Interleukin-6 Could Be a Potential Prognostic Factor in Ambulatory Elderly Patients with Stable Heart Failure: Results from a Pilot Study


 ,
,
Abstract
:1. Introduction
2. Methods
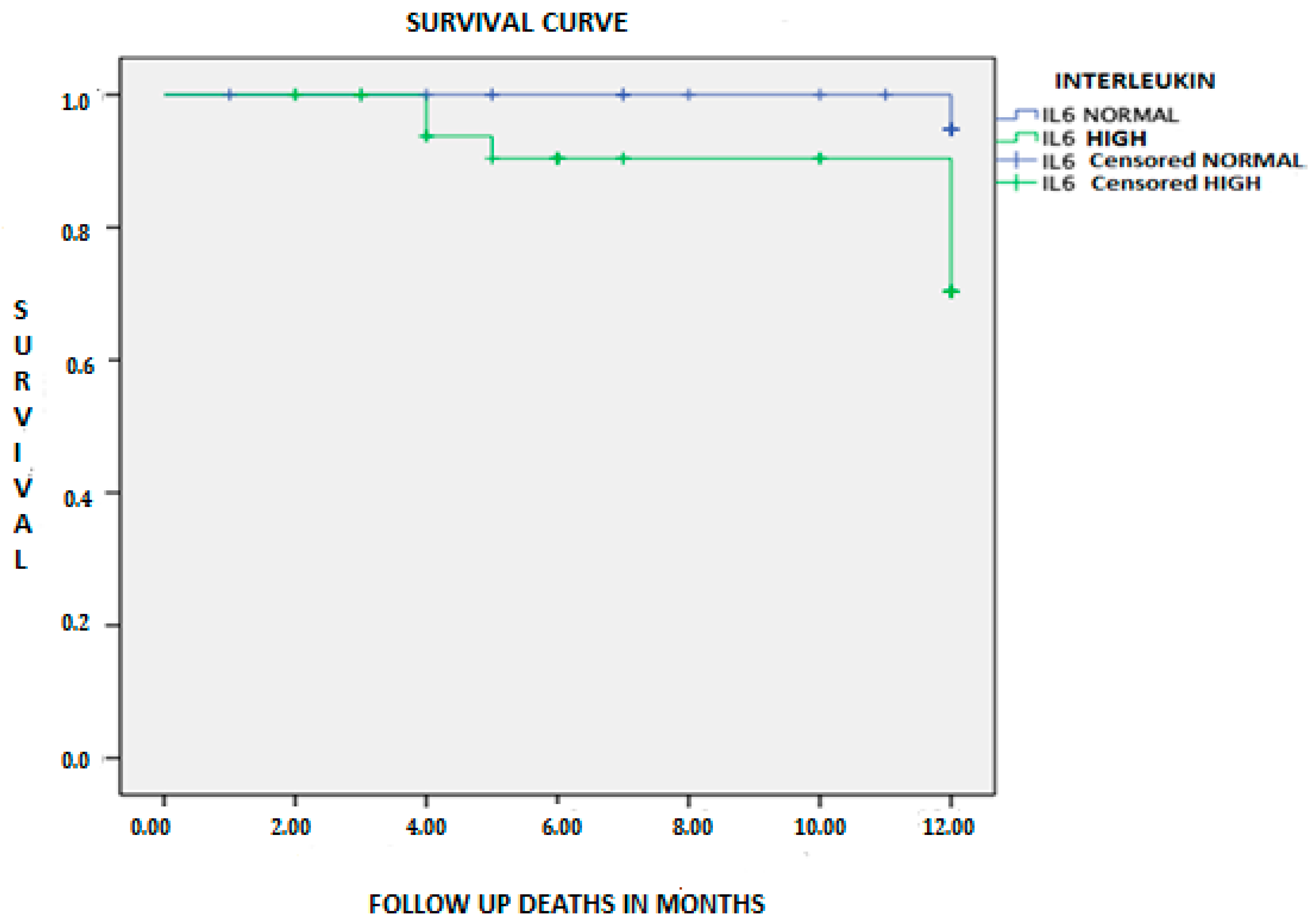
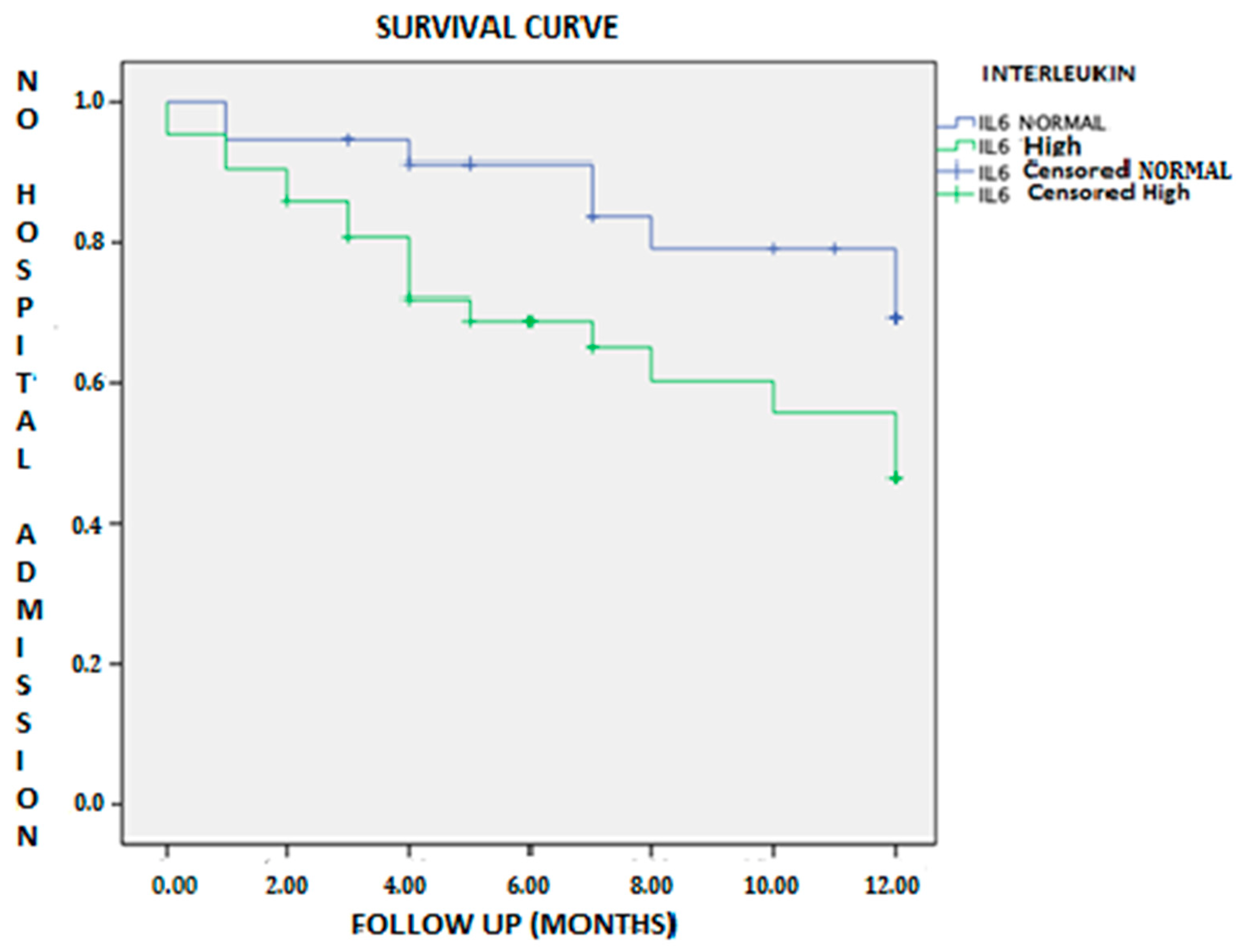
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murphy, S.P.; Kakkar, R.; McCarthy, C.P.; Januzzi, J.L. Inflammation in Heart Failure. J. Am. Coll. Cardiol. 2020, 75, 1324–1340. [Google Scholar] [CrossRef] [PubMed]
- Shirazi, L.F.; Bissett, J.; Romeo, F.M.J. Role of inflammation in heart failure. Curr. Atheroscler. Rep. 2017, 19, 27. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.; Guralnik, J.M.; Longo, D.L.F.L. Interleukin-6 in aging and chronic disease: A magnificent pathway. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 575–584. [Google Scholar] [CrossRef]
- Chung, E.S.; Packer, M.; Lo, K.H.; Fasanmade, A.A.; Willerson, J.T. Randomized, double-blind, placebo-controlled, pilot trial of infliximab, a chimeric monoclonal antibody to tumor necrosis factor-α, in patients with moderate-to-severe heart failure: Results of the anti-TNF therapy against congestive heart failure (ATTACH. Circulation 2003, 107, 3133–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, D.L.; McMurray, J.J.; Packer, M.; Swedberg, K.; Borer, J.S.; Colucci, W.S.; Djian, J.; Drexler, H.; Feldman, A.; Kober, L.; et al. Targeted anticytokine therapy in patients with chronic heart failure: Results of the Randomized Etanercept Worldwide Evaluation (RENEWAL). Circulation 2004, 109, 1594–1602. [Google Scholar] [CrossRef] [Green Version]
- Markousis-Mavrogenis, G.; Tromp, J.; Ouwerkerk, W.; Devalaraja, M.; Anker, S.D.; Cleland, J.G.; Dickstein, K.; Filippatos, G.S.; van der Hast, P.; Lang, C.C. The clinical significance of interleukin-6 in heart failure: Results from the BIOSTAT-CHF study. Eur. J. Heart Fail. 2019, 6, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M.; Everett, B.; Thuren, T.; Macfadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. GR on behalf of the CTG. Anti-inflammatory therapy with canakinumab for atherosclerotic disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Ridker, P.M.; Libby, P.; MacFadyen, J.G.; Thuren, T.; Ballantyne, C.; Fonseca, F.; Koening, W.; Shimokawa, H.; Everett, B.M.; Glynn, J.R. Modulation of the interleukin-6 signalling pathway and incidence rates of atherosclerotic events and all-cause mortality: Analyses from the Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS). Eur. Heart J. 2018, 39, 3499–3507. [Google Scholar] [CrossRef] [Green Version]
