
Dynamic Susceptibility Perfusion Imaging for Differentiating Progressive Disease from Pseudoprogression in Diffuse Glioma Molecular Subtypes

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
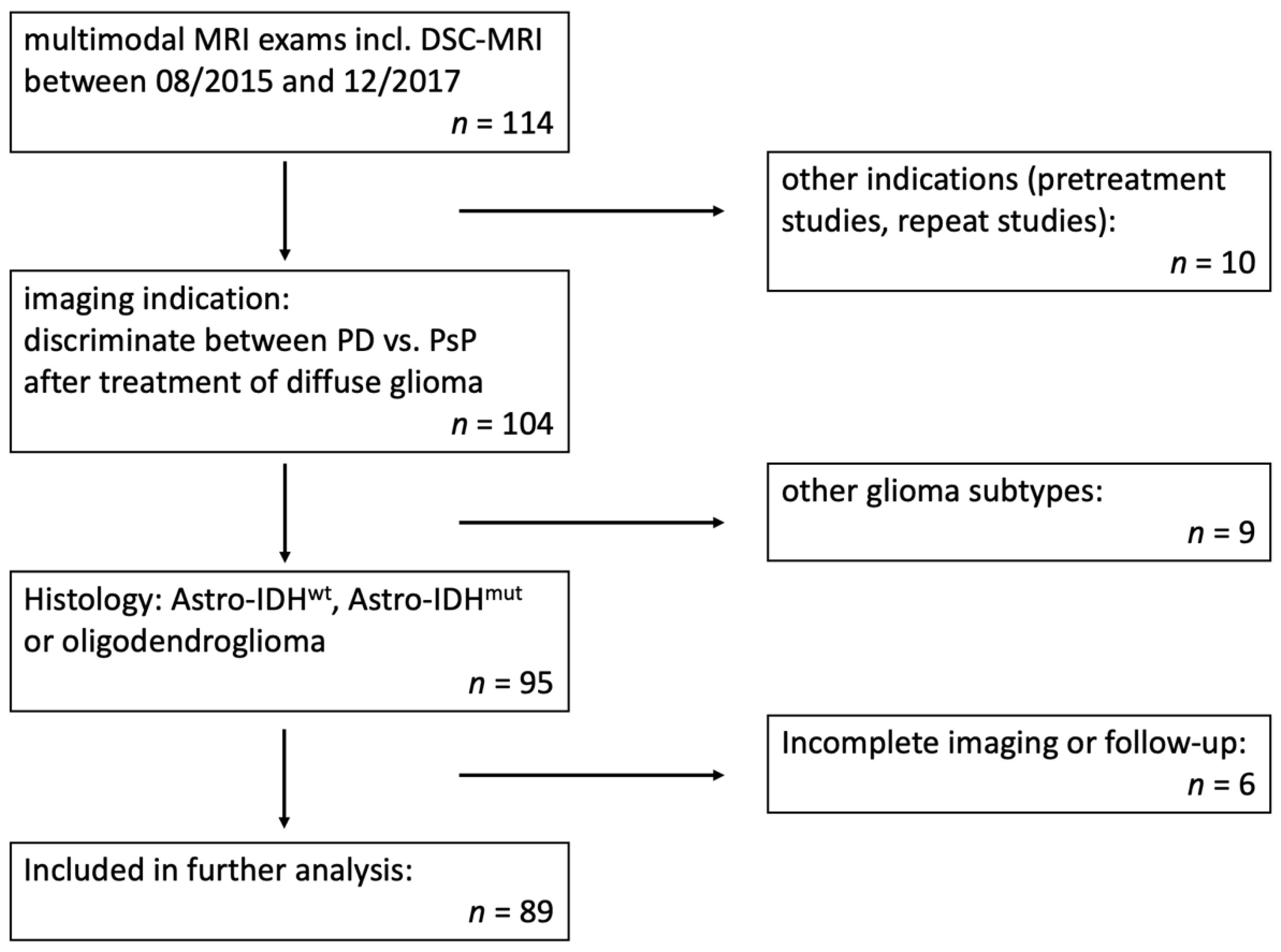
2.1. Patients
2.2. MRI Examinations
2.3. Statistical Analysis
3. Results
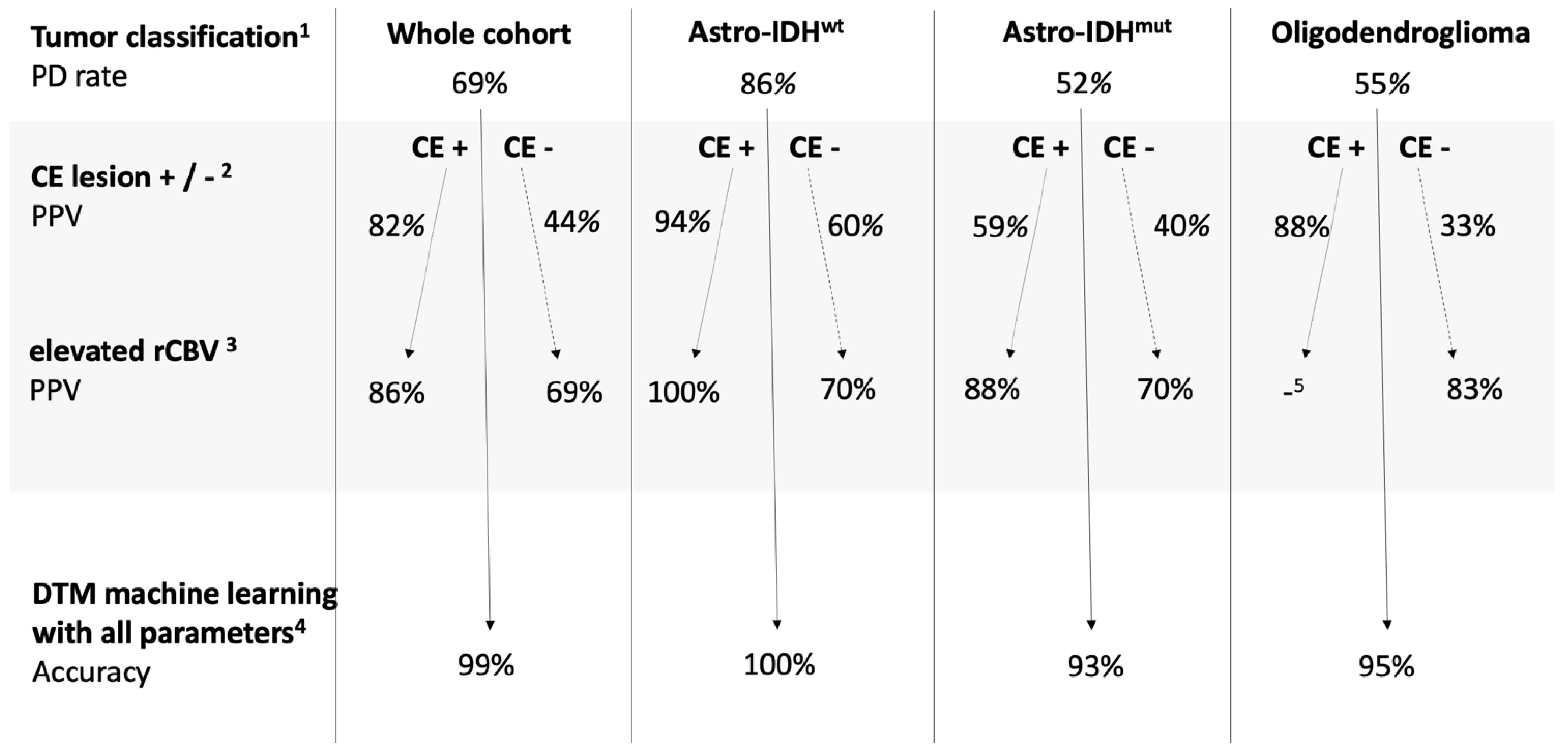
Multilevel Classification by Tumor Subtype and Imaging Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Astro-IDHmut | astrocytic tumor with isocitrate dehydrogenase mutation |
| Astro-IDHwt | isocitrate dehydrogenase wildtype astrocytic tumor |
| CBV | cerebral blood volume |
| CE | contrast enhancement |
| CNS | central nervous system |
| DSC-MRI | dynamic susceptibility perfusion imaging |
| DTM | decision tree model |
| FLAIR | fluid-attenuated inversion recovery |
| IDH | isocitrate dehydrogenase |
| MGMT | O6-methylguanine-DNA methyl-transferase |
| MRI | magnetic resonance imaging |
| PD | progressive disease |
| PPV | positive predictive value |
| PsP | pseudoprogression |
| RANO | Response Assessment in Neuro-Oncology |
| ROC | receiver operating characteristics |
| rCBV | relative cerebral blood volume |
| SD | standard deviation |
| VOIce | contrast-enhancing disease-specific volume of interest |
| VOIflair | volume of interest with suspicious disease-specific signal alterations in the FLAIR |
| WHO | World Health Organization |
References
- Zikou, A.; Sioka, C.; Alexiou, G.A.; Fotopoulos, A.; Voulgaris, S.; Argyropoulou, M.I. Radiation Necrosis, Pseudoprogression, Pseudoresponse, and Tumor Recurrence: Imaging Challenges for the Evaluation of Treated Gliomas. Contrast Media Mol. Imaging 2018, 2018, 6828396. [Google Scholar] [CrossRef]
- Delgado-Lopez, P.D.; Rinones-Mena, E.; Corrales-Garcia, E.M. Treatment-related changes in glioblastoma: A review on the controversies in response assessment criteria and the concepts of true progression, pseudoprogression, pseudoresponse and radionecrosis. Clin. Transl. Oncol. 2018, 20, 939–953. [Google Scholar] [CrossRef]
