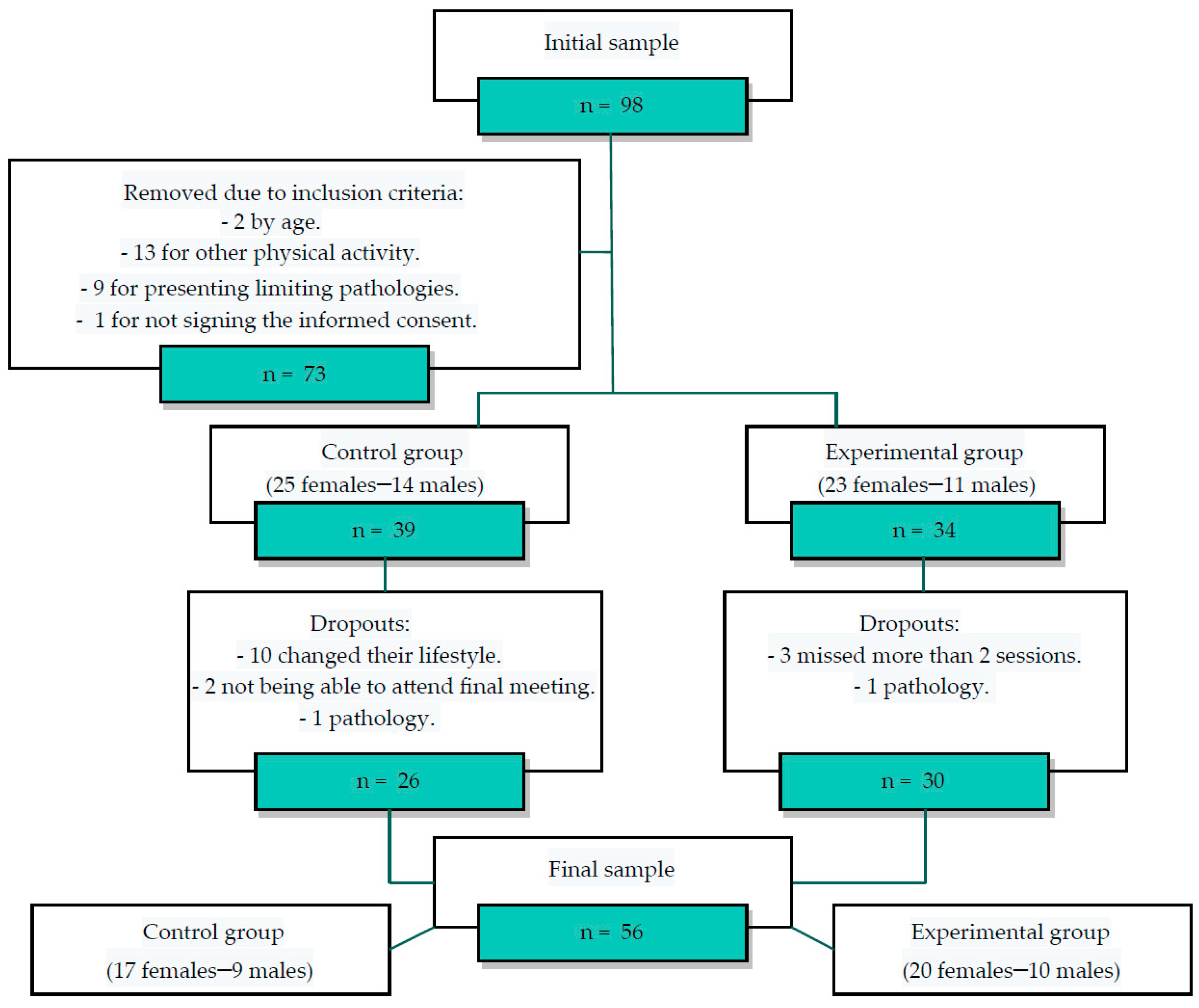
2.2. Participants
2.3. Studied Variables
2.3.1. Anthropometric variables
2.3.2. Lower Body Strength
2.3.3. Quality of Life
2.3.4. Balance
2.4. Intervention
2.4.1. Assessment
2.4.2. Training Sessions
2.5. Ethics
2.6. Statistics Analysis
3. Results
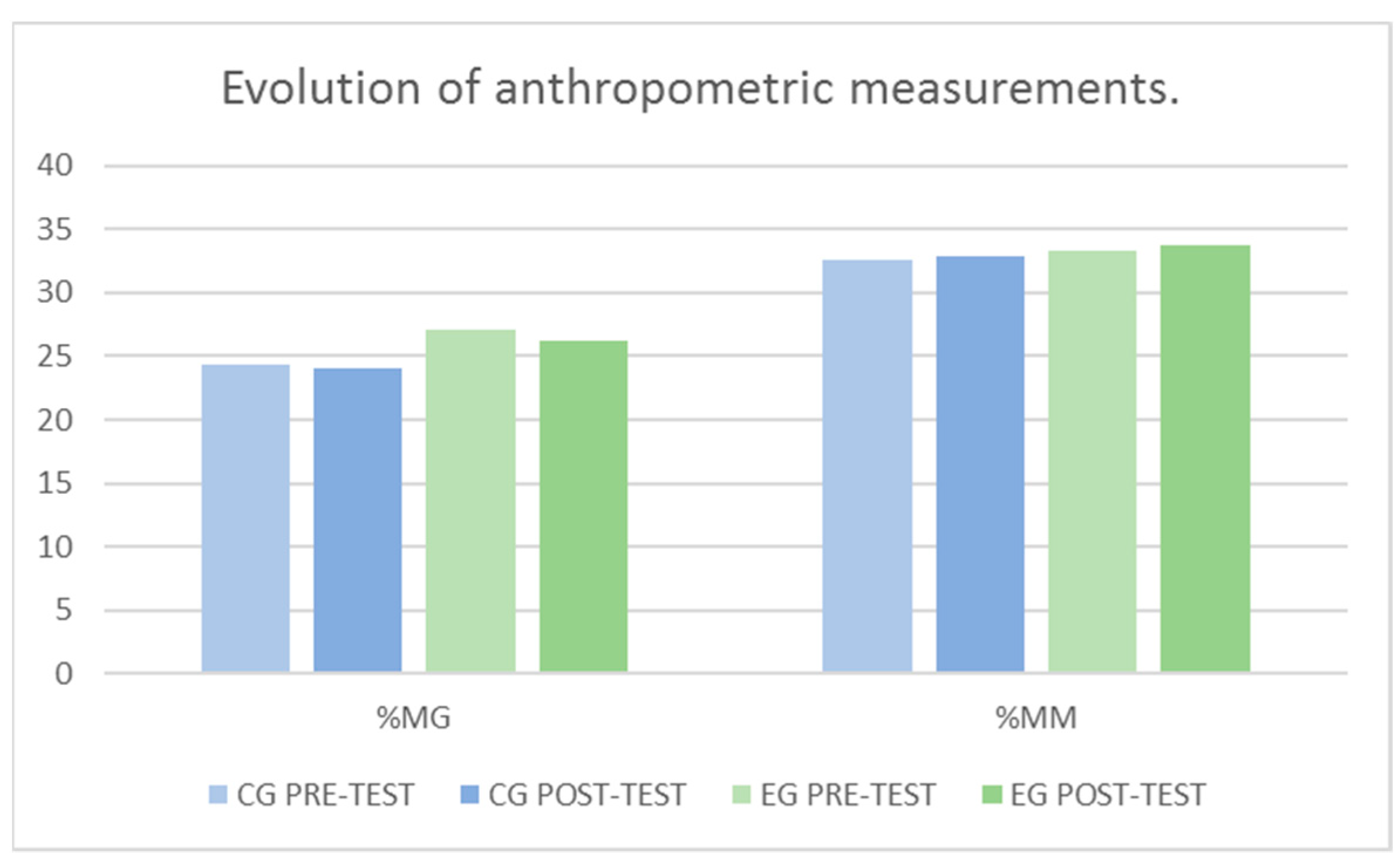
3.1. Results of Anthropometric Variables
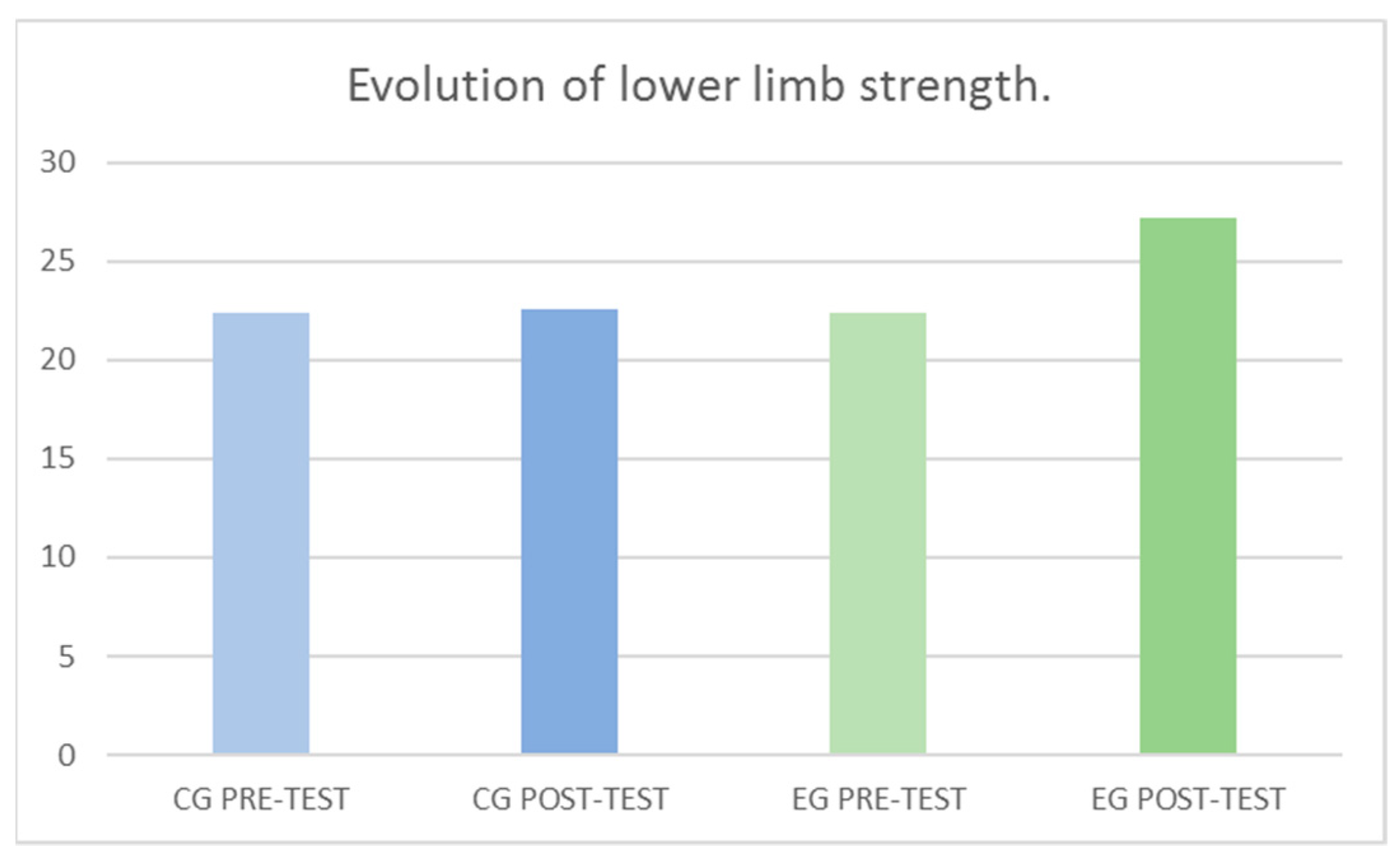
3.2. Results of the Strength of the Lower Body Musculature (SJ)
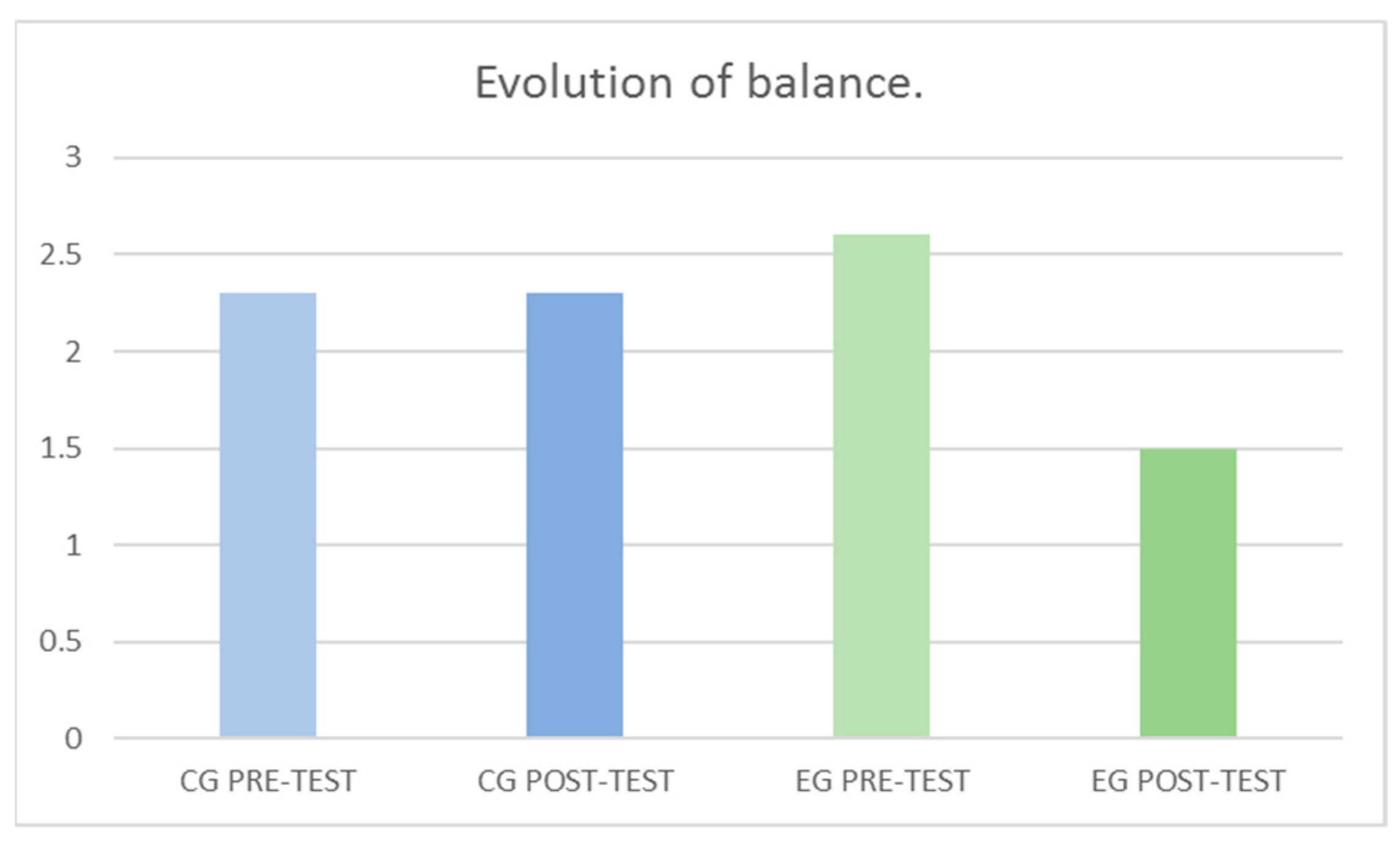
3.3. Results of the Capacity to Control Balance (EQUI)
3.4. Results of the Quality of Life (QoL)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Olson, S.L.; Chen, S.-S.; Wang, C.-Y. Effect of a Home Exercise Program on Dynamic Balance in Elderly with a History of Falls. J. Aging Phys. Act. 2011, 19, 291–305. [Google Scholar] [CrossRef]
- Graafmans, W.; Ooms, M.; Hofstee, H.; Bezemer, P.; Bouter, L.M.; Lips, P. Falls in the Elderly: A Prospective Study of Risk Factors and Risk Profiles. Am. J. Epidemiol. 1996, 143, 1129–1136. [Google Scholar] [CrossRef] [Green Version]
- Alamgir, H.; Muazzam, S.; Nasrullah, M. Unintentional Falls Mortality among Elderly in the United States: Time for Action. Injury 2012, 43, 2065–2071. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Tang, Q.; Xu, S.; Leng, P.; Pan, Z. Design and Evaluation of an Augmented Reality-Based Exergame System to Reduce Fall Risk in the Elderly. Int. J. Environ. Res. Public Health 2020, 17, 7208. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H.; Bok, S.K.; Kim, Y.-J.; Hwang, S.L. Effect of Lower Limb Strength on Falls and Balance of the Elderly. Ann. Rehabil. Med. 2012, 36, 386. [Google Scholar] [CrossRef] [PubMed]