- Vázquez, Á.J.; García, M.; Sánchez, G.M.; Álvarez, L.M.; Herrero, V.A.; Herrero, P.P. MR-proadrenomedulina y copeptina como predictores de reconsulta precoz en insuficiencia cardiaca aguda. Emergencias 2018, 30, 358–359. [Google Scholar]
- Maeda, K.; Tsutamoto, T.; Wada, A.; Mabuchi, N.; Hayashi, M.; Tsutsui, T.; Ohnishi, M.; Sawaki, M.; Fujii, M.; Matsumoto, T.K.M. High levels of plasma brain natriuretic peptide and interleukin-6 after optimized treatment for heart failure are independent risk factors for morbidity and mortality in patients with congestive heart failure. J. Am. Coll. Cardiol. 2000, 36, 1587–1589. [Google Scholar] [CrossRef] [Green Version]
- Hamzic-Mehmedbasic, A. Inflammatory cytokines as risk factors for mortality after acute cardiac events. Med. Arch. 2016, 70, 252–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollenberg, S.M.; Warner, S.L.; Ahmad, T.; Amin, V.J.; Bozkurt, B.; Butler, J.; Davis, L.L.; Drazner, M.H.; Kirkpatrick, J.N.; Peterson, P.N.; et al. 2019 ACC Expert Consensus Decision Pathway on Risk Assessment, Management, and Clinical Trajectory of Patients Hospitalized with Heart Failure: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2019, 74, 1966–2011. [Google Scholar] [CrossRef] [PubMed]
- Ohkuma, T.; Jun, M.; Woodward, M.; Zoungas, S.; Cooper, M.E.; Grobbee, D.E.; Hamet, P.; Mancia, G.; Williams, B.; Welsh, P.; et al. Cardiac stress and inflammatory markers as predictors of heart failure in patients with type 2 diabetes: The ADVANCE trial. Diabetes Care 2017, 40, 1203–1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, F.B.; Meigs, J.B.; Li, T.Y.; Rifai, N.M.J. Inflammatory markers and risk of developing type 2 diabetes in women. Diabetes 2004, 53, 693–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spranger, J.; Kroke, A.; Möhlig, M.; Hoffmann, K.; Bergmann, M.M.; Ristow, M.; Boeing, H.; Pfeiffer, A.F.H. Inflammatory cytokines and the risk to develop type 2 diabetes: Results of the prospective population-based European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam Study. Diabetes 2003, 52, 812–817. [Google Scholar] [CrossRef] [Green Version]