- Rowe, L.S.; Butman, J.A.; Mackey, M.; Shih, J.H.; Cooley-Zgela, T.; Ning, H.; Gilbert, M.R.; Smart, D.K.; Camphausen, K.; Krauze, A.V. Differentiating pseudoprogression from true progression: Analysis of radiographic, biologic, and clinical clues in GBM. J. Neurooncol. 2018, 139, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; Degroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated response assessment criteria for high-grade gliomas: Response assessment in neuro-oncology working group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef]
- Ellingson, B.M.; Wen, P.Y.; Cloughesy, T.F. Modified Criteria for Radiographic Response Assessment in Glioblastoma Clinical Trials. Neurotherapeutics 2017, 14, 307–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, H.; Weller, M.; Huang, R.; Finocchiaro, G.; Gilbert, M.R.; Wick, W.; Ellingson, B.M.; Hashimoto, N.; Pollack, I.F.; Brandes, A.A.; et al. Immunotherapy response assessment in neuro-oncology: A report of the RANO working group. Lancet Oncol. 2015, 16, E534–E542. [Google Scholar] [CrossRef] [Green Version]
- Brendle, C.; Hempel, J.M.; Schittenhelm, J.; Skardelly, M.; Reischl, G.; Bender, B.; Ernemann, U.; la Fougere, C.; Klose, U. Glioma grading by dynamic susceptibility contrast perfusion and (11)C-methionine positron emission tomography using different regions of interest. Neuroradiology 2018, 60, 381–389. [Google Scholar] [CrossRef]
- Kickingereder, P.; Sahm, F.; Radbruch, A.; Wick, W.; Heiland, S.; Deimling, A.; Bendszus, M.; Wiestler, B. IDH mutation status is associated with a distinct hypoxia/angiogenesis transcriptome signature which is non-invasively predictable with rCBV imaging in human glioma. Sci. Rep. 2015, 5, 16238. [Google Scholar] [CrossRef]
- SongTao, Q.; Lei, Y.; Si, G.; YanQing, D.; HuiXia, H.; XueLin, Z.; LanXiao, W.; Fei, Y. IDH mutations predict longer survival and response to temozolomide in secondary glioblastoma. Cancer Sci. 2012, 103, 269–273. [Google Scholar] [CrossRef]
- Patel, P.; Baradaran, H.; Delgado, D.; Askin, G.; Christos, P.; John Tsiouris, A.; Gupta, A. MR perfusion-weighted imaging in the evaluation of high-grade gliomas after treatment: A systematic review and meta-analysis. Neuro Oncol. 2017, 19, 118–127. [Google Scholar] [CrossRef] [Green Version]
- Prager, A.J.; Martinez, N.; Beal, K.; Omuro, A.; Zhang, Z.; Young, R.J. Diffusion and perfusion MRI to differentiate treatment-related changes including pseudoprogression from recurrent tumors in high-grade gliomas with histopathologic evidence. AJNR Am. J. Neuroradiol. 2015, 36, 877–885. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Goh, M.J.; Kim, N.; Choi, C.G.; Kim, S.J.; Kim, J.H. Which combination of MR imaging modalities is best for predicting recurrent glioblastoma? Study of diagnostic accuracy and reproducibility. Radiology 2014, 273, 831–843. [Google Scholar] [CrossRef]