- Díaz, L.B.; Casuso-Holgado, M.J.; Labajos-Manzanares, M.T.; Barón-López, F.J.; Pinero-Pinto, E.; Romero-Galisteo, R.P.; Moreno-Morales, N. Analysis of Fall Risk Factors in an Aging Population Living in Long-Term Care Institutions in Spain: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 7234. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.J.; Borrie, M.J.; Spears, G.F. Risk Factors for Falls in a Community-Based Prospective Study of People 70 Years and Older. J. Gerontol. 1989, 44, M112–M117. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk Factors for Falls among Elderly Persons Living in the Community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef]
- Mora, M.; Villalobos, D.; Araya, G.; Ozols, A. Perspectiva Subjetiva de La Calidad de Vida Del Adulto Mayor, Diferencias Ligadas al Género Ya La Práctica de La Actividad Físico Recreativa. MHSALUD Rev. En Cienc. Del Mov. Hum. Y Salud 2004, 1, 1–11. [Google Scholar] [CrossRef]
- Loecker, C.; Schmaderer, M.; Zimmerman, L. Frailty in Young and Middle-Aged Adults: An Integrative Review. J. Frailty Aging 2021, 10, 327–333. [Google Scholar] [CrossRef]
- Motalebi, S.A.; Cheong, L.S.; Iranagh, J.A.; Mohammadi, F. Effect of Low-Cost Resistance Training on Lower-Limb Strength and Balance in Institutionalized Seniors. Exp. Aging Res. 2018, 44, 48–61. [Google Scholar] [CrossRef] [PubMed]