- Jankowska, E.A.; Von Haehling, S.; Anker, S.D.; MacDougall, I.C.P.P. Iron deficiency and heart failure: Diagnostic dilemmas and therapeutic perspectives. Eur. Heart J. 2013, 34, 816–829. [Google Scholar] [CrossRef] [Green Version]
- Nemeth, E.; Valore, E.V.; Territo, M.; Schiller, G.; Lichtenstein, A.G.T. Hepcidin, a putative mediator of anemia of inflammation, is a type II acute-phase protein. Blood 2003, 101, 2461–2463. [Google Scholar] [CrossRef]
- Means, R.T., Jr. Advances in the anemia of chronic disease. Int. J. Hematol. 1999, 70, 7–12. [Google Scholar]
- Wu, C.K.; Lee, J.K.; Chiang, F.T.; Yang, C.H.; Huang, S.W.; Hwang, J.J.; Lin, J.L.; Tseng, C.D.; Chen, J.J.T.C. Plasma levels of tumor necrosis factor-? and interleukin-6 are associated with diastolic heart failure through downregulation of sarcoplasmic reticulum Ca2+ ATPase. Crit. Care Med. 2011, 39, 984–992. [Google Scholar] [CrossRef]
- Periasamy, M.H.S. SERCA pump level is a critical determinant of Ca(2+)homeostasis and cardiac contractility. J. Mol. Cell. Cardiol. 2001, 33, 1053–1063. [Google Scholar] [CrossRef]
- Hanberg, J.S.; Rao, V.; Ahmad, T.; Chunara, Z.; Mahoney, D.; Jackson, K. Inflammation and cardio-renal interactions in heart failure: A potential role for interleukin-6. Eur. J. Heart Fail. 2016, 118, 6072–6078. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Xu, H.; Davies, J.L.H.G. Increase of plasma IL-6 concentration with age in healthy subjects. Life Sci. 1992, 51, 1953–1956. [Google Scholar] [CrossRef]
- Ershler, W.B.; Sun, W.H.; Binkley, N.; Gravenstein, S.; Volk, M.J.; Kamoske, G.; Klopp, R.G.; Roecker, E.B.; Daynes, R.A.; Weindruch, R. Interleukin-6 and aging: Blood levels and mononuclear cell production increase with advancing age and in vitro production is modifiable by dietary restriction. Lymphokine Cytokine Res. 1993, 12, 225–230. [Google Scholar] [PubMed]
- Hager, K.; Machein, U.; Krieger, S.; Platt, D.; Seefried, G.B.J. Interleukin-6 and selected plasma proteins in healthy persons of different ages. Neurobiol. Aging 1994, 15, 771–772. [Google Scholar] [CrossRef]
- McKane, W.R.; Khosla, S.; Peterson, J.M.; Egan, K.R.B. Circulating levels of cytokines that modulate bone resorption: Effects of age and menopause in women. J. Bone Min. Res. 1994, 9, 1313–1318. [Google Scholar] [CrossRef]