- Boxerman, J.L.; Ellingson, B.M.; Jeyapalan, S.; Elinzano, H.; Harris, R.J.; Rogg, J.M.; Pope, W.B.; Safran, H. Longitudinal DSC-MRI for Distinguishing Tumor Recurrence From Pseudoprogression in Patients With a High-grade Glioma. Am. J. Clin. Oncol. 2017, 40, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Elshafeey, N.; Kotrotsou, A.; Hassan, A.; Elshafei, N.; Hassan, I.; Ahmed, S.; Abrol, S.; Agarwal, A.; El Salek, K.; Bergamaschi, S.; et al. Multicenter study demonstrates radiomic features derived from magnetic resonance perfusion images identify pseudoprogression in glioblastoma. Nat. Commun. 2019, 10, 3170. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.; Wong, K.K.; Young, G.S.; Guo, L.; Wong, S.T. Support vector machine multiparametric MRI identification of pseudoprogression from tumor recurrence in patients with resected glioblastoma. J. Magn. Reson. Imaging 2011, 33, 296–305. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Martinez-Lage, M.; Sakai, Y.; Chawla, S.; Kim, S.G.; Alonso-Basanta, M.; Lustig, R.A.; Brem, S.; Mohan, S.; Wolf, R.L.; et al. Differentiating Tumor Progression from Pseudoprogression in Patients with Glioblastomas Using Diffusion Tensor Imaging and Dynamic Susceptibility Contrast MRI. AJNR Am. J. Neuroradiol. 2016, 37, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Leao, D.J.; Craig, P.G.; Godoy, L.F.; Leite, C.C.; Policeni, B. Response Assessment in Neuro-Oncology Criteria for Gliomas: Practical Approach Using Conventional and Advanced Techniques. AJNR Am. J. Neuroradiol. 2020, 41, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Lu, V.M.; Welby, J.P.; Laack, N.N.; Mahajan, A.; Daniels, D.J. Pseudoprogression after radiation therapies for low grade glioma in children and adults: A systematic review and meta-analysis. Radiother. Oncol. 2020, 142, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Chukwueke, U.N.; Wen, P.Y. Use of the Response Assessment in Neuro-Oncology (RANO) criteria in clinical trials and clinical practice. CNS Oncol. 2019, 8, CNS28. [Google Scholar] [CrossRef] [Green Version]