- Muehlbauer, T.; Gollhofer, A.; Granacher, U. Associations between Measures of Balance and Lower-Extremity Muscle Strength/Power in Healthy Individuals across the Lifespan: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1671–1692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benford, J.; Hughes, J.; Waldron, M.; Theis, N. Concentric versus Eccentric Training: Effect on Muscle Strength, Regional Morphology, and Architecture. Transl. Sports Med. 2021, 4, 46–55. [Google Scholar] [CrossRef]
- Büker, N.; Şavkin, R.; Süzer, A.; Akkaya, N. Effect of Eccentric and Concentric Squat Exercise on Quadriceps Thickness and Lower Extremity Performance in Healthy Young Males. Acta Gymnica 2021, 51. [Google Scholar] [CrossRef]
- Chen, T.C.; Hsieh, C.-C.; Tseng, K.-W.; Ho, C.-C.; Nosaka, K. Effects of Descending Stair Walking on Health and Fitness of Elderly Obese Women. Med. Sci. Sports Exerc. 2017, 49, 1614–1622. [Google Scholar] [CrossRef]
- Chen, T.C.-C.; Tseng, W.-C.; Huang, G.-L.; Chen, H.-L.; Tseng, K.-W.; Nosaka, K. Superior Effects of Eccentric to Concentric Knee Extensor Resistance Training on Physical Fitness, Insulin Sensitivity and Lipid Profiles of Elderly Men. Front. Physiol. 2017, 8, 209. [Google Scholar] [CrossRef] [Green Version]
- Gremeaux, V.; Duclay, J.; Deley, G.; Philipp, J.; Laroche, D.; Pousson, M.; Casillas, J. Does Eccentric Endurance Training Improve Walking Capacity in Patients with Coronary Artery Disease? A Randomized Controlled Pilot Study. Clin. Rehabil. 2010, 24, 590–599. [Google Scholar] [CrossRef]