- Kania, D.M.; Binkley, N.; Checovich, M.; Havighurst, T.; Schilling, M.E.W. Elevated plasma levels of interleukin-6 in postmenopausal women do not correlate with bone density. J. Am. Geriatr. Soc. 1995, 43, 236–239. [Google Scholar] [CrossRef]
- Cohen, H.J.; Pieper, C.F.; Harris, T.; Rao, K.M.M.; Curie, M.S. The association of plasma IL-6 levels with functional disability in community-dwelling elderly. J. Gerontol. A Biol. Sci. Med. Sci. 1997, 52, M201–M208. [Google Scholar] [CrossRef] [Green Version]
- Harris, T.B.; Ferrucci, L.; Tracy, R.P.; Corti, M.C.; Wacholder, S.; Ettinger, W.H., Jr.; Heimovitz, H.; Cohen, H.J.; Wallace, R. Associations of elevated interleukin-6 and C-reactive protein levels with mortality in the elderly. Am. J. Med. 1999, 106, 506–512. [Google Scholar] [CrossRef]
- Ferrucci, L.; Corsi, A.; Lauretani, F.; Bandinelli, S.; Bartali, B.; Taub, D.D.; Gurlanik, J.M.; Longo, D.M. The origins of age-related proinflammatory state. Blood 2005, 105, 2294–2299. [Google Scholar] [CrossRef] [Green Version]
- Sarkar, D.F.P. Molecular mechanisms of aging-associated inflammation. Cancer Lett. 2006, 236, 13–23. [Google Scholar] [CrossRef]
- Giuliani, N.; Sansoni, P.; Girasole, G.; Vescovini, R.; Passeri, G.; Passeri, M.; Pedrazzoni, M. Serum interleukin-6, soluble interleukin-6 receptor and soluble gp130 exhibit different patterns of age- and menopause-related changes. Exp. Gerontol. 2001, 36, 547–557. [Google Scholar] [CrossRef]
- Ticinesi, A.; Meschi, T.; Lauretani, F.; Felis, G.; Franchi, F.; Pedrolli, C.; Barichella, M.; Benati, G.; Di Nuzzo, S.; Ceda, G.P.; et al. Nutrition and inflammation in older individuals: Focus on vitamin D, n-3 polyunsaturated fatty acids and whey proteins. Nutrients 2006, 8, 186. [Google Scholar] [CrossRef] [Green Version]
- Fried, S.K.; Bunkin, D.A.; Greenberg, A. Omental and subcutaneous adipose tissues of obese subjects release interleukin-6: Depot difference and regulation by glucocorticoid. J. Clin. Endocrinol. Metab. 1998, 83, 847–850. [Google Scholar] [CrossRef] [PubMed]
- Malhi, N.; Moghaddam, N.; Andrade, J.; Hawkins, N.; Krahn, A.; Deyell, M. Catheter Ablation of Atrial Fibrillation in Heart Failure with Reduced Ejection Fraction: A Systematic Review and Meta-Analysis. Can. J. Cardiol. 2018, 34, S47–S48. [Google Scholar] [CrossRef]