- Ellingson, B.M.; Bendszus, M.; Boxerman, J.; Barboriak, D.; Erickson, B.J.; Smits, M.; Nelson, S.J.; Gerstner, E.; Alexander, B.; Goldmacher, G.; et al. Consensus recommendations for a standardized Brain Tumor Imaging Protocol in clinical trials. Neuro Oncol. 2015, 17, 1188–1198. [Google Scholar] [CrossRef] [Green Version]
- Batash, R.; Asna, N.; Schaffer, P.; Francis, N.; Schaffer, M. Glioblastoma Multiforme, Diagnosis and Treatment; Recent Literature Review. Curr. Med. Chem. 2017, 24, 3002–3009. [Google Scholar] [CrossRef]
- Audureau, E.; Chivet, A.; Ursu, R.; Corns, R.; Metellus, P.; Noel, G.; Zouaoui, S.; Guyotat, J.; Le Reste, P.J.; Faillot, T.; et al. Prognostic factors for survival in adult patients with recurrent glioblastoma: A decision-tree-based model. J. Neurooncol. 2018, 136, 565–576. [Google Scholar] [CrossRef]
- Shah, R.; Vattoth, S.; Jacob, R.; Manzil, F.F.; O’Malley, J.P.; Borghei, P.; Patel, B.N.; Cure, J.K. Radiation necrosis in the brain: Imaging features and differentiation from tumor recurrence. Radiographics 2012, 32, 1343–1359. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.J.; Leeds, N.E.; Fuller, G.N.; Van Tassel, P.; Maor, M.H.; Sawaya, R.E.; Levin, V.A. Malignant gliomas: MR imaging spectrum of radiation therapy- and chemotherapy-induced necrosis of the brain after treatment. Radiology 2000, 217, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Welker, K.; Boxerman, J.; Kalnin, A.; Kaufmann, T.; Shiroishi, M.; Wintermark, M. American Society of Functional Neuroradiology MR Perfusion Standards and Practice Subcommittee of the ASFNR Clinical Practice Committee: ASFNR recommendations for clinical performance of MR dynamic susceptibility contrast perfusion imaging of the brain. AJNR Am. J. Neuroradiol. 2015, 36, E41–E51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, B.; Wang, S.; Tu, M.; Wu, B.; Han, P.; Xu, H. The diagnostic performance of perfusion MRI for differentiating glioma recurrence from pseudoprogression: A meta-analysis. Medicine 2017, 96, e6333. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, G.; Hammam, A.; Anjari, M.; D’Arco, D.F.; Bisdas, D.S. Glioma surveillance imaging: Current strategies, shortcomings, challenges and outlook. BJR Open 2020, 2, 20200009. [Google Scholar] [CrossRef] [PubMed]