- Wilke, J.; Alfredson, H. Eccentric Training: The Key for a Stronger, More Resilient Athlete? In Oncology Massage; Handspring Publishing Limited: Pencaitland, UK, 2021. [Google Scholar]
- Lukman, G. Osnovne Pilates Vaje z Drsniki; Handspring Publishing Limited: Pencaitland, UK, 2018. [Google Scholar]
- Prieto, J.A.; Valle, M.D.; Nistal, P.; Méndez, D.; Barcala-Furelos, R.; Abelairas-Gómez, C. Relevancia de Un Programa de Equilibrio En La Calidad de Vida Relacionada Con La Salud de Mujeres Adultas Mayores Obesas. Nutr. Hosp. 2015, 32, 2800–2807. [Google Scholar] [CrossRef] [PubMed]
- Sylejmani, B.; Myrtaj, N.; Maliqi, A.; Gontarev, S.; Georgiev, G.; Kalac, R. Physical Fitness in Children and Adolescents in Rural and Urban Areas. J. Hum. Sport Exerc. 2019, 14, 866–875. [Google Scholar] [CrossRef]
- Gatterer, H.; Haacke, S.; Burtscher, M.; Faulhaber, M.; Melmer, A.; Ebenbichler, C.; Strohl, K.P.; Högel, J.; Netzer, N.C. Normobaric Intermittent Hypoxia over 8 Months Does Not Reduce Body Weight and Metabolic Risk Factors-a Randomized, Single Blind, Placebo-Controlled Study in Normobaric Hypoxia and Normobaric Sham Hypoxia. Obes. Facts 2015, 8, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Bosco, C.; Viitasalo, J.; Komi, P.; Luhtanen, P. Combined Effect of Elastic Energy and Myoelectrical Potentiation during Stretch-shortening Cycle Exercise. Acta Physiol. Scand. 