- Issac, T.T.; Dokainish, H.; Lakkis, N.M. Role of Inflammation in Initiation and Perpetuation of Atrial Fibrillation. A Systematic Review of the Published Data. J. Am. Coll. Cardiol. 2007, 50, 2021–2028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taniguchi, N.; Miyasaka, Y.; Suwa, Y.; Harada, S.; Nakai, E.; Shiojima, I. Heart failure in atrial fibrillation: An update on clinical and echocardiographic implications. Circ. J. 2020, 84, 1212–1217. [Google Scholar] [CrossRef]
- Abe, I.; Teshima, Y.; Kondo, H.; Kaku, H.; Kira, S.; Ikebe, Y.; Saito, S.; Fukui, A.; Shinohara, T.; Yufu, K.; et al. Association of fibrotic remodeling and cytokines/chemokines content in epicardial adipose tissue with atrial myocardial fibrosis in patients with atrial fibrillation. Hear Rhythm 2018, 15, 1717–1727. [Google Scholar] [CrossRef]
- Zhao, L.; Li, S.; Ma, X.; Bai, R.; Liu, N.; Li, N.; Schoenhagen, P.; Ma, C. Prognostic Significance of Left Ventricular Fibrosis Assessed by T1 Mapping in Patients with Atrial Fibrillation and Heart Failure. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Total (N = 78) | IL-6 Normal (N = 36) | IL-6 High (N = 42) | p | |
|---|---|---|---|---|
| Baseline characteristics | ||||
| Age in years—median (SD) | 79.2 ± 6.6 | 78.5 ± 5.3 | 79.8 ± 7.5 | 0.374 a |
| Sex female—n (%) | 46 (59) | 21 (58.3) | 25 (59.5) | 0.915 b |
| Smoking | 4 (5.1) | 2 (5.6) | 2 (4.8) | 0.874 b |
| Sedentary | 48 (61.5) | 21 (58.3) | 27 (64.3) | 0.590 b |
| Underlying cardiomyopathy | ||||
| Hypertensive cardiomyopathy | 32 (41.1) | 17 (47.2) | 15 (35.7) | 0.303 b |
| Ischemic cardiomyopathy | 17 (21.8) | 5 (13.9) | 12(28.6) | 0.117 b |
| Valvulopathy | 20 (25.6) | 10 (27.8) | 10 (23.8) | 0.689 b |
| Nonischemic dilated cardiomyopathy | 6 (7.7) | 3 (8.3) | 3 (7.1) | 0.844 b |
| Cor pulmonale | 3 (3.8) | 1 (2.8) | 2 (4,8) | 0.65 b |
| Comorbidities | ||||
| Arterial hypertension | 78(100) | 36 (46) | 42 (54) | 0.521 b |
| Diabetes mellitus | 42 (53.8) | 15 (41.7) | 27 (64.3) | 0.046b |
| Hypercholesterolemia | 51 (65.4) | 19 (52.8) | 32 (76.2) | 0.030b |
| Metabolic syndrome | 24 (30.8) | 8 (22.2) | 16 (38.1) | 0.130 b |
| Atrial fibrillation | 56 (71.8) | 30 (83.3) | 26 (61.9) | 0.036b |