- Steidl, E.; Müller, M.; Müller, A.; Herrlinger, U.; Hattingen, E. Longitudinal, leakage corrected and uncorrected rCBV during the first-line treatment of glioblastoma: A prospective study. J. Neurooncol. 2019. [Google Scholar] [CrossRef]
- Lee, J.; Wang, N.; Turk, S.; Mohammed, S.; Lobo, R.; Kim, J.; Liao, E.; Camelo-Piragua, S.; Kim, M.; Junck, L.; et al. Discriminating pseudoprogression and true progression in diffuse infiltrating glioma using multi-parametric MRI data through deep learning. Sci Rep. 2020, 10, 20331. [Google Scholar] [CrossRef] [PubMed]
- Akbari, H.; Rathore, S.; Bakas, S.; Nasrallah, M.P.; Shukla, G.; Mamourian, E.; Rozycki, M.; Bagley, S.J.; Rudie, J.D.; Flanders, A.E.; et al. Histopathology-validated machine learning radiographic biomarker for noninvasive discrimination between true progression and pseudo-progression in glioblastoma. Cancer 2020, 126, 2625–2636. [Google Scholar] [CrossRef]
- Li, H.; Li, J.; Cheng, G.; Zhang, J.; Li, X. IDH mutation and MGMT promoter methylation are associated with the pseudoprogression and improved prognosis of glioblastoma multiforme patients who have undergone concurrent and adjuvant temozolomide-based chemoradiotherapy. Clin. Neurol. Neurosurg. 2016, 151, 31–36. [Google Scholar] [CrossRef]
- Lin, A.L.; White, M.; Miller-Thomas, M.M.; Fulton, R.S.; Tsien, C.I.; Rich, K.M.; Schmidt, R.E.; Tran, D.D.; Dahiya, S. Molecular and histologic characteristics of pseudoprogression in diffuse gliomas. J. Neurooncol. 2016, 130, 529–533. [Google Scholar] [CrossRef] [Green Version]
- Boxerman, J.L.; Zhang, Z.; Safriel, Y.; Rogg, J.M.; Wolf, R.L.; Mohan, S.; Marques, H.; Sorensen, A.G.; Gilbert, M.R.; Barboriak, D.P. Prognostic value of contrast enhancement and FLAIR for survival in newly diagnosed glioblastoma treated with and without bevacizumab: Results from ACRIN 6686. Neuro Oncol. 2018, 20, 1400–1410. [Google Scholar] [CrossRef]
- Wen, P.Y.; Chang, S.M.; Van den Bent, M.J.; Vogelbaum, M.A.; Macdonald, D.R.; Lee, E.Q. Response Assessment in Neuro-Oncology Clinical Trials. J. Clin. Oncol. 2017, 35, 2439–2449. [Google Scholar] [CrossRef]