1982, 114, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, C.; Layte, R. Development and Testing of the UK SF-12. J. Health Serv. Res. Policy 1997, 2, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Leirós-Rodríguez, R.; Romo-Pérez, V.; García-Soidán, J.L. Validity and Reliability of a Tool for Accelerometric Assessment of Static Balance in Women. Eur. J. Physiother. 2017, 19, 243–248. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Lawrence Earlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Gordon, J.P.; Thompson, B.J.; Crane, J.S.; Bressel, E.; Wagner, D.R. Effects of Isokinetic Eccentric versus Traditional Lower Body Resistance Training on Muscle Function: Examining a Multiple-Joint Short-Term Training Model. Appl. Physiol. Nutr. Metab. 2019, 44, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.; Chen, S.; Tsou, Y. Effects of Whole-Body Vibration and Balance Training on Female Athletes with Chronic Ankle Instability. J. Clin. Med. 2021, 10, 2380. [Google Scholar] [CrossRef]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. Interpretación de Los Cuestionarios de Salud SF-36 y SF-12 En España: Componentes Físico y Mental. Med. Clínica 2008, 130, 726–735. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercise | Starting/Ending Position | Middle Position |
|---|---|---|
| Back split |  |  |
| Lateral split |  |  |
| Front split |  |  |
| Hamstring curl |  |  |
| Variable | ALL (n = 56) | CG (n = 25) | EG (n = 31) | p-Value | |||
|---|---|---|---|---|---|---|---|