| Chronic renal failure | 31 (39.7) | 15 (41.7) | 16 (38.1) | 0.748 b |
| Anemia | 31 (39.7) | 9 (25) | 22 (52.4) | 0.014b |
| Obesity (BMI >30) | 17 (21.8) | 9 (25) | 8 (19) | 0.526 b |
| Functional evaluation | ||||
| Pfeiffer Test | ||||
| 0-2 mistakes | 73 (93.6) | 33 (91.7) | 40 (95.2) | 0.465 b |
| >2 mistakes | 5 (6.4) | 3 (8.3) | 2 (4.8) | |
| Nutritional evaluation (MNA Test) | ||||
| Normal (≥24 points) | 52 (66.7) | 25 (75.8) | 27 (67.5) | 0.438 b |
| At risk of malnutrition or established malnutrition (<24 points) | 21 (26.9) | 8 (24.2) | 13 (32.5) | |
| Frailty (Barber >1) | 71 (91) | 32 (88.9) | 39 (92.9) | 0.541 b |
| Echocardiographic parameters | ||||
| Left ventricular hypertrophy | 47 (60.3) | 21 (58.3) | 26 (61.9) | 0.648 b |
| Preserved LVEF (≥50%) | 50 (64.1) | 20 (55.6) | 30 (71.4) | 0.145b |
| Reduced LVEF (<50%) | 28(35.8) | 16 (44.4) | 12 (28.6) | 0.163 d |
| Vital parameters | ||||
| SBP (mmHg) | 136 ± 21 | 136 ± 19 | 135 ± 23 | 0.230 |
| DBP (mmHg) | 68 ± 10 | 70 ± 9 | 66 ± 10 | 0.697 |
| Heart rate (beats/min) | 78 ± 16 | 77 ± 17 | 78 ± 16 | 0.582 |
| Blood results | ||||
| Hemoglobin (g/dl) | 12.7 ± 1.9 | 13.2 ± 2.3 | 12.3 ±2.1 | <0.001 |
| Ferritin (ng/mL) | 175 ± 289 | 147 ± 223 | 194 ± 322 | 0.108 c |
| Creatinine (mg/dl) | 1.28 ± 0.65 | 1.08 ± 0.57 | 1.35 ± 0.69 | 0.024 |
| CKD-EPI glomerular filtration rate (mL/min/m2) | 46 ± 26 | 59.95 ± 35 | 43.6 ± 19 | 0.007 |
| Microalbuminuria (mg/L) | 16.9 ± 60.7 | 15.9 ± 25.8 | 17.6 ± 99 | 0.451 c |
| HbA1c (%) | 6 ± 1 | 6 ± 1 | 6.3 ± 1 | 0.108 c |
| NT-ProBNP (pg/mL) | 1613 ± 2297 | 1244 ± 2780 | 1990 ± 4019 | 0.061 c |
| Usual treatment | ||||
| Beta Blockers | 52 (66.7) | 21 (58.3) | 31 (73.8) | 0.148 b |
| Furosemide | 65 (83.3) | 31 (86.1) | 34 (81) | 0.542 b |
| Chlorthalidone | 6 (7.7) | 5 (13.9) | 1 (2.4) | 0.057 b |
| Spironolactone/Eplerenone | 33 (42.3) | 13 (36.1) | 20 (47.6) | 0.305 b |
| ACE inhibitors/Angiotensin II Antagonist | 23 (29.5) | 13 (36.1) | 10 (23.8) | 0.235 b |
| Statins | 52 (66.7) | 23 (63.9) | 29 (69) | 0.63 b |
| Anticoagulation | 56 (71.8) | 31 (86.1) | 25 (59.5) | 0.009b |
| Follow-up | ||||
| Event (combined) | 40 (51.3) | 15 (41.7) | 25 (59.5) | 0.116 b |
| HF hospitalization | 25 (32.1) | 8 (22.2) | 17 (40.5) | 0.069d |
| Visit to ED for HF | 13 (16.7) | 4 (11.1) | 9 (21.4) | 0.223 b |