- Pope, W.B.; Hessel, C. Response assessment in neuro-oncology criteria: Implementation challenges in multicenter neuro-oncology trials. AJNR Am. J. Neuroradiol. 2011, 32, 794–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latysheva, A.; Emblem, K.E.; Brandal, P.; Vik-Mo, E.O.; Pahnke, J.; Roysland, K.; Hald, J.K.; Server, A. Dynamic susceptibility contrast and diffusion MR imaging identify oligodendroglioma as defined by the 2016 WHO classification for brain tumors: Histogram analysis approach. Neuroradiology 2019, 61, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Xing, Z.; Zhang, H.; She, D.; Lin, Y.; Zhou, X.; Zeng, Z.; Cao, D. IDH genotypes differentiation in glioblastomas using DWI and DSC-PWI in the enhancing and peri-enhancing region. Acta Radiol. 2019, 60, 1663–1672. [Google Scholar] [CrossRef]
- Suh, C.H.; Kim, H.S.; Jung, S.C.; Choi, C.G.; Kim, S.J. Imaging prediction of isocitrate dehydrogenase (IDH) mutation in patients with glioma: A systemic review and meta-analysis. Eur. Radiol. 2019, 29, 745–758. [Google Scholar] [CrossRef] [PubMed]
- Galante, J.R.; Rodriguez, F.; Grossman, S.A.; Strowd, R.E. Late post-treatment radiographic changes 3 years following chemoradiation for glioma: The importance of histopathology. CNS Oncol. 2017. [Google Scholar] [CrossRef]
- Voss, M.; Franz, K.; Steinbach, J.P.; Fokas, E.; Forster, M.T.; Filipski, K.; Hattingen, E.; Wagner, M.; Breuer, S. Contrast enhancing spots as a new pattern of late onset pseudoprogression in glioma patients. J. Neurooncol. 2019, 142, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Shirahata, M.; Ono, T.; Stichel, D.; Schrimpf, D.; Reuss, D.E.; Sahm, F.; Koelsche, C.; Wefers, A.; Reinhardt, A.; Huang, K.; et al. Novel, improved grading system(s) for IDH-mutant astrocytic gliomas. Acta Neuropathol. 2018, 136, 153–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasselblatt, M.; Jaber, M.; Reuss, D.; Grauer, O.; Bibo, A.; Terwey, S.; Schick, U.; Ebel, H.; Niederstadt, T.; Stummer, W.; et al. Diffuse Astrocytoma, IDH-Wildtype: A Dissolving Diagnosis. J. Neuropathol. Exp. Neurol. 2018, 77, 422–425. [Google Scholar] [CrossRef] [Green Version]
- Zhou, M.; Niu, C.; Jia, L.; He, H. The value of MGMT promote methylation and IDH-1 mutation on diagnosis of pseudoprogression in patients with high-grade glioma: A meta-analysis. Medicine 2019, 98, e18194. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Astro-IDHwt | Astro-IDHmut | Oligodendroglioma | |
|---|---|---|---|
| Number of patients (n) | 42 | 27 | 20 |