| x ± SD | Median | x ± SD | P50 | x ± SD | Median | ||
| Age (Years) | 30.9 ± 10.5 | 27.5 | 30.6 ± 8.9 | 28 | 31.2 ± 11.8 | 27 | 0.827 |
| Weight (Kg) | 72.1 ± 12.7 | 71 | 69.8 ± 11.5 | 69 | 74 ± 13.5 | 71.1 | 0.313 |
| Height (cm) | 1.7 ± 0.1 | 1.7 | 1.7 ± 0.1 | 1.68 | 1.7 ±0.1 | 1.7 | 0.219 |
| BMI (Kg/m2) | 24.9 ± 2.7 | 24.7 | 24.5 ± 2.4 | 24.62 | 25.2 ± 3.1 | 24.5 | 0.359 |
| %MG | 25.6 ± 7.9 | 23.8 | 24.3 ± 6.9 | 22.6 | 27.1 ± 9.1 | 27.7 | 0.207 |
| %MM | 33.1 ± 5.6 | 32.4 | 32.6 ± 5 | 31.5 | 33.3 ± 6.4 | 33.1 | 0.633 |
| SJ | 23.8 ± 6.2 | 23.8 | 22.4 ± 5.6 | 21.3 | 22.4 ± 6.7 | 21.9 | 0.987 |
| EQUI | 2.2 ± 1.1 | 2 | 2.3 ± 1.2 | 1.99 | 2.6 ± 1.2 | 2.4 | 0.339 |
| mSF-12 | 50.2 ± 1.9 | 51 | 49.9 ± 2.1 | 51 | 49.6 ± 2.3 | 51 | 0.594 |
| fSF-12 | 52.8 ± 2.8 | 53 | 52.1 ± 2.4 | 53 | 52.7 ± 3.3 | 53 | 0.611 |
| Variable | Group | Pre-Test Mean 95% CI | Post-Test Mean 95% CI | Cohen’s d | Group M Group × M p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| %MG | CG | 24.3 | (21.4–27.2) | 24.1 | (21.2–26.9) | −0.10 | 0.107 | 0.727 | 0.818 |
| EG | 27.1 | (23.8–30.4) | 26.2 | (23.2–29.3) | |||||
| %MM | CG | 32.6 | (30.5–34.6) | 32.8 | (30.7–34.9) | 0.06 | 0.438 | 0.777 | 0.933 |
| EG | 33.3 | (30.9–35.6) | 33.7 | (31.5–35.9) | |||||
| SJ | CG | 22.4 | (20.1–24.8) | 22.6 | (20.6–24.7) | 0.76 | 0.043 | 0.027 | 0.045 |
| EG | 22.4 | (19.9–24.9) | 27.2 | (25.1–29.3) | |||||
| EQUI | CG | 2.3 | (1.8–2.8) | 2.3 | (1.9–2.8) | −1.11 | 0.226 | 0.010 | 0.008 |