| Visit to Day Care Hospital for HF | 11 (14.1) | 6 (16.7) | 5 (11.9) | 0.547 b |
| Mortality from any cause | 8 (10.3) | 1 (2.8) | 7 (16.7) | 0.044b |
| Multivariable OR (95%CI) | p | |
|---|---|---|
| Atrial fibrillation | 1.240 (0.332–4.626) | 0.749 |
| Diabetes mellitus | 0.41 (0.128–01.134) | 0.134 |
| Anemia | 3.513 (1.163–10.607) | 0.026 |
| Hypercholesterolemia | 0.565 (0.177–1.802) | 0.335 |
| GFR CKD EPI | 0.963 (0.936–0.991) | 0.009 |
| Multivariable | ||
|---|---|---|
| Factors Associated with Mortality | OR (95%CI) | p |
| Age | 1.131 (0.992–1.290) | 0.066 |
| Left ventricular ejection fraction | 0.207 (0.018–2.393) | 0.207 |
| IL-6 levels | 1.037 (1.000–1.074) | 0.048 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Povar-Echeverría, M.; Auquilla-Clavijo, P.E.; Andrès, E.; Martin-Sánchez, F.J.; Laguna-Calle, M.V.; Calvo-Elías, A.E.; Lorenzo-Villalba, N.; Méndez-Bailón, M. Interleukin-6 Could Be a Potential Prognostic Factor in Ambulatory Elderly Patients with Stable Heart Failure: Results from a Pilot Study. J. Clin. Med. 2021, 10, 504. https://doi.org/10.3390/jcm10030504
Povar-Echeverría M, Auquilla-Clavijo PE, Andrès E, Martin-Sánchez FJ, Laguna-Calle MV, Calvo-Elías AE, Lorenzo-Villalba N, Méndez-Bailón M. Interleukin-6 Could Be a Potential Prognostic Factor in Ambulatory Elderly Patients with Stable Heart Failure: Results from a Pilot Study. Journal of Clinical Medicine. 2021; 10(3):504. https://doi.org/10.3390/jcm10030504
Chicago/Turabian StylePovar-Echeverría, Marina, Pablo Esteban Auquilla-Clavijo, Emmanuel Andrès, Francisco Javier Martin-Sánchez, María Victoria Laguna-Calle, Alberto Elpidio Calvo-Elías, Noel Lorenzo-Villalba, and Manuel Méndez-Bailón. 2021. "Interleukin-6 Could Be a Potential Prognostic Factor in Ambulatory Elderly Patients with Stable Heart Failure: Results from a Pilot Study" Journal of Clinical Medicine 10, no. 3: 504. https://doi.org/10.3390/jcm10030504
APA StylePovar-Echeverría, M., Auquilla-Clavijo, P. E., Andrès, E., Martin-Sánchez, F. J., Laguna-Calle, M. V., Calvo-Elías, A. E., Lorenzo-Villalba, N., & Méndez-Bailón, M. (2021). Interleukin-6 Could Be a Potential Prognostic Factor in Ambulatory Elderly Patients with Stable Heart Failure: Results from a Pilot Study. Journal of Clinical Medicine, 10(3), 504. https://doi.org/10.3390/jcm10030504