| Age (mean ± SD) | 53 ± 14 | 40 ± 9 | 50 ± 10 |
| Sex (female/male) | 13/29 | 14/13 | 12/8 |
| Progressive Disease (n) | 36 | 14 | 11 |
| Tumor grade | |||
| WHO grade II (n) | 4 | 13 | 13 |
| WHO grade III (n) | 7 | 9 | 7 |
| WHO grade IV (n) | 31 | 5 | 0 |
| MGMT promoter | |||
| Methylated (n) | 16 | 11 | 20 |
| Unmethylated (n) | 25 | 8 | 0 |
| Not known (n) | 1 | 8 | 0 |
| Preceding therapy | |||
| Radiochemotherapy (n) | 27 | 15 | 10 |
| Immunotherapy (n) | 11 | 4 | 1 |
| None within 2 years (n) | 4 | 8 | 9 |
| Astro-IDHwt | Astro-IDHmut | Oligodendroglioma | |
|---|---|---|---|
| Prevalence of CE lesion | 74% (31/42) | 63% (17/27) | 40% (8/20) |
| PD Rate in the Presence of a CE Lesion | 94% (29/31) | 59% (10/17) | 88% (7/8) |
| p-value | 0.0214 * | 0.4401 | 0.0281 * |
| Accuracy | 0.81 (0.66–0.91) | 0.59 (0.39–0.78) | 0.75 (0.51–0.91) |
| Sensitivity | 0.83 (0.67–0.94) | 0.71 (0.42–0.92) | 0.63 (0.31–0.89) |
| Specificity | 0.67 (0.22–0.96) | 0.46 (0.19–0.75) | 0.89 (0.52–1) |
| Parameter | Whole Tumor (VOIflair) | Contrast-Enhancing Lesion (VOIce) | Whole Tumor (VOIflair) in Tumors without Contrast-Enhancing Lesion | |||
|---|---|---|---|---|---|---|
| Mean rCBV | Maximal rCBV | Mean rCBV | Maximal rCBV | Mean rCBV | Maximal rCBV | |
| Astro-IDHwt | ||||||
| Cut-off value a | 0.81 | 1.7 | 0.77 | 1.18 | 1.03 | 2.06 |
| Accuracy | 0.64 (0.48–0.78) | 0.62 (0.46–0.76) | 1 (0.89–1) | 1 (0.89–1) | 0.7 (0.35–0.93) | 0.7 (0.35–0.93) |
| Sensitivity | 0.58 (0.41–0.75) | 0.56 (0.38–0.72) | 1 (0.88–1) | 1 (0.88–1) | 0.5 (0.12–0.88) | 0.5 (0.12–0.88) |
| Specificity | 1 (0.54–1) | 1 (0.54–1) | 1 (0.16–1) | 1 (0.16–1) | 1 (0.4–1) | 1 (0.4–1) |
| Astro-IDHmut | ||||||
| Cut-off value a | 0.98 | 1.82 | 1.03 | 1.93 | 1.31 | 2.34 |
| Accuracy | 0.81 (0.62–0.94) | 0.74 (0.54–0.89) | 0.82 (0.57–0.96) | 0.76 (0.5–0.93) | 0.6 (0.26–0.88) | 0.7 (0.35–0.93) |
| Sensitivity | 0.93 (0.66–1) | 0.79 (0.49–0.95) | 0.9 (0.56–1) | 0.7 (0.35–0.93) | 1 (0.4–1) | 1 (0.4–1) |
| Specificity | 0.69 (0.39–0.91) | 0.69 (0.39–0.91) | 0.71 (0.29–0.96) | 0.86 (0.42–1) | 0.33 (0.04–0.78) | 0.5 (0.12–0.88) |
| Oligodendroglioma | ||||||
| Cut-off value a | 0.87 | 1.55 | no data b | 0.81 | 1.55 | |
| Accuracy | 0.75 (0.51–0.91) | 0.8 (0.56–0.94) | 0.75 (0.43–0.95) | 0.83 (0.52–0.98) | ||