| EG | 2.6 | (2.2–3) | 1.5 | (1.3–1.8) | |||||
| pSF-12 | CG | 49.9 | (48.6–51.1) | 49.8 | (48.4–50.9) | −0.01 | 0.654 | 0.754 | 0.862 |
| EG | 49.6 | (48.4–50.9) | 49.8 | (48.5–50.7) | 0.02 | ||||
| fSF-12 | CG | 53.1 | (52.1–54.1) | 53 | (51.9–54.1) | −0.03 | 0.424 | 0.899 | 0.958 |
| EG | 52.7 | (51.5–53.9) | 52.6 | (51.6–53.6) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Barreiro, J.; Hernandez-Lucas, P.; Garcia-Soidan, J.L.; Romo-Perez, V. Effects of an Eccentric Training Protocol Using Gliding Discs on Balance and Lower Body Strength in Healthy Adults. J. Clin. Med. 2021, 10, 5965. https://doi.org/10.3390/jcm10245965
Lopez-Barreiro J, Hernandez-Lucas P, Garcia-Soidan JL, Romo-Perez V. Effects of an Eccentric Training Protocol Using Gliding Discs on Balance and Lower Body Strength in Healthy Adults. Journal of Clinical Medicine. 2021; 10(24):5965. https://doi.org/10.3390/jcm10245965
Chicago/Turabian StyleLopez-Barreiro, Juan, Pablo Hernandez-Lucas, Jose Luis Garcia-Soidan, and Vicente Romo-Perez. 2021. "Effects of an Eccentric Training Protocol Using Gliding Discs on Balance and Lower Body Strength in Healthy Adults" Journal of Clinical Medicine 10, no. 24: 5965. https://doi.org/10.3390/jcm10245965
APA StyleLopez-Barreiro, J., Hernandez-Lucas, P., Garcia-Soidan, J. L., & Romo-Perez, V. (2021). Effects of an Eccentric Training Protocol Using Gliding Discs on Balance and Lower Body Strength in Healthy Adults. Journal of Clinical Medicine, 10(24), 5965. https://doi.org/10.3390/jcm10245965