| Sensitivity | 0.82 (0.48–0.98) | 0.91 (0.59–1) | 1 (0.4–1) | 1 (0.4–1) | ||
| Specificity | 0.67 (0.3–0.93) | 0.67 (0.3–0.93) | 0.63 (0.25–0.91) | 0.75 (0.35–0.97) | ||
| Astro-IDHwt | Astro-IDHmut | Oligodendroglioma | |
|---|---|---|---|
| r2 | 0.87 | 0.70 | 0.72 |
| Cross-validated r2 | 0.97 | 0.32 | 0.55 |
| Accuracy | 1.0 (0.92–1) | 0.93 (0.76–0.99) | 0.95 (0.75–1) |
| Sensitivity | 1.0 (0.9–1) | 0.93 (0.66–1) | 1.0 (0.72–1) |
| Specificity | 1.0 (0.54–1) | 0.92 (0.64–1) | 0.89 (0.52–1) |
| Most Important rCBV Histogram Parameter a | Mean rCBV in VOIce | Mean rCBV in VOIflair | Standard deviation of rCBV in VOIflair |
| Further Important rCBV Parameters | Skewness of rCBV in VOIflair | Kurtosis of rCBV in VOIflair; Minimal rCBV in VOIflair | 75th percentile of rCBV in VOIflair |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richter, V.; Klose, U.; Bender, B.; Rabehl, K.; Skardelly, M.; Schittenhelm, J.; Tabatabai, G.; Hempel, J.-M.; Ernemann, U.; Brendle, C. Dynamic Susceptibility Perfusion Imaging for Differentiating Progressive Disease from Pseudoprogression in Diffuse Glioma Molecular Subtypes. J. Clin. Med. 2021, 10, 598. https://doi.org/10.3390/jcm10040598
Richter V, Klose U, Bender B, Rabehl K, Skardelly M, Schittenhelm J, Tabatabai G, Hempel J-M, Ernemann U, Brendle C. Dynamic Susceptibility Perfusion Imaging for Differentiating Progressive Disease from Pseudoprogression in Diffuse Glioma Molecular Subtypes. Journal of Clinical Medicine. 2021; 10(4):598. https://doi.org/10.3390/jcm10040598
Chicago/Turabian StyleRichter, Vivien, Uwe Klose, Benjamin Bender, Katharina Rabehl, Marco Skardelly, Jens Schittenhelm, Ghazaleh Tabatabai, Johann-Martin Hempel, Ulrike Ernemann, and Cornelia Brendle. 2021. "Dynamic Susceptibility Perfusion Imaging for Differentiating Progressive Disease from Pseudoprogression in Diffuse Glioma Molecular Subtypes" Journal of Clinical Medicine 10, no. 4: 598. https://doi.org/10.3390/jcm10040598
APA StyleRichter, V., Klose, U., Bender, B., Rabehl, K., Skardelly, M., Schittenhelm, J., Tabatabai, G., Hempel, J. -M., Ernemann, U., & Brendle, C. (2021). Dynamic Susceptibility Perfusion Imaging for Differentiating Progressive Disease from Pseudoprogression in Diffuse Glioma Molecular Subtypes. Journal of Clinical Medicine, 10(4), 598. https://doi.org/10.3390/jcm10040598